psoriasis: a cutaneous or systemic disease · • affects 2-3% of people worldwide2 ... (4 vs 40...
TRANSCRIPT
Psoriasis:
A Cutaneous or Systemic Disease
Ian D.R. Landells, MD, FRCPCClinical Chief Dermatology, Eastern Health
Clinical Assistant Professor
Disciplines of Medicine and Paediatrics
Faculty of Medicine
Memorial University of Newfoundland
Copyright © 2017 by Sea Courses Inc.
All rights reserved. No part of this document may be
reproduced, copied, stored, or transmitted in any form or
by any means – graphic, electronic, or mechanical,
including photocopying, recording, or information storage
and retrieval systems without prior written permission of
Sea Courses Inc. except where permitted by law.
Sea Courses is not responsible for any speaker or
participant’s statements, materials, acts or omissions.
Overview and Epidemiology of
Psoriasis• Chronic, immune-mediated inflammatory disease of the skin1
– But really much more than the skin
• Affects 2-3% of people worldwide2
– An estimated 1 million Canadians have psoriasis3
• Nearly one quarter of psoriasis patients have moderate-to-severe
disease
1. Gudjonsson JE, Elder JT. Clin Dermatol 2007;25:535
2. NIAMS. NIH Publication No 03-5040; 2003
3. Guenther L, et al. J Cutan Med Surg 2004;8:321
4. National Psoriasis Foundation: Statistics 2003
Psoriasis Pathogenesis
• TH1/TH17 T-Cell Mediated Disease of Skin
• Hyperproliferation of keratinocytes (4 vs 40
days)
• Abnormal keratinocyte differentiation
• Infiltration of inflammatory cells
• Impaired barrier function
• Likely polygenic and multifactorial
• Genes CARD14, TNF-A, HLA-CW6 + trigger
Psoriasis in Canada
• ~ 3% (1 million) people have psoriasis
• ~150,000 people with psoriasis are being treated
– 60,000 psoriasis patients have moderate-to-severe disease
• ~40 psoriasis-related deaths each year
– Includes suicide; treatment-related complications, & other disease-related issues
– The National Psoriasis Foundation survey reported that psoriasis patients in the youngest group (18 to 34 years of age) contemplated suicide (10%), experienced depression (54%)
– * Canadian rates calculated from US rates
National Psoriasis Foundation.
Krueger G, et al. Arch Dermatol. 2001;137:280-284.
O V E R V I E W
Nail psoriasis 3
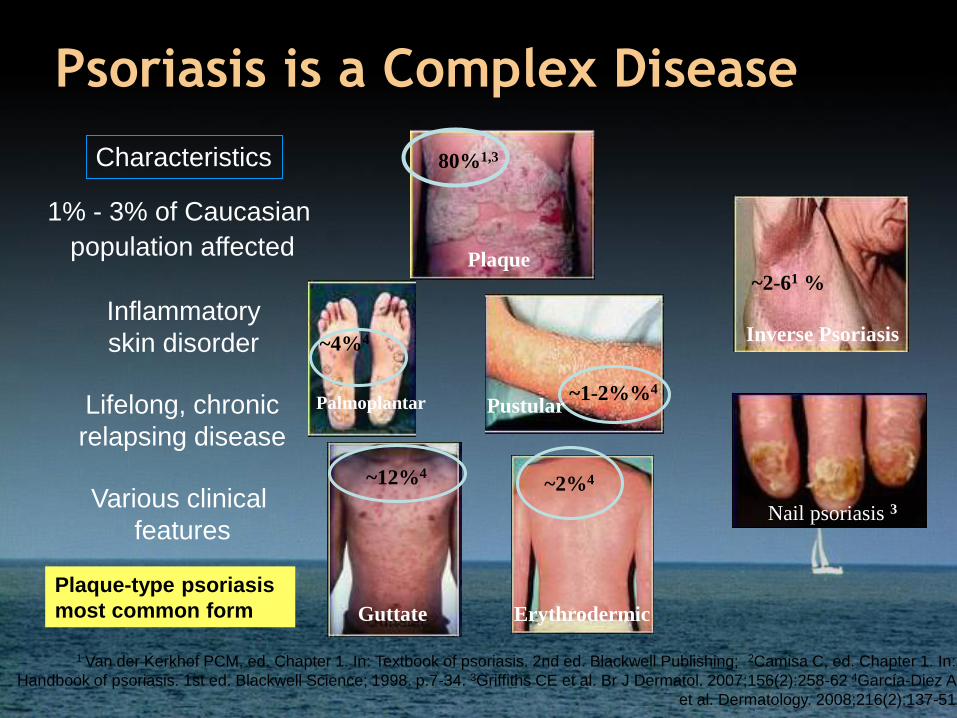
Psoriasis is a Complex Disease
Characteristics
Inflammatory
skin disorder
Various clinical
features
Lifelong, chronic
relapsing disease
Plaque-type psoriasis
most common form
1% - 3% of Caucasian
population affected
1 Van der Kerkhof PCM, ed. Chapter 1. In: Textbook of psoriasis. 2nd ed. Blackwell Publishing; 2Camisa C, ed. Chapter 1. In:
Handbook of psoriasis. 1st ed. Blackwell Science; 1998. p.7-34. 3Griffiths CE et al. Br J Dermatol. 2007;156(2):258-62 4García-Diez A
et al. Dermatology. 2008;216(2):137-51
80%1,3
~1-2%%4
~12%4~2%4
~2-61 %
Guttate Erythrodermic
Inverse Psoriasis
Pustular
Plaque
Palmoplantar
~4%4
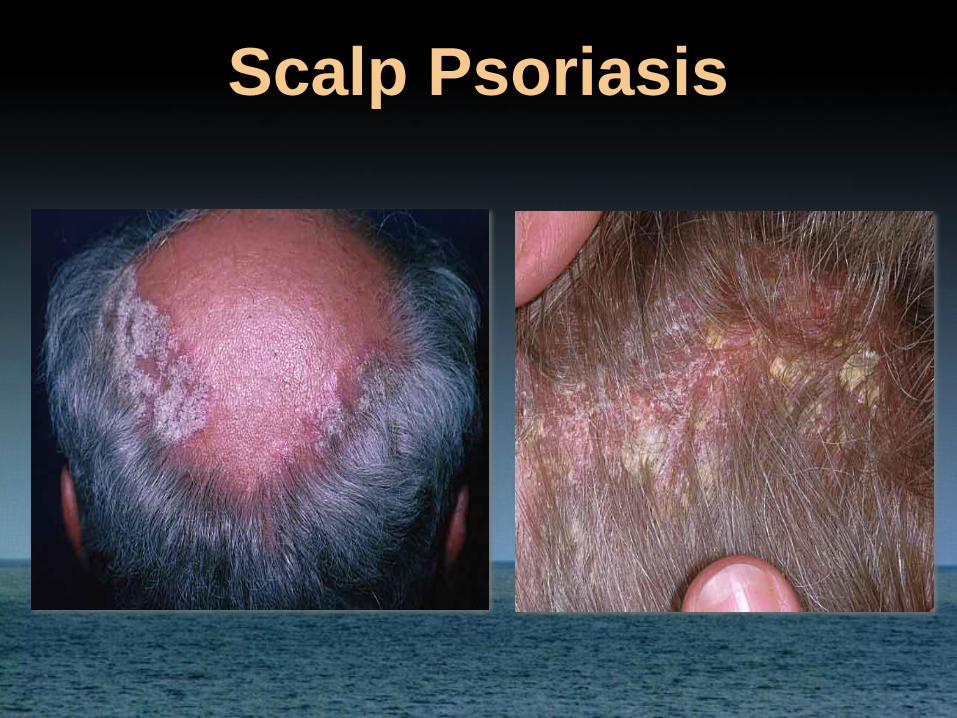
Scalp Psoriasis

Inverse Psoriasis

Palmoplantar Pustular Psoriasis

Guttate Psoriasis
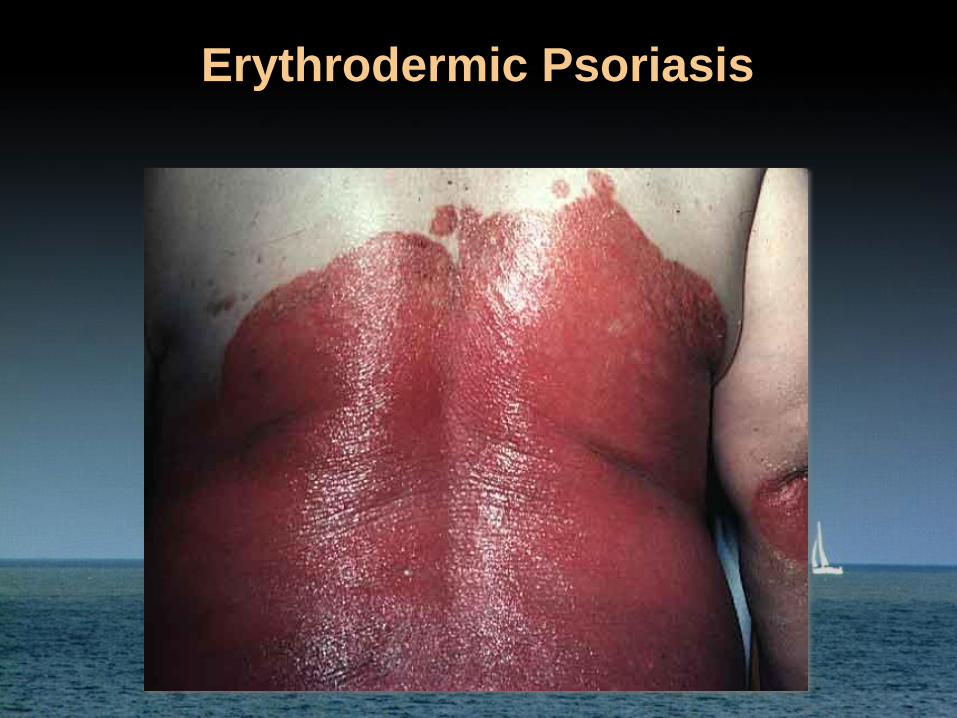
Erythrodermic Psoriasis

Don’t Forget to Check…
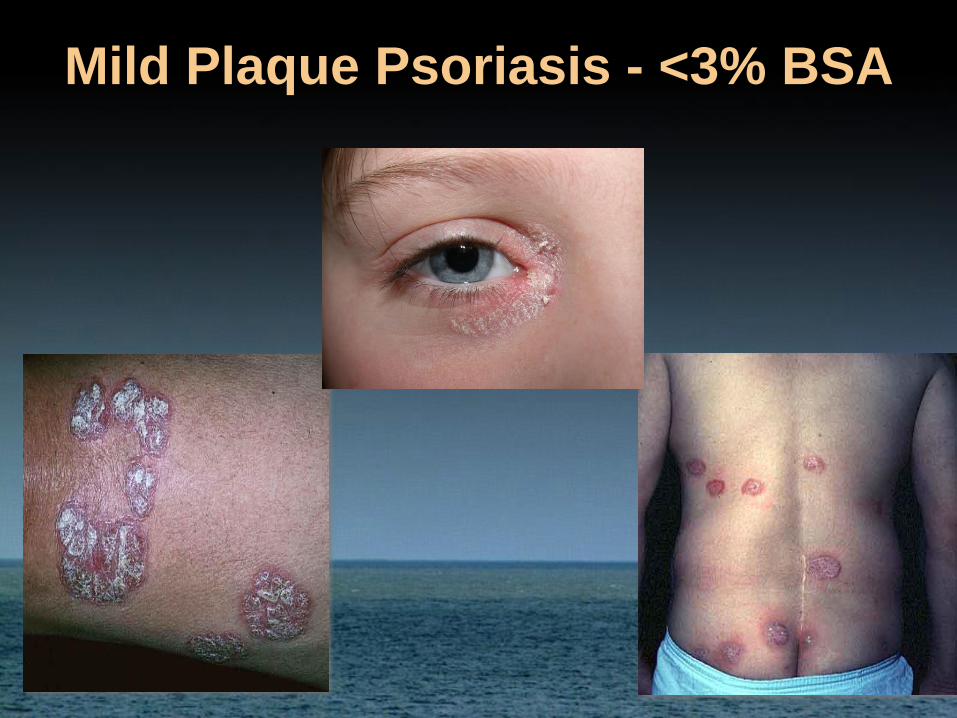
Mild Plaque Psoriasis - <3% BSA

Mod-Severe Plaque Psoriasis
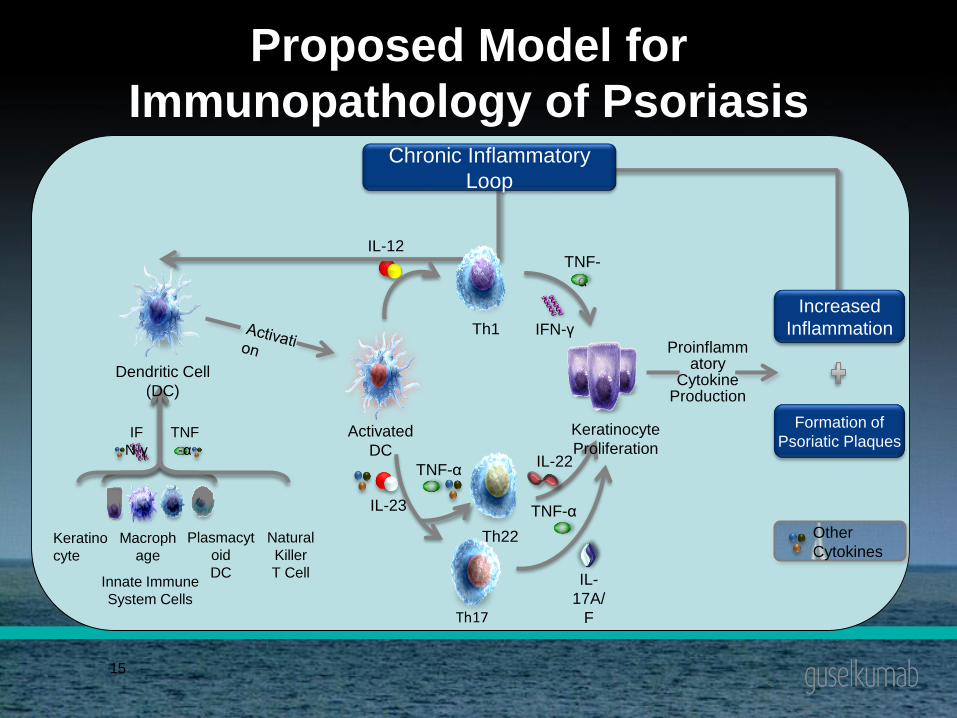
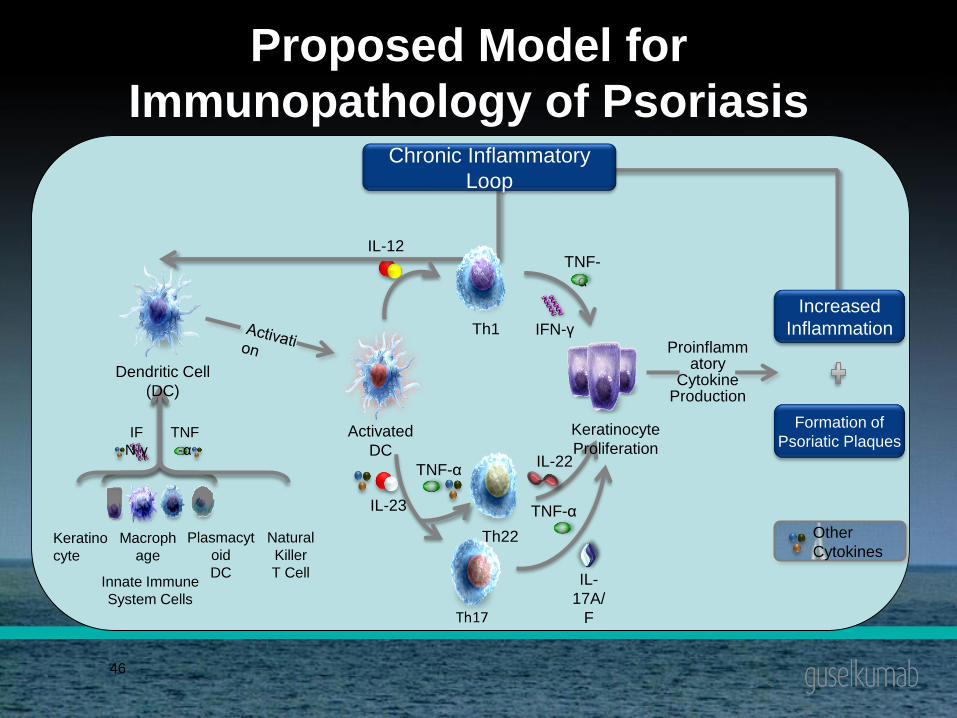
Proposed Model for
Immunopathology of Psoriasis
15
TNF-α
Keratino
cyte
Macroph
age
Plasmacyt
oid
DC
Natural
Killer
T Cell
Dendritic Cell
(DC)
IF
N-γ
TNF
-α
Th22
Chronic Inflammatory
Loop
Formation of
Psoriatic Plaques
Increased
Inflammation
Activated
DC
Th17
IL-22TNF-α
Th1
TNF-
α
IL-23
IL-12
Keratinocyte
Proliferation
Proinflammatory
Cytokine Production
IFN-γ
Other
Cytokines
Innate Immune
System Cells
IL-
17A/
F
Psoriasis - “The Tie that Binds”• Chronic state of systemic inflammation
• Co-morbidities now recognized
• Multi-system disease
• Multi-discipline approach
• Psychosocial burden, 1,2,3
• Reactive Depression • Higher suicidal ideation• Alcoholism
1Kimball et al. Am J Clin Dermatol 2005;6:383. 2Naldi et al. Br J Dermatol
1992;127:212. 3Mrowietz U et al. Arch Dermatol Res. 2006 Dec;298(7):309-
19.; photo from http://www.fitnessfanatic.org
Psycho-social Morbidity and Psoriasis
Mrowietz U et al. Arch Dermatol Res. 2006 Dec;298(7):309-19.
Psoriatic Arthritis
Psoriatic Arthritis 7-30%
Spondyloarthropathies
Psoriatic Arthritis
• 7-30% OF PsO PTS - Usually sero-negative
• Men and women affected equally1
• Disease onset between age 30-501
Psoriasis precedes PsA in 2/3
Usually by ~10yrs
• More than one-half of the patients with PsA may have evidence of erosions on x-rays4,5
• Up to 40% of the patients develop severe, erosive arthropathy4,5E
• Spondylitis & Enthesitis also seen
1Jiaravuthisan et al. J Am Acad Dermatol. 2007;57:1-27 2De jong et al. Dermatology. 1996;193(4):300-3033Van Laborde S, Scher RK. Dermatol Clin. 2000;18:37-46
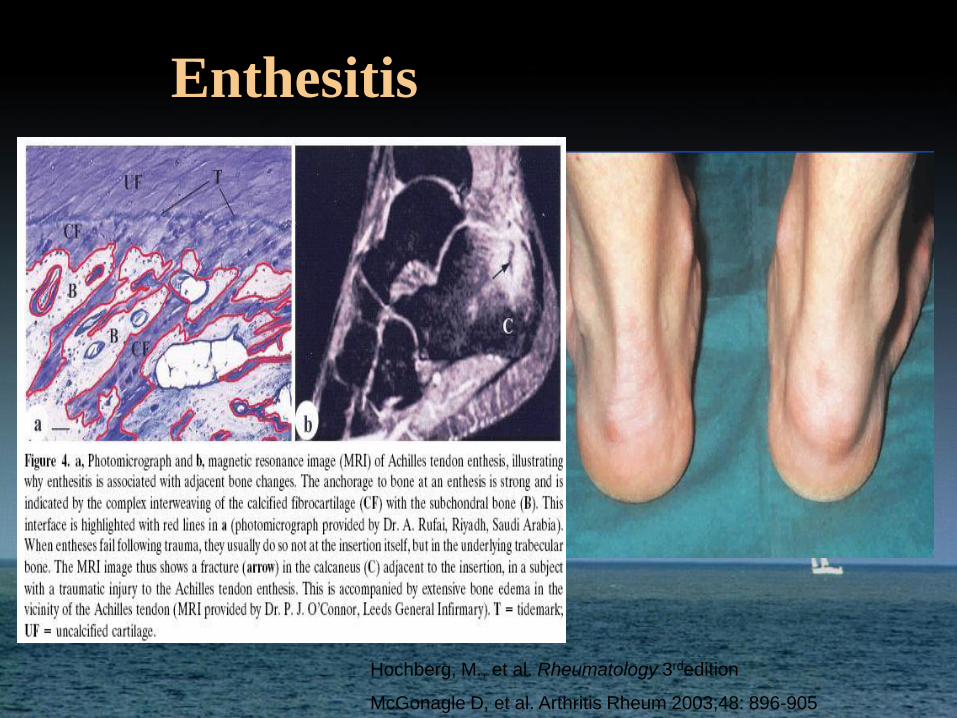
Enthesitis
Hochberg, M., et al. Rheumatology 3rdedition
McGonagle D, et al. Arthritis Rheum 2003;48: 896-905
Nail psoriasis 40-50%
Griffiths CE et al. Br J Dermatol. 2007;156(2):258-62.
Nail Psoriasis
Incidence of Nail Psoriasis in Patients
With Psoriasis
• 15%–50% of psoriasis patients have nail
involvement1
– Fingernails > Toenails
• Only 1%–5% in patients have nail involvement
without other cutaneous findings3
• Up to 85% of patients with PsA have nail
involvement
1Jiaravuthisan et al. J Am Acad Dermatol. 2007;57:1-272De jong et al. Dermatology. 1996;193(4):300-303
3Van Laborde S, Scher RK. Dermatol Clin. 2000;18:37-46
Nail Psoriasis Linked to…
• Positively associated with longer duration
and greater extent of skin disease1
• Higher incidence in PsA patients compared
with psoriasis alone2-4
• Severe disease is correlated to enthesitis,
polyarticular disease and unremitting and
progressive arthritis4
Nail pathology may provide a mechanistic link between skin disease
and joint disease in PsA3,4
1de Jong EM, et al. Dermatology. 1996;193(4):300-303; 2Jiaravuthisan MM, et al. J Am Acad Dermatol. 2007;
57:1-27; 3Williamson L, et al. Rheumatology. 2004;43:790-794; 4Lawry M. Dermatol Ther. 2007:20;60-67.
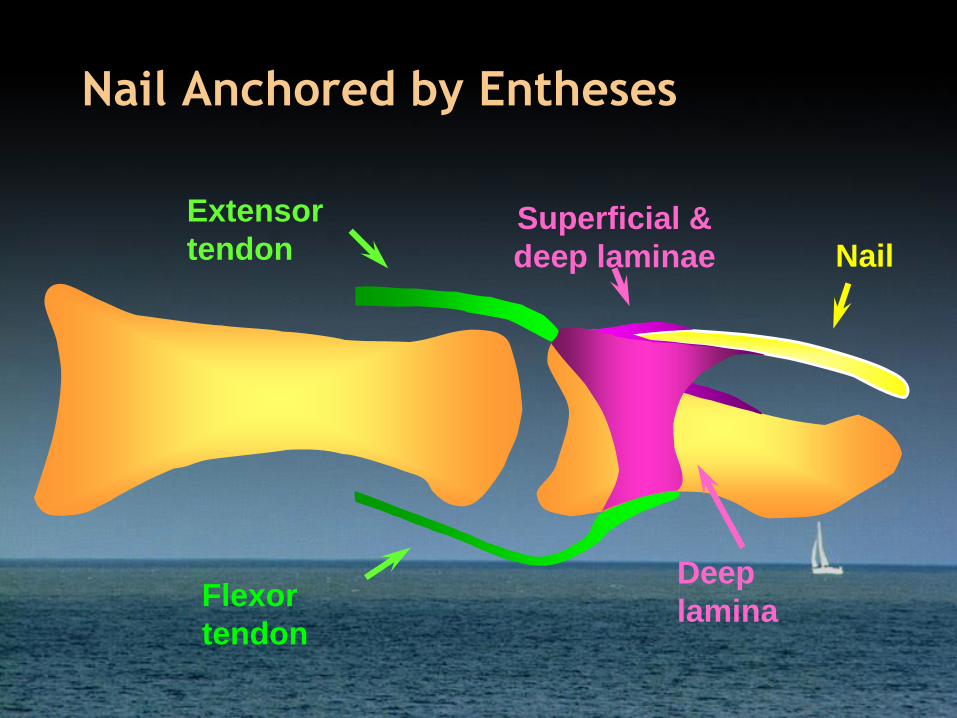
Nail Anchored by Entheses
Extensor
tendon
Flexor
tendon
Nail
Superficial &
deep laminae
Deep
lamina
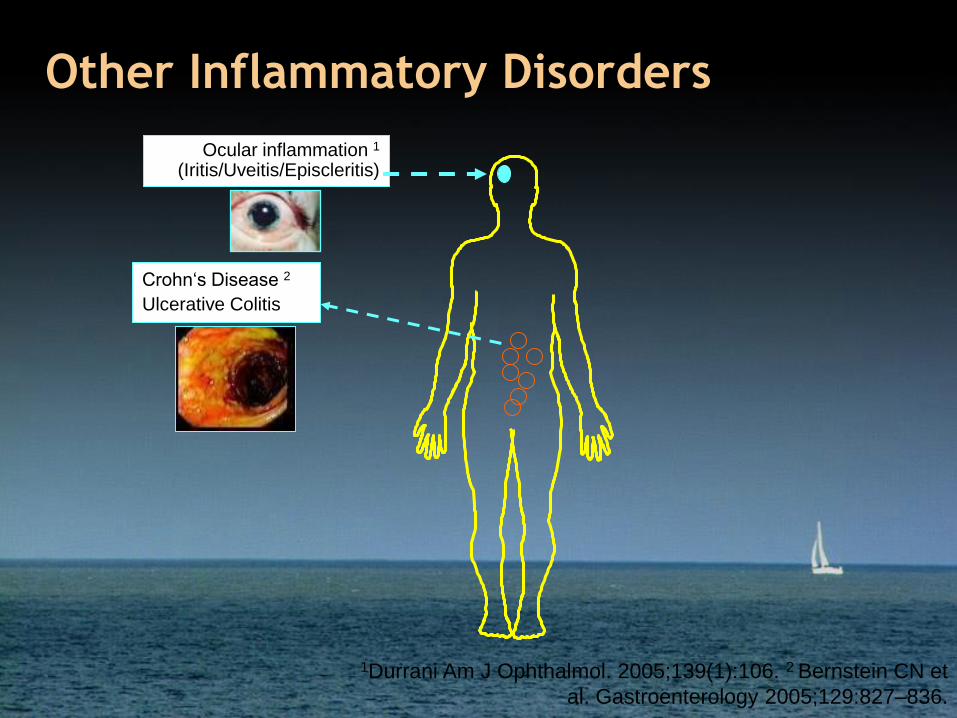
Ocular inflammation 1
(Iritis/Uveitis/Episcleritis)
Crohn‘s Disease 2
Ulcerative Colitis
1Durrani Am J Ophthalmol. 2005;139(1):106. 2 Bernstein CN et
al. Gastroenterology 2005;129:827–836.
Other Inflammatory Disorders
•The Prevalence Ratios (95% CIs) of Having IBD if a Person Has a
Diagnosis of Psoriasis
•Crohn’s disease = 1.52 (1.22–1.89)
•UC = 1.56 (1.24–1.95)
Bernstein Gastroenterology 2005;129:827–836
•Psoriasis occurs in 7-11% of the IBD population compared to 2-3%
of the general population
Tavarela et al. Aliment Pharmacol Ther. 2004;20 s4:50-3
Inflammatory Bowel Disease
•Ocular inflammation is a common feature of PsA occuring in
almost 30% PsA patients
•Conjunctivitis (20%)I
•Iritis occurring in 7% of the pts
Van de Kerkhof Textbook of Psoriasis 2nd ed. 2003 p.34
Iritis
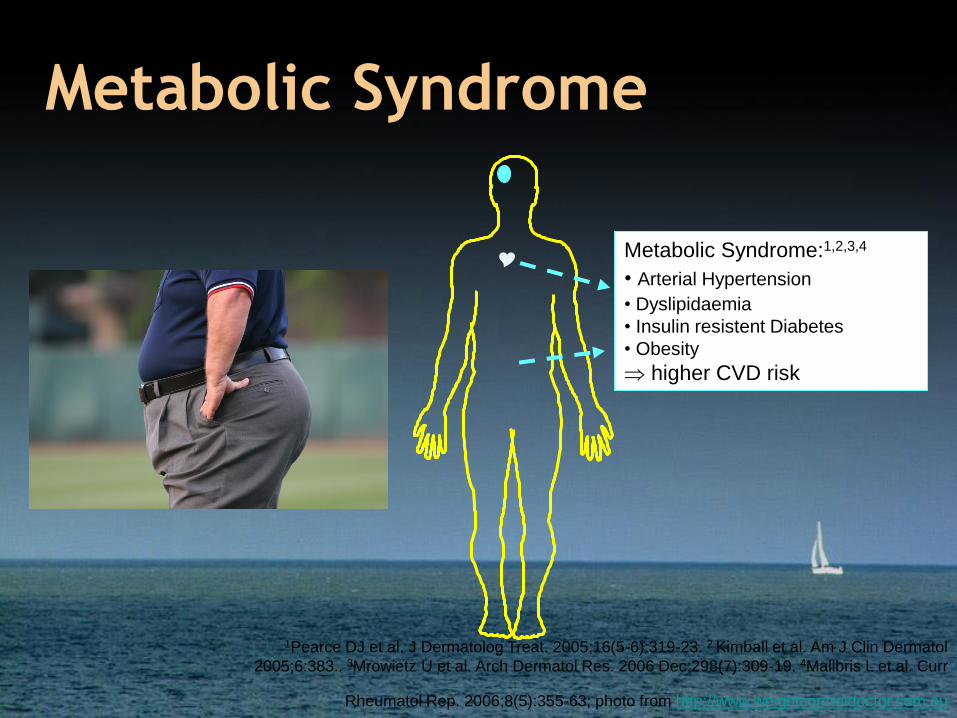
Metabolic Syndrome:1,2,3,4
• Arterial Hypertension
• Dyslipidaemia
• Insulin resistent Diabetes
• Obesity
higher CVD risk
1Pearce DJ et al. J Dermatolog Treat. 2005;16(5-6):319-23. 2 Kimball et al. Am J Clin Dermatol
2005;6:383.. 3Mrowietz U et al. Arch Dermatol Res. 2006 Dec;298(7):309-19. 4Mallbris L et al. Curr
Rheumatol Rep. 2006;8(5):355-63; photo from http://www.weightcontroldoctor.com.au
Metabolic Syndrome
•Respective prevalence rates of risk factors in those with severe
psoriasis, mild psoriasis, and in controls follows:
•Diabetes (7.1%, 4.4%, 3.3%)
•Hypertension (20%, 14.7%, 11.9%)
•Hyperlipidemia (6%, 4.7%, 3.3%)
•Obesity (20.7%, 15.8%, 13.2%)
•Smoking (30.1%, 28%, 21.3%)
•Neimann A et al. J Am Acad Dermatol 2006;55:829-35
Metabolic Syndrome
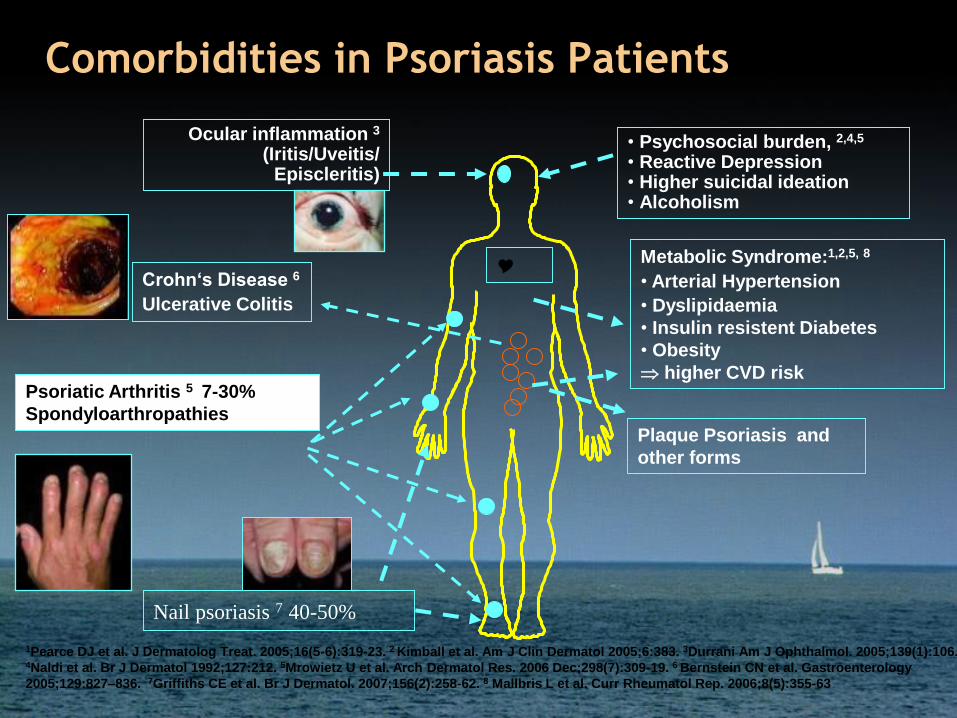
Plaque Psoriasis and
other forms
• Psychosocial burden, 2,4,5
• Reactive Depression • Higher suicidal ideation• Alcoholism
Metabolic Syndrome:1,2,5, 8
• Arterial Hypertension
• Dyslipidaemia
• Insulin resistent Diabetes
• Obesity
higher CVD risk
Nail psoriasis 7 40-50%
Ocular inflammation 3
(Iritis/Uveitis/ Episcleritis)
Crohn‘s Disease 6
Ulcerative Colitis
1Pearce DJ et al. J Dermatolog Treat. 2005;16(5-6):319-23. 2 Kimball et al. Am J Clin Dermatol 2005;6:383. 3Durrani Am J Ophthalmol. 2005;139(1):106. 4Naldi et al. Br J Dermatol 1992;127:212. 5Mrowietz U et al. Arch Dermatol Res. 2006 Dec;298(7):309-19. 6 Bernstein CN et al. Gastroenterology
2005;129:827–836. 7Griffiths CE et al. Br J Dermatol. 2007;156(2):258-62. 8 Mallbris L et al. Curr Rheumatol Rep. 2006;8(5):355-63
Comorbidities in Psoriasis Patients
Psoriatic Arthritis 5 7-30%
Spondyloarthropathies
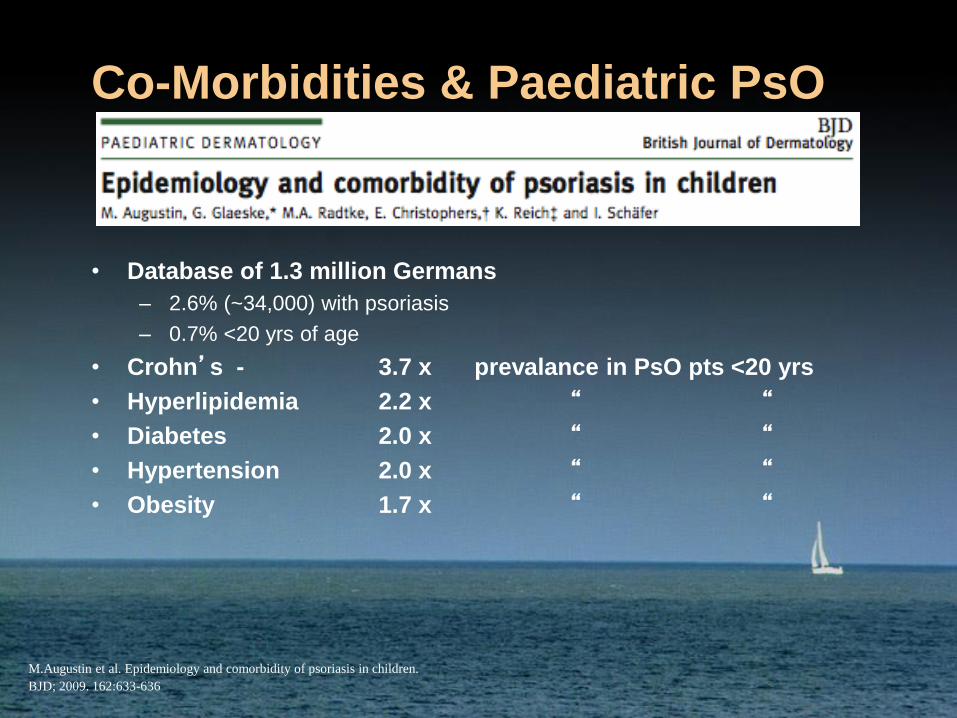
Co-Morbidities & Paediatric PsO
• Database of 1.3 million Germans
– 2.6% (~34,000) with psoriasis
– 0.7% <20 yrs of age
• Crohn’s - 3.7 x prevalance in PsO pts <20 yrs
• Hyperlipidemia 2.2 x “ “
• Diabetes 2.0 x “ “
• Hypertension 2.0 x “ “
• Obesity 1.7 x “ “
M.Augustin et al. Epidemiology and comorbidity of psoriasis in children.
BJD; 2009. 162:633-636
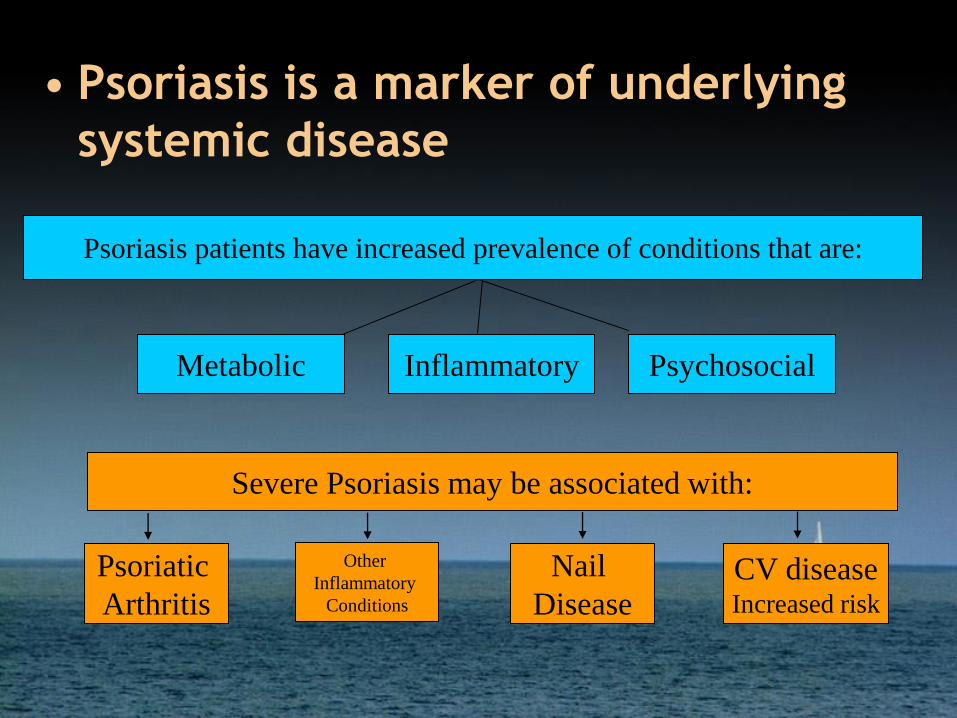
• Psoriasis is a marker of underlying
systemic disease
Psoriasis patients have increased prevalence of conditions that are:
Metabolic Inflammatory Psychosocial
Severe Psoriasis may be associated with:
Psoriatic
Arthritis
Other
Inflammatory
Conditions
Nail
DiseaseCV diseaseIncreased risk
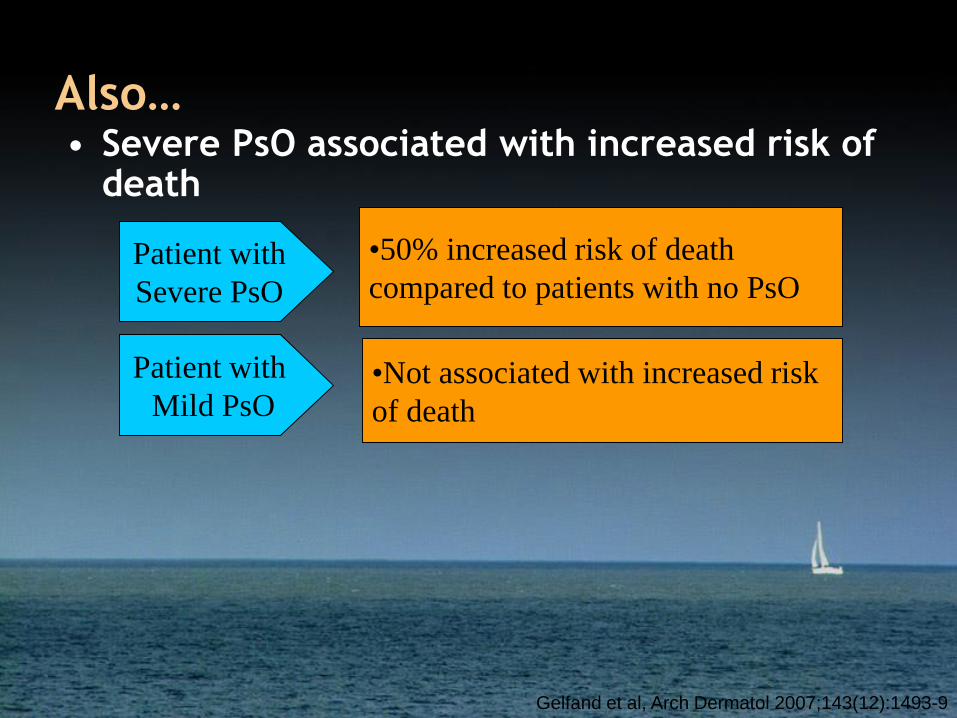
Also…• Severe PsO associated with increased risk of
death
Patient with
Severe PsO
Patient with
Mild PsO
•50% increased risk of death
compared to patients with no PsO
•Not associated with increased risk
of death
Gelfand et al, Arch Dermatol 2007;143(12):1493-9
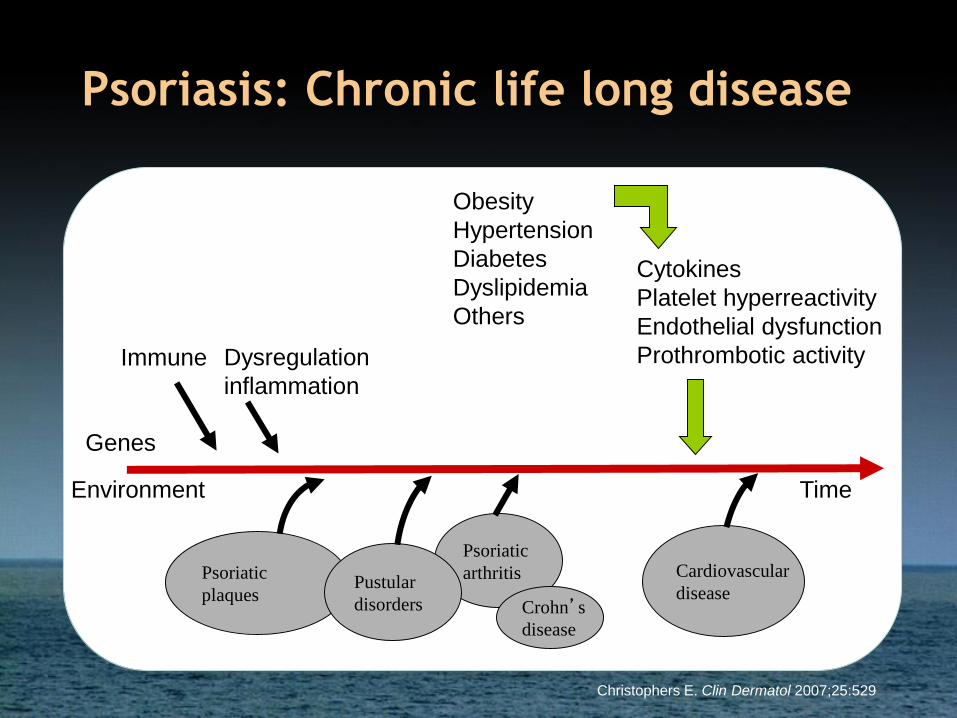
Psoriasis: Chronic life long disease
Christophers E. Clin Dermatol 2007;25:529
Genes
Environment
Immune Dysregulation
inflammation
Cytokines
Platelet hyperreactivity
Endothelial dysfunction
Prothrombotic activity
Obesity
Hypertension
Diabetes
Dyslipidemia
Others
Time
Psoriatic
plaques
Psoriatic
arthritis
Crohn’s
disease
Cardiovascular
diseasePustular
disorders
Psoriasis Treatment
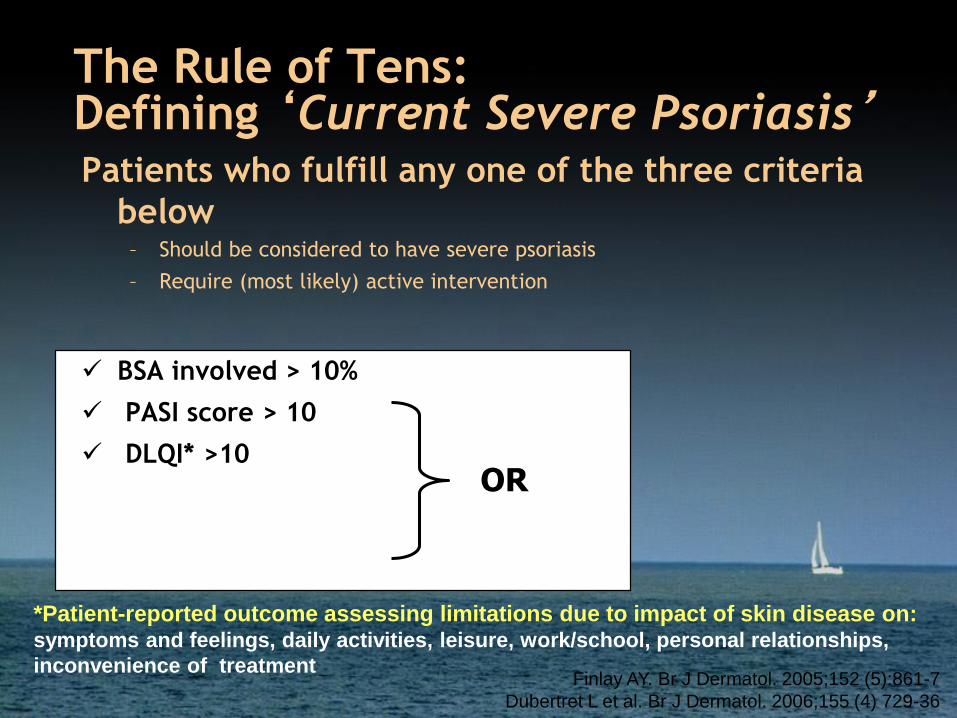
The Rule of Tens: Defining ‘Current Severe Psoriasis’Patients who fulfill any one of the three criteria
below – Should be considered to have severe psoriasis
– Require (most likely) active intervention
✓ BSA involved > 10%
✓ PASI score > 10
✓ DLQI* >10OR
Finlay AY. Br J Dermatol. 2005;152 (5):861-7
Dubertret L et al. Br J Dermatol. 2006;155 (4) 729-36
*Patient-reported outcome assessing limitations due to impact of skin disease on: symptoms and feelings, daily activities, leisure, work/school, personal relationships,
inconvenience of treatment
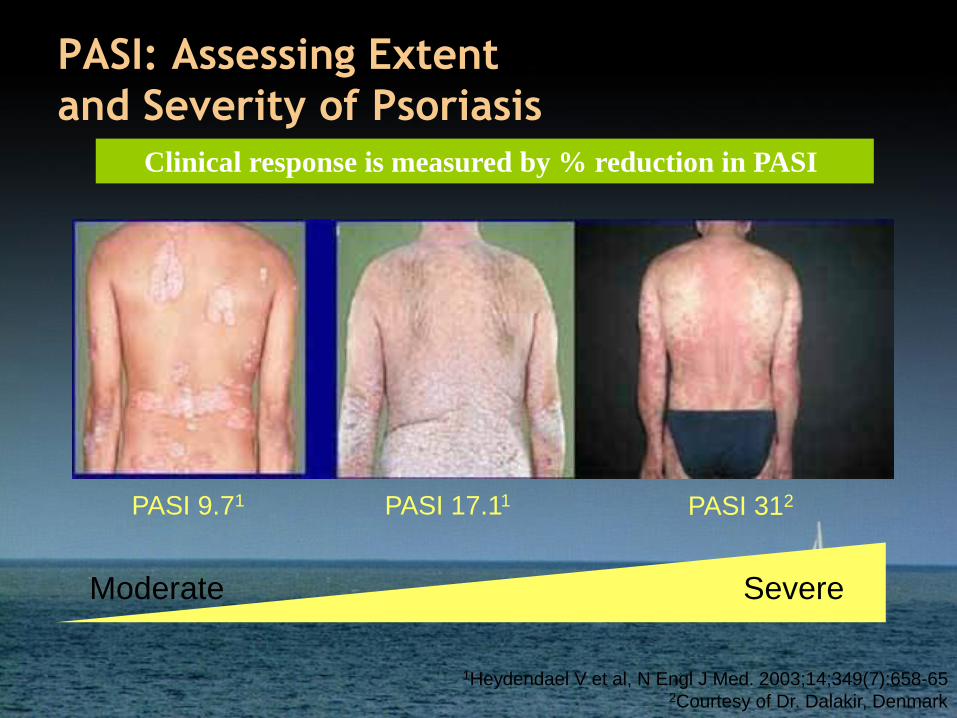
1Heydendael V et al, N Engl J Med. 2003;14;349(7):658-652Courtesy of Dr. Dalakir, Denmark
PASI 9.71 PASI 17.11 PASI 312
Severe
Clinical response is measured by % reduction in PASI
Moderate
PASI: Assessing Extent
and Severity of Psoriasis
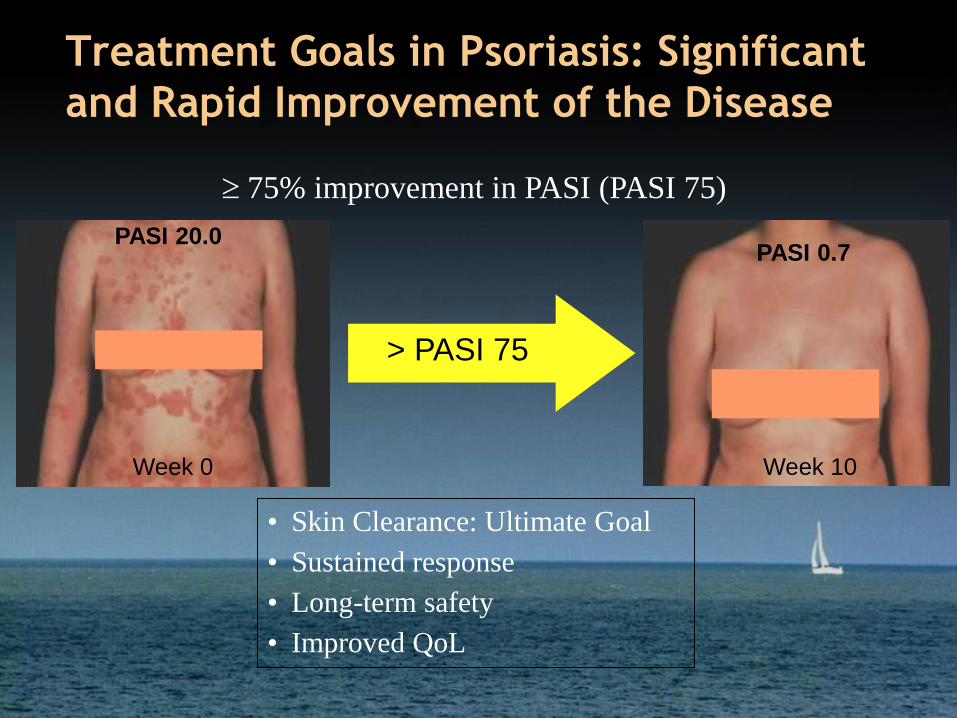
• Skin Clearance: Ultimate Goal
• Sustained response
• Long-term safety
• Improved QoL
75% improvement in PASI (PASI 75)
> PASI 75
PASI 20.0PASI 0.7
Week 0 Week 10
Treatment Goals in Psoriasis: Significant
and Rapid Improvement of the Disease
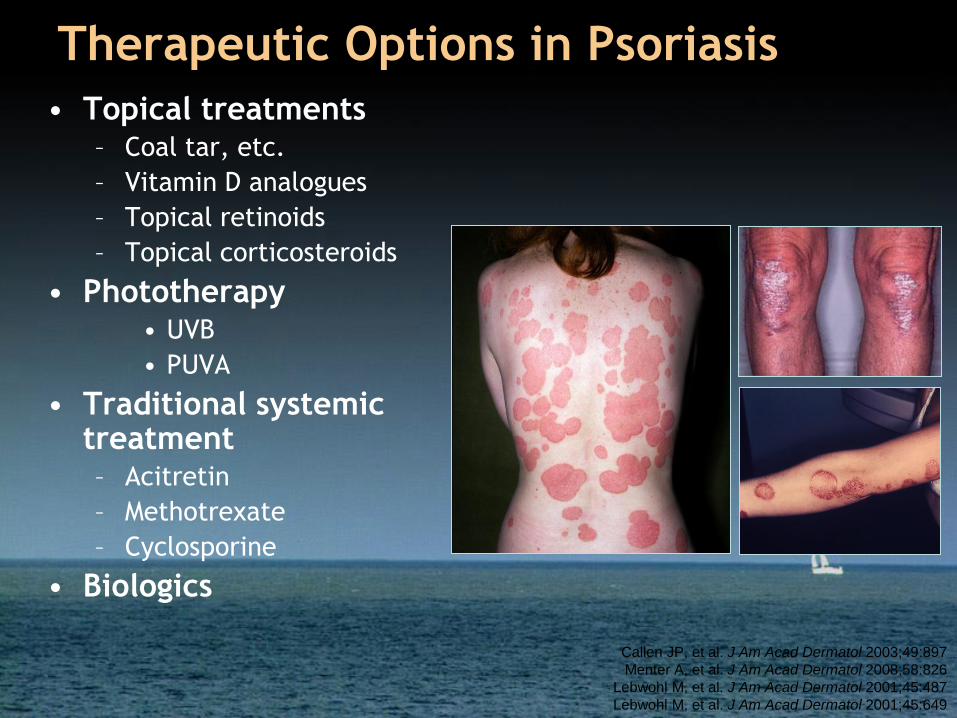
Therapeutic Options in Psoriasis
• Topical treatments– Coal tar, etc.
– Vitamin D analogues
– Topical retinoids
– Topical corticosteroids
• Phototherapy• UVB
• PUVA
• Traditional systemic treatment– Acitretin
– Methotrexate
– Cyclosporine
• Biologics
Callen JP, et al. J Am Acad Dermatol 2003;49:897
Menter A, et al. J Am Acad Dermatol 2008;58:826
Lebwohl M, et al. J Am Acad Dermatol 2001;45:487
Lebwohl M, et al. J Am Acad Dermatol 2001;45:649
• Oral Agents:• Acitretin
» Hard on liver and can elevate lipids.
» Works well in about 20-40% of patients
• Methotrexate» Hard on liver and can drop blood cells. Can affect
lungs.
» Works well in about 30-50% of patients.
• Cyclosporine» Hard on kidneys and causes increase blood pressure
and lipids. Increased risk of mailgnancy
» Works well in 60-80% of patients.
• Phototherapy: (Need to be close to light unit)• Either twice per week (PUVA) for 15+ weeks.
• Three times per week (nb & bbUVb) for 10+ weeks.
• Works well in 60-80% of patients.
• Biological Agents:• Injectables from twice weekly to every 3 months.
Systemic Treatment Options to
Patient:
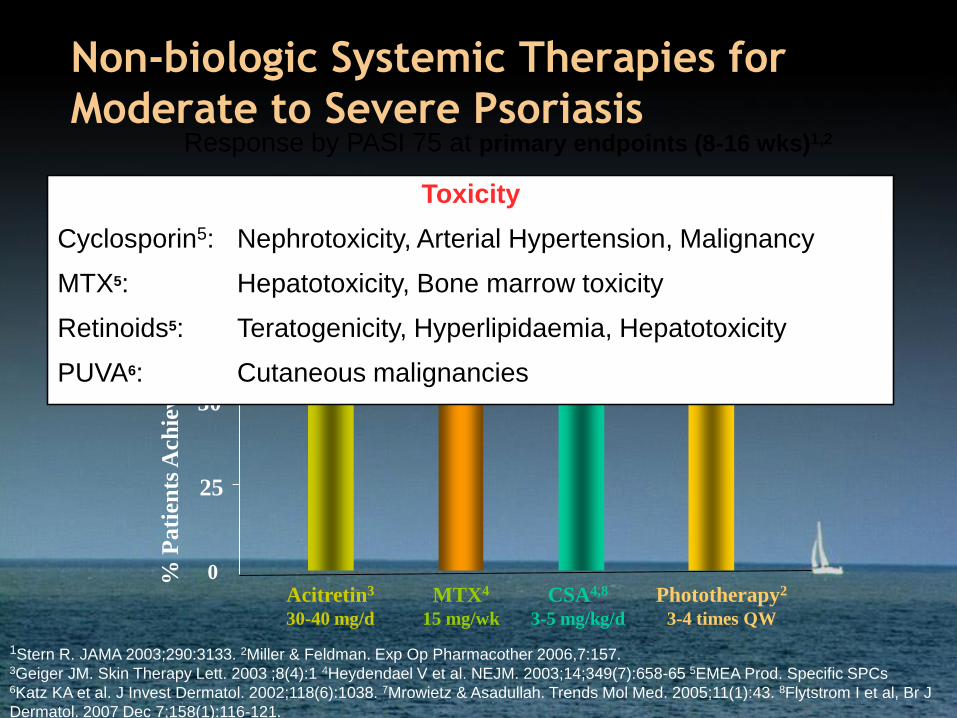
Non-biologic Systemic Therapies for
Moderate to Severe PsoriasisResponse by PASI 75 at primary endpoints (8-16 wks)1,2
No head to head trials%
Pati
ents
Ach
ievin
g P
AS
I 75
0
25
50
75
100
CSA4,8
3-5 mg/kg/d
Phototherapy2
3-4 times QW
MTX4
15 mg/wk
60
58-71
70-80
1Stern R. JAMA 2003;290:3133. 2Miller & Feldman. Exp Op Pharmacother 2006,7:157. 3Geiger JM. Skin Therapy Lett. 2003 ;8(4):1 4Heydendael V et al. NEJM. 2003;14;349(7):658-65 5EMEA Prod. Specific SPCs 6Katz KA et al. J Invest Dermatol. 2002;118(6):1038. 7Mrowietz & Asadullah. Trends Mol Med. 2005;11(1):43. 8Flytstrom I et al, Br J
Dermatol. 2007 Dec 7;158(1):116-121.
Acitretin3
30-40 mg/d
52
Toxicity
Cyclosporin5: Nephrotoxicity, Arterial Hypertension, Malignancy
MTX5: Hepatotoxicity, Bone marrow toxicity
Retinoids5: Teratogenicity, Hyperlipidaemia, Hepatotoxicity
PUVA6: Cutaneous malignancies
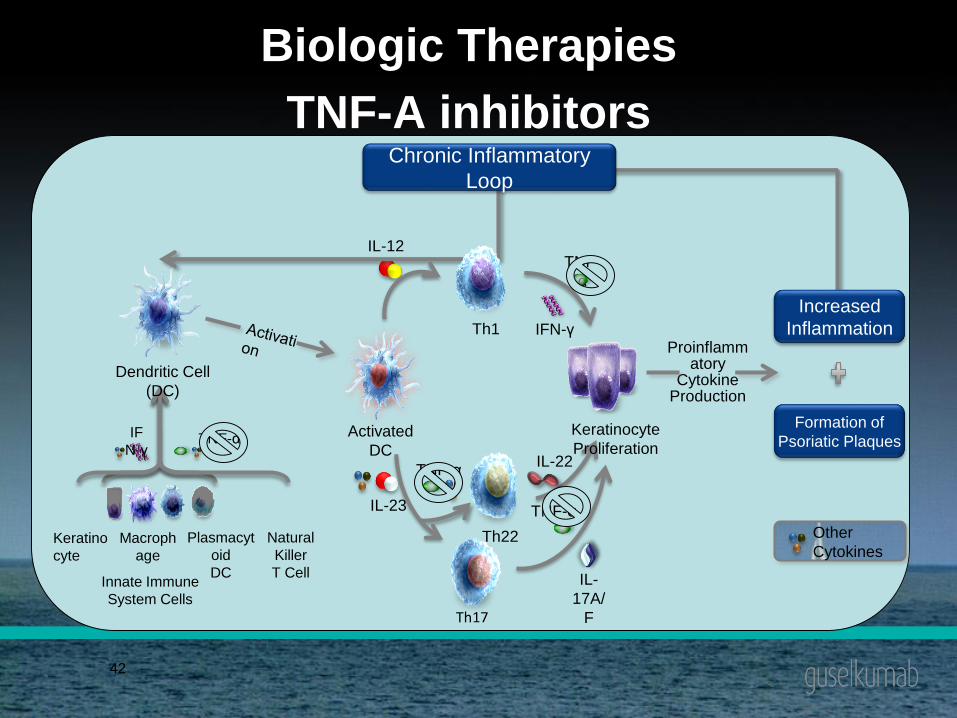
Biologic Therapies
TNF-A inhibitors
42
TNF-α
Keratino
cyte
Macroph
age
Plasmacyt
oid
DC
Natural
Killer
T Cell
Dendritic Cell
(DC)
IF
N-γTNF-α
Th22
Chronic Inflammatory
Loop
Formation of
Psoriatic Plaques
Increased
Inflammation
Activated
DC
Th17
IL-22TNF-α
Th1
TNF-
α
IL-23
IL-12
Keratinocyte
Proliferation
Proinflammatory
Cytokine Production
IFN-γ
Other
Cytokines
Innate Immune
System Cells
IL-
17A/
F
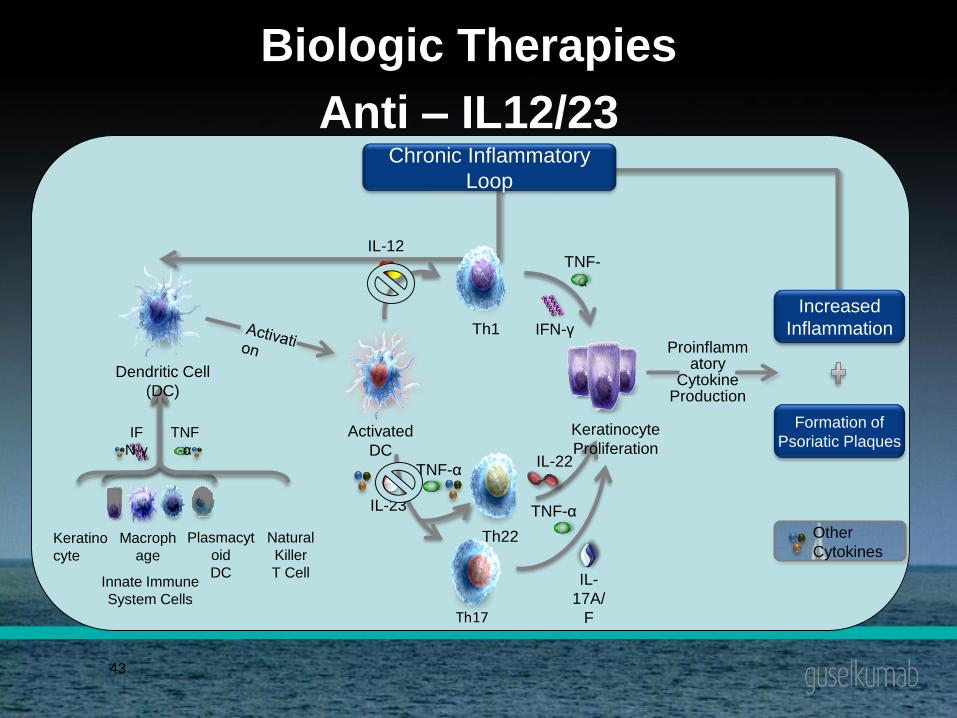
Biologic Therapies
Anti – IL12/23
43
TNF-α
Keratino
cyte
Macroph
age
Plasmacyt
oid
DC
Natural
Killer
T Cell
Dendritic Cell
(DC)
IF
N-γ
TNF
-α
Th22
Chronic Inflammatory
Loop
Formation of
Psoriatic Plaques
Increased
Inflammation
Activated
DC
Th17
IL-22TNF-α
Th1
TNF-
α
IL-23
IL-12
Keratinocyte
Proliferation
Proinflammatory
Cytokine Production
IFN-γ
Other
Cytokines
Innate Immune
System Cells
IL-
17A/
F
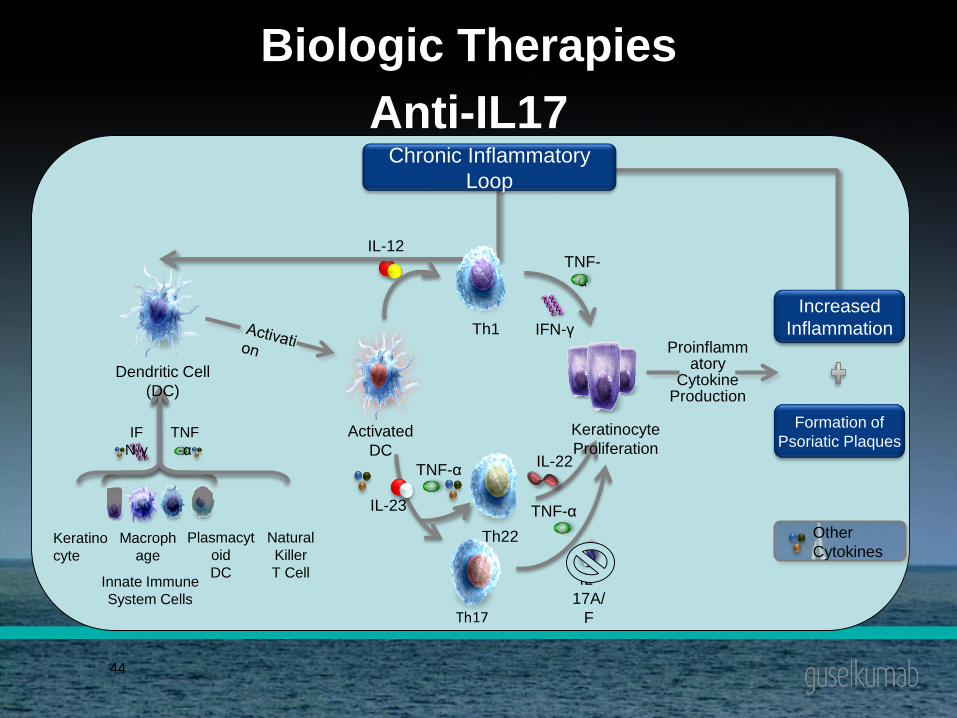
Biologic Therapies
Anti-IL17
44
TNF-α
Keratino
cyte
Macroph
age
Plasmacyt
oid
DC
Natural
Killer
T Cell
Dendritic Cell
(DC)
IF
N-γ
TNF
-α
Th22
Chronic Inflammatory
Loop
Formation of
Psoriatic Plaques
Increased
Inflammation
Activated
DC
Th17
IL-22TNF-α
Th1
TNF-
α
IL-23
IL-12
Keratinocyte
Proliferation
Proinflammatory
Cytokine Production
IFN-γ
Other
Cytokines
Innate Immune
System Cells
IL-
17A/
F
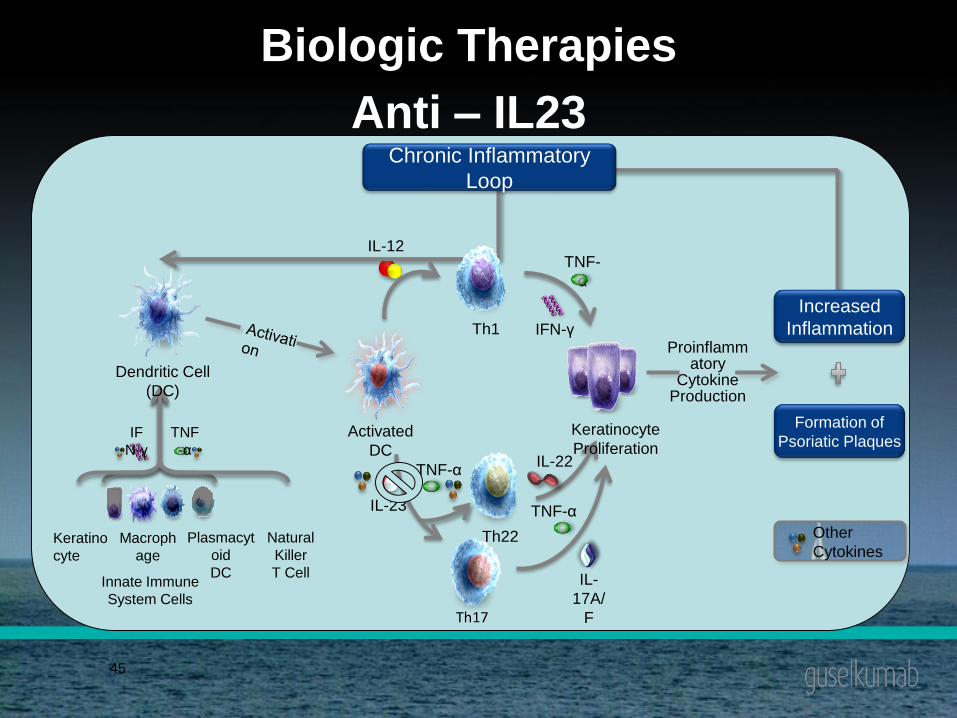
Biologic Therapies
Anti – IL23
45
TNF-α
Keratino
cyte
Macroph
age
Plasmacyt
oid
DC
Natural
Killer
T Cell
Dendritic Cell
(DC)
IF
N-γ
TNF
-α
Th22
Chronic Inflammatory
Loop
Formation of
Psoriatic Plaques
Increased
Inflammation
Activated
DC
Th17
IL-22TNF-α
Th1
TNF-
α
IL-23
IL-12
Keratinocyte
Proliferation
Proinflammatory
Cytokine Production
IFN-γ
Other
Cytokines
Innate Immune
System Cells
IL-
17A/
F
Proposed Model for
Immunopathology of Psoriasis
46
TNF-α
Keratino
cyte
Macroph
age
Plasmacyt
oid
DC
Natural
Killer
T Cell
Dendritic Cell
(DC)
IF
N-γ
TNF
-α
Th22
Chronic Inflammatory
Loop
Formation of
Psoriatic Plaques
Increased
Inflammation
Activated
DC
Th17
IL-22TNF-α
Th1
TNF-
α
IL-23
IL-12
Keratinocyte
Proliferation
Proinflammatory
Cytokine Production
IFN-γ
Other
Cytokines
Innate Immune
System Cells
IL-
17A/
F
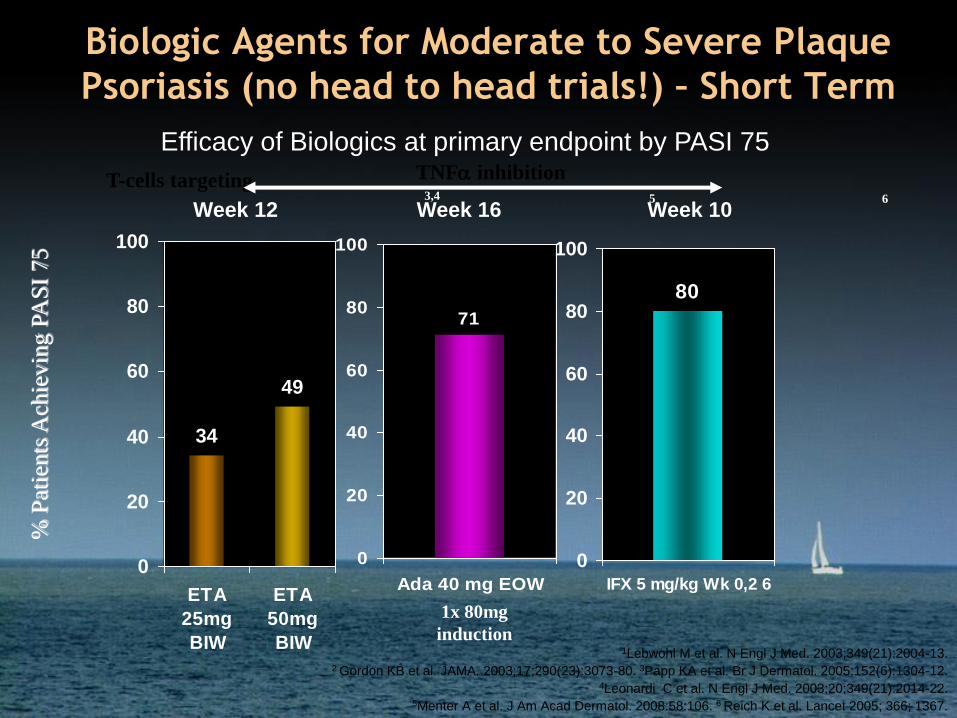
Biologic Agents for Moderate to Severe Plaque
Psoriasis (no head to head trials!) – Short Term
Efficacy of Biologics at primary endpoint by PASI 75
% P
atie
nts
Ach
ievin
g P
AS
I 75
1Lebwohl M et al. N Engl J Med. 2003;349(21):2004-13.2 Gordon KB et al. JAMA. 2003;17;290(23):3073-80. 3Papp KA et al. Br J Dermatol. 2005;152(6):1304-12.
4Leonardi C et al. N Engl J Med. 2003;20;349(21):2014-22. 5Menter A et al. J Am Acad Dermatol. 2008:58:106. 6 Reich K et al. Lancet 2005; 366; 1367.
T-cells targeting
34
49
0
20
40
60
80
100
ETA
25mg
BIW
ETA
50mg
BIW
Week 123,4
1x 80mg
induction
71
0
20
40
60
80
100
Ada 40 mg EOW
Week 165
80
0
20
40
60
80
100
IFX 5 mg/kg Wk 0,2 6
TNFa inhibition
Week 106
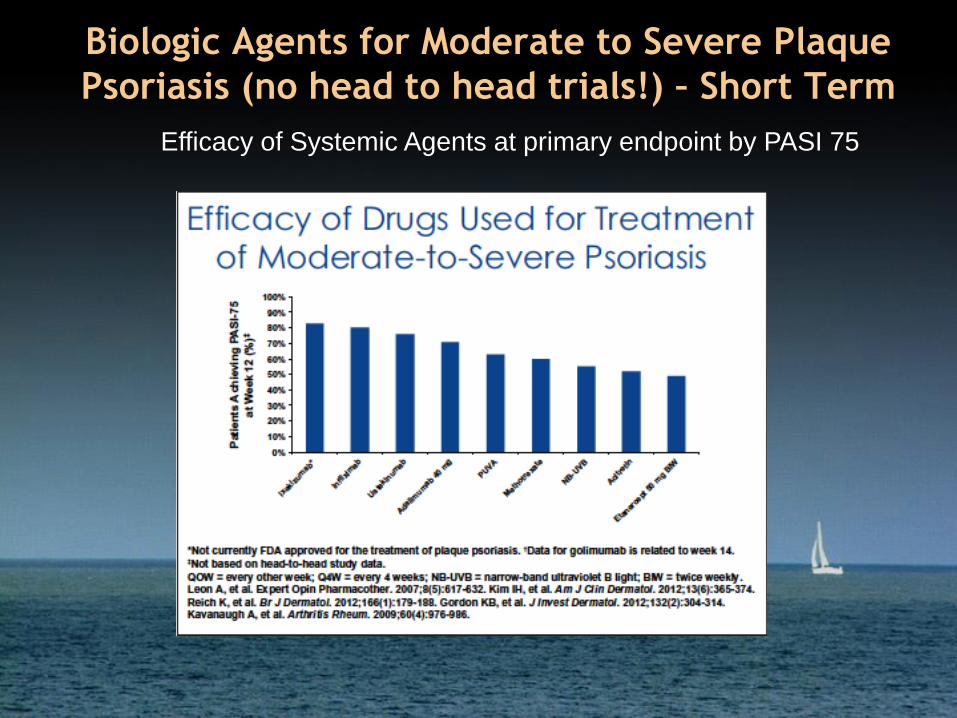
Biologic Agents for Moderate to Severe Plaque
Psoriasis (no head to head trials!) – Short Term
Efficacy of Systemic Agents at primary endpoint by PASI 75
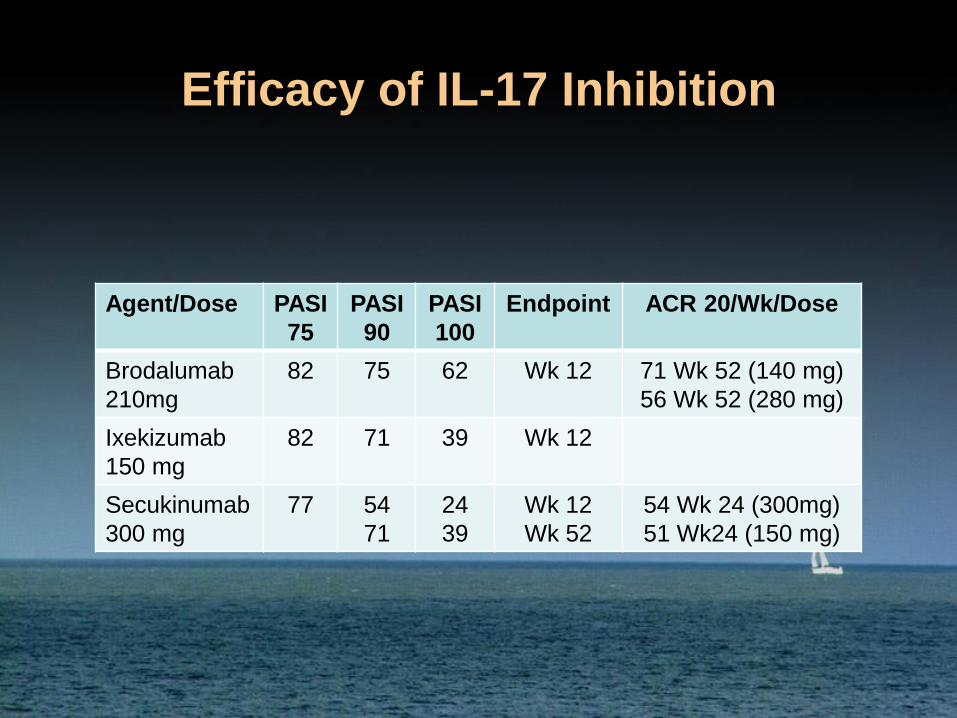
Efficacy of IL-17 Inhibition
Agent/Dose PASI
75
PASI
90
PASI
100
Endpoint ACR 20/Wk/Dose
Brodalumab
210mg
82 75 62 Wk 12 71 Wk 52 (140 mg)
56 Wk 52 (280 mg)
Ixekizumab
150 mg
82 71 39 Wk 12
Secukinumab
300 mg
77 54
71
24
39
Wk 12
Wk 52
54 Wk 24 (300mg)
51 Wk24 (150 mg)
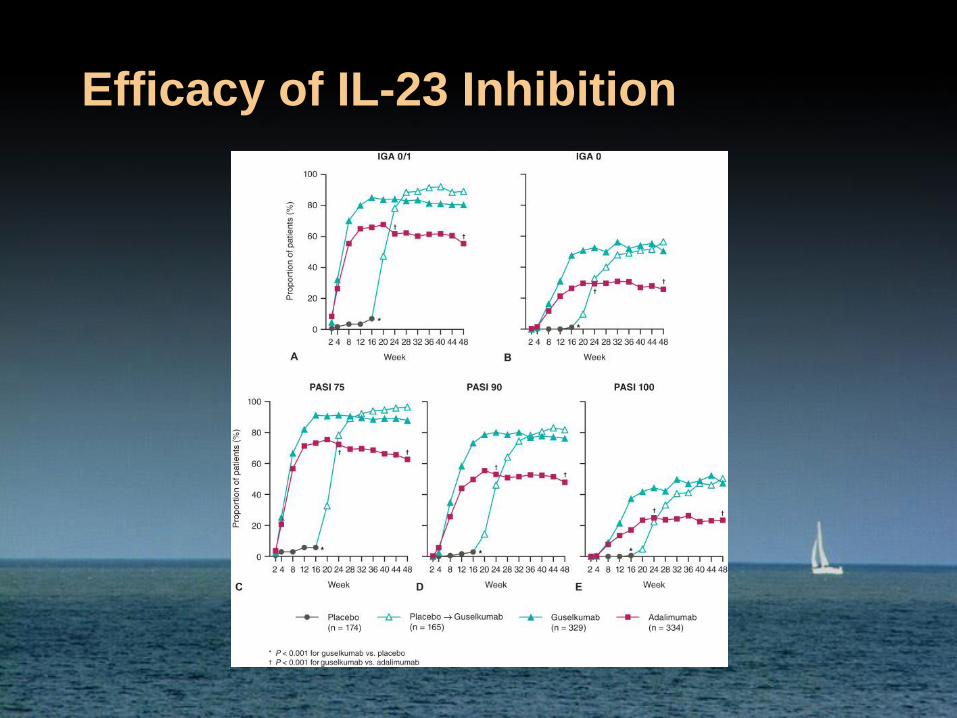
Efficacy of IL-23 Inhibition
Apremilast (Otezla) PDE4 Inhibitor
• 30 mg PO BID 29% achieved PASI 75 at 16 wks
• Approved for PsO and PsA
• No lab monitoring
• Diarrhea & Depression reported
Psoriasis Conclusions
• Chronic, immune-mediated inflammatory disease
of the skin1
• Associated with numerous co-morbidities
• Initiate treatment that effectively clears the
patient’s skin and observe for co-morbidities
• Choose treatment effective against psoriasis and
co-morbidities
• Evaluate and monitor skin & co-morbidities in
concert with medical colleagues

Thank You!!