province-wide contract for infant formula: one step closer to baby friendly designation april 17,...
TRANSCRIPT
Province-Wide Contract for Infant Formula: One Step Closer to Baby Friendly DesignationApril 17, 2015
Kim Williams, RN, MSN
Provincial Executive Director
Perinatal Services BC

2
Objectives
Participants will: • understand the provincial commitment to the
WHO Code for Marketing of Breast Milk Substitutes;
• learn how this is only part of the process to becoming Baby-Friendly;
• learn about the process that led to the province-wide infant formula contract; and
• discuss the implications for local site implementation.
3
Our Province
• ~ 45,000 births/year• 5 regional health authorities + BC Women’s• First Nations Health Authority• 54 sites with planned maternity services• Range from 10 to 6,700+ births/year• 13 NICUs (4 Level 3 and 9 Level 2)• 225 registered midwives• Increasing numbers of nurse practitioners

4
Births by Facility

5
6
7
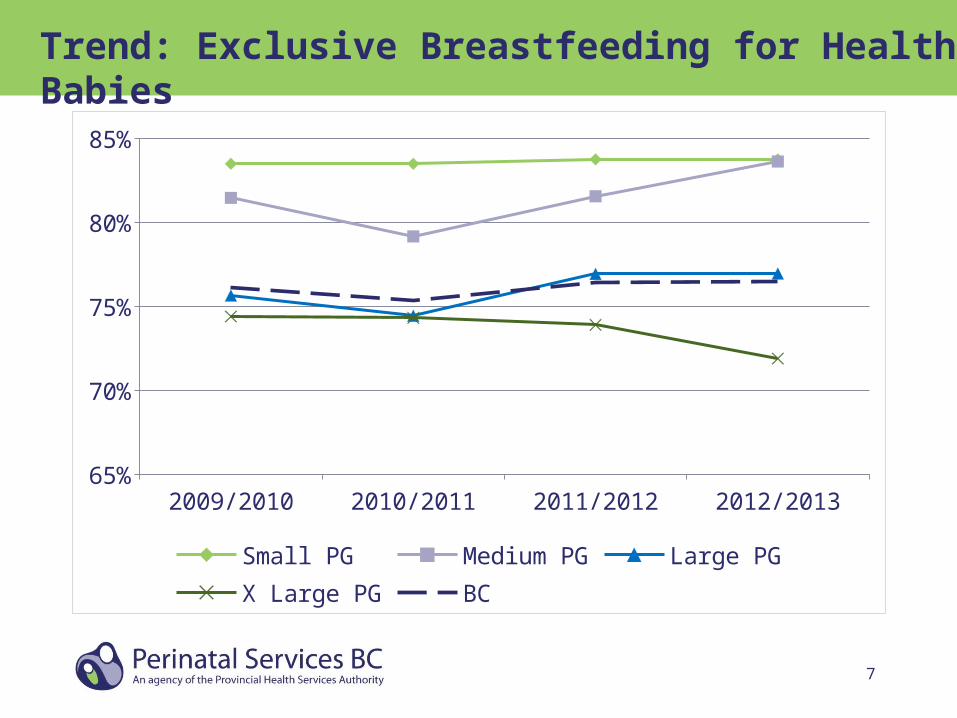
Trend: Exclusive Breastfeeding for Healthy Babies
2009/2010 2010/2011 2011/2012 2012/201365%
70%
75%
80%
85%
Small PG Medium PG Large PGX Large PG BC

8
Process
October 2012 – Perinatal Services BC Oversight Council endorsed the following statement:
The Baby Friendly Initiative (BFI) is recognized as the minimum standard for the commitment to promotion and protection of breastfeeding for all of British Columbia.
9
WHO International Code of Marketing of Breast Milk Substitutes
To be accredited as ‘baby-friendly’, a hospital is required to:
• avoid all promotion of breast-milk substitutes and related products, bottles, and teats;
• not accept free or low-cost supplies or give out samples of those products;
• infant formula needed for infants with medical reasons for its use should be obtained through normal procurement channels.

10
Adhering to the WHO International Code does not imply Baby-Friendly status.
It is only one of the steps required.

11
Getting Started
Spring 2013 – Perinatal Services BC was asked by the Perinatal Services BC Oversight Council to lead the coordination of working with HSSBC to negotiate a province-wide contract for infant formula that was in accordance with BFI and the WHO International Code of Marketing of Breast Milk Substitutes.
12
Collaboration
• A working group from the five regional health authorities in BC was convened
• Consisted of dietitians, nurses, and physicians • Reviewed the literature relevant to infant
formula indications of use• Established clinical specifications for each
formula subcategory

13
Governing Principles
• Recognition that breast milk and breastfeeding is the preferred food for infants.
• Infant formula should be used only when medically necessary and when all options to feed an infant mom’s own breast milk or pasteurized donor breast milk has been fully explored.
14
Working Group Mandate
• Evaluate the subcategories of infant formula based on current research to support the usage in a hospital and community setting
• Review the nutrient compositions of infant formula products available in Canada
• Establish clinical specifications required for each particular formula subcategory
• Engage key stakeholders from each health authority to provide feedback and review proposed clinical specifications

15
Clinical Specifications Subworking Groups• Term Infant Formula• Premature Infant Formula• Therapeutic Formula• Specialized Products• Feeding Related Supplies
16
Clinical Specifications Working Groups• Review current literature for the formula
categories • Grade literature (level of evidence)• Update products available and nutrient
information on compendium• Establish clinical specifications (up to five
general criteria of the critical factors that we feel the product must achieve)
• Share literature review summaries and updated nutrient information compendium

17
Gaining HA Support
March 2014 – Letter requesting endorsement in principle to proceed with the Request for Qualifications (RFQ) was sent to all health authority senior leadership
May 2014 – Issued to the market
August 2014 – Working group reviewed responses to RFQ and endorsed moving forward with one vendor as main supplier with secondary vendor providing product not available through the primary vendor.

18
Vendor Agreement
August 2014 – Preferred vendor was selected
February 2015 – Contract for all health authorities signed
19
Patient-Centred Care
• By purchasing human milk substitute that meets clinical specifications, infants will be provided with the best product to meet their specific clinical need when they cannot receive human milk
• By following the WHO code, health authorities can work towards obtaining Baby-Friendly status, which supports optimal infant nutrition
20
Financial Impact
• Historically, some health authorities were receiving formula at no cost while others were paying (depending on the product and movement towards Baby-Friendly Initiative).
• Some health authorities will see cost savings while others will see added costs as they had been obtaining free or below market cost products or other value add grants in the past.
• By coordinating provincial purchasing power and signing with one primary vendor, we will collectively save money.

21
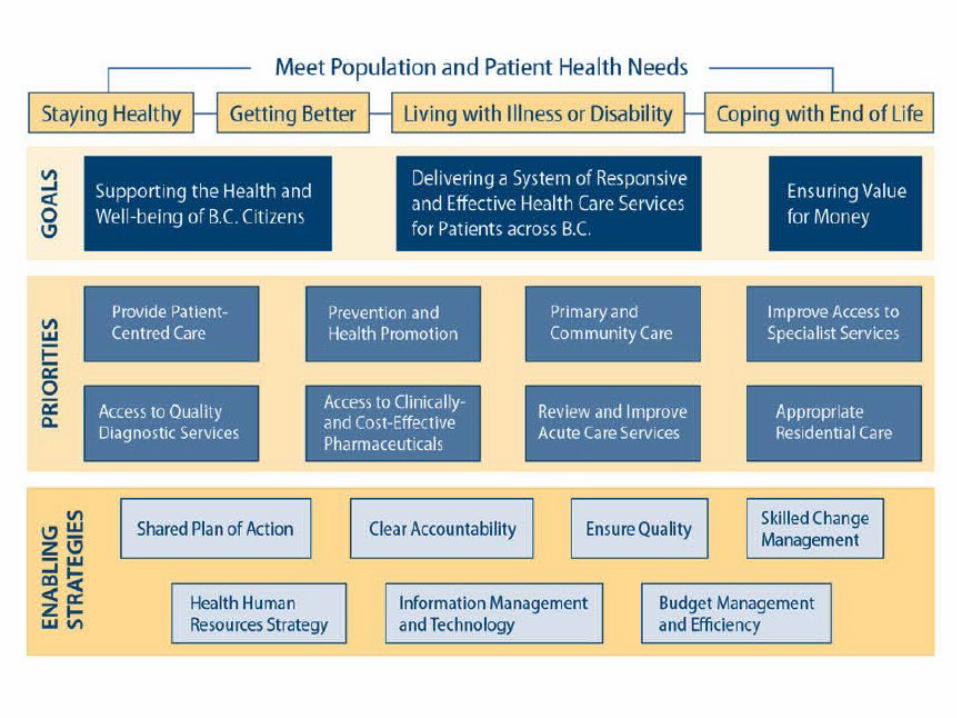
Ministry of Health Priorities
• This collective purchasing strategy supports Ministry of Health strategic goals, including priority of patient-centred care and enabling strategies of ensuring quality and budget management and efficiency.
• Moving to single primary vendor through a province-wide contract will save up to approximately $61,000/year.
22
What Worked well
• Representation from each health authority public health and acute care was key.
• Dietitians embraced this challenge and it worked well to have a champion for each product or group of products based on clinical expertise.
• Support and commitment from senior leadership
23
Lessons Learned
• Obtain broader input and feedback into clinical specifications
• Include an appendix for review process, who contributed feedback and how it was incorporated/or not into the clinical specs
• Separate out feeding supplies from the infant formula contract.
• Have the product standardization groups (across HA) participate in the clinical specs for formula working group.
• Have the product standardization groups (across HA) lead the development of clinical specs feeding related supplies.
24
Lessons Learned
• Consider a standard response form to collate the feedback and share the feedback as an appendix of the clinical specs document.
• Consider the composition of the RFQ development team to include a clinical representative and business/ operations lead from each health authority.
• Ensure that contract team members work closely with the clinical leads to ensure best practice is followed
25
Next Steps
• Each health authority will determine the phasing in of contract deliverables that is best suited to its BFI implementation strategy
• Transition to new products occurring over the next few months
Questions?
