prophylactic mesh for prevention of parastomal hernia: a · pdf file ·...
TRANSCRIPT

Prophylactic Mesh for prevention of
Parastomal Hernia A Meta-analysis
of Randomized Controlled Trials
Patel SV Zhang L Chadi SA Wexner S
Presenter Sunil Patel
July 6 2016
ACPGBI Annual Meeting
Declaration
bull The authors have no applicable conflicts of interests or financial declarations
Parastomal Hernia
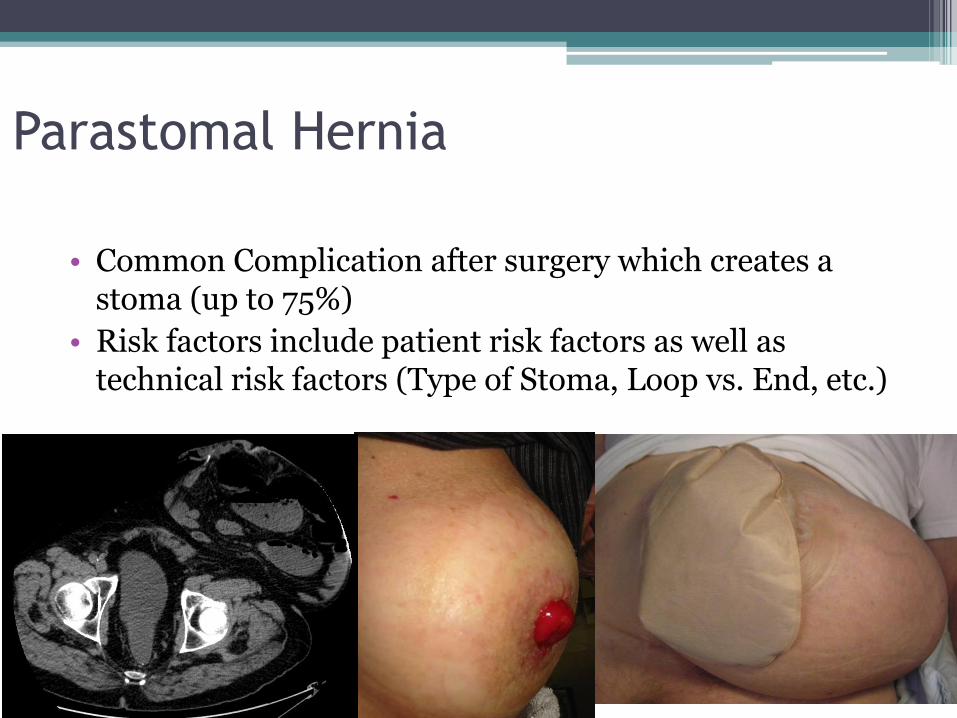
bull Common Complication after surgery which creates a stoma (up to 75)
bull Risk factors include patient risk factors as well as technical risk factors (Type of Stoma Loop vs End etc)
Prophylactic Mesh Placement
Definitionbull The placement of mesh at the index operation to
prevent parastomal hernia
bull Multiple mesh placements and techniques described Onlay vs Sublay vs Preperitoneal Keyhole vs Sugar Baker Biologic vs Synthetic Mesh
bull Opponents of Prophylactic Mesh are concerned with mesh infection erosion fistula and other stoma related complications
Prevention of Parastomal Hernia
bull An older meta-analysis (3 RCT N = 128) showed a reduction in parastomal hernia with the use of prophylactic mesh [1]
bull Several RCTrsquos have been published recently which were not included in this review
1 Shabbir et al Colorectal Dis 2012
Objective
bull To perform an updated meta-analysis to determine the efficacy of prophylactic mesh in patients requiring a temporary or permanent stoma
Inclusion Criteria
bull Randomized Controlled trials comparing the prophylactic placement of mesh vs no mesh
bull Any type of stoma
bull Any type of mesh (biologic vs synthetic) or position (onlay sublay preperitoneal etc)
bull At least 12 months of follow up
Outcomes
Primary Outcome
bull Development of parastomal hernia diagnosed clinically or radiographically
Secondary Outcomes
bull Parastomal hernia requiring subsequent surgical repair
bull Perioperative Complications
bull Stoma Specific Complications
Information Sources amp Search Strategy
bull EMBASE (1947 ndash 2015) MEDLINE (1946 ndash2015) (Searched Oct 1 2015 and January 4 2016)
bull Included English and non-English language publications
Study Selection amp Data Collection
bull Title Abstract and Full text review were undertaken independently and in duplicate to determine eligibility for inclusion
bull Data was collected using a standardized form and in duplicate
Study Quality Assessment
bull Risk of bias was assessed as per the Cochrane Handbook
Randomization
Allocation Concealment
Blinding
Attrition Bias (Loss to Follow Up)
Selective Reporting
Other bias
Data Analysis
bull Statistical Analysis completed in REVMAN using a random effects model
bull A Priori Subgroup Analyses
Biologic vs Synthetic Permanent Mesh
Hernia Diagnosis technique (Clinical vs Radiographic)
Mesh Location
Search Results
bull 107 Results screened
bull 7 RCTrsquos fit our inclusion criteria
An additional study was identified which published the 5 year follow up of an included study
N = 20 ndash 113
Follow up 12 ndash 60 months
Study Characteristics
Pathology Malignant Only ndash4 Studies
Benign amp Malignant ndash3 Studies
Type Of Stoma Colostomy Only ndash5 Studies
Colostomy amp Ileostomy ndash 2 Studies
Permanent Stomas ndash6 Studies
Permanent amp Temporary ndash1 Study
Type of Mesh Synthetic Light Weight ndash 5 Studies
Biologic Mesh ndash2 Studies
Diagnosis Clinical Exam ndash3 Studies
Routine Radiologic Exam ndash5 Studies
Risk of Bias
bull 2 Studies with low risk of bias across all assessed categories
bull 2 Studies with unclear risk of bias Unclear allocation concealment Unclear if assessors were blinded
bull 3 Studies had high risk of bias in at least one category High loss to follow up (35) Per Protocol Analysis (Not ITT) Changed Diagnostic Criteria partway through the
study
Parastomal Hernia
bull Reduced Odds with Prophylactic Mesh
OR 022 95CI 009 ndash 049 I2 = 49
Parastomal Hernia requiring
subsequent surgerybull Reduced odds with Prophylactic Mesh
OR 031 95CI 011 ndash 086 I2 = 0
Surgical Complications (All)
bull No difference in overall complications (P = 023)
Stoma Specific Complications
bull No difference in stoma specific complications (P = 024)
Subgroup Analyses (Hernia Formation)bull No subgroup effect of mesh position (P = 093)
bull No subgroup effect noted based on how hernia was diagnosed (P = 085)
Subgroup Analysisbull A significant subgroup effect was found based on
biologic vs synthetic permanent mesh (P = 002)
Discussion
bull Prophylactic Mesh associated with
A decrease in parastomal hernia after at least 1 year of follow up (Primary Outcome)
A decrease in subsequent surgical repair (Secondary Outcome)
bull Not associated with
Surgical or Stoma Specific Complications
Limitations
bull Heterogeneity
Primary outcome showed moderate heterogeneity (I2 = 49)
Reduced with Subgroup analysis based on biologic vs synthetic mesh (I2 = 15)
Limitations
bull Inconsistent complication Rates
Overall Complications Between 0 - gt90
Stoma Specific Complications Between 0 -gt50
bull Widely varying definitions of complications
Vs ldquoComplicationsrdquo
Conclusions
bull Placement of prophylactic mesh at the time of index surgery
Decreased odds of developing a parastomal hernia
Decreased odds of requiring subsequent surgical repair of hernia
Not associated with increased odds of complications or stoma specific complications
Questions
patels2kghkarinet
epipatelmd
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018
Declaration
bull The authors have no applicable conflicts of interests or financial declarations
Parastomal Hernia
bull Common Complication after surgery which creates a stoma (up to 75)
bull Risk factors include patient risk factors as well as technical risk factors (Type of Stoma Loop vs End etc)
Prophylactic Mesh Placement
Definitionbull The placement of mesh at the index operation to
prevent parastomal hernia
bull Multiple mesh placements and techniques described Onlay vs Sublay vs Preperitoneal Keyhole vs Sugar Baker Biologic vs Synthetic Mesh
bull Opponents of Prophylactic Mesh are concerned with mesh infection erosion fistula and other stoma related complications
Prevention of Parastomal Hernia
bull An older meta-analysis (3 RCT N = 128) showed a reduction in parastomal hernia with the use of prophylactic mesh [1]
bull Several RCTrsquos have been published recently which were not included in this review
1 Shabbir et al Colorectal Dis 2012
Objective
bull To perform an updated meta-analysis to determine the efficacy of prophylactic mesh in patients requiring a temporary or permanent stoma
Inclusion Criteria
bull Randomized Controlled trials comparing the prophylactic placement of mesh vs no mesh
bull Any type of stoma
bull Any type of mesh (biologic vs synthetic) or position (onlay sublay preperitoneal etc)
bull At least 12 months of follow up
Outcomes
Primary Outcome
bull Development of parastomal hernia diagnosed clinically or radiographically
Secondary Outcomes
bull Parastomal hernia requiring subsequent surgical repair
bull Perioperative Complications
bull Stoma Specific Complications
Information Sources amp Search Strategy
bull EMBASE (1947 ndash 2015) MEDLINE (1946 ndash2015) (Searched Oct 1 2015 and January 4 2016)
bull Included English and non-English language publications
Study Selection amp Data Collection
bull Title Abstract and Full text review were undertaken independently and in duplicate to determine eligibility for inclusion
bull Data was collected using a standardized form and in duplicate
Study Quality Assessment
bull Risk of bias was assessed as per the Cochrane Handbook
Randomization
Allocation Concealment
Blinding
Attrition Bias (Loss to Follow Up)
Selective Reporting
Other bias
Data Analysis
bull Statistical Analysis completed in REVMAN using a random effects model
bull A Priori Subgroup Analyses
Biologic vs Synthetic Permanent Mesh
Hernia Diagnosis technique (Clinical vs Radiographic)
Mesh Location
Search Results
bull 107 Results screened
bull 7 RCTrsquos fit our inclusion criteria
An additional study was identified which published the 5 year follow up of an included study
N = 20 ndash 113
Follow up 12 ndash 60 months
Study Characteristics
Pathology Malignant Only ndash4 Studies
Benign amp Malignant ndash3 Studies
Type Of Stoma Colostomy Only ndash5 Studies
Colostomy amp Ileostomy ndash 2 Studies
Permanent Stomas ndash6 Studies
Permanent amp Temporary ndash1 Study
Type of Mesh Synthetic Light Weight ndash 5 Studies
Biologic Mesh ndash2 Studies
Diagnosis Clinical Exam ndash3 Studies
Routine Radiologic Exam ndash5 Studies
Risk of Bias
bull 2 Studies with low risk of bias across all assessed categories
bull 2 Studies with unclear risk of bias Unclear allocation concealment Unclear if assessors were blinded
bull 3 Studies had high risk of bias in at least one category High loss to follow up (35) Per Protocol Analysis (Not ITT) Changed Diagnostic Criteria partway through the
study
Parastomal Hernia
bull Reduced Odds with Prophylactic Mesh
OR 022 95CI 009 ndash 049 I2 = 49
Parastomal Hernia requiring
subsequent surgerybull Reduced odds with Prophylactic Mesh
OR 031 95CI 011 ndash 086 I2 = 0
Surgical Complications (All)
bull No difference in overall complications (P = 023)
Stoma Specific Complications
bull No difference in stoma specific complications (P = 024)
Subgroup Analyses (Hernia Formation)bull No subgroup effect of mesh position (P = 093)
bull No subgroup effect noted based on how hernia was diagnosed (P = 085)
Subgroup Analysisbull A significant subgroup effect was found based on
biologic vs synthetic permanent mesh (P = 002)
Discussion
bull Prophylactic Mesh associated with
A decrease in parastomal hernia after at least 1 year of follow up (Primary Outcome)
A decrease in subsequent surgical repair (Secondary Outcome)
bull Not associated with
Surgical or Stoma Specific Complications
Limitations
bull Heterogeneity
Primary outcome showed moderate heterogeneity (I2 = 49)
Reduced with Subgroup analysis based on biologic vs synthetic mesh (I2 = 15)
Limitations
bull Inconsistent complication Rates
Overall Complications Between 0 - gt90
Stoma Specific Complications Between 0 -gt50
bull Widely varying definitions of complications
Vs ldquoComplicationsrdquo
Conclusions
bull Placement of prophylactic mesh at the time of index surgery
Decreased odds of developing a parastomal hernia
Decreased odds of requiring subsequent surgical repair of hernia
Not associated with increased odds of complications or stoma specific complications
Questions
patels2kghkarinet
epipatelmd
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018
Parastomal Hernia
bull Common Complication after surgery which creates a stoma (up to 75)
bull Risk factors include patient risk factors as well as technical risk factors (Type of Stoma Loop vs End etc)
Prophylactic Mesh Placement
Definitionbull The placement of mesh at the index operation to
prevent parastomal hernia
bull Multiple mesh placements and techniques described Onlay vs Sublay vs Preperitoneal Keyhole vs Sugar Baker Biologic vs Synthetic Mesh
bull Opponents of Prophylactic Mesh are concerned with mesh infection erosion fistula and other stoma related complications
Prevention of Parastomal Hernia
bull An older meta-analysis (3 RCT N = 128) showed a reduction in parastomal hernia with the use of prophylactic mesh [1]
bull Several RCTrsquos have been published recently which were not included in this review
1 Shabbir et al Colorectal Dis 2012
Objective
bull To perform an updated meta-analysis to determine the efficacy of prophylactic mesh in patients requiring a temporary or permanent stoma
Inclusion Criteria
bull Randomized Controlled trials comparing the prophylactic placement of mesh vs no mesh
bull Any type of stoma
bull Any type of mesh (biologic vs synthetic) or position (onlay sublay preperitoneal etc)
bull At least 12 months of follow up
Outcomes
Primary Outcome
bull Development of parastomal hernia diagnosed clinically or radiographically
Secondary Outcomes
bull Parastomal hernia requiring subsequent surgical repair
bull Perioperative Complications
bull Stoma Specific Complications
Information Sources amp Search Strategy
bull EMBASE (1947 ndash 2015) MEDLINE (1946 ndash2015) (Searched Oct 1 2015 and January 4 2016)
bull Included English and non-English language publications
Study Selection amp Data Collection
bull Title Abstract and Full text review were undertaken independently and in duplicate to determine eligibility for inclusion
bull Data was collected using a standardized form and in duplicate
Study Quality Assessment
bull Risk of bias was assessed as per the Cochrane Handbook
Randomization
Allocation Concealment
Blinding
Attrition Bias (Loss to Follow Up)
Selective Reporting
Other bias
Data Analysis
bull Statistical Analysis completed in REVMAN using a random effects model
bull A Priori Subgroup Analyses
Biologic vs Synthetic Permanent Mesh
Hernia Diagnosis technique (Clinical vs Radiographic)
Mesh Location
Search Results
bull 107 Results screened
bull 7 RCTrsquos fit our inclusion criteria
An additional study was identified which published the 5 year follow up of an included study
N = 20 ndash 113
Follow up 12 ndash 60 months
Study Characteristics
Pathology Malignant Only ndash4 Studies
Benign amp Malignant ndash3 Studies
Type Of Stoma Colostomy Only ndash5 Studies
Colostomy amp Ileostomy ndash 2 Studies
Permanent Stomas ndash6 Studies
Permanent amp Temporary ndash1 Study
Type of Mesh Synthetic Light Weight ndash 5 Studies
Biologic Mesh ndash2 Studies
Diagnosis Clinical Exam ndash3 Studies
Routine Radiologic Exam ndash5 Studies
Risk of Bias
bull 2 Studies with low risk of bias across all assessed categories
bull 2 Studies with unclear risk of bias Unclear allocation concealment Unclear if assessors were blinded
bull 3 Studies had high risk of bias in at least one category High loss to follow up (35) Per Protocol Analysis (Not ITT) Changed Diagnostic Criteria partway through the
study
Parastomal Hernia
bull Reduced Odds with Prophylactic Mesh
OR 022 95CI 009 ndash 049 I2 = 49
Parastomal Hernia requiring
subsequent surgerybull Reduced odds with Prophylactic Mesh
OR 031 95CI 011 ndash 086 I2 = 0
Surgical Complications (All)
bull No difference in overall complications (P = 023)
Stoma Specific Complications
bull No difference in stoma specific complications (P = 024)
Subgroup Analyses (Hernia Formation)bull No subgroup effect of mesh position (P = 093)
bull No subgroup effect noted based on how hernia was diagnosed (P = 085)
Subgroup Analysisbull A significant subgroup effect was found based on
biologic vs synthetic permanent mesh (P = 002)
Discussion
bull Prophylactic Mesh associated with
A decrease in parastomal hernia after at least 1 year of follow up (Primary Outcome)
A decrease in subsequent surgical repair (Secondary Outcome)
bull Not associated with
Surgical or Stoma Specific Complications
Limitations
bull Heterogeneity
Primary outcome showed moderate heterogeneity (I2 = 49)
Reduced with Subgroup analysis based on biologic vs synthetic mesh (I2 = 15)
Limitations
bull Inconsistent complication Rates
Overall Complications Between 0 - gt90
Stoma Specific Complications Between 0 -gt50
bull Widely varying definitions of complications
Vs ldquoComplicationsrdquo
Conclusions
bull Placement of prophylactic mesh at the time of index surgery
Decreased odds of developing a parastomal hernia
Decreased odds of requiring subsequent surgical repair of hernia
Not associated with increased odds of complications or stoma specific complications
Questions
patels2kghkarinet
epipatelmd
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018
Prophylactic Mesh Placement
Definitionbull The placement of mesh at the index operation to
prevent parastomal hernia
bull Multiple mesh placements and techniques described Onlay vs Sublay vs Preperitoneal Keyhole vs Sugar Baker Biologic vs Synthetic Mesh
bull Opponents of Prophylactic Mesh are concerned with mesh infection erosion fistula and other stoma related complications
Prevention of Parastomal Hernia
bull An older meta-analysis (3 RCT N = 128) showed a reduction in parastomal hernia with the use of prophylactic mesh [1]
bull Several RCTrsquos have been published recently which were not included in this review
1 Shabbir et al Colorectal Dis 2012
Objective
bull To perform an updated meta-analysis to determine the efficacy of prophylactic mesh in patients requiring a temporary or permanent stoma
Inclusion Criteria
bull Randomized Controlled trials comparing the prophylactic placement of mesh vs no mesh
bull Any type of stoma
bull Any type of mesh (biologic vs synthetic) or position (onlay sublay preperitoneal etc)
bull At least 12 months of follow up
Outcomes
Primary Outcome
bull Development of parastomal hernia diagnosed clinically or radiographically
Secondary Outcomes
bull Parastomal hernia requiring subsequent surgical repair
bull Perioperative Complications
bull Stoma Specific Complications
Information Sources amp Search Strategy
bull EMBASE (1947 ndash 2015) MEDLINE (1946 ndash2015) (Searched Oct 1 2015 and January 4 2016)
bull Included English and non-English language publications
Study Selection amp Data Collection
bull Title Abstract and Full text review were undertaken independently and in duplicate to determine eligibility for inclusion
bull Data was collected using a standardized form and in duplicate
Study Quality Assessment
bull Risk of bias was assessed as per the Cochrane Handbook
Randomization
Allocation Concealment
Blinding
Attrition Bias (Loss to Follow Up)
Selective Reporting
Other bias
Data Analysis
bull Statistical Analysis completed in REVMAN using a random effects model
bull A Priori Subgroup Analyses
Biologic vs Synthetic Permanent Mesh
Hernia Diagnosis technique (Clinical vs Radiographic)
Mesh Location
Search Results
bull 107 Results screened
bull 7 RCTrsquos fit our inclusion criteria
An additional study was identified which published the 5 year follow up of an included study
N = 20 ndash 113
Follow up 12 ndash 60 months
Study Characteristics
Pathology Malignant Only ndash4 Studies
Benign amp Malignant ndash3 Studies
Type Of Stoma Colostomy Only ndash5 Studies
Colostomy amp Ileostomy ndash 2 Studies
Permanent Stomas ndash6 Studies
Permanent amp Temporary ndash1 Study
Type of Mesh Synthetic Light Weight ndash 5 Studies
Biologic Mesh ndash2 Studies
Diagnosis Clinical Exam ndash3 Studies
Routine Radiologic Exam ndash5 Studies
Risk of Bias
bull 2 Studies with low risk of bias across all assessed categories
bull 2 Studies with unclear risk of bias Unclear allocation concealment Unclear if assessors were blinded
bull 3 Studies had high risk of bias in at least one category High loss to follow up (35) Per Protocol Analysis (Not ITT) Changed Diagnostic Criteria partway through the
study
Parastomal Hernia
bull Reduced Odds with Prophylactic Mesh
OR 022 95CI 009 ndash 049 I2 = 49
Parastomal Hernia requiring
subsequent surgerybull Reduced odds with Prophylactic Mesh
OR 031 95CI 011 ndash 086 I2 = 0
Surgical Complications (All)
bull No difference in overall complications (P = 023)
Stoma Specific Complications
bull No difference in stoma specific complications (P = 024)
Subgroup Analyses (Hernia Formation)bull No subgroup effect of mesh position (P = 093)
bull No subgroup effect noted based on how hernia was diagnosed (P = 085)
Subgroup Analysisbull A significant subgroup effect was found based on
biologic vs synthetic permanent mesh (P = 002)
Discussion
bull Prophylactic Mesh associated with
A decrease in parastomal hernia after at least 1 year of follow up (Primary Outcome)
A decrease in subsequent surgical repair (Secondary Outcome)
bull Not associated with
Surgical or Stoma Specific Complications
Limitations
bull Heterogeneity
Primary outcome showed moderate heterogeneity (I2 = 49)
Reduced with Subgroup analysis based on biologic vs synthetic mesh (I2 = 15)
Limitations
bull Inconsistent complication Rates
Overall Complications Between 0 - gt90
Stoma Specific Complications Between 0 -gt50
bull Widely varying definitions of complications
Vs ldquoComplicationsrdquo
Conclusions
bull Placement of prophylactic mesh at the time of index surgery
Decreased odds of developing a parastomal hernia
Decreased odds of requiring subsequent surgical repair of hernia
Not associated with increased odds of complications or stoma specific complications
Questions
patels2kghkarinet
epipatelmd
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018
Prevention of Parastomal Hernia
bull An older meta-analysis (3 RCT N = 128) showed a reduction in parastomal hernia with the use of prophylactic mesh [1]
bull Several RCTrsquos have been published recently which were not included in this review
1 Shabbir et al Colorectal Dis 2012
Objective
bull To perform an updated meta-analysis to determine the efficacy of prophylactic mesh in patients requiring a temporary or permanent stoma
Inclusion Criteria
bull Randomized Controlled trials comparing the prophylactic placement of mesh vs no mesh
bull Any type of stoma
bull Any type of mesh (biologic vs synthetic) or position (onlay sublay preperitoneal etc)
bull At least 12 months of follow up
Outcomes
Primary Outcome
bull Development of parastomal hernia diagnosed clinically or radiographically
Secondary Outcomes
bull Parastomal hernia requiring subsequent surgical repair
bull Perioperative Complications
bull Stoma Specific Complications
Information Sources amp Search Strategy
bull EMBASE (1947 ndash 2015) MEDLINE (1946 ndash2015) (Searched Oct 1 2015 and January 4 2016)
bull Included English and non-English language publications
Study Selection amp Data Collection
bull Title Abstract and Full text review were undertaken independently and in duplicate to determine eligibility for inclusion
bull Data was collected using a standardized form and in duplicate
Study Quality Assessment
bull Risk of bias was assessed as per the Cochrane Handbook
Randomization
Allocation Concealment
Blinding
Attrition Bias (Loss to Follow Up)
Selective Reporting
Other bias
Data Analysis
bull Statistical Analysis completed in REVMAN using a random effects model
bull A Priori Subgroup Analyses
Biologic vs Synthetic Permanent Mesh
Hernia Diagnosis technique (Clinical vs Radiographic)
Mesh Location
Search Results
bull 107 Results screened
bull 7 RCTrsquos fit our inclusion criteria
An additional study was identified which published the 5 year follow up of an included study
N = 20 ndash 113
Follow up 12 ndash 60 months
Study Characteristics
Pathology Malignant Only ndash4 Studies
Benign amp Malignant ndash3 Studies
Type Of Stoma Colostomy Only ndash5 Studies
Colostomy amp Ileostomy ndash 2 Studies
Permanent Stomas ndash6 Studies
Permanent amp Temporary ndash1 Study
Type of Mesh Synthetic Light Weight ndash 5 Studies
Biologic Mesh ndash2 Studies
Diagnosis Clinical Exam ndash3 Studies
Routine Radiologic Exam ndash5 Studies
Risk of Bias
bull 2 Studies with low risk of bias across all assessed categories
bull 2 Studies with unclear risk of bias Unclear allocation concealment Unclear if assessors were blinded
bull 3 Studies had high risk of bias in at least one category High loss to follow up (35) Per Protocol Analysis (Not ITT) Changed Diagnostic Criteria partway through the
study
Parastomal Hernia
bull Reduced Odds with Prophylactic Mesh
OR 022 95CI 009 ndash 049 I2 = 49
Parastomal Hernia requiring
subsequent surgerybull Reduced odds with Prophylactic Mesh
OR 031 95CI 011 ndash 086 I2 = 0
Surgical Complications (All)
bull No difference in overall complications (P = 023)
Stoma Specific Complications
bull No difference in stoma specific complications (P = 024)
Subgroup Analyses (Hernia Formation)bull No subgroup effect of mesh position (P = 093)
bull No subgroup effect noted based on how hernia was diagnosed (P = 085)
Subgroup Analysisbull A significant subgroup effect was found based on
biologic vs synthetic permanent mesh (P = 002)
Discussion
bull Prophylactic Mesh associated with
A decrease in parastomal hernia after at least 1 year of follow up (Primary Outcome)
A decrease in subsequent surgical repair (Secondary Outcome)
bull Not associated with
Surgical or Stoma Specific Complications
Limitations
bull Heterogeneity
Primary outcome showed moderate heterogeneity (I2 = 49)
Reduced with Subgroup analysis based on biologic vs synthetic mesh (I2 = 15)
Limitations
bull Inconsistent complication Rates
Overall Complications Between 0 - gt90
Stoma Specific Complications Between 0 -gt50
bull Widely varying definitions of complications
Vs ldquoComplicationsrdquo
Conclusions
bull Placement of prophylactic mesh at the time of index surgery
Decreased odds of developing a parastomal hernia
Decreased odds of requiring subsequent surgical repair of hernia
Not associated with increased odds of complications or stoma specific complications
Questions
patels2kghkarinet
epipatelmd
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018
Objective
bull To perform an updated meta-analysis to determine the efficacy of prophylactic mesh in patients requiring a temporary or permanent stoma
Inclusion Criteria
bull Randomized Controlled trials comparing the prophylactic placement of mesh vs no mesh
bull Any type of stoma
bull Any type of mesh (biologic vs synthetic) or position (onlay sublay preperitoneal etc)
bull At least 12 months of follow up
Outcomes
Primary Outcome
bull Development of parastomal hernia diagnosed clinically or radiographically
Secondary Outcomes
bull Parastomal hernia requiring subsequent surgical repair
bull Perioperative Complications
bull Stoma Specific Complications
Information Sources amp Search Strategy
bull EMBASE (1947 ndash 2015) MEDLINE (1946 ndash2015) (Searched Oct 1 2015 and January 4 2016)
bull Included English and non-English language publications
Study Selection amp Data Collection
bull Title Abstract and Full text review were undertaken independently and in duplicate to determine eligibility for inclusion
bull Data was collected using a standardized form and in duplicate
Study Quality Assessment
bull Risk of bias was assessed as per the Cochrane Handbook
Randomization
Allocation Concealment
Blinding
Attrition Bias (Loss to Follow Up)
Selective Reporting
Other bias
Data Analysis
bull Statistical Analysis completed in REVMAN using a random effects model
bull A Priori Subgroup Analyses
Biologic vs Synthetic Permanent Mesh
Hernia Diagnosis technique (Clinical vs Radiographic)
Mesh Location
Search Results
bull 107 Results screened
bull 7 RCTrsquos fit our inclusion criteria
An additional study was identified which published the 5 year follow up of an included study
N = 20 ndash 113
Follow up 12 ndash 60 months
Study Characteristics
Pathology Malignant Only ndash4 Studies
Benign amp Malignant ndash3 Studies
Type Of Stoma Colostomy Only ndash5 Studies
Colostomy amp Ileostomy ndash 2 Studies
Permanent Stomas ndash6 Studies
Permanent amp Temporary ndash1 Study
Type of Mesh Synthetic Light Weight ndash 5 Studies
Biologic Mesh ndash2 Studies
Diagnosis Clinical Exam ndash3 Studies
Routine Radiologic Exam ndash5 Studies
Risk of Bias
bull 2 Studies with low risk of bias across all assessed categories
bull 2 Studies with unclear risk of bias Unclear allocation concealment Unclear if assessors were blinded
bull 3 Studies had high risk of bias in at least one category High loss to follow up (35) Per Protocol Analysis (Not ITT) Changed Diagnostic Criteria partway through the
study
Parastomal Hernia
bull Reduced Odds with Prophylactic Mesh
OR 022 95CI 009 ndash 049 I2 = 49
Parastomal Hernia requiring
subsequent surgerybull Reduced odds with Prophylactic Mesh
OR 031 95CI 011 ndash 086 I2 = 0
Surgical Complications (All)
bull No difference in overall complications (P = 023)
Stoma Specific Complications
bull No difference in stoma specific complications (P = 024)
Subgroup Analyses (Hernia Formation)bull No subgroup effect of mesh position (P = 093)
bull No subgroup effect noted based on how hernia was diagnosed (P = 085)
Subgroup Analysisbull A significant subgroup effect was found based on
biologic vs synthetic permanent mesh (P = 002)
Discussion
bull Prophylactic Mesh associated with
A decrease in parastomal hernia after at least 1 year of follow up (Primary Outcome)
A decrease in subsequent surgical repair (Secondary Outcome)
bull Not associated with
Surgical or Stoma Specific Complications
Limitations
bull Heterogeneity
Primary outcome showed moderate heterogeneity (I2 = 49)
Reduced with Subgroup analysis based on biologic vs synthetic mesh (I2 = 15)
Limitations
bull Inconsistent complication Rates
Overall Complications Between 0 - gt90
Stoma Specific Complications Between 0 -gt50
bull Widely varying definitions of complications
Vs ldquoComplicationsrdquo
Conclusions
bull Placement of prophylactic mesh at the time of index surgery
Decreased odds of developing a parastomal hernia
Decreased odds of requiring subsequent surgical repair of hernia
Not associated with increased odds of complications or stoma specific complications
Questions
patels2kghkarinet
epipatelmd
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018
Inclusion Criteria
bull Randomized Controlled trials comparing the prophylactic placement of mesh vs no mesh
bull Any type of stoma
bull Any type of mesh (biologic vs synthetic) or position (onlay sublay preperitoneal etc)
bull At least 12 months of follow up
Outcomes
Primary Outcome
bull Development of parastomal hernia diagnosed clinically or radiographically
Secondary Outcomes
bull Parastomal hernia requiring subsequent surgical repair
bull Perioperative Complications
bull Stoma Specific Complications
Information Sources amp Search Strategy
bull EMBASE (1947 ndash 2015) MEDLINE (1946 ndash2015) (Searched Oct 1 2015 and January 4 2016)
bull Included English and non-English language publications
Study Selection amp Data Collection
bull Title Abstract and Full text review were undertaken independently and in duplicate to determine eligibility for inclusion
bull Data was collected using a standardized form and in duplicate
Study Quality Assessment
bull Risk of bias was assessed as per the Cochrane Handbook
Randomization
Allocation Concealment
Blinding
Attrition Bias (Loss to Follow Up)
Selective Reporting
Other bias
Data Analysis
bull Statistical Analysis completed in REVMAN using a random effects model
bull A Priori Subgroup Analyses
Biologic vs Synthetic Permanent Mesh
Hernia Diagnosis technique (Clinical vs Radiographic)
Mesh Location
Search Results
bull 107 Results screened
bull 7 RCTrsquos fit our inclusion criteria
An additional study was identified which published the 5 year follow up of an included study
N = 20 ndash 113
Follow up 12 ndash 60 months
Study Characteristics
Pathology Malignant Only ndash4 Studies
Benign amp Malignant ndash3 Studies
Type Of Stoma Colostomy Only ndash5 Studies
Colostomy amp Ileostomy ndash 2 Studies
Permanent Stomas ndash6 Studies
Permanent amp Temporary ndash1 Study
Type of Mesh Synthetic Light Weight ndash 5 Studies
Biologic Mesh ndash2 Studies
Diagnosis Clinical Exam ndash3 Studies
Routine Radiologic Exam ndash5 Studies
Risk of Bias
bull 2 Studies with low risk of bias across all assessed categories
bull 2 Studies with unclear risk of bias Unclear allocation concealment Unclear if assessors were blinded
bull 3 Studies had high risk of bias in at least one category High loss to follow up (35) Per Protocol Analysis (Not ITT) Changed Diagnostic Criteria partway through the
study
Parastomal Hernia
bull Reduced Odds with Prophylactic Mesh
OR 022 95CI 009 ndash 049 I2 = 49
Parastomal Hernia requiring
subsequent surgerybull Reduced odds with Prophylactic Mesh
OR 031 95CI 011 ndash 086 I2 = 0
Surgical Complications (All)
bull No difference in overall complications (P = 023)
Stoma Specific Complications
bull No difference in stoma specific complications (P = 024)
Subgroup Analyses (Hernia Formation)bull No subgroup effect of mesh position (P = 093)
bull No subgroup effect noted based on how hernia was diagnosed (P = 085)
Subgroup Analysisbull A significant subgroup effect was found based on
biologic vs synthetic permanent mesh (P = 002)
Discussion
bull Prophylactic Mesh associated with
A decrease in parastomal hernia after at least 1 year of follow up (Primary Outcome)
A decrease in subsequent surgical repair (Secondary Outcome)
bull Not associated with
Surgical or Stoma Specific Complications
Limitations
bull Heterogeneity
Primary outcome showed moderate heterogeneity (I2 = 49)
Reduced with Subgroup analysis based on biologic vs synthetic mesh (I2 = 15)
Limitations
bull Inconsistent complication Rates
Overall Complications Between 0 - gt90
Stoma Specific Complications Between 0 -gt50
bull Widely varying definitions of complications
Vs ldquoComplicationsrdquo
Conclusions
bull Placement of prophylactic mesh at the time of index surgery
Decreased odds of developing a parastomal hernia
Decreased odds of requiring subsequent surgical repair of hernia
Not associated with increased odds of complications or stoma specific complications
Questions
patels2kghkarinet
epipatelmd
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018

Outcomes
Primary Outcome
bull Development of parastomal hernia diagnosed clinically or radiographically
Secondary Outcomes
bull Parastomal hernia requiring subsequent surgical repair
bull Perioperative Complications
bull Stoma Specific Complications
Information Sources amp Search Strategy
bull EMBASE (1947 ndash 2015) MEDLINE (1946 ndash2015) (Searched Oct 1 2015 and January 4 2016)
bull Included English and non-English language publications
Study Selection amp Data Collection
bull Title Abstract and Full text review were undertaken independently and in duplicate to determine eligibility for inclusion
bull Data was collected using a standardized form and in duplicate
Study Quality Assessment
bull Risk of bias was assessed as per the Cochrane Handbook
Randomization
Allocation Concealment
Blinding
Attrition Bias (Loss to Follow Up)
Selective Reporting
Other bias
Data Analysis
bull Statistical Analysis completed in REVMAN using a random effects model
bull A Priori Subgroup Analyses
Biologic vs Synthetic Permanent Mesh
Hernia Diagnosis technique (Clinical vs Radiographic)
Mesh Location
Search Results
bull 107 Results screened
bull 7 RCTrsquos fit our inclusion criteria
An additional study was identified which published the 5 year follow up of an included study
N = 20 ndash 113
Follow up 12 ndash 60 months
Study Characteristics
Pathology Malignant Only ndash4 Studies
Benign amp Malignant ndash3 Studies
Type Of Stoma Colostomy Only ndash5 Studies
Colostomy amp Ileostomy ndash 2 Studies
Permanent Stomas ndash6 Studies
Permanent amp Temporary ndash1 Study
Type of Mesh Synthetic Light Weight ndash 5 Studies
Biologic Mesh ndash2 Studies
Diagnosis Clinical Exam ndash3 Studies
Routine Radiologic Exam ndash5 Studies
Risk of Bias
bull 2 Studies with low risk of bias across all assessed categories
bull 2 Studies with unclear risk of bias Unclear allocation concealment Unclear if assessors were blinded
bull 3 Studies had high risk of bias in at least one category High loss to follow up (35) Per Protocol Analysis (Not ITT) Changed Diagnostic Criteria partway through the
study
Parastomal Hernia
bull Reduced Odds with Prophylactic Mesh
OR 022 95CI 009 ndash 049 I2 = 49
Parastomal Hernia requiring
subsequent surgerybull Reduced odds with Prophylactic Mesh
OR 031 95CI 011 ndash 086 I2 = 0
Surgical Complications (All)
bull No difference in overall complications (P = 023)
Stoma Specific Complications
bull No difference in stoma specific complications (P = 024)
Subgroup Analyses (Hernia Formation)bull No subgroup effect of mesh position (P = 093)
bull No subgroup effect noted based on how hernia was diagnosed (P = 085)
Subgroup Analysisbull A significant subgroup effect was found based on
biologic vs synthetic permanent mesh (P = 002)
Discussion
bull Prophylactic Mesh associated with
A decrease in parastomal hernia after at least 1 year of follow up (Primary Outcome)
A decrease in subsequent surgical repair (Secondary Outcome)
bull Not associated with
Surgical or Stoma Specific Complications
Limitations
bull Heterogeneity
Primary outcome showed moderate heterogeneity (I2 = 49)
Reduced with Subgroup analysis based on biologic vs synthetic mesh (I2 = 15)
Limitations
bull Inconsistent complication Rates
Overall Complications Between 0 - gt90
Stoma Specific Complications Between 0 -gt50
bull Widely varying definitions of complications
Vs ldquoComplicationsrdquo
Conclusions
bull Placement of prophylactic mesh at the time of index surgery
Decreased odds of developing a parastomal hernia
Decreased odds of requiring subsequent surgical repair of hernia
Not associated with increased odds of complications or stoma specific complications
Questions
patels2kghkarinet
epipatelmd
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018

Information Sources amp Search Strategy
bull EMBASE (1947 ndash 2015) MEDLINE (1946 ndash2015) (Searched Oct 1 2015 and January 4 2016)
bull Included English and non-English language publications
Study Selection amp Data Collection
bull Title Abstract and Full text review were undertaken independently and in duplicate to determine eligibility for inclusion
bull Data was collected using a standardized form and in duplicate
Study Quality Assessment
bull Risk of bias was assessed as per the Cochrane Handbook
Randomization
Allocation Concealment
Blinding
Attrition Bias (Loss to Follow Up)
Selective Reporting
Other bias
Data Analysis
bull Statistical Analysis completed in REVMAN using a random effects model
bull A Priori Subgroup Analyses
Biologic vs Synthetic Permanent Mesh
Hernia Diagnosis technique (Clinical vs Radiographic)
Mesh Location
Search Results
bull 107 Results screened
bull 7 RCTrsquos fit our inclusion criteria
An additional study was identified which published the 5 year follow up of an included study
N = 20 ndash 113
Follow up 12 ndash 60 months
Study Characteristics
Pathology Malignant Only ndash4 Studies
Benign amp Malignant ndash3 Studies
Type Of Stoma Colostomy Only ndash5 Studies
Colostomy amp Ileostomy ndash 2 Studies
Permanent Stomas ndash6 Studies
Permanent amp Temporary ndash1 Study
Type of Mesh Synthetic Light Weight ndash 5 Studies
Biologic Mesh ndash2 Studies
Diagnosis Clinical Exam ndash3 Studies
Routine Radiologic Exam ndash5 Studies
Risk of Bias
bull 2 Studies with low risk of bias across all assessed categories
bull 2 Studies with unclear risk of bias Unclear allocation concealment Unclear if assessors were blinded
bull 3 Studies had high risk of bias in at least one category High loss to follow up (35) Per Protocol Analysis (Not ITT) Changed Diagnostic Criteria partway through the
study
Parastomal Hernia
bull Reduced Odds with Prophylactic Mesh
OR 022 95CI 009 ndash 049 I2 = 49
Parastomal Hernia requiring
subsequent surgerybull Reduced odds with Prophylactic Mesh
OR 031 95CI 011 ndash 086 I2 = 0
Surgical Complications (All)
bull No difference in overall complications (P = 023)
Stoma Specific Complications
bull No difference in stoma specific complications (P = 024)
Subgroup Analyses (Hernia Formation)bull No subgroup effect of mesh position (P = 093)
bull No subgroup effect noted based on how hernia was diagnosed (P = 085)
Subgroup Analysisbull A significant subgroup effect was found based on
biologic vs synthetic permanent mesh (P = 002)
Discussion
bull Prophylactic Mesh associated with
A decrease in parastomal hernia after at least 1 year of follow up (Primary Outcome)
A decrease in subsequent surgical repair (Secondary Outcome)
bull Not associated with
Surgical or Stoma Specific Complications
Limitations
bull Heterogeneity
Primary outcome showed moderate heterogeneity (I2 = 49)
Reduced with Subgroup analysis based on biologic vs synthetic mesh (I2 = 15)
Limitations
bull Inconsistent complication Rates
Overall Complications Between 0 - gt90
Stoma Specific Complications Between 0 -gt50
bull Widely varying definitions of complications
Vs ldquoComplicationsrdquo
Conclusions
bull Placement of prophylactic mesh at the time of index surgery
Decreased odds of developing a parastomal hernia
Decreased odds of requiring subsequent surgical repair of hernia
Not associated with increased odds of complications or stoma specific complications
Questions
patels2kghkarinet
epipatelmd
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018

Study Selection amp Data Collection
bull Title Abstract and Full text review were undertaken independently and in duplicate to determine eligibility for inclusion
bull Data was collected using a standardized form and in duplicate
Study Quality Assessment
bull Risk of bias was assessed as per the Cochrane Handbook
Randomization
Allocation Concealment
Blinding
Attrition Bias (Loss to Follow Up)
Selective Reporting
Other bias
Data Analysis
bull Statistical Analysis completed in REVMAN using a random effects model
bull A Priori Subgroup Analyses
Biologic vs Synthetic Permanent Mesh
Hernia Diagnosis technique (Clinical vs Radiographic)
Mesh Location
Search Results
bull 107 Results screened
bull 7 RCTrsquos fit our inclusion criteria
An additional study was identified which published the 5 year follow up of an included study
N = 20 ndash 113
Follow up 12 ndash 60 months
Study Characteristics
Pathology Malignant Only ndash4 Studies
Benign amp Malignant ndash3 Studies
Type Of Stoma Colostomy Only ndash5 Studies
Colostomy amp Ileostomy ndash 2 Studies
Permanent Stomas ndash6 Studies
Permanent amp Temporary ndash1 Study
Type of Mesh Synthetic Light Weight ndash 5 Studies
Biologic Mesh ndash2 Studies
Diagnosis Clinical Exam ndash3 Studies
Routine Radiologic Exam ndash5 Studies
Risk of Bias
bull 2 Studies with low risk of bias across all assessed categories
bull 2 Studies with unclear risk of bias Unclear allocation concealment Unclear if assessors were blinded
bull 3 Studies had high risk of bias in at least one category High loss to follow up (35) Per Protocol Analysis (Not ITT) Changed Diagnostic Criteria partway through the
study
Parastomal Hernia
bull Reduced Odds with Prophylactic Mesh
OR 022 95CI 009 ndash 049 I2 = 49
Parastomal Hernia requiring
subsequent surgerybull Reduced odds with Prophylactic Mesh
OR 031 95CI 011 ndash 086 I2 = 0
Surgical Complications (All)
bull No difference in overall complications (P = 023)
Stoma Specific Complications
bull No difference in stoma specific complications (P = 024)
Subgroup Analyses (Hernia Formation)bull No subgroup effect of mesh position (P = 093)
bull No subgroup effect noted based on how hernia was diagnosed (P = 085)
Subgroup Analysisbull A significant subgroup effect was found based on
biologic vs synthetic permanent mesh (P = 002)
Discussion
bull Prophylactic Mesh associated with
A decrease in parastomal hernia after at least 1 year of follow up (Primary Outcome)
A decrease in subsequent surgical repair (Secondary Outcome)
bull Not associated with
Surgical or Stoma Specific Complications
Limitations
bull Heterogeneity
Primary outcome showed moderate heterogeneity (I2 = 49)
Reduced with Subgroup analysis based on biologic vs synthetic mesh (I2 = 15)
Limitations
bull Inconsistent complication Rates
Overall Complications Between 0 - gt90
Stoma Specific Complications Between 0 -gt50
bull Widely varying definitions of complications
Vs ldquoComplicationsrdquo
Conclusions
bull Placement of prophylactic mesh at the time of index surgery
Decreased odds of developing a parastomal hernia
Decreased odds of requiring subsequent surgical repair of hernia
Not associated with increased odds of complications or stoma specific complications
Questions
patels2kghkarinet
epipatelmd
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018
Study Quality Assessment
bull Risk of bias was assessed as per the Cochrane Handbook
Randomization
Allocation Concealment
Blinding
Attrition Bias (Loss to Follow Up)
Selective Reporting
Other bias
Data Analysis
bull Statistical Analysis completed in REVMAN using a random effects model
bull A Priori Subgroup Analyses
Biologic vs Synthetic Permanent Mesh
Hernia Diagnosis technique (Clinical vs Radiographic)
Mesh Location
Search Results
bull 107 Results screened
bull 7 RCTrsquos fit our inclusion criteria
An additional study was identified which published the 5 year follow up of an included study
N = 20 ndash 113
Follow up 12 ndash 60 months
Study Characteristics
Pathology Malignant Only ndash4 Studies
Benign amp Malignant ndash3 Studies
Type Of Stoma Colostomy Only ndash5 Studies
Colostomy amp Ileostomy ndash 2 Studies
Permanent Stomas ndash6 Studies
Permanent amp Temporary ndash1 Study
Type of Mesh Synthetic Light Weight ndash 5 Studies
Biologic Mesh ndash2 Studies
Diagnosis Clinical Exam ndash3 Studies
Routine Radiologic Exam ndash5 Studies
Risk of Bias
bull 2 Studies with low risk of bias across all assessed categories
bull 2 Studies with unclear risk of bias Unclear allocation concealment Unclear if assessors were blinded
bull 3 Studies had high risk of bias in at least one category High loss to follow up (35) Per Protocol Analysis (Not ITT) Changed Diagnostic Criteria partway through the
study
Parastomal Hernia
bull Reduced Odds with Prophylactic Mesh
OR 022 95CI 009 ndash 049 I2 = 49
Parastomal Hernia requiring
subsequent surgerybull Reduced odds with Prophylactic Mesh
OR 031 95CI 011 ndash 086 I2 = 0
Surgical Complications (All)
bull No difference in overall complications (P = 023)
Stoma Specific Complications
bull No difference in stoma specific complications (P = 024)
Subgroup Analyses (Hernia Formation)bull No subgroup effect of mesh position (P = 093)
bull No subgroup effect noted based on how hernia was diagnosed (P = 085)
Subgroup Analysisbull A significant subgroup effect was found based on
biologic vs synthetic permanent mesh (P = 002)
Discussion
bull Prophylactic Mesh associated with
A decrease in parastomal hernia after at least 1 year of follow up (Primary Outcome)
A decrease in subsequent surgical repair (Secondary Outcome)
bull Not associated with
Surgical or Stoma Specific Complications
Limitations
bull Heterogeneity
Primary outcome showed moderate heterogeneity (I2 = 49)
Reduced with Subgroup analysis based on biologic vs synthetic mesh (I2 = 15)
Limitations
bull Inconsistent complication Rates
Overall Complications Between 0 - gt90
Stoma Specific Complications Between 0 -gt50
bull Widely varying definitions of complications
Vs ldquoComplicationsrdquo
Conclusions
bull Placement of prophylactic mesh at the time of index surgery
Decreased odds of developing a parastomal hernia
Decreased odds of requiring subsequent surgical repair of hernia
Not associated with increased odds of complications or stoma specific complications
Questions
patels2kghkarinet
epipatelmd
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018
Data Analysis
bull Statistical Analysis completed in REVMAN using a random effects model
bull A Priori Subgroup Analyses
Biologic vs Synthetic Permanent Mesh
Hernia Diagnosis technique (Clinical vs Radiographic)
Mesh Location
Search Results
bull 107 Results screened
bull 7 RCTrsquos fit our inclusion criteria
An additional study was identified which published the 5 year follow up of an included study
N = 20 ndash 113
Follow up 12 ndash 60 months
Study Characteristics
Pathology Malignant Only ndash4 Studies
Benign amp Malignant ndash3 Studies
Type Of Stoma Colostomy Only ndash5 Studies
Colostomy amp Ileostomy ndash 2 Studies
Permanent Stomas ndash6 Studies
Permanent amp Temporary ndash1 Study
Type of Mesh Synthetic Light Weight ndash 5 Studies
Biologic Mesh ndash2 Studies
Diagnosis Clinical Exam ndash3 Studies
Routine Radiologic Exam ndash5 Studies
Risk of Bias
bull 2 Studies with low risk of bias across all assessed categories
bull 2 Studies with unclear risk of bias Unclear allocation concealment Unclear if assessors were blinded
bull 3 Studies had high risk of bias in at least one category High loss to follow up (35) Per Protocol Analysis (Not ITT) Changed Diagnostic Criteria partway through the
study
Parastomal Hernia
bull Reduced Odds with Prophylactic Mesh
OR 022 95CI 009 ndash 049 I2 = 49
Parastomal Hernia requiring
subsequent surgerybull Reduced odds with Prophylactic Mesh
OR 031 95CI 011 ndash 086 I2 = 0
Surgical Complications (All)
bull No difference in overall complications (P = 023)
Stoma Specific Complications
bull No difference in stoma specific complications (P = 024)
Subgroup Analyses (Hernia Formation)bull No subgroup effect of mesh position (P = 093)
bull No subgroup effect noted based on how hernia was diagnosed (P = 085)
Subgroup Analysisbull A significant subgroup effect was found based on
biologic vs synthetic permanent mesh (P = 002)
Discussion
bull Prophylactic Mesh associated with
A decrease in parastomal hernia after at least 1 year of follow up (Primary Outcome)
A decrease in subsequent surgical repair (Secondary Outcome)
bull Not associated with
Surgical or Stoma Specific Complications
Limitations
bull Heterogeneity
Primary outcome showed moderate heterogeneity (I2 = 49)
Reduced with Subgroup analysis based on biologic vs synthetic mesh (I2 = 15)
Limitations
bull Inconsistent complication Rates
Overall Complications Between 0 - gt90
Stoma Specific Complications Between 0 -gt50
bull Widely varying definitions of complications
Vs ldquoComplicationsrdquo
Conclusions
bull Placement of prophylactic mesh at the time of index surgery
Decreased odds of developing a parastomal hernia
Decreased odds of requiring subsequent surgical repair of hernia
Not associated with increased odds of complications or stoma specific complications
Questions
patels2kghkarinet
epipatelmd
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018
Search Results
bull 107 Results screened
bull 7 RCTrsquos fit our inclusion criteria
An additional study was identified which published the 5 year follow up of an included study
N = 20 ndash 113
Follow up 12 ndash 60 months
Study Characteristics
Pathology Malignant Only ndash4 Studies
Benign amp Malignant ndash3 Studies
Type Of Stoma Colostomy Only ndash5 Studies
Colostomy amp Ileostomy ndash 2 Studies
Permanent Stomas ndash6 Studies
Permanent amp Temporary ndash1 Study
Type of Mesh Synthetic Light Weight ndash 5 Studies
Biologic Mesh ndash2 Studies
Diagnosis Clinical Exam ndash3 Studies
Routine Radiologic Exam ndash5 Studies
Risk of Bias
bull 2 Studies with low risk of bias across all assessed categories
bull 2 Studies with unclear risk of bias Unclear allocation concealment Unclear if assessors were blinded
bull 3 Studies had high risk of bias in at least one category High loss to follow up (35) Per Protocol Analysis (Not ITT) Changed Diagnostic Criteria partway through the
study
Parastomal Hernia
bull Reduced Odds with Prophylactic Mesh
OR 022 95CI 009 ndash 049 I2 = 49
Parastomal Hernia requiring
subsequent surgerybull Reduced odds with Prophylactic Mesh
OR 031 95CI 011 ndash 086 I2 = 0
Surgical Complications (All)
bull No difference in overall complications (P = 023)
Stoma Specific Complications
bull No difference in stoma specific complications (P = 024)
Subgroup Analyses (Hernia Formation)bull No subgroup effect of mesh position (P = 093)
bull No subgroup effect noted based on how hernia was diagnosed (P = 085)
Subgroup Analysisbull A significant subgroup effect was found based on
biologic vs synthetic permanent mesh (P = 002)
Discussion
bull Prophylactic Mesh associated with
A decrease in parastomal hernia after at least 1 year of follow up (Primary Outcome)
A decrease in subsequent surgical repair (Secondary Outcome)
bull Not associated with
Surgical or Stoma Specific Complications
Limitations
bull Heterogeneity
Primary outcome showed moderate heterogeneity (I2 = 49)
Reduced with Subgroup analysis based on biologic vs synthetic mesh (I2 = 15)
Limitations
bull Inconsistent complication Rates
Overall Complications Between 0 - gt90
Stoma Specific Complications Between 0 -gt50
bull Widely varying definitions of complications
Vs ldquoComplicationsrdquo
Conclusions
bull Placement of prophylactic mesh at the time of index surgery
Decreased odds of developing a parastomal hernia
Decreased odds of requiring subsequent surgical repair of hernia
Not associated with increased odds of complications or stoma specific complications
Questions
patels2kghkarinet
epipatelmd
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018

Study Characteristics
Pathology Malignant Only ndash4 Studies
Benign amp Malignant ndash3 Studies
Type Of Stoma Colostomy Only ndash5 Studies
Colostomy amp Ileostomy ndash 2 Studies
Permanent Stomas ndash6 Studies
Permanent amp Temporary ndash1 Study
Type of Mesh Synthetic Light Weight ndash 5 Studies
Biologic Mesh ndash2 Studies
Diagnosis Clinical Exam ndash3 Studies
Routine Radiologic Exam ndash5 Studies
Risk of Bias
bull 2 Studies with low risk of bias across all assessed categories
bull 2 Studies with unclear risk of bias Unclear allocation concealment Unclear if assessors were blinded
bull 3 Studies had high risk of bias in at least one category High loss to follow up (35) Per Protocol Analysis (Not ITT) Changed Diagnostic Criteria partway through the
study
Parastomal Hernia
bull Reduced Odds with Prophylactic Mesh
OR 022 95CI 009 ndash 049 I2 = 49
Parastomal Hernia requiring
subsequent surgerybull Reduced odds with Prophylactic Mesh
OR 031 95CI 011 ndash 086 I2 = 0
Surgical Complications (All)
bull No difference in overall complications (P = 023)
Stoma Specific Complications
bull No difference in stoma specific complications (P = 024)
Subgroup Analyses (Hernia Formation)bull No subgroup effect of mesh position (P = 093)
bull No subgroup effect noted based on how hernia was diagnosed (P = 085)
Subgroup Analysisbull A significant subgroup effect was found based on
biologic vs synthetic permanent mesh (P = 002)
Discussion
bull Prophylactic Mesh associated with
A decrease in parastomal hernia after at least 1 year of follow up (Primary Outcome)
A decrease in subsequent surgical repair (Secondary Outcome)
bull Not associated with
Surgical or Stoma Specific Complications
Limitations
bull Heterogeneity
Primary outcome showed moderate heterogeneity (I2 = 49)
Reduced with Subgroup analysis based on biologic vs synthetic mesh (I2 = 15)
Limitations
bull Inconsistent complication Rates
Overall Complications Between 0 - gt90
Stoma Specific Complications Between 0 -gt50
bull Widely varying definitions of complications
Vs ldquoComplicationsrdquo
Conclusions
bull Placement of prophylactic mesh at the time of index surgery
Decreased odds of developing a parastomal hernia
Decreased odds of requiring subsequent surgical repair of hernia
Not associated with increased odds of complications or stoma specific complications
Questions
patels2kghkarinet
epipatelmd
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018

Risk of Bias
bull 2 Studies with low risk of bias across all assessed categories
bull 2 Studies with unclear risk of bias Unclear allocation concealment Unclear if assessors were blinded
bull 3 Studies had high risk of bias in at least one category High loss to follow up (35) Per Protocol Analysis (Not ITT) Changed Diagnostic Criteria partway through the
study
Parastomal Hernia
bull Reduced Odds with Prophylactic Mesh
OR 022 95CI 009 ndash 049 I2 = 49
Parastomal Hernia requiring
subsequent surgerybull Reduced odds with Prophylactic Mesh
OR 031 95CI 011 ndash 086 I2 = 0
Surgical Complications (All)
bull No difference in overall complications (P = 023)
Stoma Specific Complications
bull No difference in stoma specific complications (P = 024)
Subgroup Analyses (Hernia Formation)bull No subgroup effect of mesh position (P = 093)
bull No subgroup effect noted based on how hernia was diagnosed (P = 085)
Subgroup Analysisbull A significant subgroup effect was found based on
biologic vs synthetic permanent mesh (P = 002)
Discussion
bull Prophylactic Mesh associated with
A decrease in parastomal hernia after at least 1 year of follow up (Primary Outcome)
A decrease in subsequent surgical repair (Secondary Outcome)
bull Not associated with
Surgical or Stoma Specific Complications
Limitations
bull Heterogeneity
Primary outcome showed moderate heterogeneity (I2 = 49)
Reduced with Subgroup analysis based on biologic vs synthetic mesh (I2 = 15)
Limitations
bull Inconsistent complication Rates
Overall Complications Between 0 - gt90
Stoma Specific Complications Between 0 -gt50
bull Widely varying definitions of complications
Vs ldquoComplicationsrdquo
Conclusions
bull Placement of prophylactic mesh at the time of index surgery
Decreased odds of developing a parastomal hernia
Decreased odds of requiring subsequent surgical repair of hernia
Not associated with increased odds of complications or stoma specific complications
Questions
patels2kghkarinet
epipatelmd
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018

Parastomal Hernia
bull Reduced Odds with Prophylactic Mesh
OR 022 95CI 009 ndash 049 I2 = 49
Parastomal Hernia requiring
subsequent surgerybull Reduced odds with Prophylactic Mesh
OR 031 95CI 011 ndash 086 I2 = 0
Surgical Complications (All)
bull No difference in overall complications (P = 023)
Stoma Specific Complications
bull No difference in stoma specific complications (P = 024)
Subgroup Analyses (Hernia Formation)bull No subgroup effect of mesh position (P = 093)
bull No subgroup effect noted based on how hernia was diagnosed (P = 085)
Subgroup Analysisbull A significant subgroup effect was found based on
biologic vs synthetic permanent mesh (P = 002)
Discussion
bull Prophylactic Mesh associated with
A decrease in parastomal hernia after at least 1 year of follow up (Primary Outcome)
A decrease in subsequent surgical repair (Secondary Outcome)
bull Not associated with
Surgical or Stoma Specific Complications
Limitations
bull Heterogeneity
Primary outcome showed moderate heterogeneity (I2 = 49)
Reduced with Subgroup analysis based on biologic vs synthetic mesh (I2 = 15)
Limitations
bull Inconsistent complication Rates
Overall Complications Between 0 - gt90
Stoma Specific Complications Between 0 -gt50
bull Widely varying definitions of complications
Vs ldquoComplicationsrdquo
Conclusions
bull Placement of prophylactic mesh at the time of index surgery
Decreased odds of developing a parastomal hernia
Decreased odds of requiring subsequent surgical repair of hernia
Not associated with increased odds of complications or stoma specific complications
Questions
patels2kghkarinet
epipatelmd
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018
Parastomal Hernia requiring
subsequent surgerybull Reduced odds with Prophylactic Mesh
OR 031 95CI 011 ndash 086 I2 = 0
Surgical Complications (All)
bull No difference in overall complications (P = 023)
Stoma Specific Complications
bull No difference in stoma specific complications (P = 024)
Subgroup Analyses (Hernia Formation)bull No subgroup effect of mesh position (P = 093)
bull No subgroup effect noted based on how hernia was diagnosed (P = 085)
Subgroup Analysisbull A significant subgroup effect was found based on
biologic vs synthetic permanent mesh (P = 002)
Discussion
bull Prophylactic Mesh associated with
A decrease in parastomal hernia after at least 1 year of follow up (Primary Outcome)
A decrease in subsequent surgical repair (Secondary Outcome)
bull Not associated with
Surgical or Stoma Specific Complications
Limitations
bull Heterogeneity
Primary outcome showed moderate heterogeneity (I2 = 49)
Reduced with Subgroup analysis based on biologic vs synthetic mesh (I2 = 15)
Limitations
bull Inconsistent complication Rates
Overall Complications Between 0 - gt90
Stoma Specific Complications Between 0 -gt50
bull Widely varying definitions of complications
Vs ldquoComplicationsrdquo
Conclusions
bull Placement of prophylactic mesh at the time of index surgery
Decreased odds of developing a parastomal hernia
Decreased odds of requiring subsequent surgical repair of hernia
Not associated with increased odds of complications or stoma specific complications
Questions
patels2kghkarinet
epipatelmd
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018

Surgical Complications (All)
bull No difference in overall complications (P = 023)
Stoma Specific Complications
bull No difference in stoma specific complications (P = 024)
Subgroup Analyses (Hernia Formation)bull No subgroup effect of mesh position (P = 093)
bull No subgroup effect noted based on how hernia was diagnosed (P = 085)
Subgroup Analysisbull A significant subgroup effect was found based on
biologic vs synthetic permanent mesh (P = 002)
Discussion
bull Prophylactic Mesh associated with
A decrease in parastomal hernia after at least 1 year of follow up (Primary Outcome)
A decrease in subsequent surgical repair (Secondary Outcome)
bull Not associated with
Surgical or Stoma Specific Complications
Limitations
bull Heterogeneity
Primary outcome showed moderate heterogeneity (I2 = 49)
Reduced with Subgroup analysis based on biologic vs synthetic mesh (I2 = 15)
Limitations
bull Inconsistent complication Rates
Overall Complications Between 0 - gt90
Stoma Specific Complications Between 0 -gt50
bull Widely varying definitions of complications
Vs ldquoComplicationsrdquo
Conclusions
bull Placement of prophylactic mesh at the time of index surgery
Decreased odds of developing a parastomal hernia
Decreased odds of requiring subsequent surgical repair of hernia
Not associated with increased odds of complications or stoma specific complications
Questions
patels2kghkarinet
epipatelmd
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018

Stoma Specific Complications
bull No difference in stoma specific complications (P = 024)
Subgroup Analyses (Hernia Formation)bull No subgroup effect of mesh position (P = 093)
bull No subgroup effect noted based on how hernia was diagnosed (P = 085)
Subgroup Analysisbull A significant subgroup effect was found based on
biologic vs synthetic permanent mesh (P = 002)
Discussion
bull Prophylactic Mesh associated with
A decrease in parastomal hernia after at least 1 year of follow up (Primary Outcome)
A decrease in subsequent surgical repair (Secondary Outcome)
bull Not associated with
Surgical or Stoma Specific Complications
Limitations
bull Heterogeneity
Primary outcome showed moderate heterogeneity (I2 = 49)
Reduced with Subgroup analysis based on biologic vs synthetic mesh (I2 = 15)
Limitations
bull Inconsistent complication Rates
Overall Complications Between 0 - gt90
Stoma Specific Complications Between 0 -gt50
bull Widely varying definitions of complications
Vs ldquoComplicationsrdquo
Conclusions
bull Placement of prophylactic mesh at the time of index surgery
Decreased odds of developing a parastomal hernia
Decreased odds of requiring subsequent surgical repair of hernia
Not associated with increased odds of complications or stoma specific complications
Questions
patels2kghkarinet
epipatelmd
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018
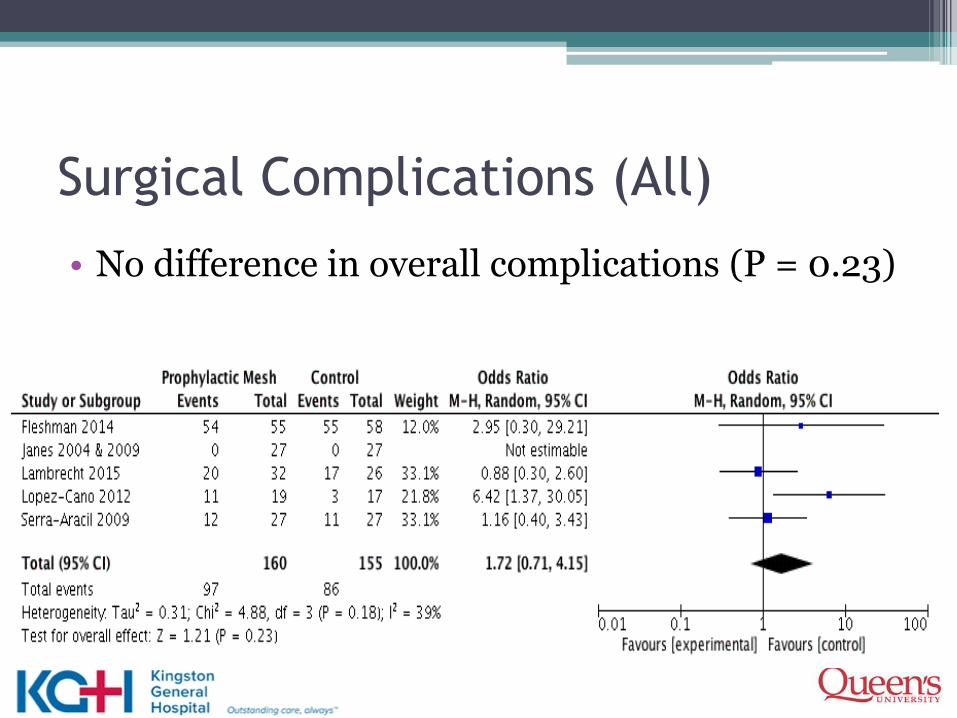
Subgroup Analyses (Hernia Formation)bull No subgroup effect of mesh position (P = 093)
bull No subgroup effect noted based on how hernia was diagnosed (P = 085)
Subgroup Analysisbull A significant subgroup effect was found based on
biologic vs synthetic permanent mesh (P = 002)
Discussion
bull Prophylactic Mesh associated with
A decrease in parastomal hernia after at least 1 year of follow up (Primary Outcome)
A decrease in subsequent surgical repair (Secondary Outcome)
bull Not associated with
Surgical or Stoma Specific Complications
Limitations
bull Heterogeneity
Primary outcome showed moderate heterogeneity (I2 = 49)
Reduced with Subgroup analysis based on biologic vs synthetic mesh (I2 = 15)
Limitations
bull Inconsistent complication Rates
Overall Complications Between 0 - gt90
Stoma Specific Complications Between 0 -gt50
bull Widely varying definitions of complications
Vs ldquoComplicationsrdquo
Conclusions
bull Placement of prophylactic mesh at the time of index surgery
Decreased odds of developing a parastomal hernia
Decreased odds of requiring subsequent surgical repair of hernia
Not associated with increased odds of complications or stoma specific complications
Questions
patels2kghkarinet
epipatelmd
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018

Subgroup Analysisbull A significant subgroup effect was found based on
biologic vs synthetic permanent mesh (P = 002)
Discussion
bull Prophylactic Mesh associated with
A decrease in parastomal hernia after at least 1 year of follow up (Primary Outcome)
A decrease in subsequent surgical repair (Secondary Outcome)
bull Not associated with
Surgical or Stoma Specific Complications
Limitations
bull Heterogeneity
Primary outcome showed moderate heterogeneity (I2 = 49)
Reduced with Subgroup analysis based on biologic vs synthetic mesh (I2 = 15)
Limitations
bull Inconsistent complication Rates
Overall Complications Between 0 - gt90
Stoma Specific Complications Between 0 -gt50
bull Widely varying definitions of complications
Vs ldquoComplicationsrdquo
Conclusions
bull Placement of prophylactic mesh at the time of index surgery
Decreased odds of developing a parastomal hernia
Decreased odds of requiring subsequent surgical repair of hernia
Not associated with increased odds of complications or stoma specific complications
Questions
patels2kghkarinet
epipatelmd
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018
Discussion
bull Prophylactic Mesh associated with
A decrease in parastomal hernia after at least 1 year of follow up (Primary Outcome)
A decrease in subsequent surgical repair (Secondary Outcome)
bull Not associated with
Surgical or Stoma Specific Complications
Limitations
bull Heterogeneity
Primary outcome showed moderate heterogeneity (I2 = 49)
Reduced with Subgroup analysis based on biologic vs synthetic mesh (I2 = 15)
Limitations
bull Inconsistent complication Rates
Overall Complications Between 0 - gt90
Stoma Specific Complications Between 0 -gt50
bull Widely varying definitions of complications
Vs ldquoComplicationsrdquo
Conclusions
bull Placement of prophylactic mesh at the time of index surgery
Decreased odds of developing a parastomal hernia
Decreased odds of requiring subsequent surgical repair of hernia
Not associated with increased odds of complications or stoma specific complications
Questions
patels2kghkarinet
epipatelmd
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018

Limitations
bull Heterogeneity
Primary outcome showed moderate heterogeneity (I2 = 49)
Reduced with Subgroup analysis based on biologic vs synthetic mesh (I2 = 15)
Limitations
bull Inconsistent complication Rates
Overall Complications Between 0 - gt90
Stoma Specific Complications Between 0 -gt50
bull Widely varying definitions of complications
Vs ldquoComplicationsrdquo
Conclusions
bull Placement of prophylactic mesh at the time of index surgery
Decreased odds of developing a parastomal hernia
Decreased odds of requiring subsequent surgical repair of hernia
Not associated with increased odds of complications or stoma specific complications
Questions
patels2kghkarinet
epipatelmd
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018

Limitations
bull Inconsistent complication Rates
Overall Complications Between 0 - gt90
Stoma Specific Complications Between 0 -gt50
bull Widely varying definitions of complications
Vs ldquoComplicationsrdquo
Conclusions
bull Placement of prophylactic mesh at the time of index surgery
Decreased odds of developing a parastomal hernia
Decreased odds of requiring subsequent surgical repair of hernia
Not associated with increased odds of complications or stoma specific complications
Questions
patels2kghkarinet
epipatelmd
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018

Vs ldquoComplicationsrdquo
Conclusions
bull Placement of prophylactic mesh at the time of index surgery
Decreased odds of developing a parastomal hernia
Decreased odds of requiring subsequent surgical repair of hernia
Not associated with increased odds of complications or stoma specific complications
Questions
patels2kghkarinet
epipatelmd
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018
Conclusions
bull Placement of prophylactic mesh at the time of index surgery
Decreased odds of developing a parastomal hernia
Decreased odds of requiring subsequent surgical repair of hernia
Not associated with increased odds of complications or stoma specific complications
Questions
patels2kghkarinet
epipatelmd
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018

Questions
patels2kghkarinet
epipatelmd
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018
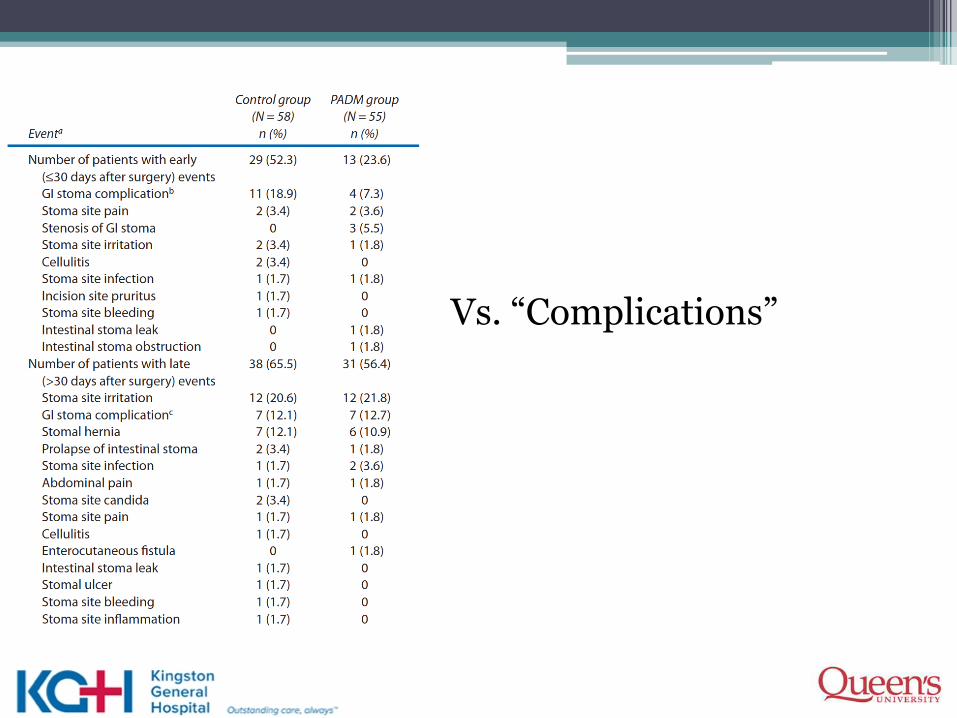
References to Included Studies1 Janes A Cengiz Y and Israelsson L A (2004) Randomized clinical trial of the use of a prosthetic mesh to
prevent parastomal hernia British Journal of Surgery 91 280-282 doi 101002bjs44172 Serra-Aracil X Bombardo-Junca J Moreno-Matias J Darnell A Mora-Lopez L Alcantara-Moral M
Ayguavives-Garnica I and Navarro-Soto S (2009) Randomized controlled prospective trial of the use of a mesh to prevent parastomal hernia Annals of Surgery 249 583-587 doi 101097SLA0b013e31819ec809
3 Hammond T M Huang A Prosser K Frye J N and Williams N S (2008) Parastomal hernia prevention using a novel collagen implant a randomised controlled phase 1 study Hernia 12 475-481 doi 101007s10029-008-0383-
4 Lambrecht J R Larsen S G Reiertsen O Vaktskjold A Julsrud L and Flatmark K (2015) Prophylactic mesh at end-colostomy construction reduces parastomal hernia rate a randomized trial Colorectal Diseases 17 191-197 doi 101111codi13065
5 Fleshman J W Beck D E Hyman N Wexner S D Bauer J and George V (2014) A prospective multicenter randomized controlled study of non-cross-linked porcine acellular dermal matrix fascial sublayfor parastomal reinforcement in patients undergoing surgery for permanent abdominal wall ostomies Diseases of the Colon amp Rectum 57 623-631 doi 101097DCR0000000000000106
6 Lopez-Cano M Lozoya-Trujillo R Quiroga S Sanchez J L Vallribera F Martiacute M Jimenez L M Armengol-Carrasco M and Espiacuten E (2012) Use of a prosthetic mesh to prevent parastomal hernia during laparoscopic abdominoperineal resection a randomized controlled trial Hernia 16 661-667 doi 101007s10029-012-0952-z
7 Vierimaa M Klintrup K Biancari F Victorzon M Carpelan-Holmstroumlm M Koumlssi J Kellokumpu I Rauvala E Ohtonen P Maumlkelauml J and Rautio T (2015) Prospective Randomized Study on the Use of a Prosthetic Mesh for Prevention of Parastomal Hernia of Permanent Colostomy Diseases of the Colon amp Rectum 58 943-949 doi 101097DCR0000000000000443
8 Janes A Cengiz Y and Israelsson L A (2009) Preventing parastomal hernia with a prosthetic mesh a 5-year follow-up of a randomized study World Journal of Surgery 33 118-121 doi 101007s00268-008-9785-4
References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018

References1 Cingi A Cakir T Sever A and Aktan A O (2006) Enterostomy site hernias a clinical and computerized
tomographic evaluation Diseases of the Colon amp Rectum 49 1559-1563 doi 101007s10350-006-0681-4
2 Pilgrim C H McIntyre R and Bailey M (2010) Prospective audit of parastomal hernia prevalence and associated comorbidities Diseases of the Colon amp Rectum 53 71-76 doi 101007DCR0b013e3181bdee8c
3 Carne P W Robertson G M and Frizelle F A (2003) Parastomal hernia British Journal of Surgery 90 784-793 doi 101002bjs4220
4 Shabbir J Chaudhary B N and Dawson R (2012) A systematic review on the use of prophylactic mesh during primary stoma formation to prevent parastomal hernia formation Colorectal Disease 14 931-936 doi 101111j1463-1318201102835x
5 Hansson BM1 Morales-Conde S Mussack T Valdes J Muysoms FE Bleichrodt RP The laparoscopic modified Sugarbaker technique is safe and has a low recurrence rate a multicenter cohortstudy Surg Endosc 2013 Feb27(2)494-500
6 Figure 2 Schematic drawings of the anatomic positions of mesh placement - Scientific Figure on ResearchGate Available from httpswwwresearchgatenetfigure271560312_fig2_Figure-2-Schematic-drawings-of-the-anatomic-positions-of-mesh-placement-in-incisional [accessed Jun 20 2016]
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018
Summary of FindingsSummary of findings
Prophylactive Mesh compared to No Mesh for reducing parastomal hernia in patients with an ostomy
Patient or population reducing parastomal hernia in patients with an ostomy Setting Patients undergoing creation of permanent or temporary ostomy Intervention Prophylactive Mesh Comparison No Mesh
Outcomes Anticipated absolute effects (95 CI)
Relative effect (95 CI)
of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with No Mesh
Risk with Prophylactive Mesh
Parastomal Hernia (Hernia) assessed with Clinical or Radiologic Diagnosis follow up range 12 months to 60 months
Study population OR 023
(010 to 052)
385 (7 RCTs)
⨁⨁⨁
MODERATE 1
1 Quality downgraded for serious concerns regarding a) risk of bias (3 of 7 studies with high risk of bias) b) Inconsistency (moderate heterogeneity) Quality upgraded for a) Large effect
376 per 1000
122 per 1000 (57 to 239)
The risk in the intervention group (and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95 CI) CI Confidence interval OR Odds ratio
GRADE Working Group grades of evidence High quality We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality We are moderately confident in the effect estimate The true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different Low quality Our confidence in the effect estimate is limited The true effect may be substantially different from the estimate of the effect Very low quality We have very little confidence in the effect estimate The true effect is likely to be substantially different from the estimate of effect
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018
Risk of Bias
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75 100
Low risk of bias Unclear risk of bias High risk of bias
Outcome Assessors Not blinded (4)
Loss to Follow up ~35 (5)
1 Changed diagnostic Criteria (4)
2 Per protocol analysis (2)
Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018

Onlay
Sublay
Intraperitoneal
Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018

Techniques
bull Keyhole technique vs Sugarbaker Technique [1]
1 Hansson Surg Endosc 2013
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018
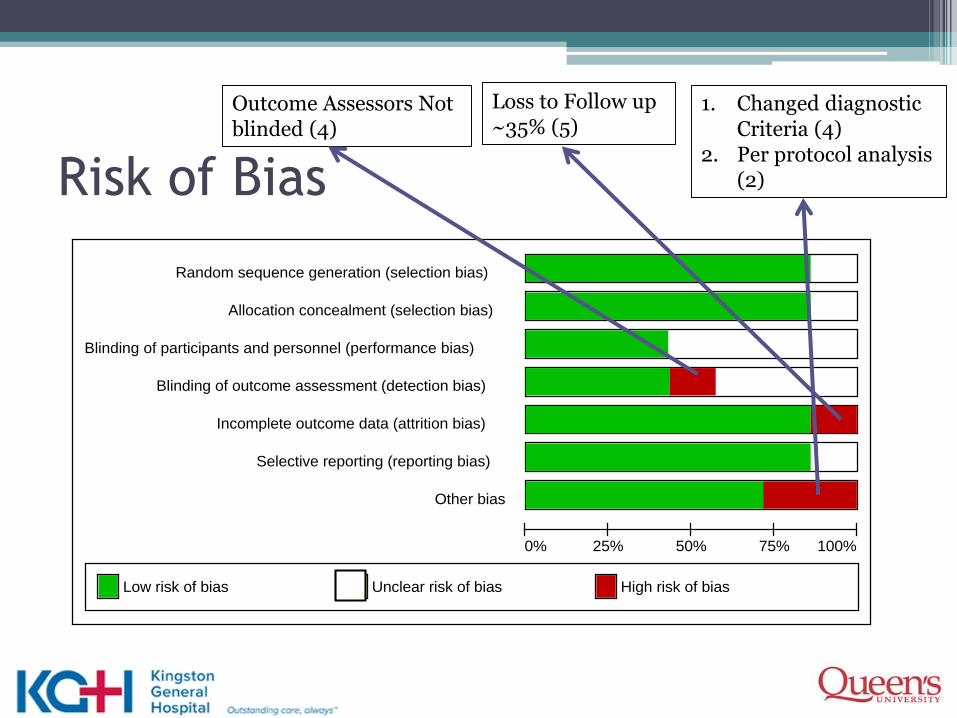
Table 1
Study N Pathology Type of Stoma Type of Mesh
Mesh
Placement
Follow Up
Duration
(Months) Hernia Diagnosis
Fleshman 2014 113Both Benign and
Malignant Colorectal
63 Colostomy
37 Ileostomy
100 Permanent
BiologicSublay
Keyhole24
Physical Exam
confirmed with CT
Scan
Hammond 2008 20Both Benign and
Malignant Colorectal
Not described
40 PermanentBiologic
Preperitoneal
Keyhole12
Physical Exam +-
Imaging
Janes 2004 amp 2009 54Both Benign and
Malignant Colorectal
Permanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole60 Physical Exam
Lambrecht 2015 58 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Keyhole40 Routine CT Scan
Lopez-Cano 2012 36 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Serra - Aracil 2009 54 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Sublay
Uncleargt13 Routine CT Scan
Vierimaa 2015 70 Malignant Disease OnlyPermanent
Colostomy onlySynthetic non-absorbable
Intraperitoneal
Keyhole12 Routine CT Scan
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018
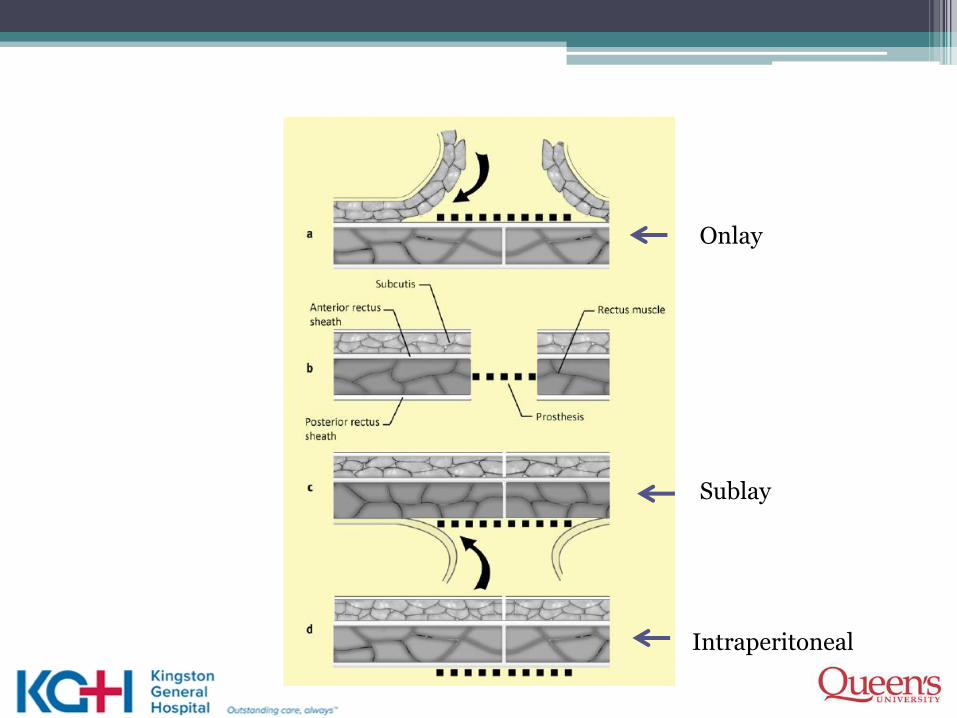
Ann R Coll Surg Engl 2016 Jun 81-10 [Epub ahead of print]
Prophylactic mesh use during primary stoma formation to
prevent parastomal hernia
Cornille JB1 Pathak S1 Daniels IR1 Smart NJ1
INTRODUCTION Parastomal hernia (PSH) is a common problem following stoma formation The optimal technique for stoma formation is unknown although recent studies have focused on whether placement of prophylactic mesh at stoma formation can reduce PSH rates The aim of this study was to systematically review use of prophylactic mesh versus no mesh with regard to occurrence of PSH and peristomal complications
METHODS A systematic search was performed using PubMed Embasetrade and the Cochrane Library to identify randomised controlled trials that analysed placement of prophylactic mesh versus no mesh at time of initial surgery Meta-analysis was performed using random effects methods
RESULTS A total of 506 studies were identified by our search strategy Of these 8 studies were included involving 430 patients (217 mesh vs 213 no mesh) Prophylactic mesh placement resulted in a significantly lower rate of PSH formation (42217 [194] vs 92213 [432]) with a combined risk ratio of 040 (95 confidence interval [CI] 021-075 p=0004) Placement of prophylactic mesh did not result in increased peristomal complications (15218 [69] vs 16227 [70]) with a combined risk ratio of 10 (95 CI 049-201 p=0990)
CONCLUSIONS Prophylacticplacement of mesh at primary stoma formation may reduce the incidence of PSH without an increase in peristomal complications However the overall quality of the randomised controlled trials included in the meta-analysis was poor and should prompt caution regarding the applicability of the findings of the individual studies and the meta-analysis to everyday practice
World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018

World J Surg 2016 May 23 [Epub ahead of print]
Efficacy of Prophylactic Mesh in End-Colostomy Construction A Systematic
Review and Meta-analysis of Randomized Controlled Trials
Wang S1 Wang W2 Zhu B3 Song G3 Jiang C3
bull BACKGROUNDbull Parastomal hernia is a very common complication after colostomy especially end-colostomy It is unclear
whether prophylactic placement of mesh at the time of stoma formation could prevent parastomal hernia formation after surgery for rectal cancer A systematic review and meta-analysis were conducted to evaluate the efficacy of prophylactic mesh in end-colostomy construction
bull METHODSbull PubMed Embase and the Cochrane Library were searched covering records entered from their
inception to September 2015 Randomized controlled trials (RCTs) comparing stoma with mesh to stoma without mesh after surgery for rectal cancer were included The primary outcome was the incidence of parastomal hernia Pooled risk ratios (RR) with 95 confidence intervals (CI) were obtained using random effects models
bull RESULTSbull Six RCTs containing 309 patients were included Parastomal hernia occurred in 244 (38 of 156) of
patients with mesh and 503 (77 of 153) of patients without mesh Meta-analysis showed a lower incidence of parastomal hernia (RR 042 95 CI 022-082) and reoperation related to parastomalhernia (RR 023 95 CI 006-089) in patients with mesh Stoma-related morbidity was similar between mesh group and non-mesh group (RR 065 95 CI 033-130)
bull CONCLUSIONSbull Prophylactic placement of a mesh at the time of a stoma formation seems to be associated with a
significant reduction in the incidence of parastomal hernia and reoperation related to parastomal hernia after surgery for rectal cancer but not the rate of stoma-related morbidity However the results should be interpreted with caution because of the heterogeneity among the studies
Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018

Hernia 2015 Oct 28 [Epub ahead of print]
Prophylactic mesh placement to prevent parastomal hernia early results of a prospective
multicentre randomized trial
Brandsma HT1 Hansson BM2 Aufenacker TJ3 van Geldere D4 van Lammeren FM5 Mahabier
C6 Steenvoorde P7 de Vries Reilingh TS8 Wiezer RJ9 de Wilt JH10 Bleichrodt RP2 Rosman C2
bull PURPOSEbull Parastomal hernia (PSH) is a common complication after colostomy formation Recent studies indicate
that mesh implantation during formation of a colostomy might prevent a PSH To determine if placement of a retromuscular mesh at the colostomy site is a feasible safe and effective procedure in preventing a parastomal hernia we performed a multicentre randomized controlled trial in 11 large teaching hospitals and three university centres in The Netherlands
bull METHODSbull Augmentation of the abdominal wall with a retromuscular light-weight polypropylene mesh (Parietene
Lighttrade Covidien) around the trephine was compared with traditional colostomy formation Patients undergoing elective open formation of a permanent end-colostomy were eligible 150 patients were randomized between 2010 and 2012 Primary endpoint of the PREVENT trial is the incidence of parastomal hernia Secondary endpoints are morbidity pain quality of life mortality and cost-effectiveness This article focussed on the early results of the PREVENT trial and therefore operation time postoperative morbidity pain and quality of life were measured
bull RESULTSbull Outcomes represent results after 3 months of follow-up A total of 150 patients were randomized Mean
operation time of the mesh group (N = 72) was significantly longer than in the control group (N = 78) (1826 vs 1568 min P = 0018) Four (27 ) peristomal infections occurred of which one (14 ) in the mesh group No infection of the mesh occurred Most of the other infections were infections of the perineal wound equally distributed over both groups No statistical differences were discovered in stoma or mesh-related complications fistula or stricture formation pain or quality of life
bull CONCLUSIONSbull During open and elective formation of an end-colostomy primary placement of a retromuscular light-
weight polypropylene mesh for prevention of a parastomal hernia is a safe and feasible procedure The PREVENT trial is registered at httpwwwtrialregisternltrialregadminrctviewaspTC=2018