promoting physical activity - d.umn.edudmillsla/courses/exercise adherence/documents... ·...
TRANSCRIPT

Unit III: Chapters 8-11 & 17-19 1
Promoting Physical Activity
Individual Level Intervention StrategiesGroup Level Intervention StrategiesCommunity Level Intervention Strategies
Unit III: Chapters 8-11 & 17-19 2
Individual Intervention Strategies

Unit III: Chapters 8-11 & 17-19 3
Types of Interventions
Behavior modificationReinforcementGoal settingContractsClient profiling (e.g. barriers to exercise)Self-monitoring(e.g. logs, fitness testing)

Unit III: Chapters 8-11 & 17-19 4
Types of Interventions
Health EducationBenefits of exercise
Health risk appraisalConfronting the client about their risk
Exercise prescriptionDuration, intensity, frequencyProgression
Physical Education Programs
Unit III: Chapters 8-11 & 17-19 5
Individual InterventionsWhat chance will one adhere to exercise in the absence of an interventionBenefits of an intervention program was:
Identical for both genders, across ages, and race.Greater for healthy clients then non-healthy
Small to moderate effect size for people who were high risk for CV disease
Found to increase adherence rates by as much as 38%

Unit III: Chapters 8-11 & 17-19 6
Which type of intervention is the most important?
Behavior modification had a very largeeffect size on increasing physical activity where as all others approaches were small.

Unit III: Chapters 8-11 & 17-19 7
How should the intervention be delivered?
Mediated Interventions were more effective then face-to-faceInterventions delivered in groups were better then those delivered individuallyLarger in non-supervised than supervisedInterventions delivered in community settings had greatest impact then schools, home, work site and health care settings.

Unit III: Chapters 8-11 & 17-19 8
Delivery (continued!)
Interactive software over the computer has been shown be an effective intervention.
Webcam’sUse the web & internet

Unit III: Chapters 8-11 & 17-19 9
Exercise Prescription Intervention
Interventions that targeted a more active leisure time lifestyle was greater then specific strength and/or aerobic exercise programming.Low-intensity PA was greater then high intensity PA. Shorter exercise bouts were greater than longer.
“It would seem that people are more likely to be physically activity if the behavior (exercise) is not perceived to be overly stressful and integrated into their lifestyle”

Unit III: Chapters 8-11 & 17-19 10
Behavior Modification Interventions
Based upon:Bandura’s Model of Self-efficacyTranstheortical or Stage Model

Unit III: Chapters 8-11 & 17-19 11
Self-Efficacy
Belief and expectations about how capable one is to perform PA or exercise to achieve an outcome( e.g. low weight, fitness).Major determinate of adherence in all the models

Unit III: Chapters 8-11 & 17-19 12
Self-EfficacySpecific to a type of exercise
High self-efficacy for following an aerobic routines increases the likelihood someone will enroll in an aerobic class but may not generalize to beginning a weight training class.High self-efficacy for low to moderate exercise dance but not high intensity, high impact aerobic dance
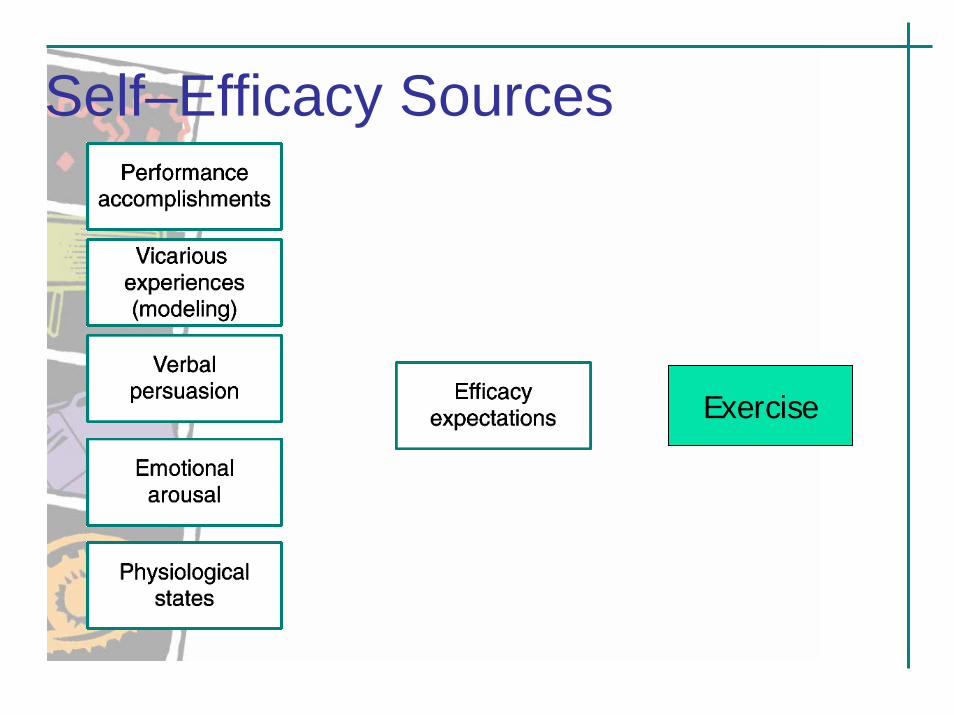
Self–Efficacy Sources
ExerciseExercise

Unit III: Chapters 8-11 & 17-19 14
Stage TheoryStage model reflects behavior change in exercise adherenceAssumes individuals in same stage are similar with respect to characteristics, such as level of PA.Therefore, there are specific behavior modification interventions that are appropriate at each stage.

Unit III: Chapters 8-11 & 17-19 15
Stage Model
1. Pre-contemplation2. Contemplation3. Preparation4. Action5. Maintenance

Unit III: Chapters 8-11 & 17-19 16
Precontemplation Stage
Individual are inactive and have no intention to start exercising. They are not seriously thinking about changing their level of PA within the next six months.

Unit III: Chapters 8-11 & 17-19 17
Behavior Interventions at Precontemplation Stage
Goal: To begin thinking about changing
Strategies:Provide them health information of benefitsReduce the actual and perceived costs & barriers
Intention to exercise is lowWillingness is lowSelf-efficacy is lowPerceived & actual access to facilities
Strengthen actual and perceived benefits of PA

Unit III: Chapters 8-11 & 17-19 18
Pre-contemplation Stage
Health pamphletsMedia advertisingAwareness of risksBenefits of exercisingHealth clinics & workshopsWellness seminars (topics such as weight loss and physical activity)

Unit III: Chapters 8-11 & 17-19 19
Contemplation Stage
Individuals are also inactive, but they intend to start regular exercise within the next six months.

Unit III: Chapters 8-11 & 17-19 20
Behavior Intervention at Contemplation State
Goal: To adopt regular exercise
StrategiesMarketing and media campaigns with accurate informationActivities to increase self-efficacy
Modeling, demonstrating, verbal persuasionEvaluate pros and cons of exercise

Unit III: Chapters 8-11 & 17-19 21
Decision Balance SheetPositive Negative

Unit III: Chapters 8-11 & 17-19 22
Preparation Stage
Individuals are active below the criterion level (CDC or ASCM) but intend to become more active in near future (1 month)Starters or irregular exercisers

Unit III: Chapters 8-11 & 17-19 23
Intervention for Preparation Stage
Goals: To adopt regular exercise at criterion levels
StrategiesAssessment of physical and psychosocial traitsGoal SettingEvaluate one’s environment and social supportEvaluate one’s barriers to modifying behavior

Unit III: Chapters 8-11 & 17-19 24
Preparation StrategiesSelf-Monitoring activities
Weekly workout progress logComputer programs that record your workouts
Self-monitoring exerciser checklist of type, mode, intensity of exercise, time, distance, heart rate, number of steps, kcal, etc.
Cue controlsStarter Program
Unit III: Chapters 8-11 & 17-19 25
Cue Controls
Have a set time for PASeparate PA from other activitiesPA is pleasant surroundingsSeek to spend time with friendsExercise postersModeling effect from spouse
Unit III: Chapters 8-11 & 17-19 26
Starter Program3-5 METS (low in intensity)Establish a exercise habit3 days a week!Just do it! 6-8 weeks!Short in duration
Aerobic 10 -15 minutesWeight 7-10 stations; 8-15 reps.
Gradually work on duration not intensity.Client choiceKeep a logBefore and after (Show benefit in weight, inches, etc.)

Unit III: Chapters 8-11 & 17-19 27
Action Stage
Individual engaged in regular exercise at the criterion level for less than six months.This is the least stable stage are are at great risk of relapse.

Unit III: Chapters 8-11 & 17-19 28
Assessment Physiological
Medical HistoryExercise restrictionsResting HR/BPBMI (obesity)Body Fat %Functional capacityDietary information
PsychosocialExercise HistorySelf-efficacyBarriers to exerciseExercise thoughtsStage of changeMeasures of stress, depression, & anxietyGoals

Unit III: Chapters 8-11 & 17-19 29
Psychosocial ThemeDetermine one’s risk for non-adherence:
Based on assessmentsExercise thoughts, level of self-efficacy, etc.
OccupationLevel of activity at work, time demands, and flexible schedule
StressLevel of job stress and style of coping with stress.
Social SupportLevel of support from others, spouse, etc.
Attendence RateFrequency in attending PA faculty or class.
GoalsVague in nature or specific
Unit III: Chapters 8-11 & 17-19 30
Interventions at Action StageGoal: To establish exercise as a habit
Strategies:Rewards and punishment
Contingency contracts
Slippage controlBoredom, lack of time, laziness, vacations, and illness
Proper exercise prescription

Unit III: Chapters 8-11 & 17-19 31
Contracts
I will:______I will enlist the help of:____My responsibilities are:______My helper’s responsibilities are:____My reward:____My punishment:____

Unit III: Chapters 8-11 & 17-19 32
Effective Rewards What kinds of things do you like to have?What are your major interests? Hobbies?Who do you like to be with?What do you do for fun?What do you do to relax?What makes you feel good?What would you hate to lose?

Unit III: Chapters 8-11 & 17-19 33
Slippage ControlTime management trainingStress management trainingBarriers to exercise
Tape the TV showBackup Plan (type & place)
Swimming pool not open I will walk on treadmillSnowing can’t walk, put on a aerobic tape

Unit III: Chapters 8-11 & 17-19 34
Maintenance Stage
Individuals who have been exercising regularly for more than six months.Risk of relapse is low.

Unit III: Chapters 8-11 & 17-19 35
Intervention at Maintenance Stage
Re-evaluate goals at regular intervals every 6-8 weeks.ACSM Exercise prescription GuidelinesVariety of exercise routines

Unit III: Chapters 8-11 & 17-19 36
Group level Strategies
Unit III: Chapters 8-11 & 17-19 37
Group Level Interventions
50% of people who come to private fitness clubs, community centers, universities, and etc., drop out in 3-6 months.Goal is to keeping them together and get them to interact toward a common goal!!---Become physically involved and fit

Unit III: Chapters 8-11 & 17-19 38
Dyersville Experience
450 participants lost a combined 7,500 pounds
Each week, entire team stepped onto a giant truck scale to monitor their progress
Example of Group level intervention that worked but WHY!!

Unit III: Chapters 8-11 & 17-19 39
Keys to Group CohesionEach PA groups must be made distinctive(foster feelings of distinctiveness)
Group name, group T-shirtHave the individuals be given the right to choose
Intensity, duration, and goals of programHave each experienced group member spend time helping new members
New members will learn individual sacrifice, techniques necessary for participation in the class, and gain skills

Unit III: Chapters 8-11 & 17-19 40
Keys to CohesionThe group should have a common goal
Lose weight, finish grandma’sIndividual accountability
Self-responsibility to do your partYou need to communicate
Positive, specific, sincere, frequent early, and focus on effort

Unit III: Chapters 8-11 & 17-19 41
Group-based InterventionsEnvironmental Strategies
Have group nameT-shirts, head bands, or shoelacesMake up posters/slogans for class
Group Structure StrategiesAbility group the members based on fitness levelProvide exercises for low, medium, & high impact exercisesEstablish a group goal

Unit III: Chapters 8-11 & 17-19 42
Group-based InterventionsGroup processes strategies
Set daily workout goalsNew group members should be assigned to another member who does exercises in the group on regular basisStress the effort not the outcome of exercises
Interaction StrategiesWork in small groups (3-5 sub groups max)Use more partner activitiesGet to know each other
Unit III: Chapters 8-11 & 17-19 43
Long-term consequencesGroup based interventions are effective in the short term but what happens when the class or program ends?
Do the clients stop exercising or regain the weight?Do the clients PA behavior regress?
Group-mediated programs maintain a higher rate of PA after the program then traditional exercise programs.

Unit III: Chapters 8-11 & 17-19 44
Community Intervention Strategies
Considered to be the most important!!

Unit III: Chapters 8-11 & 17-19 45
Community Level Interventions
Interventions that assist entire communities
Cross country trailsWalking & Biking TrailsOpen GymUniversity, School, & Community Projects

Unit III: Chapters 8-11 & 17-19 46
Key Factor in Community Intervention
Must be a shared common value to people in the community and by all institutions (government, private business, mass media, schools, university, etc)
Interventions must associate with their way of life in the regionIntervention must provide the people with some distinctiveness

Unit III: Chapters 8-11 & 17-19 47
Community PA Delivery Sites
SchoolsWork siteHealth Care Facilities

Unit III: Chapters 8-11 & 17-19 48
School Sites
Offered through Physical EducationSchool today offer few PE classesDuration of PE classes are usually short
School-based interventions have shownImprove knowledge and attitudes toward PADoes increase PA during PE classes but typically, are unsuccessful in increasing out-of-school PA
School based (CATCH) interventions has shown out-of-school PA increases.
Unit III: Chapters 8-11 & 17-19 49
Work Sites
Industry assumes that there is a link between worker productivity and fitness
To date work site PA interventions have had little impact.
Unit III: Chapters 8-11 & 17-19 50
Health Care SitesTouches both healthy and CV diseased populationMost primary prevention programs have had short term positive effects but no long term changes
PACE used DR’s as an intervention to promote PA supports the above results
Programs for CV diseased clients also indicated the above findings.

Unit III: Chapters 8-11 & 17-19 51
Let’s take a look at PACE
Example of Community Intervention Program at a Health Care Site

Unit III: Chapters 8-11 & 17-19 52
Project PACEhttp://www.paceproject.org

Unit III: Chapters 8-11 & 17-19 53
Project PACE
Physician-based Assessment and Counseling for Exercise
1990
Unit III: Chapters 8-11 & 17-19 54
Helping your patients improve their physical activity and nutrition behaviors is an important part of good primary medical care.

Unit III: Chapters 8-11 & 17-19 55
Project PACE is a practical system of matching physician counseling with patient readiness for physical activity.

Unit III: Chapters 8-11 & 17-19 56
Project PACE was developed in 1990 with support from the Centers for Disease Control and Prevention and San Diego State University.
Unit III: Chapters 8-11 & 17-19 57
Counseling patients about the value of physical activity and nutrition is one of many areas primary care physicians can positively impact the lifestyle choices of their patients.

Unit III: Chapters 8-11 & 17-19 58
Physicians counsel less often about physical activity than about other important health behaviors.

Unit III: Chapters 8-11 & 17-19 59
Barriers preventing physicians from counseling include:
Lack of knowledgeLack of third party reimbursementInadequate training & skills in health promotion & counselingLack of timeNeed standardized counseling protocols

Unit III: Chapters 8-11 & 17-19 60
PACE teaches physicians to spend precious counseling time targeting change.
Unit III: Chapters 8-11 & 17-19 61
PACE teaches physicians to use the most effective behavior-changing skills.

Unit III: Chapters 8-11 & 17-19 62
PACE focuses on moderate-intensity activities that are safe, effective, and familiar to most patients. They may be recommended without a sophisticated evaluation or complicated exercise prescription.

Unit III: Chapters 8-11 & 17-19 63
Why are physicians effective clinical coaches?
80% of Americans indicate that their primary source of health information is their personal physician. Americans average 2.7 visits per person per year. 60% of these visits are to a primary care physician.Physicians are in a unique position to improve their patients’ physical activity levels and have access to their medical records and health history.
Unit III: Chapters 8-11 & 17-19 64
Why are physicians effective clinical coaches?
Patient surveys show that patients want information about physical activity and that they feel their personal physician is a reliable source of information.

Unit III: Chapters 8-11 & 17-19 65
PACE MaterialsPhysician’s Manual: reference on the benefits of physical activity, risk assessment guide to PACE counseling and answering patients’ questions.Physical Activity Assessment Form: A questionnaire that determines the patient’s level of physical activity and their readiness to increase or maintain activity.

Unit III: Chapters 8-11 & 17-19 66
Physical Activity Levels Identified in the Self-Assessment Phase
Precontemplator (1) - People not willing to consider making a change. Contemplator (2 - 4) - People thinking about making a health behavior change, but don’t have the skills, knowledge, or incentive to do so.Active (5 - 11) - People in this stage are doing something!

Unit III: Chapters 8-11 & 17-19 67
How does the PACE scale work?
Patients select one statement that best describes their activity pattern.The number determines the physician’s counseling protocol.
1 Pre-contemplators 10%2 - 5 Contemplators 50%6 - 11 Actives 40%
Unit III: Chapters 8-11 & 17-19 68
How PACE worksThe entire PACE process requires only 2-5 minutes of interaction between physician and patient.Before seeing the physician, the patient completes the PACEassessment form.

Unit III: Chapters 8-11 & 17-19 69
How PACE Works
Based on the patient’s PACE score, the office staff gives him/her three PACE counseling protocols, which the patient completes in 2 -3 minutes before seeing the physician.The protocols are printed so that the patient can take home a copy and the physician has one for the medical record.
Unit III: Chapters 8-11 & 17-19 70
How PACE WorksThe outcome is strengthened by brief, inexpensive follow-up procedures such as a phone call from the office staff and/or a postcard.Follow-up prompts the patients to continue their activity program. Accountability.

Unit III: Chapters 8-11 & 17-19 71
Benefits of PACESimple and inexpensivePAR-Q identifies those at risk of a cardiovascular event.Roadblocks of exercise - Stages of Change theoryGuidelines for “moderate activity”developed by ACSM

Unit III: Chapters 8-11 & 17-19 72
Benefits of PACEScore relates directly to the counseling protocol to be used.Encourages follow-up assessmentLevels of both under-exercisers and over-exercisers are usedHelps to retain patients and build a good rapport
Unit III: Chapters 8-11 & 17-19 73
Summary and Key Findings
Conclusions: Physician-based counseling produced a moderate physical activity among previously sedentary patients.Conclusions: Physicians found PACE improved their confidence to counsel patients about physical activity in 1 - 5 minutes.

Unit III: Chapters 8-11 & 17-19 74
Community Wide Interventions
Legislative, Policy, and Community wide changes in PA
Naval Community ProjectStanford Five-City Project
Most power long lasting impact on individuals level of PA

Unit III: Chapters 8-11 & 17-19 75
Mass Media Interventions
Telephone based intervention in weight lossMailing interventionBoth intervention techniques were very positive.

Unit III: Chapters 8-11 & 17-19 76
CDC StrategiesPublic Policy
Increase budget toward recreationZoning & codes
EnvironmentRequire sidewalks Bike lanesOpen gyms, community centers
Physical EducationHave it in the school!Emphasis on fitnessIncrease frequency and duration
Health EducationBenefits of exercise
ExtracurricularIncrease access
Health ServicesHospitals need be involved!Doctors, nurses, PT’s & AT’s need to involved
Community ProgramsInvolve all institutionBe a common goal of community
Increase Parental InvolvementIncrease the Density of Personal Training

Unit III: Chapters 8-11 & 17-19 77
CDC Strategies
To change the physical activity patterns of a population, one should not rely on just one to see long term effects. Change occurs when a community implements all the strategies.

Unit III: Chapters 8-11 & 17-19 78
SummaryInterventions based on model of PA involvement are the best strategy.Behavioral modification interventions are the best.Stage theory and Bandura’s Self-efficacy models are key models today.Groups interventions relate highly to social cohesion.Community interventions are the most important.Health-care programs outweigh worksite or school site programs