prolotherapy is the iatrogenic stimulation of the wound healing and tissue repair process
TRANSCRIPT

Prolotherapy is the iatrogenic stimulation of the wound healing
and tissue repair process

PROLOTHERAPY or REGENERATIVE INJECTION
THERAPY RIT is an interventional technique for
treatment of chronic pain due to connective tissue diathesis by induction of collagen chemo-modulation through inflammatory, proliferative and regenerative/reparative responses mediated by multiple growth factors.

REGENERATIVE INJECTION THERAPY
Mechanism1. Mechanical transection of cells and matrix
induced by needle “trauma” stimulates an inflammatory cascade
2. Compression of cells by the extra-cellular volume of injected solution stimulates intracellular growth factors

REGENERATIVE INJECTION THERAPY
3. Chemomodulation of collagen through inflammatory proliferative, regenerative/reparative responses induced by the chemical properties of the proliferants and mediated by cytokines and multiple growth factors

Dextrose exposure to human periodontal fibroblasts
Elevates polypeptide growth factors within minutes to hours after injection
Causes cell multiplication and matrix formation

Human ligaments after injury
Elevated levels of PDGF, TGF-beta, EGF, bFGF and IGF

In vitro exposure of human cells to extra-cellular glucose
0.5% (normal intracellular concentration 1.1%) results in activation of 15 different gene segments within minutes to hours of exposure = growth factor production

Hypertonic Solutions Exposure of human and animal cells to
hypertonic solution has been found by several researchers to result in a rise of growth factors
This rise is more limited than with dextrose elevation and in studies comparing equal osmolar concentrations of glucose and mannitol, glucose caused more GF elevation

Effect on Disrepair Factors In osteoarthritis a variety of interleukins and
plasminogen activator are involved in damage to cartilaginous tissue
Dextrose exposed to human cells has been shown to decrease activity of interleukins 2, 6, and 10 and plasminogen activator
Not just growth factor production but limitation of destructive activity

REGENERATIVE INJECTION THERAPY
4. Chemoneuromodulation of peripheral nociceptors and antidromic, orhthodromic, sympathetic and axon reflex transmissions

REGENERATIVE INJECTION THERAPY
5. Modulation of local hemodynamics with changes in intra-osseous pressure leading to the reduction of pain (dextrose/lidocaine combination more prolonged action than lidocaine alone)

REGENERATIVE INJECTION THERAPY
6. A temporary repetitive stabilization of the painful hyper-mobile joints, induced by the inflammatory response to the proliferants, provides a better environment for regeneration and repair of affected ligaments and tendons.

Wound Healing

Prolotherapy is the iatrogenic stimulation of the wound healing
and tissue repair process

Wound Healing has distinct phases that overlap in
time.
InflammationGranulationRemodeling

Wound Healing has distinct phases that overlap in time.

Inflammation Phase
Coagulation cascade initiatedFibrin clot results in the release
cytokines and growth factors from platelets. Platelet derived growth factor (PDFG)Transforming growth factor- (TGF-)Platelet activating factor (PAF)

Inflammation Phase
Local fibrin clot serves as scaffolding for invading cellsNeutrophilsMonocytesFibroblastsEndothelial cells
Receptors on the cells and clot ensure selectivity of response

Inflammation Phase Attraction of cells to the wound by
chemotaxis is followed by functional activation.
Particularly important is the activation of the macrophages and lymphocytes.DebridementMatrix synthesisAngiogenesis

Inflammation Phase
Soft tissue injury releases many chemical mediators that sensitize the nociceptors = painHistamineProstaglandin E2Bradykinin
These are also the major activators of the macrophages
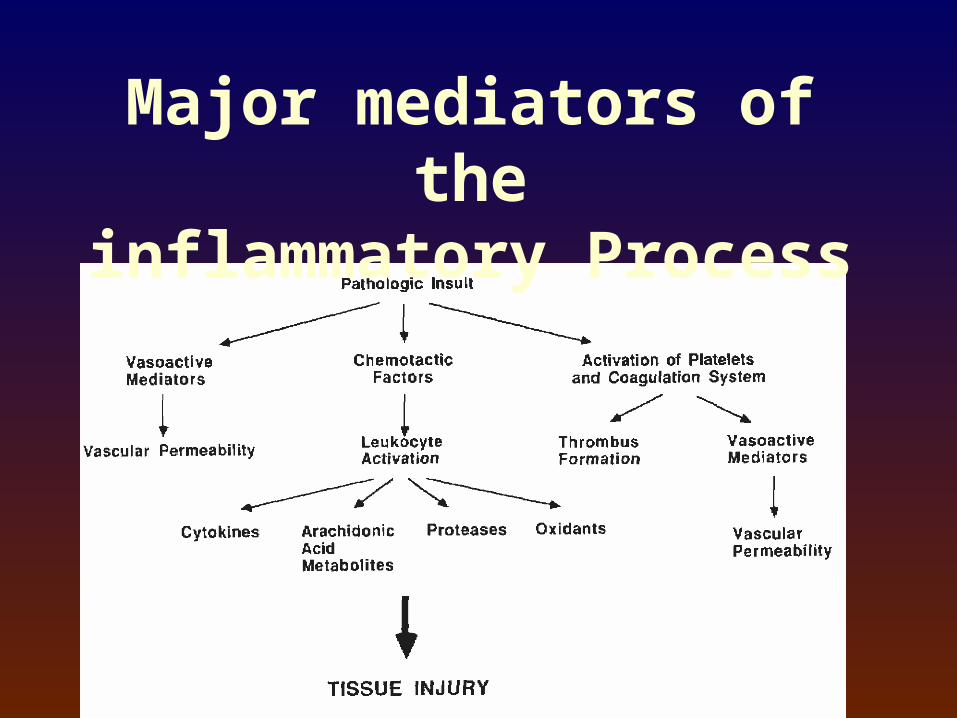
Major mediators of the
inflammatory Process

At the end of the inflammation phase the
production of the cytokine mediators ceases and the granulation phase begins

Granulation Phase
Dominated by the activity of the fibroblasts and endothelial cells beginning 100 hours after the injury
Macrophages, fibroblasts and blood vessels move into the wound space as a unit.

Granulation Phase
Fibroblasts construct new extra-cellular matrix (ECM) to support cellular growth.
Neovascularity supplies the oxygen and nutrients.

Granulation Phase Fibroblasts differentiate to myofibroblasts
which pull the wound together

Granulation Phase
At the end of the granulation phase the fibroblasts begin to produce collagen.
Net collagen synthesis is increased for 4-5 weeks during the remodeling phase.
Remodeling Phase Main feature is deposition of collagen in the
wound Fibroblasts under tensile stress produce
SM actin and as the stress increases they form adhesion complexes with the extracellular matrix
These cells predominate in connective tissue injuries

Remodeling Phase

Remodeling Phase This leads to connective tissue contracture that
is incremental and a true anatomical shortening of the extra cellular matrix (ECM).
As the ECM is remodeled, the myofibroblasts become surrounded by the new load-carrying matrix.
As myofibroblasts are shielded from the stress they disappear by apotosis.

Remodeling Phase The final ECM is not distinguishable from the
original by any analytical means. There is no scar tissue. This process gives animals the resources to
repair minor injuries in such away that they will have lost no capability to survive.

Pre prolotherapy Post prolotherapy
12 wks0 weeks

Remodeling Phase To complete healing of ligament and tendons,
movement and loading of the tissue is critical to a good outcome.
There is period of vulnerability when the curve of wound healing is plotted against pain and ligament strength.
Period of vulnerability is proportional to original severity of injury and expected demand.

Remodeling Phase

Chronic Injuries
May result from: Chronic postural dysfunctions Repetitive work Chronically contracted muscles responding
to pain such as in old ligament or enthesis injuries
Chronic Injuries
If present for years, it may take up to 1 or 2 years for the ligaments to heal and for the associated pain to finally settle down

The enthesis Normal tendons and ligaments (TL) share a
common feature where they attach to bone—the enthesis.
This site creates a firm union by splaying out the fibers to create a larger surface area.
The enthesis has 2-3 times the cross sectional area as the mid substance TL.

The enthesis
Two basic types differentiated by structure and locationFibrocartilaginousFibrous

Fibrocartilaginous
Found at apophyses and epiphysis of long bones and in short bones in hands and feet
Fibrocartilage cells and matrix are present at the attachment site.

Fibrous
Characteristic of tendons and ligaments that attach to the metaphases and diaphyses of long bones by dense fibrous connective tissue known as Sharpey’s fibers.

The enthesis
Bone and enthesis interlock Allowing for stress dissipation at
the attachment siteUn-calcified fibrocartilage
dissipates bending forces during insertional angle changes

Chronic Enthesis Injuries

Chronic Enthesis Injuries Consequence of chronic stress at enthesis is
tissue micro trauma with altered or incomplete tissue repair.
Orderly phased wound repair is absent or aborted in these areas of micro trauma because of hypoxia.
This is enthesopathy or tendinosis.

Enthesopathy & Tendinosis
Failed adaptation of the tendon or ligament to physical load and use
Designates these altered focal areas of degeneration.

ligament and tendon changes

Fissures and Cracks

Fatty & Hyaline Degeneration
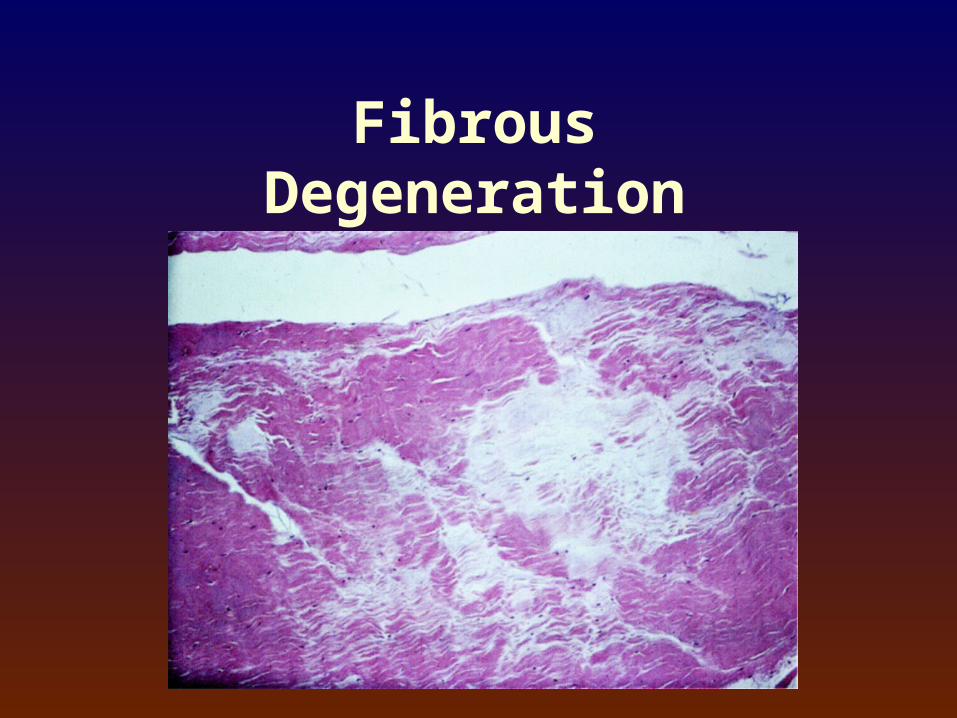
Fibrous Degeneration

Enthesopathy & Tendinosis
Enthesis is the most richly innervated region of a ligament or tendon.1. Myelinated A afferent fibers
2. Non myelinated C afferent fibers
(Sensitive to chemical mediators)

Pain & Soft Tissues
Soft tissue injury releases many
chemical mediators that sensitize
the nociceptorsHistamineProstaglandin E2Bradykinin

Pain & Soft Tissues

Pain & Soft Tissues
Effects of neural stimulation includeSpinal reflex contraction of flexor musclesFacilitation of the flexor reflex leading to
reflex muscle spasmInhibition of antagonistic musclesSensitization of nociceptors

Pain & Soft Tissues
The spinothalamic tract carries pain to the thalamus
Connections between thalamus and hypothalamus integrate the autonomic nervous system response

Pain effects on the brain
Hormones ReleasedGrowth Hormone - HypothalamusNeural Growth Factor Cortisol - Adrenal Cortex
Pain effects on the brain

Chronic Enthesopathy
Often painless in spite of degenerative changes Micro insults do not trigger release of growth
factors Pain does not develop until damage reaches an
area where vessels are present

Pain Moderators
Treating the pain without interfering with wound healing
Corticosteroids and NSAIDs effect wound healing and collagen repair
Pain Moderators
Eicosanoid biosynthesis begins afterTraumaInfection Inflammation

Trauma releases arachidonic acid from cell wall
Arachidonic acid is converted into eicosanoids mediated by two different pathways Cyclo-oxygenase
Prostaglandin Thromboxanes
Lipo-oxygenase Leukotrienes

Eicosanoid Pathways

Pain Moderators
In trauma there is a shift to the cyclo-oxygenase pathway

Pain Moderators
ProstaglandinsPotent stimulators of macrophagesStrong attractors of neutrophilsDegree of macrophage activation is
proportional to stimulus

Pain Moderators
NSAID’sInhibitor of the major cytokinin synthesis
pathwaysAlter the production of eicosanoids
ProstaglandinThromboxanesLeukotrienes

Pain Moderators

Pain Moderators
CorticosteroidsInhibit expression of the genes involved in
the inflammatory and immune response.These genes include those of the:
CytokinesChemokinesCell-surface receptorsAdhesion moleculesCyclo-oxygenase

Pain ModeratorsCorticosteroids alter gene expression in
two waysBinding directly to DNA acting to affect
transcription factorsBinding to and interfering with other
transcription factors

Pain Moderators
Glucocorticoid EffectsInjection into ligament and tendons
causes weakness and failure with less stress.*
Wiggins ME, et al. Healing characteristics of a type I collagenous structure treated with corticosteroids. Am J Sports Med 22:2790288, 1994.

Regenerative Injection Therapy
Inform the patient about wound healing Use narcotics for pain
SafeDose efficientFew side effects

Contraindications to RIT
1. Allergy to local anesthetic or proliferant solutions or their ingredients2. Acute non-reduced subluxations or dislocations3. Acute arthritis, bursitis or tendinitis, gout or rheumatoid arthritis

Contraindications to RIT
4. Recent onset of progressive neurological
deficit, neoplasm
5. Severe exacerbation of pain or lack of
improvement after local anesthetic blocks
6. Relative contraindications: central spinal
stenosis, lateral recess and neural
foraminal stenosis

Temperomandibular Joint Dysfunction
“Studies in the Paleopathology of Egypt” – Sir Marc Armand Ruffer M.D. – 1921 – The University of Chicago Press
Skeleton of a man called Nefermaat found by Mr. G. Wainwright dating to the Third Dynasty (2890 – 2900 B.C.)

Temperomandibular Joint Dysfunction
“In the bones of the skull which were left, nothing particular was found except that the internal surface of both condyles were rough and showed distinct signs of inflammation.”

TMJ/Jaw Pain
Ligament laxity of the joint (Recurrent subluxation of intra-articular disc)Laxity at a distant location Failure to respond to current treatment

TMJ HistoryMandibular motion Requires stability and mobility of joint Precise coordination of muscles Dysfunction results from
• Blows to the jaw--Ligament injuries• Injuries to the articular disc• Poor coordination of muscles• Tonsilar scars

TMJ HistoryMandibular Dysfunction
results from• Blows to the jaw
Boxing Falls
• Whiplash motions

TMJ ANATOMYBones

TMJ ANATOMYLigaments: Joint capsule Stylomandibular

TMJ ANATOMYLigaments: Sphenomandibular

TMJ ANATOMYJoint Disc

TMJ ANATOMYMuscles: Lateral Pterygoid

TMJ ANATOMYMuscles: Lateral Pterygoid

TMJ ANATOMYNerves/Danger Zones

TMJ MovementsMandibular motion: Two joints allow for Speech Respiration Mastication
Mandibular motions include Elevation Depression Protrusion Retraction

TMJ pain Locally Referred-Lateral pterygoid

TMJ Physical Examination
Dental misalignment
Midline space between upper and lower teeth Protrusion deviation Decreased ability to open mouth: less than 50mm

TMJ Physical Examination Palpation
Joint line tender to palpation Muscle tenderness
Temporalis Digastric Masseter Lateral pterygoid
Deep behind angle of jaw/over tonsils

Tonsil Anatomy

Tonsil injection
RIT Solutions Irritants – phenol, tannic acid, pumice Chemo - tactics – Sodium Morrhuate Osmotic – dextrose, glycerine Combination – P2G Optimal solution and concentration to yet be found
RIT Solutions Dorman and Ravin (1991) reported that the most
frequently used proliferant in contemporary practice is ‘Ongley’s solution’ known as P2G
2.5% Phenol + 25% Glucose + 25% Glycerin in pyrogenic free water to 100%

RIT Solutions Hirschberg (1985) states that ‘Neither phenol nor
glycerine are required’.
A sclerosant solution containing only 2% glucose gives excellent results

RIT Solutions
Pomeroy (1983) emphasizes: “… the incidence of serious complication from the dextrose solution itself is negligible … The skill of the physician, the cooperation of the patient and anatomical variations within the patients seem to be the only significant factors that lead to complications.”

RIT Solutions Concentrations of dextrose ranging between 12.5%
and 25% have now been shown to be adequate Concentrations in excess of 25% should be
avoided for fear of causing tissue necrosis 10% glucose used by Dr. Dean Reeves (Kansas
City) just as effective as 25% and preferred by a majority of patients (11/16)

Procedure Informed Consent Use of RIT in an ambulatory setting is an
acceptable standard of care in the community Thorough familiarity of the physician with normal,
pathologic, cross-sectional and clinical anatomy

Procedure Physician must be properly trained in this
technique via a combination of seminars/workshops, apprenticeships or visiting fellowships in order to safely and effectively utilize this treatment.
Aseptic technique

Complications Dorman (1992) survey of 95 experienced
practitioners on a patient pool of 494,845 Total of 66 ‘minor’ and 14 ‘major’ complications ‘Major’ was defined as either requiring
hospitalization or having transient or permanent nerve damage
Risk-to-benefit = low complication rate

Results In appropriately selected patients 70 – 80% receive
complete or significant relief of pain Patient should notice a significant reduction in
pain by the 5th treatment 50% of patients notice some improvement after
just one treatment

Schedule of Treatments Fibroblastic activity subsides within 6 –8 weeks
following an injection Partial or complete relief is about 60-70%
following 3 – 6 injections (Klein 1989) It seems wise to try an initial course of 6 injections Follow up 2 months after the last of the initial
course

Schedule of Treatments Debatable with large variation in practice Currently I advise a treatment every 3 to 6 weeks Concurrent physical / manual / orthopedic /
osteopathic treatment for better result No need for “maintenance” or “booster”
treatments
Schedule of Treatments The treatment protocol needs to be tailored to each
patient 60-70% of cases will show some improvement at
the time of the initial re-assessment

Prolotherapy is the iatrogenic stimulation of the wound healing
and tissue repair process