progressive disintegrative psychosis of childhood
TRANSCRIPT
J . Child Psychol. Psychiat., Vol. 18, 1977, pp. 211 to 219. Pergamon Press. Printed in Great Britain.
PROGRESSIVE DISINTEGRATIVE PSYCHOSIS OFCHILDHOOD
JOHN CORBETT,* RUTH HARRIS
The Bethlem Royal and the Maudsley Hospital, Denmark Hill, SE5 8AZ
ERIC TAYLOR
The Institute of Psychiatry, De Crespigny Park, Denmark Hill, Londoti SE5 8AF
and
MICHAEL TRIMBLE
The National Hospital for Nervous Diseases, Queen Square, Lotidon WCl
THE TERM "Disintegrative Psychosis of Childhood" was used in 1969 by a W.H.O.Seminar on Classifications {Rutter et al., 1969). This diagnostic category has sincebeen included in the multi-axial classification selieme (for child psychiatric disorders)which utilises the Nintli revision of the LCD. The glossary (Rutter et aL,1975), which is at present being evaluated (Rutter et aL, 1976), suggests thatthe category (299.1) should include "disorders in which normal or near normaldevelopment for the first few years is followed by a loss of social skills and of speech,together with a severe disorder of emotions, behaviour and relationships. Usuallythis loss of speech and social competence takes place over a period of a few monthsand is accompanied by the emergence of overactivity and of stereotypies. In mostcases there is intellectual impairment, but this is not a necessary part of the disorder.The condition may follow overt brain disease—such as measles encephalitis—butit may also occur in the absence of any known organic brain disease of damage."The glossary emphasizes that an additional code on axis four should be used to iden-tify any associated neurological disorders and adds that the category includes the con-dition previously described as Heller's Syndrome but specifically excludes InfantileAutism (299.0) and the Schizophrenic Syndrome of Childhood (299.9).
The category is also seen as distinct from the diagnosis of Dementia which isincluded with the organic psychotic conditions occurring in the senile or prcsenileperiods of adult life.
The two following cases illustrate many of the features of Disintegrative Psychosisand it is recommended that sueh cases should, in view of their course, be allocatedto a subcategory of "progressive disintegrative psychosis of childhood"; therebydistinguishing them from psychiatric disorders following non-progressive encephalo-pathies such as some cases of measles or infantile spasms.
CASE 1A boy of thirteen years whose birth and development until the age of nine years appeared to
have been normal. At that time his father and stepinolher separated following a long history of•Requests for reprints to Dr. John Corbett, The Bethlehem Royal and the Maudsley Hospital,
Denmark Hill, London SE5, 8AZ, England.Accepted manuscript received 3 December 1976
211
212 JOHN CORBETT, RUTH HARRIS, ERIC TAYLOR AND MICHAEL TRIMBLE
marital disruption and he eame under the care of an older stepsister who noted that he was forgetfuland had some difficulty in performing tasks such as tying his shoe laces. After six months he com-plained of being bullied by his peers and seemed unable to "stiek up" for himself. By the end of oneyear, he was noted to be chewing his food excessively and he reported that other boy's had forcedhim to eat caterpillars and dead mice. Shortly after this he began to truant from school and waseventually referred to a child psychiatrist who understandably attributed his behaviour disturbanceto the grossly disturbed family situation and arranged special schooling and psychotherapy. Psycho-logieal testing, six months after the first symptoms were noted, showed him to have a full scale I.Q_.on the WISC of 77 (Verbal Scale 85, Performance Scale 72). He was noted during testing to bealert, restless and cocky, admitting that he had problems in school and complaining that mem-bers of his family were hostile to him and hit him. At the special school the teachers commentedon his further deterioration and by the end of four years he was soiling his bed and having difficultyin dressing himself, for example putting his shoes on the wrong feet. He developed mannerismsincluding head shaking, thumb sucking (a thing he had not done previously) and a peculiar flickingof his front teeth with his finger. His father noted episodes of pallor without loss of consciousnesslasting up to one to two hours. He later became diurnally enuretic, stopped painting and lost hisability to read and speak and was admitted to an inpatient psychiatric unit from which he wasreferred to one of us (J.A.C.) for further investigation.
On examination five years after the onset of the illness he was found lo be a tall pubescent boy-with no stigmata of mental retardation. He responded to simple commands and occasionally re-sponded with dysarthic but appropriate, although syntactically inadequate, sentences. Most of thistime was spent sitting, rocking, grimacing and drooling. He showed echopraxia but no echolalia. Onneurological examination his head circumference was 55 cm (just over the 50th percentile). Therewas equivocal pallor of both discs and possible slight wasting of the small muscles of both hands witha grasp reflex. The tendon jerks in the lower limbs were pathologically brisk with bilateral extensorplantar responses.
Psychological testing at this time showed a marked deterioration and he was only able to respondto three subtests on the verbal scale of the WISC giving him an estimated I.Q.. of below 45. He wasstill however able to read at a 61 year level on the Schonell test.
The EEG showed moderate diffuse excess of slow wave activity but there did not appear to havebeen any marked deterioration compared with records carried out a year and six months previouslyand all three records showed relatively little of the appropriate rhythmic activity for a boy of his age.
Nerve conduction studies done as an outpatient showed marked slowing across the terminalsegment of the left lateral politeal nerve and slight delay across the terminal segment of the leftmedian nerve and borderline normal values in the velocity along the length of these nerves. Theseresults suggested a peripheral neuropathy involving the distal more than the proximal segmentsof the nerves, and taken in conjunction with the clear-cut evidence of dementia led the neurophysio-logist (R.H.) to make a tentative diagnosis of metachromatic leucodystrophy at the outpatient assess-ment. Further investigations as an inpatient were initially negative apart from the lumbar airencephalogram which showed dilation mainly of the lateral ventricles and a C.S.F. protein of50 mg/100ml.
A cerebral biopsy was therefore carried out and this showed the white matter to be replaced bynumerous macrophages containing metachromatic material. Professor Davison of the NationalHospital for Nervous Di.seases reported on the thin layer chromatography which showed an abnormalsphingo-Upid pattern with a loss of cerebroside and marked increase in sulphatide, the appearancebeing those of metachromatic leucodystrophy.
Following the biopsy he developed seizures and a left hemiplegia and when seen again at the ageof fifteen years he was profoundly demented although the teeth fiicking mannerism persisted.
Re-evaluation of the urinary deposit showed that intracellular metachromatic material had beenpreviously overlooked and subsequent assay of aryl sulphatase A activity in urine and leucocytes{very low) confirmed the diagnosis of metachromatic leucodystrophy.
CASE 2
This boy was aged twieve when he died and also had an anomalous family background similar
PROGRESSIVE DISINTEGRATIVE PSYCHOSIS OF CHILDHOOD 213
to Case 1, being an illegitimate cbild wbo lived with his widowed mother. There were no siblingsand no family bistory of mental handicap and although tlie pregnancy was normal, birth was byCaesarian section. His early development was normal apart from an episode of bronchial obstructionat the age of four years. He had been told that his father was dead, but at the age of five, his fathersuddenly turned up, and the patient's difficult behaviour was said to date from that time.
He was referred to one ofthe authors (J.A.C.) at the Brixton Child Guidance Unit at the age ofeight years because of disobedience and overactivity and was reported to have a cold and callouspersonality. On psychological assessment his full scale I.Q_. on the WISC was 101 (verbal scale 89performance 115) with a reading age of 7-1 yrs on the Schonell test. He was friendly but with im-mature, attention seeking and provocative behaviour. His mother reported that he was cruel toanimals and had dressed up in her clothes. He was disobedient, had stolen on one occasion andthreatened to run away from home, 'lhere were no neurological abnormalities and initially heseemed to improve wilh psychotherapy. After a year his behaviour deteriorated at home and he wasplaced in a hostel for maladjusted children. A year later he was reported at school to be lacking inconfidence, and lo be a target for bullies. However, he made progress in reading and was then readingat the 9-7 yr level on the Schonell test.
The following year, when he was aged eleven, his behaviour deteriorated and he became moredefiant and difficult, refusing to wash and incessantly chattering to himself, often imitating the voiceof an imaginary friend. Shortly afterwards his mother decided not to see the patient's father againand he became very upset about this: swearing at his mother and threatening her with a knife. Hesaid he had been programmed to kill his mother and that his father and voices from the televisionhad told him to do this. The voices, which sometimes seemed to come from nowhere, he called Jackand Bill. They spoke to him in the third person and told him to find the Tower of London.
He was admitted to the Children's Ward at the Maudsley Hospital where neurological examina-tion was normal, and although anxious and miserable, rapport was good and he was fully oriented.Psychological testing at that tinae showed some intellectual deterioration with a full scale I .Q. of 83(verbal scale 90, performance scale 79) and he did not appear to have made any further progress inreading.
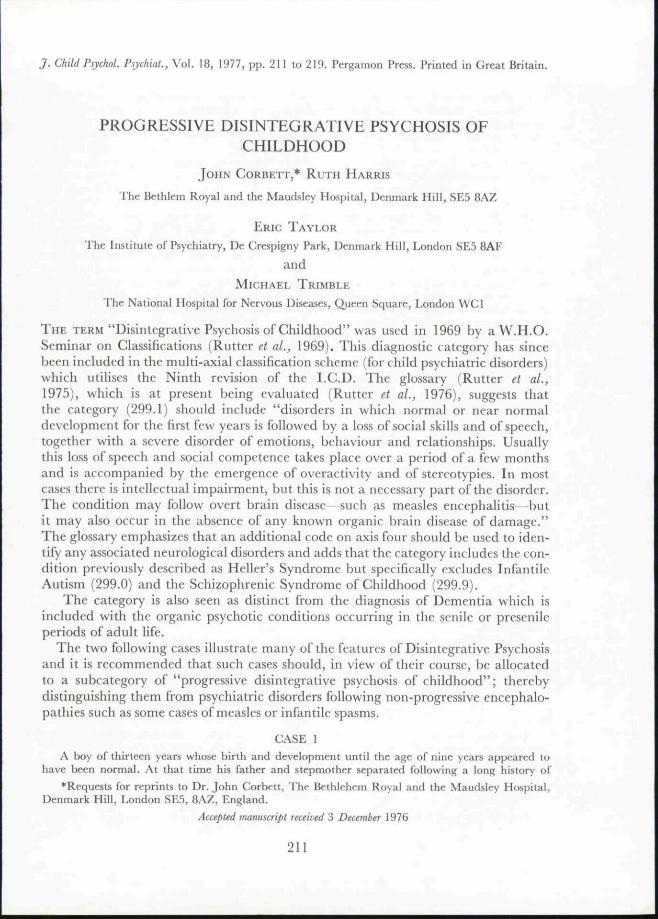
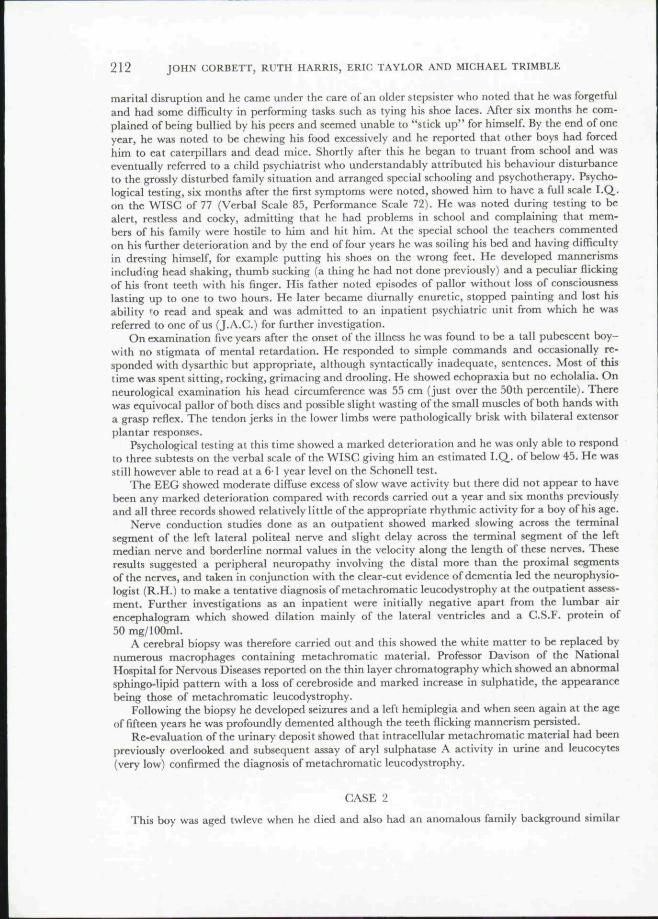
In view of this he was referred to a neurologist who found no abnormality. Over the next threemonths he made excellent progress and the acute symptoms which provoked his admission dis-appeared. Subsequently, his progress halted and over the space of two to three months he deterior-ated rapidly; his speech became incoherent, interspersed with inappropriate giggles and whistles.His EEG, which a year previously had been unremarkable, was found to be grossly abnormal withgeneralised thfta and delta activity, and deteriorated further over thf next few months (Figs. 1 and 2).Nerve conduction studies were normal.
In view of his, by now, obvious dementia, he was admitted to the Hospital for Sick Children,Great Ormond Street, under the care of Dr. J. Wilson, bul although a synacthen test was marginallyabnormal with a pre- and post-synacthen levels of 6-6 and 17 0 fig torti.sol % respectively, al] otherinvestigations were negative.
His behaviour continued to deteriorate and he became restless and inaccessible with completeloss of speech, facial grimacing and manneristic behaviour with teeth flicking (as in Case I). Follow-ing two acute episodes of pyrexia, vomiting and drowsiness, he rapidly deteriorated and died. Atpostmortem the macroscopic appearance ofthe cut surface of the brain showed great loss of myelinin white matter with preservation of U-fibres in a patchy manner. On histological examination,Professor Duchen reported the appearances as being characteristic of a sudanophilic leucodystrophy(Schilders Disease).
DISCUSSION
Bffore the category of disintegrative psychosis became available it seems possiblethat the labels of dementia praecocissima (de Sanctis, 1906), or more recentlyHeller's Syndrome (Heller, 1930) might have been applied to these two cases at thestage when psychiatric inpatient admission became necessary. It is possible to rc-examinc the evidcnrc for the continurd use of these two labels in the classification of
214 JOHN CORBETT, RUTH HARRIS, ERIC TAYLOR AND MICHAEL TRIMBLE
Stephen Mu. Uyears 12.6.74 A7314
100 3iV
FIG. 1. Case 2: Symmetriral, but rather unstable alpha rhythm Is present posteriority. (Recorded atthe time of behaviour deterioration.)
Stephen Mu. 12year8 05O2 23.9.75
15011V •^\''^\y\/^,/'^'^'''^''V\^
FIG. 2. Case 2: Just over one year later the EEG shows a severe generalised abnormality with largeamplitude irregular slow nerve activity over both hemispheres. The alpha rhythm has disappeared.
the psychoses of childhoodj and also to look at the distinction between these con-ditions and other disintegrative psychoses occurring in this age period as well as thedifffrential diagnosis from the classical form of Early Infantile Autism first describedby Kanner (1943).
Early writers used the term .schizophrenia very loosely but de Sanctis. writingin 1906, pointed out that most psychiatrists at that time had accepted thr essentials
PROGRESSIVE DISINTEGRATIVE PSYCHOSIS OF CHILDHOOD 215
of Kracpelin's concept of dementia praecox, a term, In fact, used by Morel (1860)to describe premature dementia occurring at puberty in the children of alcoholicsand of the insane. De Sanctis concluded that the characteristic adult forms ofschizophrenia did not usually occur before puberty but described a number ofchildren in whom some of the symptoms of dementia praecox occurred before thatage; a condition he termed dementia praecocissima. With hindsight the clinicalpictures shown by these children were very similar to those commonly found insome mentally retarded children with sterotypies and abnormal behaviour.
Theodor Heller (1930) described a condition which can now be distinguishedfrom infantile autism, pseudo-feeble mindedness and childhood schizophrenia. Hecalled this condition dementia infantilis and felt that it was quite distinct fromdementia praecocissima, and also that Sante de Sanctis was incorrect in describingthe condition as an early form of dementia praecox in childhood. The ehildrendescribed were often placid and lively children until the age of three or four yearsand they then became moody, disobedient and negativistic often raging withoutreason and whining, throwing their toys, showing anxiety symptoms and havingoccasional hallucinations. They then developed intellectual deterioration over thespace of a few months leaving them without speech and in a state of idiocy. Duringthis regressive period stereotyped movements and postures became frequent andthe children became incontinent needing to be fed. They were inattentive, reachingtheir lowest mental level at an average equivalent to an infant of nine monthswithout subsequent improvement. Heller did not report the duration of his follow-upbut from what he said, it seems that his patients remained in this state.
In 1943, in a paper entitled "Autistic Disturbances of Affective Contact"Kanner described eleven children with symptoms of a condition now firmly recog-nised as early infantile autism. He emphasised the child's inability to relate in anordinary way to people and situations from the beginning of life, without any with-drawal from formerly existing participation. Kanner thought that the lack of aperiod of at least two years normal development clearly distinguished this conditionfrom de Sanctis' and Heller's Syndromes.
Although eight of Kanner's eleven children acquired the ability to speak, innone did language serve to convey abstract ideas or enable the child to engage insocial conversation beyond the level of requests for simple information or exchangeof platitudes on well-worn subjects. In addition to the disorders of language andrelationships Kanner also noted other symptoms including an excessive reaction toloud noise and moving objects, stereotyped and ritualistic behaviour, an anxiouslyobsessive desire for the maintenance of sameness, and islets of ability on performancetasks.
As a result of the work of Kanner and later authors (Creak, 1961; Wing, 1975;Rutter and Lockyer, 1967) there should be Httle difficulty in diagnosing earlyinfantile autism at its most typical. The main problems arise when it is associatedwith more clear-cut organic symptomatology and particularly when features of theclinical picture are seen following an encephalopathic illness or other forms ofbrain damage in early infancy.
Kanner himself pointed out that it was customary to list Heller's Disease among
216 JOHN CORBETT, RUTH HARRIS, ERIC TAYLOR AND MICHAEL TRIMBLE
the varieties of infantile schizophrenia until pathologists began to find evidence ofcerebral degeneration in these children and he emphasised the essentially organicbasis of this condition (Kanner, 1935). Subsequent reviewers have reached similarconclusions (Bradley, 1942; Benda, 1960; Yakolev et al., 1948).
Malamud (1958) described six children with organic brain disease who hadclinically presented with "childhood schizophrenia", their symptoms closelyresembling those described by Heller. At post mortem there was clear-cut evidenceof cerebral degenerative disease suggestive of late infantile forms of cerebral lipoid-osis. Two of the cases he diagnosed as 'amaurotic family idiocy without amaurosis'while in the others the pathological changes were of a non-specific type. Althoughas recently as 1957 cases of Heller's Syndrome were being described (Hudolin,1957), Malamud felt that Heller's Disease had become a 'waste paper basket'diagnosis for all sorts of organic brain disorder, but, more importantly, it had beenconfused with childhood schizophrenia.
Other studies have described organic causes of "childhood psychoses": thesehave included Hpoidosis (Creak, 1963), tuberose sclerosis (Creak, 1963), infantilespasms (Kolvin et al., 1971; Taft and Cohen, 1971; Corbett et al., 1975), and rubellaembryopathy (Chess et al., 1971).
Rivinus and his colleagues (1975) reported twelve children who presented withpsychiatric symptoms but who were subsequently found to be suffering from neuro-logical disorder. An initial diagnosis of child psychosis was made in two of thechildren, while three others had been diagnosed as conduct disorders. The finaldiagnosis in these five children included such varying conditions as Schilder'sDisease, sub-acute sclerosing panencephalitis, congenital syphilis, metachromaticleucodystrophy and non-specific neurodegenerative disease.
It is often difficult to distinguish those cases of childhood psychosis or autismwhich are associated with organic conditions from those that apparently are not.Some, seemingly classical, cases of infantile autism develop fits in late adolescence(Rutter, 1974) and even deteriorate or die. The difference presumably lies in thesize of the lesion, its nature and the stage of the child's development at which itoccurs. The diffuse nature of the pathology which characterises our two cases isagainst a focal abnormality as has been argued by Hauser et al. (1975) in the caseof autism. It is possible, however, that the process begins focally and techniques suchas computerised axial tomography in such cases may clarify this.
In the patients described above the clinical picture may be clearly distinguishedfrom that of early childhood autism by the prolonged period of normal early develop-ment and the lack of the most characteristic features of this condition; at least untilthe inaccessibility and stereotyped behaviour which developed in the terminalstages. The final onset of rapidly progressive dementia serves to distinguish themfrom adult types of schizophrenia, although the bizarre thoughts and auditoryhallucinations which occurred at one point in the second case might have temporarilygiven rise to the suspicion of this condition. Although the onset in these cases waslater than in those described by de Sanctis and Heller, many of the features areremarkably similar. In spite of this these classical accounts must now seem too vague,inconsistent and lacking in pathological detail to merit their retention as clinicalentities. •
PROGRESSIVE DISINTEGRATIVE PSYCHOSIS OF CHILDHOOD 2 1 7
The prolonged behavioural disorders in both boys, occurring in the setting ofdisturbed family psychopathology, before the clinical appearance of dementia or anyfocal neurological signs, might be accounted for by the effects of psychological stressin neurologically vulnerable children. However, in both, the behaviour disturbanceeventually assumed psychotic proportions with bizarre and stereotyped behaviour,delusional ideas and inappropriate affect which constituted a more complex psychia-tric picture than could be accounted for by simple dementia.
It might be argued that the concept of "Dementia Infantilis" should be retainedand refined from the original description of Heller, in the light of modern biochemicaland pathological advances in the diagnosis of the neurodegenerative diseases ofchildhood. This category might then be added to the organic psychotic conditions(290-294) in the LCD. as an additional category to the dementias of adult life(e.g. 290.5) rather than including it in the psychoses with origin specific to child-hood (299). It seems preferable however to include such cases, in the subcategoryof disintegrative psychosis (299.1) as this best conveys the complexity and charac-teristic picture ofthe psychiatric condition which seems to bear remarkable similarityto the other childhood psychoses in spite of the differing neuropathology. Theother psychoses of childhood usually show some evidence of intellectual impairmentwhich is sometimes progressive and the presence of dementia does not, therefore,contraindicate this approach to classification.
From the chnical point of view a diagnosis of progressive disintegrative psychosisimplies that such symptomatology should receive early and repeated paediatricneurological investigation and it is only in this way that delays in diagnosis can beminimised in those cases where gross neurological signs do not appear until thelatter stages ofthe disease. It might of course be claimed that early diagnosis doesnothing to alter the eventual outcome. It will, however, lead to a reorientation in thepsychiatric management aimed at relieving parents of blame, and minimising theambivalent feelings which a severely and chronically disturbed child is likely toarouse.
Although the similarity between the two cases which have been described isstriking, it would be unwise to suggest additions to the glossary definitions of thedisintegrative psychosis or to imply further characteristic features which may betaken into account in their diagnosis on the basis of these examples.
The investigation and differential diagnosis of the neuro-degenerative disordersof childhood have been usefully reviewed recently (Wilson, 1974; Noronha, 1974),and it is clear that the clinical picture will differ according to whether the conditionis of infantile or late juvenile onset, whether it is associated with focal neurologicalsigns early in the course, or whether the condition involves predominantly greymatter or white matter.
As far as the psychiatric and psychological contributions to diagnosis go, thefollowing points arouse suspicion of one the neuro-degenerative disorders associatedwith a disintegrative psychosis.1. Prolonged emotional disorder in childhood which may be out of proportion to
psycho-social stresses in the child's environment, or if it occurs in the settingof an underlying family disturbance where the symptoms cannot easily berelated in dynamic terms to the stress factors concerned.
218 JOHN CORBETT, RUTH HARRIS, ERIC TAYLOR AND MICHAEL TRIMBLE
2. The failure of response of the emotional disorder to psychotherapy or otherpsychological treatments.
3. Bizarre and unusual symptomatology especially meaningless rituals, manner-isms, hallucinations and delusions.
4. A disturbance in relationships: either unusual coldness or difficulty establishinga relationship with the child.
5. An insidious fall off in educational or social performance: an initial drop inthe performance I.Q,. with later progressive loss of language functions.
6. Appearance of focal neurological signs or more overt evidence of dementia.7. Abnormalities in the EEG, particularly with deterioration in the EEG features
over a period of time or other evidence of dysfunction in neurophysiologiealtesting.
SUMMARY
The literature concerning dementia and disintegrative psychosis in childhood isreviewed. Two cases with different neurodegenerative disorders presenting withlate juvenile onset psychiatric symptoms are described.
There appears little point in retaining the eponymous syndromes of de Sanctisand Heller.
The diagnostic category of Progressive Disintegrative Psychosis is appropriate todescribe the clinical psychiatric picture in these children. Because of the rarity ofsuch conditions further collaboration between child psychiatrists, paediatric neuro-logists and neuropathologists is needed to delineate further the psychiatric syn-dromes associated with the neurodegenerative disorders.
Acknowledgements—Grateful thanks are due lo Drs. Lionel Hersov, John Wilson and Lorna Wing, andto Professor Michael Rutter for helpful advice and criticism, to Dr. Magda Erdohazi who reportedon the brain biopsy of Case 1, and Professor Duchen for the results ofthe pathological findings in thesecond case.
This paper was based on a communication to the first annual meeting of the Association ofBritish Paediatric Neurologists held at Durham University in January, 1976.
REFERENCES
BENDA, C . E . (1960) Childhood schizophrenia, autism and Heller's Disease. In Mental Retardation—Proceedings of the First International Medical Conference, Portland, Maine (Edited by BOWMAN,PETER W . and VAN MAUTNER, H . ) . Grune & Stratton, New York.
BRADLEY, C . (1942) Schizophrenia in Childhood. Macmillan, New York.CHESS, S.> KORN, S. J . and FERNANDEZ, P. B. (1971) Psychiatric Disorders of Children with Congenital
Rubella. Brunncr-Mazel, New York.CORBETT, J. A., HARRIS, R . and ROBINSON, R . (I975J Epilepsy in Aienlal Retardation and Developmental
Disabilities, Vol. VII, (Edited by WORTIS, J.). Brunner-Mazel, New York.CREAK, M . et a/. (1961) Br. med. J. 2, 889.CREAK, E . M . (1963) Childhood psychosis: a review of 100 cases. Br. J. Psychiat 109, 84-89.HAUSER, S. L . , DE LONG, G . R . and ROSMAN, N . P. (1975) Pneumographic findi, gs in the infantile
autism syndrome—a correlation with temporal lobe disease. Brain 4, 667-68 iHELLER, T . (1930) About dementia infantilis. Z- Kiriderforsch., Berlin 661-667. Translated into
English by Howells (1969).
PROGRESSIVE DISINTEGRATIVE PSYCHOSIS OF CHILDHOOD 219
HOWELLS, J. G. (1969) Modern Perspectives in International Child Psychiatry. Oliver & Boyd, Edinburgh.Translations of original papers of de Sanctis and Heller,
HuLSE, W. C. (1954) Dementia infantilis. J. J^erv. Ment. Dis. 119, 417-477.HuDOLiN, V. (1957) Dementia infantilis Heller. J. Ment. Defic. Re.s. 1, 79-90.KANNER, L . (1935) Child Psychiatry, 3rd Ed., 1957. C. C. Thomas. Springfield, III.KANNER, L . (1943) Autistic disturbances of affective contact. The Nervous Child 2, 217-250.KoLviN, L., OuNSTED, C. and ROTH, M . (1971) Cerebral dysfunction and childhood psychosis.
Br. J . Psychiat. 118, 407-414.MALAMUD, N . (1959) Heller's disease and childhood schizophrenia. Am. J. Psychiat. 116, 215-218.MOREL, F . (1860) Etudes des Maladies Mentales. Paris.NORONHA, M . J. (1974) Cerebral degenerative disorders of infancy and childhood. Develop. Med.
NeuroL 16,228-241.RiviNUS, T. M., JAMISON, D . L . and GRAHAM, P. T. (1975) Childhood organic neurological disease
presenting as psychiatric disorder. Archs. Dis. Child. 20, 115-119.RUTTER, M . and LOCKYER, L . (1967) A five to fifteen year follow-up study of infantile psychosis—1.
Description of sample. Br. J. Psychiat. 113, 1169-1182.RUTTER, M . , LEBOVICI, S., EISENBERG, L. , SNEZHNEVSKY, A. V., SADOUN, R . , BROOK, E . and LIN, T .
(1969) A triaxial classification of mental disorder in childhood. J . Child Psychol. Psychiat. 10,41-61.
RUTTER, M . (1974) Development of infantile autism. Psychol. Med. 4, 147-167.RuTTER, M. L., SHAFFER, D . and STURGE, C . (1975) A Guide to a Multi-axial Classification Scheme for
Psychiatric Disorders in Childhood and Adolescence. Department of Child and Adolescent Psychiatry,Institute of Psychiatry, London.
RUTTER, M . L . , SHAFFER, D . and SHEPHERD, M . (1976) An Evaluation ofa Proposal for a Multi-axialClassification of Child P.iychiatric Disorders. World Health Organisation Monograph, Geneva.
DE SANCTIS, S. (1906) On some variations of dementia praecox. Rivista Sperimentali di Freniatria 32,141-165.
TAFT, L . T . and COHEN, M . J. (1971) Hypsarrhythmia and infantile autism: a clinical report.J. Autism Childh. Schiz. 1, 3327-3336.
WILSON, J. (1974) Investigation of degenerative disease ofthe central nervous system. Arch. Dis.Childh. 47, 163-170.
WiNO, L. (1975) Early Childhood Autism, 2nd Edn. Pergamon, Oxford.YAKOLEV, P . I., WEINBERGER, M . and CHIPMAN, C . E . (1948) Heller's syndrome as a pattern of
schizophrenic behaviour disturbance in early childhood. Am. J. Ment. Defic. 53, 318.
