programme for ers live on understanding the 2008 imi calls
DESCRIPTION
Introduction The COPD call The Severe Asthma Call Summary and questions from participants. Programme for ERS Live on understanding the 2008 IMI calls. Leo Fabbri, ERS Ingela Wiklund, GSK Tim Higenbottam, Chiesi Chris Compton and Leo Fabbri, EFPIA and ERS. The 2008 Respiratory Calls: - PowerPoint PPT PresentationTRANSCRIPT

1
Leo Fabbri, ERS
Ingela Wiklund, GSK
Tim Higenbottam, Chiesi
Chris Compton and Leo Fabbri, EFPIA and ERS
Introduction
The COPD call
The Severe Asthma Call
Summary and questions from participants
Programme for ERS Live on understanding the 2008 IMI calls

The Innovative Medicines Initiative (IMI)
The 2008 Respiratory Calls:COPD PRO
Ingela Wiklund

3
2008 COPD Patient Reported Outcomes (PRO) call: Background
Explanation of the need:• Efficacy evaluation of new therapies
has relied on demonstration of reduction of airflow obstruction. – European Regulatory guidelines
recommend the use of symptom endpoints, in addition to lung function measurements
• A PRO is any report coming directly from patients about how they function or feel in relation to a health condition and its therapy :– Without interpretation by physicians
or others– PRO Measurement tools should be
generated with adequate patient input.
There is a need for scientifically developed and validated PRO measures that capture symptoms, exacerbations and their impact on patients
The areas that should be developed:
• Symptoms: A patient with COPD experiences a variety of symptoms including dyspnoea (shortness of breath). – Restricts patients’ ability to
exercise and perform daily activities
– Results in psychological consequences
– Significant impairments to overall health status.
• Exacerbations: Acute worsening of symptoms that often require a change in treatment or could result in hospitalization.

4
COPD call: What is it about?
• Objectives– Understanding of the patients’ experience of COPD to inform the
strategy to measure outcomes that are relevant to patients for assessing treatment benefit
– Selection and/or Development of measures with good measurement properties that capture the COPD patients’ experience of the disease and effects of treatment. Eg PRO focussed on exacerbation:
• To inform the definition of exacerbation• Understand day-to-day experience of symptoms characterizing an
exacerbation• Evaluate the impact of these symptoms
• Scope– Build consensus on the measurement strategy, especially PRO
tools, by working with the key consumers of the information on treatment benefit:
• Clinicians, academic clinical & health outcomes researchers, patients and payers

5
COPD call: Deliverables
A measurement strategy that includes specific PRO tools:– Developed using robust psychometric methods
• With input from and review by the major customer groups
– Validated for use in treatment evaluations across Europe that can link to global efforts• Using appropriate prospective studies
– Developed or adapted for capturing data using electronic data capture (EDC) devices for daily recording at home

6
COPD call: What are we expecting and going to do?
Project plan outline• Planned in two phases :
– Phase A: Develop a framework to understand the Patients experience of COPD, especially in a broad European context, to inform strategies to measure outcomes meaningful to patients in global clinical trials
– Phase B: Develop/select and validate PRO measurement tools, to use in clinical trials evaluating treatments for the disease
A Consortium or ‘Centre of Excellence’ • To develop a measurement strategy to
evaluate the benefits of COPD treatment from a patients’ point of view
• With contributions from the key customers and ‘Subject Matter Experts’. For example…
• University • Clinical centres • SME researchers• Patient groups• EMEA• Payers• Health Technology Assessment
agencies • Agencies that make decisions
about reimbursement
It is important to link to and build on existing International ‘Initiatives for the measurement of PROs in COPD’ to avoid redundancies

The Innovative Medicines Initiative (IMI)
The 2008 Respiratory Calls:Understanding Severe Asthma
Tim Higenbottam

Challenges to Drug Development in Severe Asthma
1. Heterogeneous disease (the “asthmas”)
2. Lack of standard definition of severe– Lung function– Medication requirements– Exacerbation frequency– Symptom burden
3. What are the phenotypes of a severe asthmatic?
4. Is there a genotype(s) of severe asthma?
5. Effect and detection of non-compliance
6. Lack of regulatory path in severe asthma
7. Lack of patient availability for clinical trials
8
Big gaps in care:
• There is high unmet need for more effective, convenient and safe therapies, particularly for patients with moderately severe and severe disease.
• 10% of asthmatics with the most severe disease account for up to 50% of the total costs of asthma care.

Challenges to Drug Development in Severe Asthma
1. What should we measure in severe asthma and with what instruments? Are they validated?
2. What are appropriate study designs and inclusion criteria in severe asthma?
3. Are there biomarkers to identify patient phenotypes and/or follow therapy
4. Identification of key targets and mediators of severe asthma
5. Understanding molecular pathways of steroid resistance
6. Role of imaging and/or other modalities for early decision making in development programs
7. Understanding mucosal immune function in severe asthma
Big gaps in care:
• There is high unmet need for more effective, convenient and safe therapies, particularly for patients with moderately severe and severe disease.
• 10% of asthmatics with the most severe disease account for up to 50% of the total costs of asthma care.

Longitudinal study of a severe asthma Patient Cohort
Define disease
Recruit cohort
Newly defined cohort
InnovativeClinical
measurementsNew model
development
Longitudinal
study
New clinical study design
Optimal dosing ideal PK/PD and high therapeutic index
Optimal clinical measures of efficacy

11
First part of call deliverables:
1. EU and Globally agreed Diagnostic criteria for severe asthma that are aligned to EMEA requirements
2. A longitudinal cohort of severe asthma patients with relevant phenotype and genotype ~ recruited with a standardised protocol, data collection, and database with flexibility for novel measures to be added in during the project
3. Identification as well as validation of novel targets for pharmacological therapy and biomarkers to assess response and predict effects on clinical outcomes
Second part of the call:Translating the cohort into a new therapeutic paradigm1. Identification of targets relevant to specific
phenotypes or genotypes of severe asthma.2. Understanding of aetiology and pathogenesis of
asthma exacerbations as mechanism to identify new targets and therapeutic approaches especially with regard to delaying time to exacerbation and reducing severity of exacerbation, which ultimately will deliver significant pharmaco-economic benefits.
3. Accurate targeting of an intervention to a particular, well-defined patient sub-population.
4. Capability to develop translational models for appropriate prediction of clinical relevance through preclinical modelling.
5. Access to defined patients which will facilitate enrolment and study of patients for clinical trials by academic and pharmaceutical research.
The deliverables for severe asthma over 5 years

What is needed in expression of interest in severe asthma
• A CRO or SME partner to provide management and operational processes to the patient cohort
• A multi-disciplinary scientific management board that includes clinical expertise, patients interest groups and laboratory scientists
• An accepted definition ~ including the means for achieving one and engagement that enables alignment with the EMEA [FDA] requirements
• Measurements to phenotype patients and to have agreed inclusion criteria for a database of patients
• A standardised patient recruitment process across Europe• A standardised patient management using conventional
therapy and adequate instruments/tests to determine compliance
12

Strategic Research Agenda (SRA): COPD, Asthma, Rhinitis• SRA identified one priority respiratory disease based on
medical need: Asthma ~ severe or refractory was seen as the most important be the EFPIA resp group
• As with each disease key bottlenecks fall into three main areas:– Disease understanding: Epidemiology, diagnosis, assessment of
severity, phenotyping, biochemical and genomic markers – Translational models: Identification and validation of new preclinical
and clinical models to facilitate translational research– Measurable outcomes: QOL measures that are sensitive to
pharmacological interventions and can predict pharmacoeconomic benefit
• Objective is to build a European Network or “Centre of Excellence” for asthma through the life of IMI, starting with 2008 calls– 2008 calls will be focussed to disease understanding for Asthma
and outcomes for COPD13

Joint working between the Industry, SMEs and Academia as
Consortia: IMI is different from other Framework Initiatives
“
Full Consortium
”EFPIA + Public Consortium
1. Joint preparation of the final proposal
2. Establish the process for managing the proposal
3. Establish timelines for deliverables
4. Select the partners and manner of working
Shared research agenda
Focus on disease and patient need
Tightly Managed Investment
*
*Consortium includes EFPIA colleagues as active contributors not passive donors of money

The IMI is an independent company founded by EU Commission and EFPIA Funding is 2 billion Euros over 8 years
2 Billion EUROIn kind + Cash
1Billion Euro 1Billion Euro
In kind
In-Kind ContributionA non-monetary contribution to the
consortium eg personnel, equipment,consumables etc
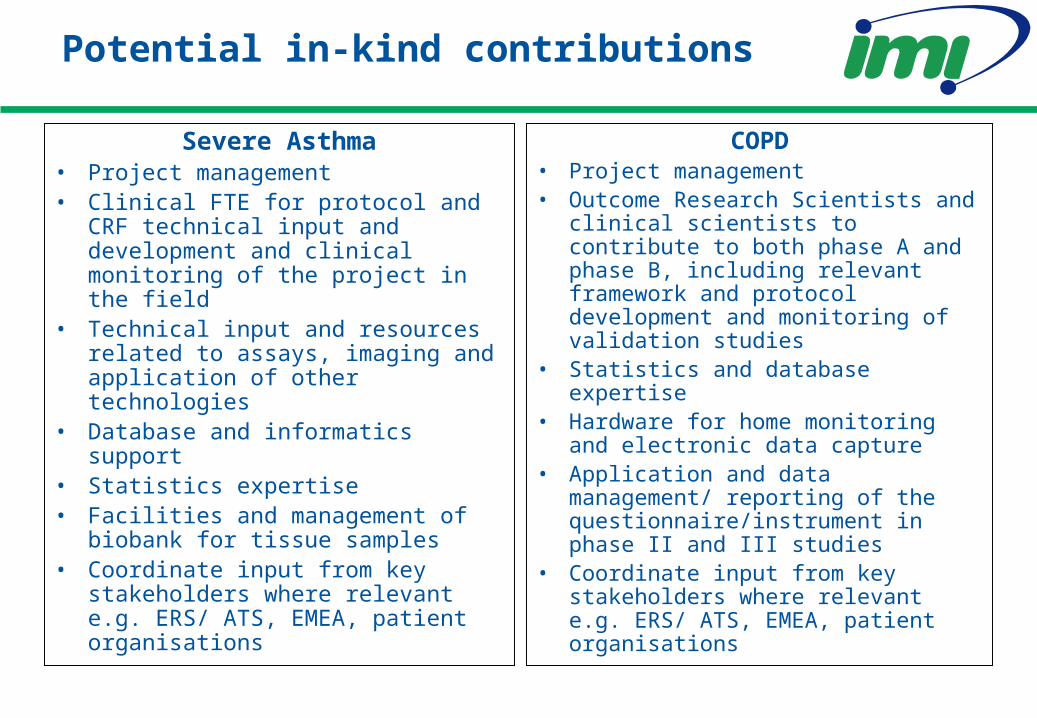
Potential in-kind contributions
Severe Asthma• Project management• Clinical FTE for protocol and CRF
technical input and development and clinical monitoring of the project in the field
• Technical input and resources related to assays, imaging and application of other technologies
• Database and informatics support• Statistics expertise• Facilities and management of
biobank for tissue samples• Coordinate input from key
stakeholders where relevant e.g. ERS/ ATS, EMEA, patient organisations
COPD• Project management • Outcome Research Scientists and
clinical scientists to contribute to both phase A and phase B, including relevant framework and protocol development and monitoring of validation studies
• Statistics and database expertise• Hardware for home monitoring
and electronic data capture• Application and data
management/ reporting of the questionnaire/instrument in phase II and III studies
• Coordinate input from key stakeholders where relevant e.g. ERS/ ATS, EMEA, patient organisations

Call
Research Agenda
Call Topics
Annual Implementation Plan
Call definition
1. Project Agreement2. Grant Agreement
Contract Execution
The Call & Evaluation Process
Expression of Interest
1st Peer Review
Invitation to Submit Full Proposal
Stage 1: Scientific excellence•“Public” consortia (academia, SME, patient organisations) only. No EFPIA
≈ 5 months
Full Project Proposal
2nd Peer Review
Stage 2: Feasibility and scientific excellence. EFPIA join successful consortium from stage 1
≈ 3 months

Evaluation Process for Successful EoI at Stage 1:EFPIA plus EC appointed independent expertsNote EoI only eligible if submitted through web-based system
1. Scientific and/ or technological excellence• Quality of the approach• Likelihood to meet key project objectives• Complementarities with EFPIA consortium• Innovation, progress beyond state-of-art, impact
2. Partnership case• Quality and relevant experience of individual participants• Appropriateness of role/ input of each applicant
3. Quality of the applicant consortium as a whole• Unique features, balance
4. Quality and soundness of the workplan• Timelines, budget
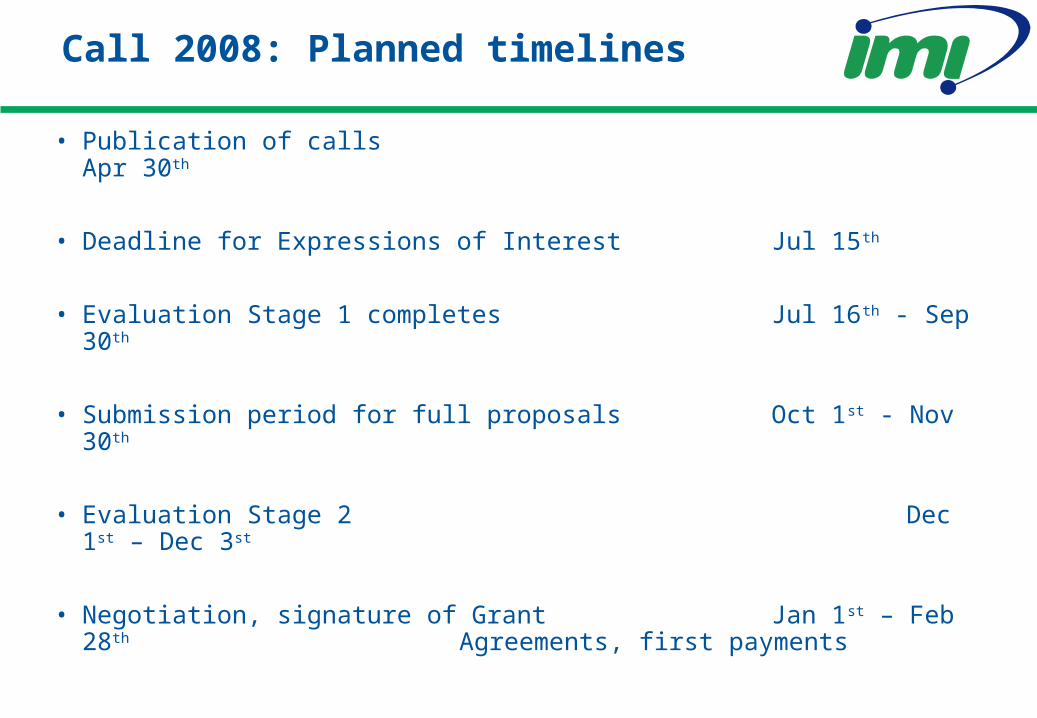
Call 2008: Planned timelines
• Publication of calls Apr 30th
• Deadline for Expressions of Interest Jul 15th
• Evaluation Stage 1 completes Jul 16th - Sep 30th
• Submission period for full proposals Oct 1st - Nov 30th
• Evaluation Stage 2 Dec 1st – Dec 3st
• Negotiation, signature of Grant Jan 1st – Feb 28th Agreements, first payments

The IMI IPR Policy Must Align with the Objectives of IMI
• IMI aims to remove the bottlenecks in R&D by conducting pre-competitive collaborative research utilising public and pharmaceutical industry resources
IMI findings must be widely and readily available for research into the discovery and development of medicines
IMI findings (Foreground IPR) must be widely and readily availablefor research into the discovery and development of medicines
Information that Participants bring into a Project (Background IPR) thatis necessary for the research use of IMI findings (Foreground IPR)must be widely and readily available for research into the discoveryand development of medicines

“Participants may use, exploit, sublicense or otherwisecommercialise their intellectual property rights as they seefit beyond the Research Use rights described in this IPRPolicy.”
Note: The IMI IPR Policy Does Not Affect Commercialisation of IPR
Total control for owner of Foreground andBackground IPR for non-research use

IMI Helpdesk can be accessed through IMI Website
• Includes call documentation, submission tool and FAQ
• Includes Helpdesk form for specific questions • http://www.imi-europe.org/Pages/IMI_Call_2008_1.aspx

The Innovative Medicines Initiative (IMI)
Thank you very much for your attention!
http://www.imi-europe.org
IMI is public-private partnership between the European Commission and the European
Pharmaceutical industry to promote biomedical innovation in Europe and to address the bottlenecks
in the R&D process.