prof. saman wimalasundera mbbs do phd professor in community medicine former head, department of...
TRANSCRIPT
Prof. Saman Wimalasundera
MBBS DO PhDMBBS DO PhDProfessor in Community MedicineProfessor in Community Medicine
Former Head, Department of Former Head, Department of Community MedicineCommunity Medicine
In charge OphthalmologistIn charge OphthalmologistCommunity Ophthalmology centerCommunity Ophthalmology center
Faculty of MedicineFaculty of MedicineUniversity of RuhunaUniversity of Ruhuna
Galle Galle Sri LankaSri Lanka

Epidemiology and
its application

The concepts of epidemiology were first
suggested by Hippocrates in the fifth century
B.C. that the development of human disease
might be related to external and personnel
environment of an individual.

The word epidemiology is derived from
Greek and means “Studies upon people”
Epi – Upon, Demos – People, Logia – Study
In contrast to clinical medicine epidemiology
involves the study of group of people rather
than individuals.

Epidemiologist vs. Epidemiologist vs. clinicianclinician
A clinician identifies the ailment in his patients
using certain scientifically developed tools to
ascertain history of illness, clinical examination
and investigations.
Epidemiologist addresses the understanding
of the distribution and determinants of a
disease in a community (not an individual)
using standard parameters.

What constitute What constitute epidemiologyepidemiology
Epidemiology includes:-
1. The methods for measuring the health of
groups and determining the attributes
and exposures that influence health.
2. The study of the occurrence of disease in its natural habitat rather than in the controlled environment of the laboratory.

3. The methods for the quantitative study of the distribution, variation, and determinantsof health related outcomes in specific groups (sub populations) of individuals, andthe application of this study to the diagnosis, treatment, and prevention of disease status or events.

Evolution of epidemiologyEvolution of epidemiology
The evolution of medical sciences in its
earlier phase was based on curative
medicine. The primary objective was to cure
a patient of his illness. Doctors in historical
times looked at their patients as ill people
who needed some treatment.

Thus medical science was individual
oriented. But gradually it became evident
that better human health could be achieved
by prevention of diseases rather than by
cure.

A Historical Sketch A Historical Sketch
A Long sketch of time ran for more than 2
millennia from Hippocrates (470-400 B.C.) to
the first third of 19th century.
Hippocrates developed the medical
approach by providing concise, accurate and
complete description of actual clinical cases.

An Italian clinician called Bernardino
Ramazzini in 1700 moved from observation of
clinical cases to the consideration of ‘work
circumstances’ in similar cases. He is now
regarded as the founder of occupational
medicine. (Explained in his book. “De Morbis
Artificum Diatriba”).
The major step forward in epidemiology occurred in 1662. John Graunt analyzed the weekly reports of births and deaths in London.
For the first time in the history, a quantified pattern of disease, deaths and births was Found. John Graunt is regarded as the founder of demography now.
His observations were published in his
book. Named “ the nature and political
observations made upon the bills of Mortality”.
After two centuries William Farr (1839) a
physician was given the responsibility for
medical statistics in England and Wales. He
set up a system for routine compilation of vital
statistics and application of data for evaluation
of deaths.

Hippocrates, Ramzinni, Graunt and Farr contributed to the understanding of diseasefrequency and distribution.
Another British physician John Snow formulated and tested a hypothesis concerningthe origins of an epidemic of cholera in Londonon the basis of available descriptive data.

Snow postulated that cholera was
transmitted by contaminated water. (then
unknown mechanism)
He observed that death rates from Cholera were particularly high in certain areas of London.
Those areas were supplied with water
by two water companies namely “Lambeth”
and “Southwark & Vauxhall” in 1849. Both the
companies that time drew water from river
Themes at a point heavily polluted with sewage.

The Lambeth company then changed its source to an area of Themes where the waterwas quite free from sewage of London.
The rate of cholera deaths then declined in those areas suppied by Lambeth company.
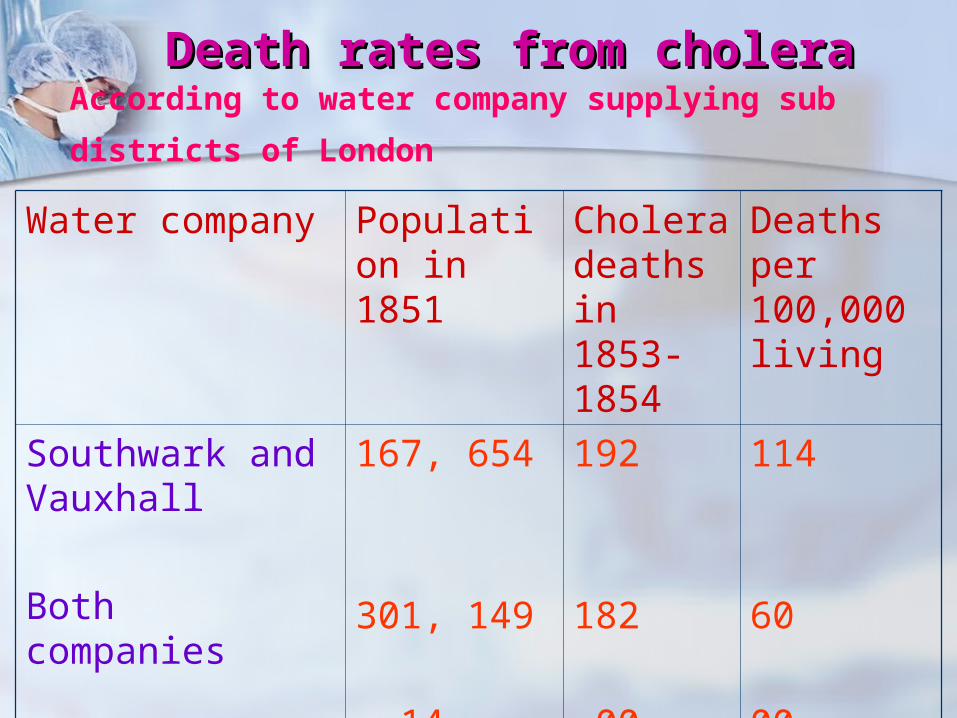
Water company Population in 1851
Cholera deaths in 1853-1854
Deaths per 100,000 living
Southwark and Vauxhall
Both companies
Lambeth
167, 654
301, 149
14, 632
192
182
00
114
60
00
Death rates from choleraDeath rates from choleraAccording to water company supplying sub districts of
London
Concepts of epidemiology Concepts of epidemiology
Definitions
“Epidemiology is defined as the study of the distribution and determinants of health related status or events in specified populations and the application of this study to control the health problems” (Last 1988)

Applications of epidemiologyApplications of epidemiology
The epidemiology is useful in:
1. Search of cause/causes of disease/diseases.
2. Helps to describe the health status of population or groups.
3. Helps to discover and bridge gaps in natural history of diseases.

4. Helps in controlling the diseases. To break
the weakest link in chain of transmission of
communicable diseases and reducing non
communicable diseases.
5. Helps in planning of health programs on
evidence basis and setting up of health
priorities.
6. Helps to evaluate health programs and
interventions.

7. Helps to determine the chances or
probability of occurrence of disease/
deaths and disability
8. Helps in better management of health
services and hospital services.
9. Helps to set-up cut-off levels between
normal and abnormal population and
establish trigger levels for action or
intervention.

Sources of Sources of epidemiological epidemiological MeasurementsMeasurements
1. Cross sectional surveys
2. Medical records
3. Death certificate
4. Census
5. Organizational data

Domains of epidemiologyDomains of epidemiology
Descriptive epidemiology
Descriptive epidemiology is the most Basic form of epidemiology. It is concerned with the description of the patterns of occurrence of health-related status or events in groups.
The determination of frequency and distribution of disease, incidence, prevalence, and mortality rates are included in descriptive epidemiology.
Analytical epidemiology
Analytical epidemiology is based on the observations made in the descriptive epidemiology. The design, execution andanalysis of subjects between groups helpsevaluate potential association between risk factors and health outcomes to answer the question “why?”.
Analytical epidemiology consists of
two types of research processes
1. Observational process
2. Experimental studies

Basic triads of descriptive and Basic triads of descriptive and analytical epidemiologyanalytical epidemiology
There are two different triads (3 essential
components) considered in studying different
sections

Descriptive epidemiology
Analytical epidemiology
Time (when) Host
Place (where) Agent
Person (who) Environment

Triad of descriptive Triad of descriptive epidemiologyepidemiology
Time
Changing or stable Seasonal variations Secular trends (long-term study of
incidence) Point source or propagated Cyclical variations (spikes of
incidences at regular intervals)
Place
Geographically restricted or wide
spread Relation to water and food supply Multiple cluster involvement or one Rural/Urban distribution
Triad of descriptive Triad of descriptive epidemiologyepidemiology

Person
Age Socio economic status Gender Ethnicity / Race Behavior
Triad of descriptive Triad of descriptive epidemiologyepidemiology

Triad of analytical Triad of analytical epidemiologyepidemiology
Agent Nutrients Poisons Allergens Radiation Physical trauma Microbes Psychological factors

Host factors
Genetic factors Immunologic state Age Personal behavior
Triad of analytical Triad of analytical epidemiologyepidemiology
Environment
Overcrowding Atmospheric changes Modes of transmission
Vector
Vehicle
Reservoir
Triad of analytical Triad of analytical epidemiologyepidemiology

Clinical epidemiology
When periodic observations are made over a long period of time in patients with a wide spectrum of clinical manifestations of the disease, a complete profile of the natural history of the disease may be obtained.
This forms the basis of clinical epidemiology.

Epidemiology of diseasesEpidemiology of diseases
Sri Lanka is said to be facing a double
disease burden due to communicable and non
communicable diseases (NCD) today.
What is triple burden???

The diseases burden in the country is given in
terms of (apart from basic measures)
1.Years of potential life lost
2.Life expectancy free from disability
3. Disability adjusted life years lost – DALYs
4.Quality adjusted life years lost - QUALYs
loss per 1000 population.
Country has to fight to control communicable
and non communicable diseases.

Epidemiology of communicable Epidemiology of communicable diseases (CCD)diseases (CCD)
Definition :- Communicable disease
A communicable or infectious disease is an
illness caused by transmission of a specific
infectious agent or its toxic products from an
infected person or animal to a susceptible
host, either directly or indirectly through an
intermediate animal host, vector or inanimate
environment (Last 1995)

Man to man
Animal to man
Disease TransmissionDisease Transmission

What is an Epidemic?What is an Epidemic?
It is the occurrence of cases of illness,
specific health related behavior or other
health related events clearly in excess of
normal expectancy in a community or region.
An Endemic diseaseAn Endemic disease
A disease that usually present in a
population or given area at a relatively high
prevalence and incidence rates in compared
to other areas.
E.g. Malaria is an endemic disease in
Polonnaruwa
Major emerging and re-emerging Major emerging and re-emerging infectious diseasesinfectious diseases
1. HIV/AIDS
2. Hepatitis B and Hepatitis C
3. Tuberculosis
4. Dengue
5. Malaria
6. Japanese encephalitis
7. Plague
8. Cholera

Major reasons for emergence of Major reasons for emergence of infectious diseasesinfectious diseases
High population growth, uncontrolled and unplanned urbanization,
Poor environmental sanitation, Migration of population, Natural disasters, Growing international trade, tourism and rapid travel, Alterations in microorganisms, Resistance to antimicrobials, Insecticide resistance, Weak public health system. Illiteracy and ignorance.

Chain of infection or chain Chain of infection or chain of transmissionof transmission
Infectious agent Transmission process Host
ENVIRONMENTS

Infectious agent
Pathogenicity Virulence Infectivity

This is the second important link in the
chain of infection.
Transmission is defined as “Spread of
infectious agent through the environment or to
another person, from the reservoir and
source”.
Transmission processTransmission process
Methods of transmissionMethods of transmission
Direct and Indirect

Direct methods of Direct methods of transmissiontransmission
Touching Kissing Sexual intercourse Child birth Breast-feeding Air borne, short distance via droplets
(by coughing, Laughing, sneezing, spitting). Transfusion of blood Transplacental from mother to fetus

Indirect transmissionIndirect transmission
Vehicle borne transmission (by
contaminated food and water) Vector borne transmission Parenteral by unsafe injection Fomite transmission Unclean hands

Control of communicable Control of communicable diseases (CCD)-discuss diseases (CCD)-discuss
under 5 headingsunder 5 headings
1. Control of infectious agents in the environments
2. Control of infectious agent in host
3. Control of outbreaks of CCD
4. Other measures
5. Specific measures for control of HIV epidemic

(1)(1) Control of infectious Control of infectious agents in the environmentsagents in the environments
Controlling sources of infection1. Supply of safe drinking water by treatment and
chlorination of water, pasteurization of milk.
2. Safe disposal of human excreta and animal excreta by sewerage system and sanitary latrines, compost pits/manure pits.
3. Control vectors of diseases – by source reduction and anti-larval and anti-adult measures.
4. Animals – vaccinate dogs against rabies and eliminate street dogs.
5. Rodent control measures-trapping and killing
6. Hospital waste management
7. Disinfections
(2)(2) Control of infectious Control of infectious agent agent in in hosthost
1. Reservoir control2. Practice of chemoprophylaxis3. Surveillance4. Notification5. Quarantine
1. Complete quarantine2. Modified quarantine
6. Isolation7. Education and behavior

(3)(3) Control of outbreaks of Control of outbreaks of CCD-different steps will beCCD-different steps will be
discussed laterdiscussed later
Communicable diseases like Malaria, JE, DHF , Hepatitis E & A, Hepatitis B andDiarrhoeal diseases quite often occur inepidemic proportion. Many local and focal outbreaks are being reported quite frequently;Hence, control of outbreaks of these diseases is an essential requirement.

(4)(4) Other measuresOther measures
1. Legislation
Epidemic disease control act. And
notification helps control of CCD.
2. Observe international health
regulations
Notifiable diseasesNotifiable diseases
Group A
• Cholera• Plague• Yellow fever

Group B
• Rubella• Diphtheria• Enteric fever• Food poisoning• Leptospirosis• Measles• Tuberculosis

• Whooping cough• Acute anterior poliomyelitis• Simple continued fever of over seven
days• Dengue• Dysentery • Encephalitis
• Human rabies• Malaria• Tetanus• Typhus fever• Viral Hepatitis



Epidemiology of non-Epidemiology of non-communicable diseases (NCD)communicable diseases (NCD)Non communicable diseases cover wide
range of heterogeneous conditions affecting
different organs and systems of different
socioeconomic groups.
Over the last two decades morbidity and
mortality due to cardiovascular diseases,
mental disorders, cancer and trauma have
been rising due to following causes.

CausesCauses
1. Rise in life expectancy and increasing
number of senior citizens.
2. Changing life styles: Faulty diet, use of
alcohol, sedentary life-physical inactivity
and rising stress-leading to obesity and
stress related problems.

3. Exposure to environmental risk factors-air
pollution.
4. Use of tobacco
5. Increasing population and rise in
automobiles and trauma incidence.

ImplicationsImplications
In view of the chronic morbidity and high cost involve in the management of non-communicable diseases attention need to be focused on prevention, early detection and appropriate management. Further, these diseases cause lot of disability and dependency and disease burden.

Multi - factorial originMulti - factorial origin
Causes of NCD are multi-factorial. Range
of life styles: risk taking behavior, changing
dietary pattern, physical inactivity, use of
alcohol and tobacco and stress in life have
been incriminated.
FutureFuture
For non-communicable diseases throughout
the all levels of care so as to reduce morbidity
and mortality.
1. Well-structured information education and
communication for primary and secondary
prevention of NCD.
2. Reorientation and skill up gradation of
health care providers
3. Establishment of Referral linkages between
primary secondary and tertiary institution.
4. Production and provision of drugs for NCD.
5. Development of institution for rehabilitation
of disabled persons due to NCD, teaching
persons to live with their disability.

6. Development of hospices for terminally ill
people who cannot have home based care.
7. Creation of epidemiological database on
NCD especially, CVD’s, strokes and
diabetes.