prof. dr. geneviève laureys stamceltransplantatie uz gent...antigen class hl lp hl cd-20...
TRANSCRIPT
11© 2008 Universitair Ziekenhuis Gent
Lymphoma in children
Prof. Dr. Geneviève Laureys
Pediatrische Hematologie, Oncologie en
Stamceltransplantatie
UZ Gent
BHS educational course: Seminar 12 - Hodgkin’s lymphoma & aggressive lymphoma 07-03-2015
22© 2008 Universitair Ziekenhuis Gent
Lymphoma in children:
• General aspects, different from treating adult
cancer
• Hodgkin Lymphoma
• Non Hodgkin Lymphoma
• Conclusions
33© 2008 Universitair Ziekenhuis Gent
Lymphoma in children: general aspects
“treating children with cancer (lymphoma) is
different from treating adults with cancer”
- Rare disease
- Definition of ‘Child’- Age limit: < 21, 18, 16, 15 y?
- International: 18 y
- Belgium:
• Cancer registry (2 groups: < 15 y and 15 - 19 y)
• PHO zorgplan/Plan cancer (MB 02/04/2014) < 16 y
• Pediatrie zorgplan/ (MB 02/04/2014) < 15 y
44© 2008 Universitair Ziekenhuis Gent
Lymphoma in children: general aspects
Lymphoma: 3rd Cildhood cancer: 13 %:
Belgium: ~40 à 45 new cases/ year
Non Hodgkin lymphoma:
Belgium < 15 y: ~25 patients/year, ~16 boys, 9 girls
Hodgkin lymphoma:
Belgium < 15 y: ~15 patients/year, ~9 boys, ~6 girls
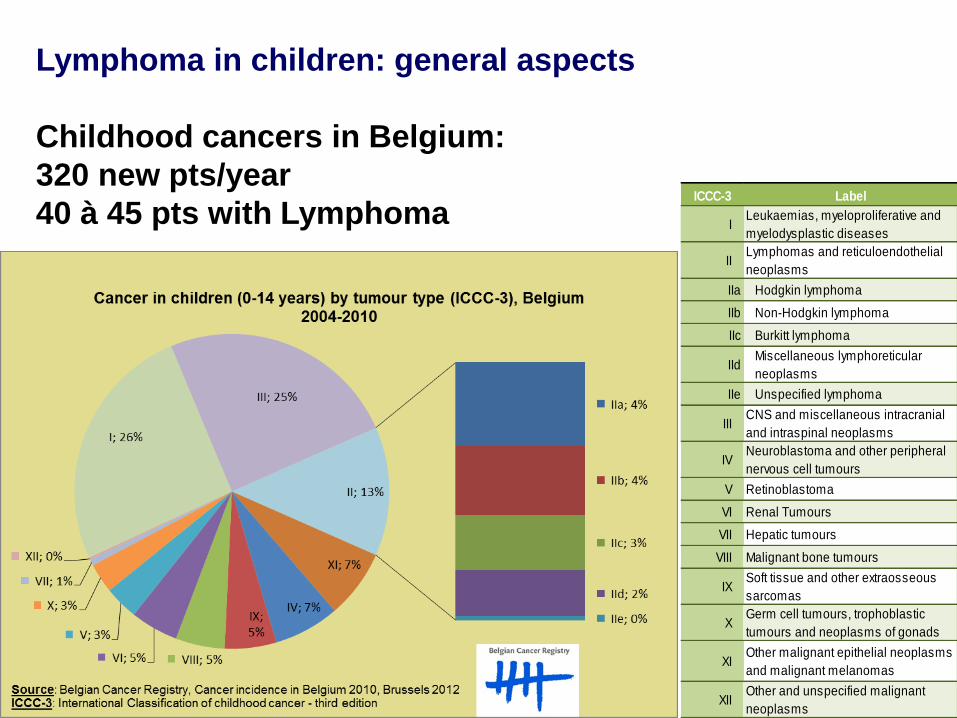
ICCC-3 Label
ILeukaemias, myeloproliferative and
myelodysplastic diseases
IILymphomas and reticuloendothelial
neoplasms
IIa Hodgkin lymphoma
IIb Non-Hodgkin lymphoma
IIc Burkitt lymphoma
IIdMiscellaneous lymphoreticular
neoplasms
IIe Unspecified lymphoma
IIICNS and miscellaneous intracranial
and intraspinal neoplasms
IVNeuroblastoma and other peripheral
nervous cell tumours
V Retinoblastoma
VI Renal Tumours
VII Hepatic tumours
VIII Malignant bone tumours
IXSoft tissue and other extraosseous
sarcomas
XGerm cell tumours, trophoblastic
tumours and neoplasms of gonads
XIOther malignant epithelial neoplasms
and malignant melanomas
XIIOther and unspecified malignant
neoplasms
Lymphoma in children: general aspects
Childhood cancers in Belgium:
320 new pts/year
40 à 45 pts with Lymphoma
66© 2008 Universitair Ziekenhuis Gent
Lymphoma in children: general aspects
Classification:
HL: diagnosis and classification comparable to adults
NHL: in children: high grade, urgency!
1. Mature B-cell NHL (Burkitt and Burkitt-like
lymphoma/leukemia and diffuse large B-cell lymphoma)
2. Lymphoblastic lymphoma (T or precursor B)
3. Anaplastic Large Cell Lymphoma
4. Rare: others
77© 2008 Universitair Ziekenhuis Gent
Lymphoma in children: general aspects
Clinical international trials: (almost) all patients registered or
in study protocols
BSPHO: Belgian Society for Pediatric Hematology and
Oncology: 7 Childhood Cancer Centers
2 Belgian representatives for each cancer type at
international meetings/working groups, HL and NHL: Anne
Uyttebroeck (Leuven), Geneviève Laureys (Gent)
Common protocols:
HL: EuroNet-PHL-Study-Group
NHL: EICNHL : European Intergroup for Childhood
Non Hodgkin Lymphoma (mature B-NHL and ALCL)
EORTC: pre-B and T-NHL (~leukemia protocol)
88© 2008 Universitair Ziekenhuis Gent
Lymphoma in children: general aspects
Prognosis:
non-Hodgkin lymphoma (NHL), 5-year overall survival:
• 88% in children < 15 years,
• 77% for adolescents (15 -19 years)
Hodgkin lymphoma:
• 94% for children and adolescents
Treatment: particular problems related to Childhood Cancer Treatment
• Off label use of drugs
• Dosages: according to age, weight, pharmacy preparations
• Chemotherapy and radiotherapy: growth, maturation in
developing body
99© 2008 Universitair Ziekenhuis Gent
Lymphoma in children: general aspects
Rehabilitation:
to achieve optimal survival and quality of life
Education/school:
to continue
Contact peers:
beneficial
Long term toxicity:
fertility
second cancers
organ toxicity
Ado weekend
1010© 2008 Universitair Ziekenhuis Gent
Lymphoma in children: general aspects
Children and adolescents with cancer:
Treated by -> multidisciplinary team of cancer specialists
with experience treating the cancers that occur during childhood
and adolescence, to insure that children receive treatment,
supportive care and rehabilitation that will achieve optimal survival
and quality of life.
Teacher Ado weekend
1111© 2008 Universitair Ziekenhuis Gent
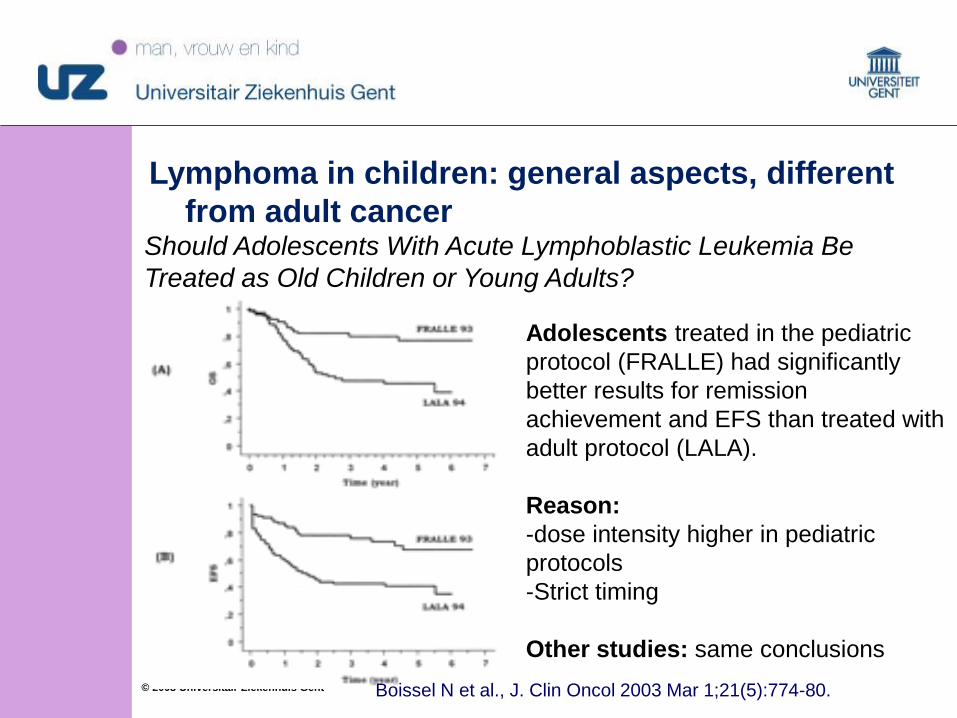
Lymphoma in children: general aspects, different
from adult cancerShould Adolescents With Acute Lymphoblastic Leukemia Be
Treated as Old Children or Young Adults?
Boissel N et al., J. Clin Oncol 2003 Mar 1;21(5):774-80.
Adolescents treated in the pediatric
protocol (FRALLE) had significantly
better results for remission
achievement and EFS than treated with
adult protocol (LALA).
Reason:
-dose intensity higher in pediatric
protocols
-Strict timing
Other studies: same conclusions
1212© 2008 Universitair Ziekenhuis Gent
Hodgkin Lymphoma in children
one of the few pediatric malignancies that shares
aspects of its biology and natural history with
an adult cancer
Epidemiology
Incidence
Diagnostic evaluation
Histology
Staging
Prognostic factors
Clinical case
Treatment/European trial
Prognosis
1313© 2008 Universitair Ziekenhuis Gent
Hodgkin Lymphoma in children
Epidemiology:
The male-to-female ratio varies markedly by age.
Children younger than 5 years show a strong male
predominance (M:F = 5.3) and children aged 15 to 19
years show a slight female predominance
Incidence:
6 % of childhood cancers?
Diagnostic evaluation
Physical examination, Blood, Rx, lymph node biopsy,
ultrasound, PET CT scan.
Bone marrow biopsy > IIA disease.,
1414© 2008 Universitair Ziekenhuis Gent
Hodgkin Lymphoma in children
Histology
1. Classical
- nodular sclerosing
- mixed cellularity
- lymphocyte-rich classical
- lymphocyte depletion
2. Lymphocyte-predominant
Staging:Ann Arbor Staging System adaptedI single lymph node region or single extralymphatic site
II 2 or more lymph node regions same side of diafragma
III lymph node regions on both sides diafragma may include
spleen or extralymphatic sites
IV diffuse extralymphatic disease (liver, bone marrow, lung,
skin)
A/B depending on symptoms
Antigen Class HL LP HL
CD-20 Occasionally
pos
Usually
pos
other B-cell
antigens
Usually neg Usually
pos
CD-30 pos negative
CD-15 Usually pos negative
Ig
expression
absent present
1515© 2008 Universitair Ziekenhuis Gent
Hodgkin Lymphoma in children
Prognostic factors:
Advanced stage of disease
Presence of B symptoms.
Presence of bulky disease.
Extranodal extension.
Elevated erythrocyte sedimentation rate.
Leukocytosis (white blood cell count 11,500/mm3 or
higher)
Anemia (hemoglobin lower than 11.0 g/dL).
Male gender

1616© 2008 Universitair Ziekenhuis Gent
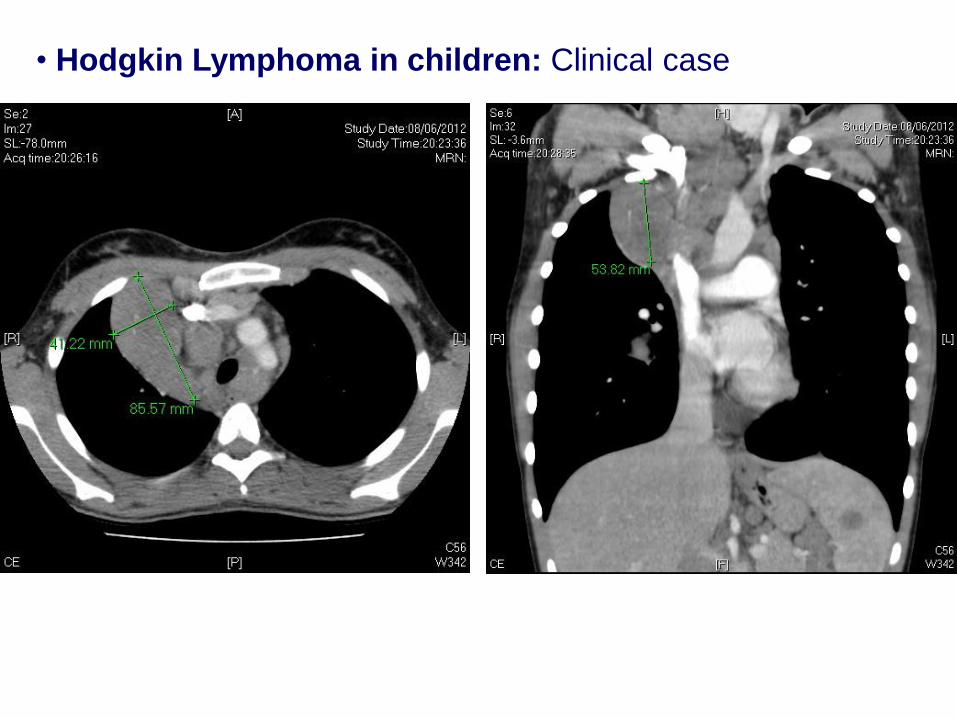
Hodgkin Lymphoma in children: Clinical case
girl, 14 years
Complaints: since a few weeks: fatigue, fever, night sweats,
weight loss, cough
Physical examination: LN supraclavicular right: 2x4cm, no
hepatosplenomegaly.
Blood: 10.3 g/dL, ESR: 59 mm, LDH: nl
Imaging: PET CT localisations: cervical, mediastinal,
parenchymatous lung lesions, spleen
Trachea: compression but not more than 50 %
• Hodgkin Lymphoma in children: Clinical case
1818© 2008 Universitair Ziekenhuis Gent
Biopsy: LN supraclavicular: Hodgkin, nodular sclerosis
Stage : IVB: Treatment Group 3
ENT: negative
bilateral bone marrow biopsy: negative,
Stage IV because of lung involvement, not contiguous
Discussion: ovarium preservation?
Done (laparascopy), during insertion PAC
Therapy: 2 x OEPA
Response evaluation: PET-CT: evaluation after 2 OEPA: adequate
response
Further treatment: Randomisation: 4 x COPDAC and no
radiotherapy
Hodgkin Lymphoma in children: Clinical case
1919© 2008 Universitair Ziekenhuis Gent
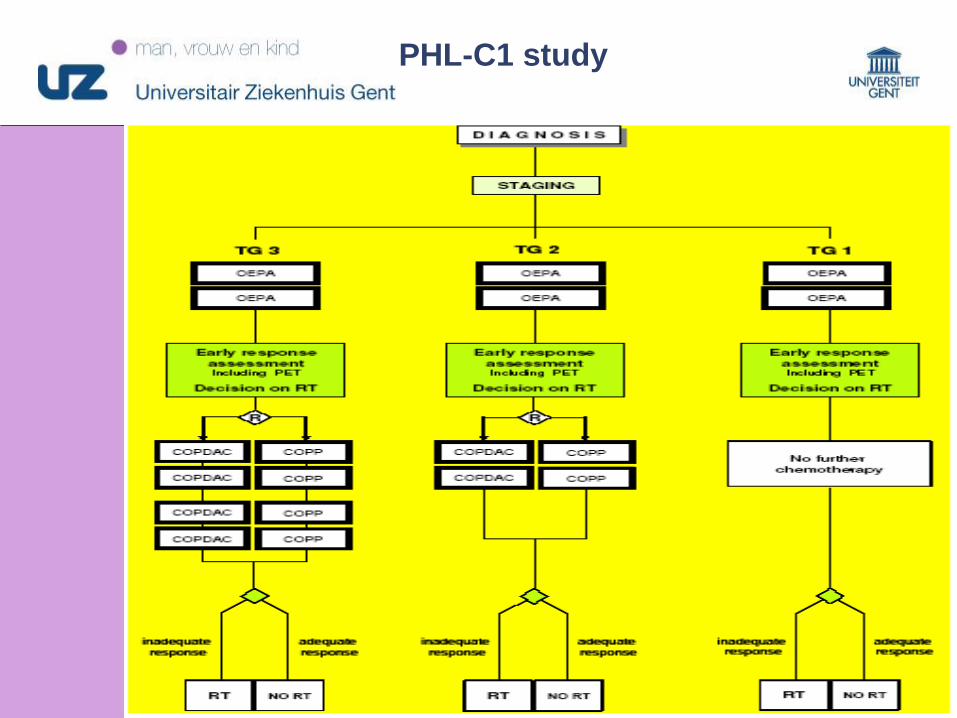
Hodgkin Lymphoma in children:
EuroNet-PHL-Study-Group C1: classic HL
Treatment groups:
TG-1: patients of stages I A/B and II A
TG-2: patients of stages IEA/B, IIEA, II B or III A
TG-3: patients of stages IIEB, IIIEA/B, III B or IV A/B
No radiotherapy if adequate reponse after 2 OEPA
Randomisation
TG-2 and TG-3: COPDAC versus COPP to avoid gonadal
damage
2020© 2008 Universitair Ziekenhuis Gent
PHL-C1 study
2121© 2008 Universitair Ziekenhuis Gent
Hodgkin Lymphoma in children
Results of PHL-C1 study: 2033 pts
TG-1: patients of stages I A/B and II A: 570pts
61 % : no RT, 39 % RT
TG-2: patients of stages IEA/B, IIEA, II B or III A
50 % : no RT, 50 % RT: 348 pts
TG-3: patients of stages IIEB, IIIEA/B, III B or IV A/B: 675 pts
32 % : no RT, 68 % RT
2222© 2008 Universitair Ziekenhuis Gent
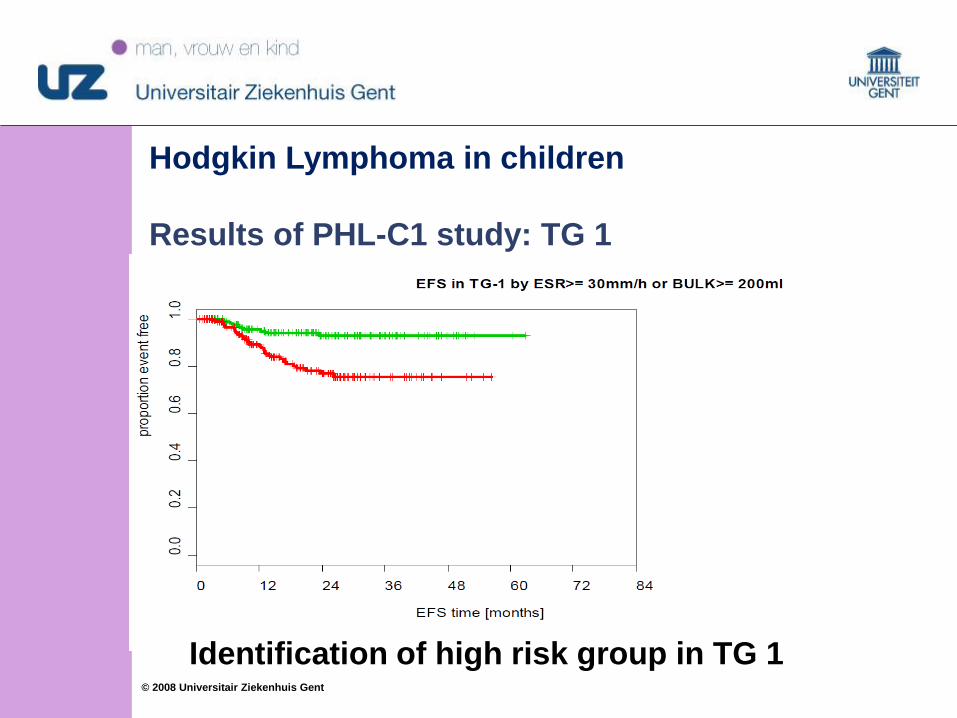
Hodgkin Lymphoma in children
Results of PHL-C1 study: TG 1
Identification of high risk group in TG 1
2323© 2008 Universitair Ziekenhuis Gent
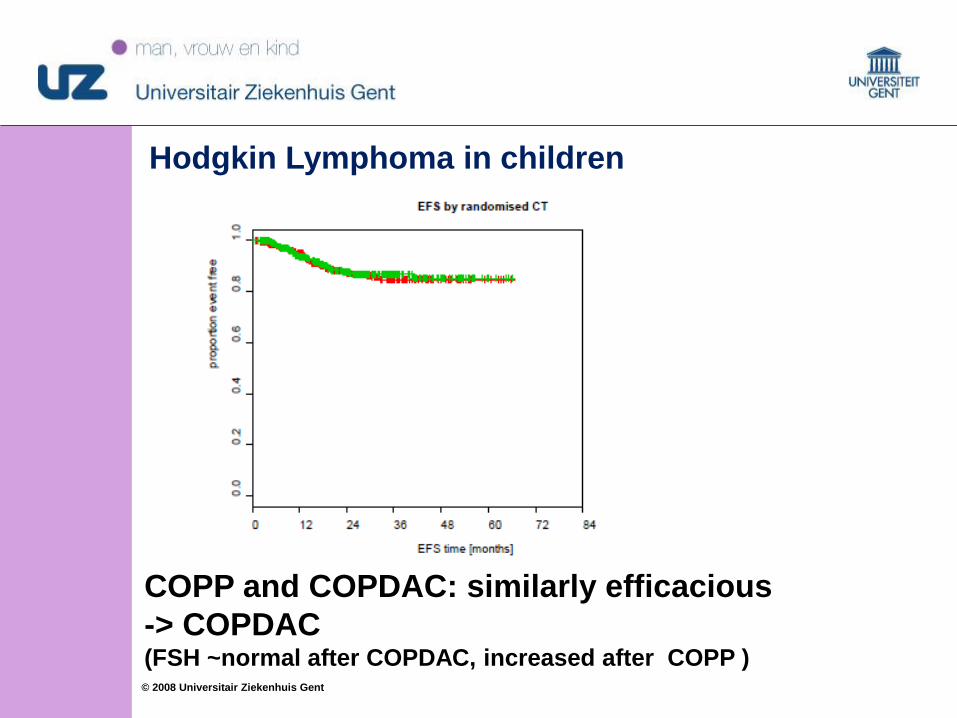
Hodgkin Lymphoma in children
COPP and COPDAC: similarly efficacious
-> COPDAC (FSH ~normal after COPDAC, increased after COPP )
2424© 2008 Universitair Ziekenhuis Gent
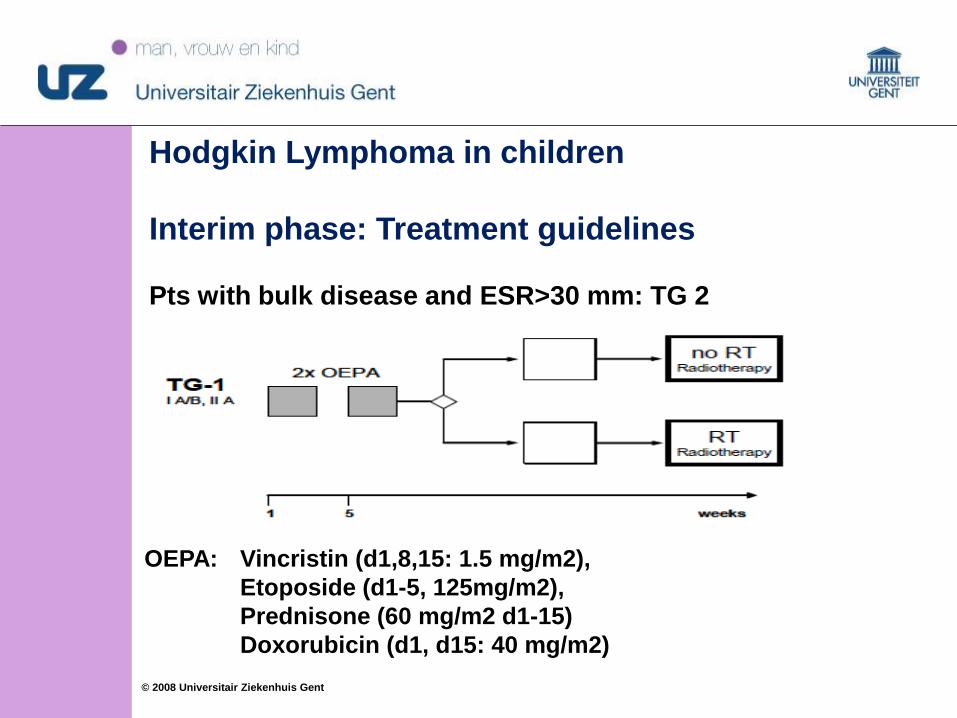
Hodgkin Lymphoma in children
Interim phase: Treatment guidelines
Pts with bulk disease and ESR>30 mm: TG 2
OEPA: Vincristin (d1,8,15: 1.5 mg/m2),
Etoposide (d1-5, 125mg/m2),
Prednisone (60 mg/m2 d1-15)
Doxorubicin (d1, d15: 40 mg/m2)
2525© 2008 Universitair Ziekenhuis Gent
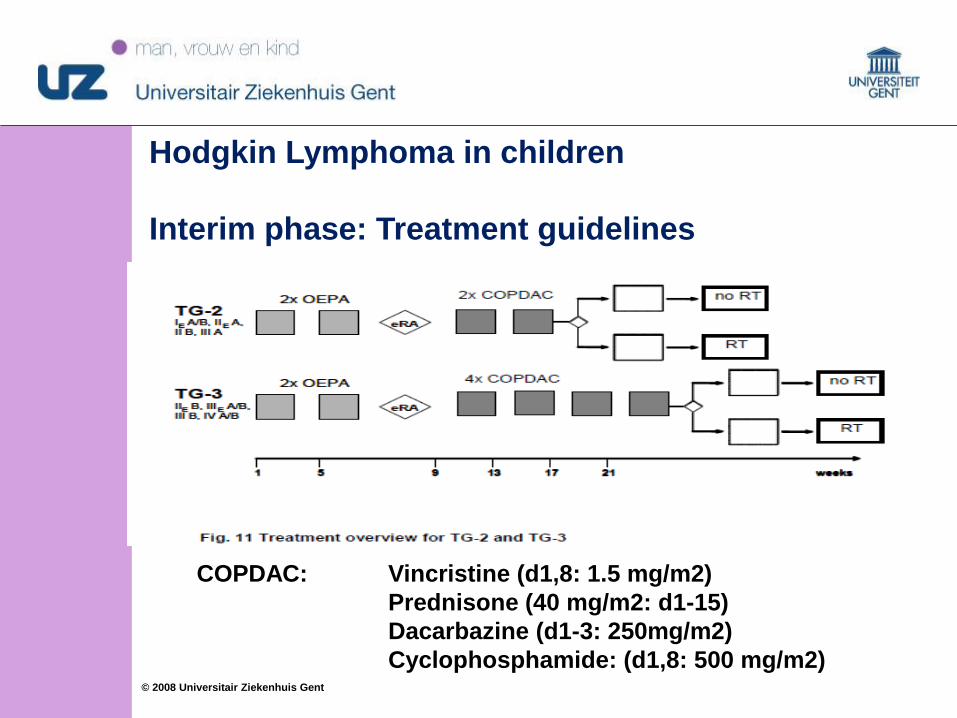
Hodgkin Lymphoma in children
Interim phase: Treatment guidelines
COPDAC: Vincristine (d1,8: 1.5 mg/m2)
Prednisone (40 mg/m2: d1-15)
Dacarbazine (d1-3: 250mg/m2)
Cyclophosphamide: (d1,8: 500 mg/m2)
2626© 2008 Universitair Ziekenhuis Gent
Hodgkin Lymphoma in children
Prognosis
EFS: > 90 %
OS : > 85 %
Late effects
- Growth impairment after radiation
- Hypothyroidy
- Second tumours
2727© 2008 Universitair Ziekenhuis Gent
Non Hodgkin Lymphoma in children
Almost all NHL in children are high grade
Different NHL subtypes require different treatment
strategies
Epidemiology
Incidence
Diagnostic evaluation
Histology
Staging
Prognostic factors
Clinical cases
Treatment/European trial
Prognosis and Late effects
2828© 2008 Universitair Ziekenhuis Gent
Non Hodgkin Lymphoma in children
1. Mature B-cell NHL (Burkitt and Burkitt-like lymphoma) and
diffuse large B-cell lymphoma
40 à 50 %, 5-y EFS: 90 %
2. Lymphoblastic lymphoma (primarily precursor T-cell
lymphoma, precursor B-cell lymphoma)
30 à 40 %, 5-y EFS: 85 %
3. Anaplastic large cell lymphoma (T-cell or null-cell
lymphomas)
10 à 15 %, 5-y EFS: 75 %
(4. Very rare: peripheral T-cell lymphoma, NK lymphomas,
cutaneous lymphomas, and indolent B-cell lymphomas (e.g.,
follicular lymphoma)
2929© 2008 Universitair Ziekenhuis Gent
Non Hodgkin Lymphoma in children
Diagnostic evaluation- Sample: tumour/ LN/ fluid/ BM
- Cytomorphology
- Histomorphology
- Immunophenotyping
- Cytogenetics
-> correct classification and allocation of patients to
appropriate treatment subgroups, according to the WHO
classification
ultrasound, PET CT scan, bone marrow (biopsy), CNS
Staging: St.Jude Staging system (Murphy)
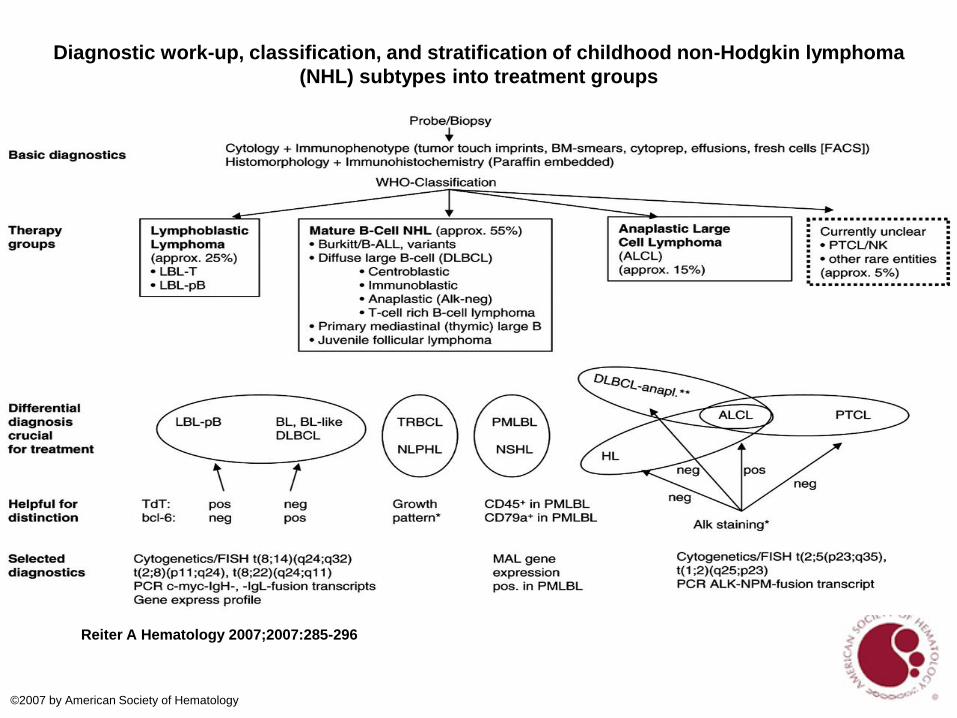
Diagnostic work-up, classification, and stratification of childhood non-Hodgkin lymphoma
(NHL) subtypes into treatment groups
Reiter A Hematology 2007;2007:285-296
©2007 by American Society of Hematology
3131© 2008 Universitair Ziekenhuis Gent
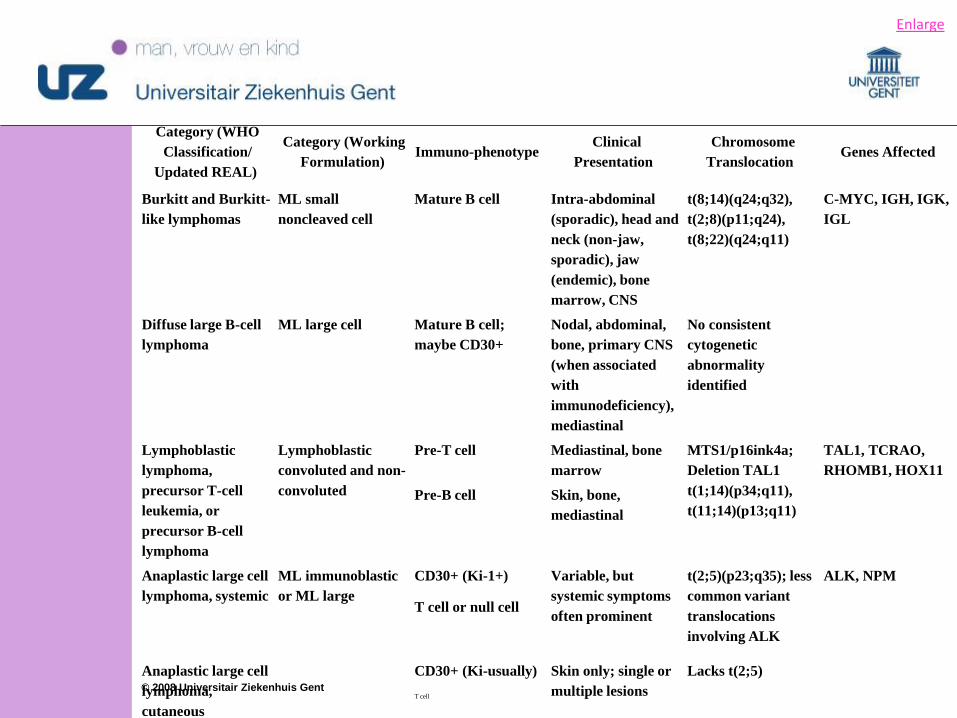
Category (WHO
Classification/
Updated REAL)
Category (Working
Formulation)Immuno-phenotype
Clinical
Presentation
Chromosome
Translocation Genes Affected
Burkitt and Burkitt-
like lymphomas
ML small
noncleaved cell
Mature B cell Intra-abdominal
(sporadic), head and
neck (non-jaw,
sporadic), jaw
(endemic), bone
marrow, CNS
t(8;14)(q24;q32),
t(2;8)(p11;q24),
t(8;22)(q24;q11)
C-MYC, IGH, IGK,
IGL
Diffuse large B-cell
lymphoma
ML large cell Mature B cell;
maybe CD30+
Nodal, abdominal,
bone, primary CNS
(when associated
with
immunodeficiency),
mediastinal
No consistent
cytogenetic
abnormality
identified
Lymphoblastic
lymphoma,
precursor T-cell
leukemia, or
precursor B-cell
lymphoma
Lymphoblastic
convoluted and non-
convoluted
Pre-T cell Mediastinal, bone
marrow
MTS1/p16ink4a;
Deletion TAL1
t(1;14)(p34;q11),
t(11;14)(p13;q11)
TAL1, TCRAO,
RHOMB1, HOX11
Pre-B cell Skin, bone,
mediastinal
Anaplastic large cell
lymphoma, systemic
ML immunoblastic
or ML large
CD30+ (Ki-1+) Variable, but
systemic symptoms
often prominent
t(2;5)(p23;q35); less
common variant
translocations
involving ALK
ALK, NPM
T cell or null cell
Anaplastic large cell
lymphoma,
cutaneous
CD30+ (Ki-usually) Skin only; single or
multiple lesions
Lacks t(2;5)
T cell
Enlarge
3232© 2008 Universitair Ziekenhuis Gent
Non Hodgkin Lymphoma in children:
Prognostic factors: Age:
> 15 years: poorer outcome, but attributable primarily to
patients with diffuse large B-cell lymphoma
rare in infants , < 1 %, but inferior outcome
Site:
no effect of bone, testicular disease
mediastinal involvement: inferior outcome
primary mediastinal B-cell lymphoma, 3-year EFS: 50% -
70%
CNS/BM disease at presentation: 3-year EFS : 70% (B-NHL)
Tumor burden
Response to treatment
Chromosomal Abnormalities
3333© 2008 Universitair Ziekenhuis Gent
Non Hodgkin Lymphoma in
children: clinical cases
Boy, 8 years old
GP: for constipation, phys. examination: fecaloma?
R/ enema -> no result
Pediatrician in hospital: R/enemas, stools but still mass
palpable, examination: ultrasound, CT scan-> abdominal
mass suprapubic
Referral to UH Ghent: 01/03/2015
Blood: Blood counts: normal, LDH: elevated < less than 2
times upper limit
3434© 2008 Universitair Ziekenhuis Gent
Non Hodgkin Lymphoma in
children: clinical cases
Open biopsy: Diagnosis: Burkitt- NHL, kappa positive
Staging
PET CT: no other localisations
Bone marrow: negative
CNS: negative
Stage III according to Murphy
3535© 2008 Universitair Ziekenhuis Gent
1. Mature B-cell NHL (Burkitt and Burkitt-like
lymphoma/leukemia and diffuse large B-cell lymphoma)
Extremely high proliferative (treatment urgent)
Principles of treatment:
-maintain cytotoxic active drug concentrations over a
period sufficient to affect as many lymphoma cells as
possible during the vulnerable active cell cycle
combining drugs with different mechanisms of action
and few overlapping toxicities
high-dose intensity over time, keeping between-
treatment- intervals short
efficient CNS-directed therapy to address the strong
tendency for invasion of the CNS
3636© 2008 Universitair Ziekenhuis Gent
Non Hodgkin Lymphoma in children
1. Mature B-cell NHL (Burkitt and Burkitt-like
lymphoma/leukemia and diffuse large B-cell lymphoma)
• current highly efficacious regimen ~ considerable acute
toxicity
• 3% risk to die from treatment-related complications, ‘acute
tumour cell lysis syndrome’
• oro-intestinal mucositis, and severe neutropenia->
admissions for febrile neutropenia episods -> prompt
antibiotic treatment
3737© 2008 Universitair Ziekenhuis Gent
Non Hodgkin Lymphoma in children
1. Mature B-cell NHL (Burkitt and Burkitt-like
lymphoma/leukemia and diffuse large B-cell lymphoma)
• Most relapses occur during therapy
• Short treatment (cfr stage and risk group):
COP-COPADEM1-COPADEM2-CYM 1-CYM2: 14 ww
COP-COPADEM1-COPADEM2-CYVE1-(HDMTX)- CYVE 2- M1-
M2 (20 ww)
• no radiotherapy
• Few relapses after 1 year post stop treatment
• 5-y EFS: 90 %
3838© 2008 Universitair Ziekenhuis Gent
Non Hodgkin Lymphoma in children: 1. Mature B-cell NHL
Treatment: Intergroup trial for children or adolescents with B-
cell NHL or B-AL: evaluation of Rituximab efficacy and
safety
Rationale:
Rituximab has extended the survival of adult pts with Diffuse
Large B-Cell lymphoma (DLBL) and is standard treatment of
B-cell lymphoma in adults.
Questions: Efficacy and safety of rituximab added to
chemotherapy in childhood lymphoma?
Results from adult B-NHL cannot be assumed to apply to
children, because of differences in biology, > 75 % of
childhood B lymphoma are Burkitt type (efficacy of
rituximab?) and not DLBL
3939© 2008 Universitair Ziekenhuis Gent
Non Hodgkin Lymphoma in children: 1. Mature B-cell NHL
Evaluation of Rituximab efficacy and safety
EFS: is high in children: 90 %,
EFS: stage III with LDH > Nx2 and stage IV or B-AL: 84 %
Rituximab: expensive, severe side effects (prolonged B-
cell depletion): clinical case: not included (LDH)
randomised trial: evaluation whether 6 injections of
Rituximab to standard chemo improves EFS
Planned: inclusion of 600 pts (Stage III-Stage IV or B-AL)
registration: Primary mediastinal large B-cell lymphoma
(PMBL): same disease as in adults? all patients receive
Rituximab!
4040© 2008 Universitair Ziekenhuis Gent
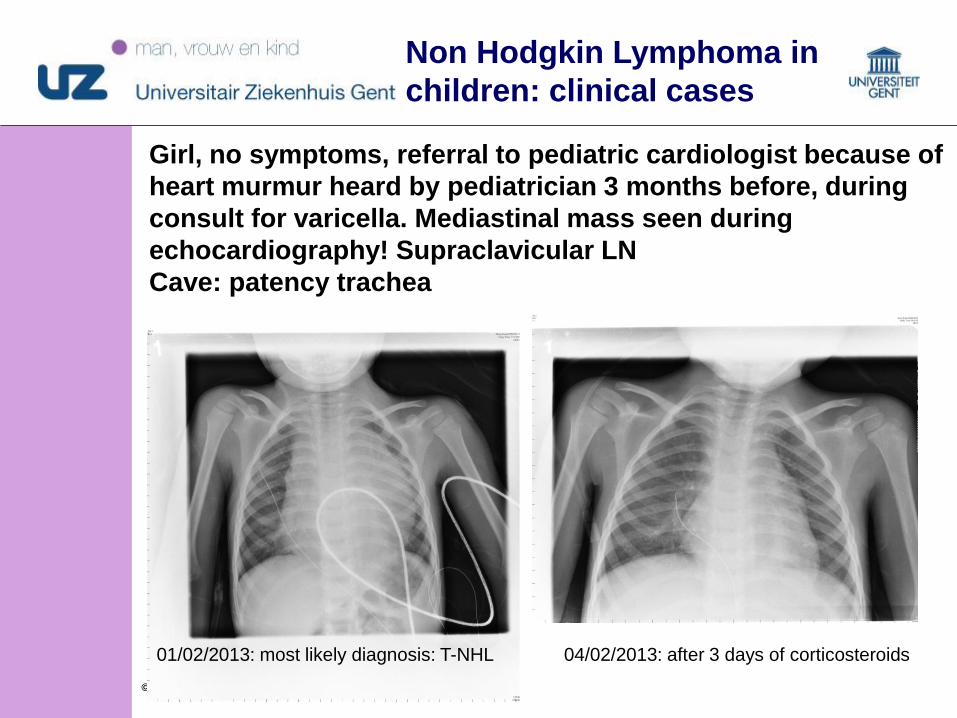
04/02/2013: after 3 days of corticosteroids01/02/2013: most likely diagnosis: T-NHL
Girl, no symptoms, referral to pediatric cardiologist because of
heart murmur heard by pediatrician 3 months before, during
consult for varicella. Mediastinal mass seen during
echocardiography! Supraclavicular LN
Cave: patency trachea
Non Hodgkin Lymphoma in
children: clinical cases
4141© 2008 Universitair Ziekenhuis Gent
Non Hodgkin Lymphoma in
children: clinical cases
CT thorax: Diameter trachea (CT) < 50 %: High risk
general/local anesthesia! Minimal touch!
Cave: Vena cava superior syndrome!
Start of corticosteroids treatment without diagnostic
biopsy
biopsy was performed from supraclavicular lymph node
4 days later
Diagnosis T-NHL
Treatment: (cfr T-ALL treatment) EORTC 58801: based
on the principle of continuous exposure to cytostatics
over long period of time (2 years) , 5-y S: 85 %
4242© 2008 Universitair Ziekenhuis Gent
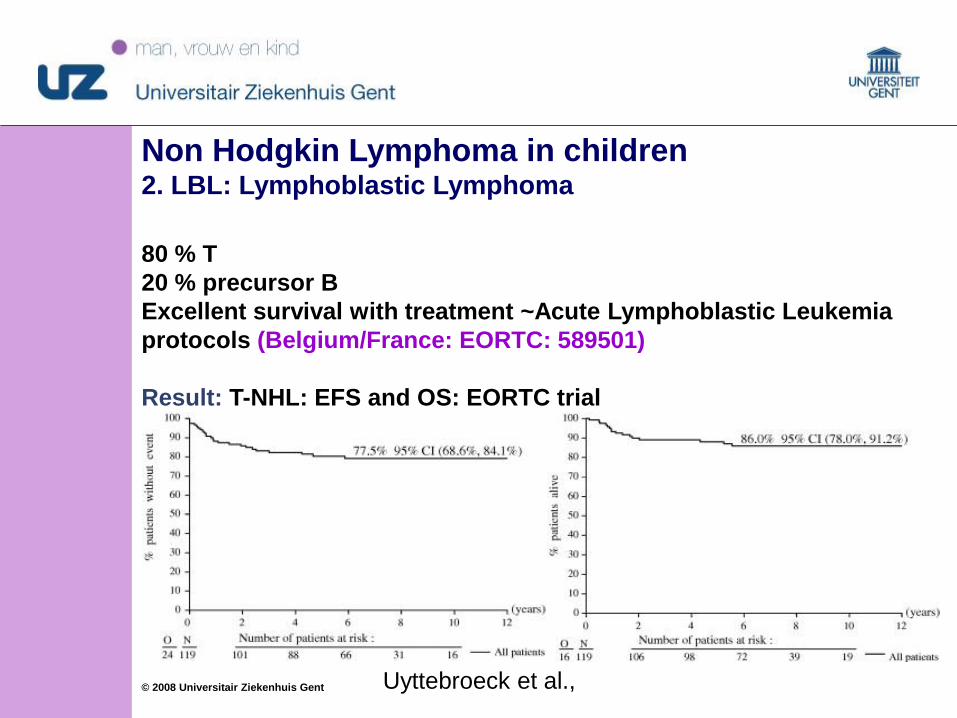
Non Hodgkin Lymphoma in children2. LBL: Lymphoblastic Lymphoma
80 % T
20 % precursor B
Excellent survival with treatment ~Acute Lymphoblastic Leukemia
protocols (Belgium/France: EORTC: 589501)
Result: T-NHL: EFS and OS: EORTC trial
Uyttebroeck et al.,
4343© 2008 Universitair Ziekenhuis Gent
Girl, 8 y
Complaints:
vomiting, diarrhea, fever,
paleness.
R/antibiotics
1 week later: Lymph nodes
enlargement, cervical, anorexia,
skin eruption
Physical examination:
hepatosplenomegaly, skin rash,
LN
Blood: normal
Non Hodgkin Lymphoma
in children: clinical cases
4444© 2008 Universitair Ziekenhuis Gent
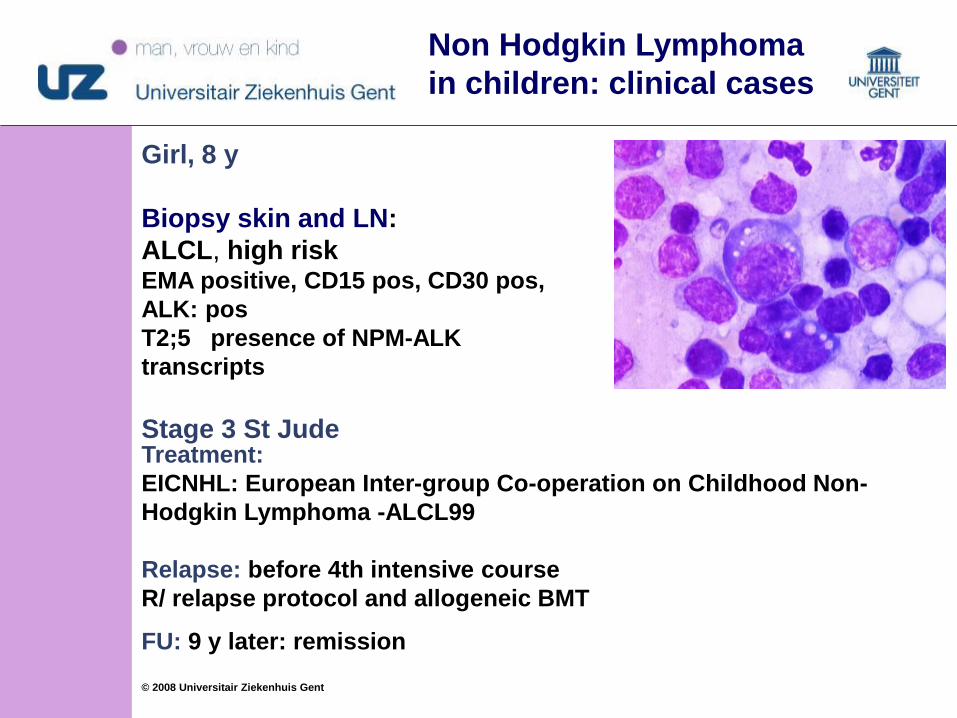
Girl, 8 y
Biopsy skin and LN:
ALCL, high riskEMA positive, CD15 pos, CD30 pos,
ALK: pos
T2;5 presence of NPM-ALK
transcripts
Stage 3 St Jude
Non Hodgkin Lymphoma
in children: clinical cases
Treatment:
EICNHL: European Inter-group Co-operation on Childhood Non-
Hodgkin Lymphoma -ALCL99
Relapse: before 4th intensive course
R/ relapse protocol and allogeneic BMT
FU: 9 y later: remission
4545© 2008 Universitair Ziekenhuis Gent
Non Hodgkin Lymphoma in children
3. ALCL: Anaplastic Large Cell Lymphoma
ALCL-99 :
Randomisation: All patients:
6 courses of MTX 1 g/m2 24 hrs and IT (MTX1 )
6 courses of MTX 3 g/m2 over 3 hours without IT (MTX3)
-> EFS comparable
Randomisation: Children and adolescents with high-risk ALCL:
After a prephase and one chemotherapy course
5 chemotherapy courses / 5 chemotherapy courses and vinblastine
injections (6 mg/m(2) during each course followed by weekly
vinblastine, 1 year of treatment.
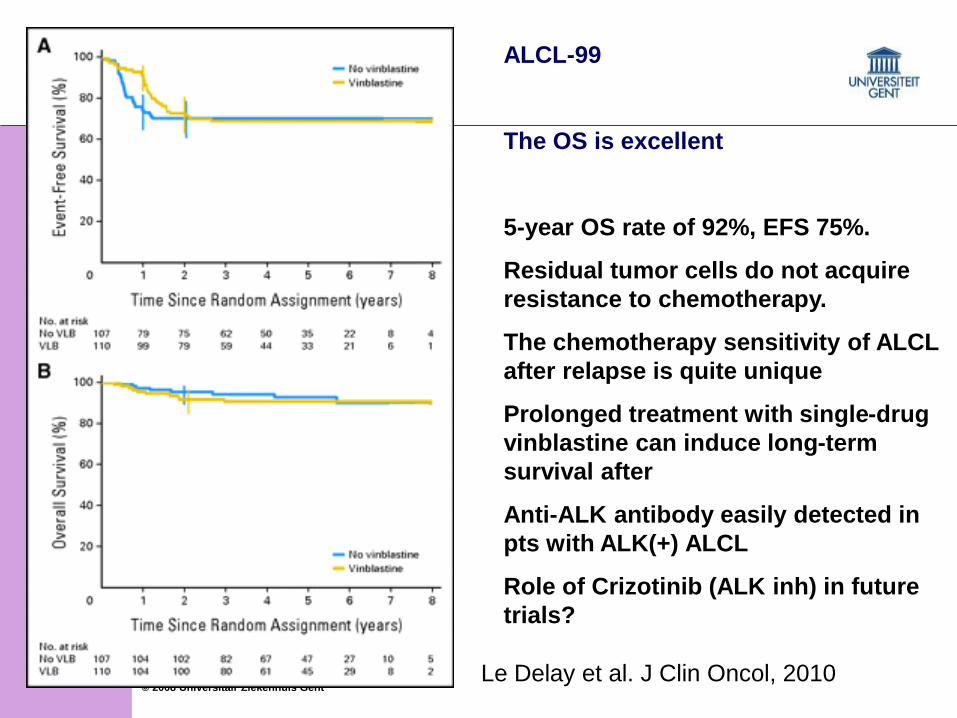
4646© 2008 Universitair Ziekenhuis Gent
ALCL-99
The OS is excellent
5-year OS rate of 92%, EFS 75%.
Residual tumor cells do not acquire
resistance to chemotherapy.
The chemotherapy sensitivity of ALCL
after relapse is quite unique
Prolonged treatment with single-drug
vinblastine can induce long-term
survival after
Anti-ALK antibody easily detected in
pts with ALK(+) ALCL
Role of Crizotinib (ALK inh) in future
trials?
Le Delay et al. J Clin Oncol, 2010
4747© 2008 Universitair Ziekenhuis Gent
• Lymphoma in children: Conclusions
- Excellent cure rates
- Challenge: to minimize long term effects without
affecting excellent survival rates
- Role of radiotherapy? used for Hodgkin lymphoma if
insufficient response after 2 chemotherapy courses
- Hodgkin disease: presentation, staging and outcome in
children is comparable with Hodgkin lymphoma in adults
- Non Hodgkin lymphoma in children: high grade cancer,
urgent treatment necessary
- Non Nodgkin lymphoma subtypes of childhood exhibit
significant differences in terms of molecular and cellular
biology and clinical features: crucial for determining
therapeutic strategies
4848© 2008 Universitair Ziekenhuis Gent
Lymphoma in children: Conclusions
- Invasive diagnostic procedures may be dangerous, e.g. in
case mediastinal tumour/v.cava superior syndrome,
typical for T-NHL, postpone biopsy and start treatment
first
- Children/adolescents with cancer -> to be treated by
multidisciplinary team of specialists with experience in
childhood cancer to ensure that children receive
treatment, supportive care, and rehabilitation that will
achieve optimal survival and quality of life.
4949© 2008 Universitair Ziekenhuis Gent
“
5050© 2008 Universitair Ziekenhuis Gent
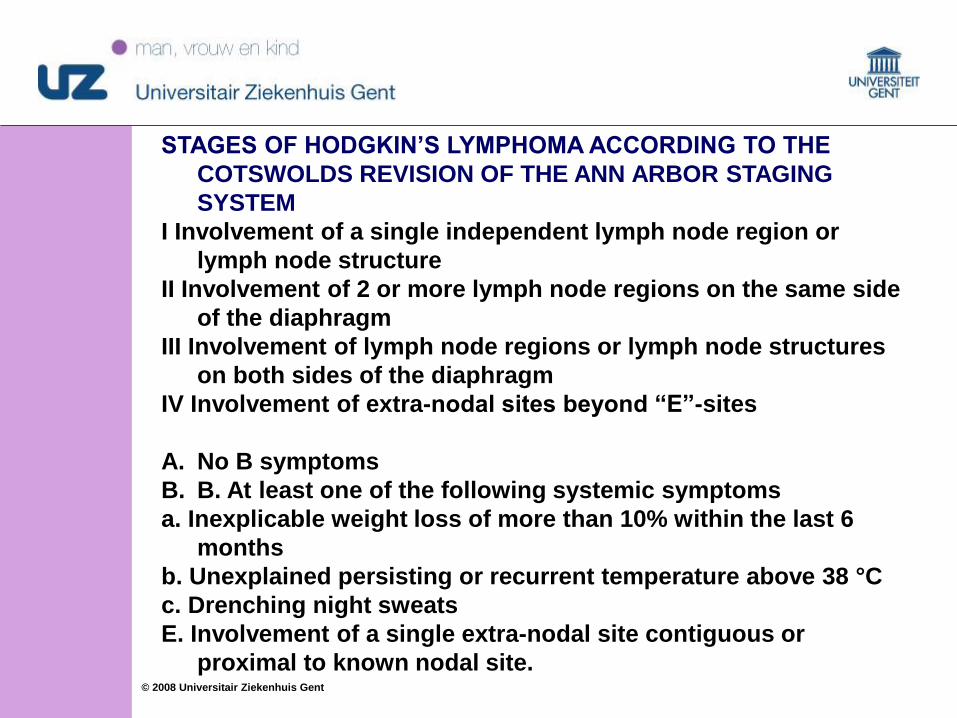
STAGES OF HODGKIN’S LYMPHOMA ACCORDING TO THE
COTSWOLDS REVISION OF THE ANN ARBOR STAGING
SYSTEM
I Involvement of a single independent lymph node region or
lymph node structure
II Involvement of 2 or more lymph node regions on the same side
of the diaphragm
III Involvement of lymph node regions or lymph node structures
on both sides of the diaphragm
IV Involvement of extra-nodal sites beyond “E”-sites
A. No B symptoms
B. B. At least one of the following systemic symptoms
a. Inexplicable weight loss of more than 10% within the last 6
months
b. Unexplained persisting or recurrent temperature above 38 °C
c. Drenching night sweats
E. Involvement of a single extra-nodal site contiguous or
proximal to known nodal site.
5151© 2008 Universitair Ziekenhuis Gent
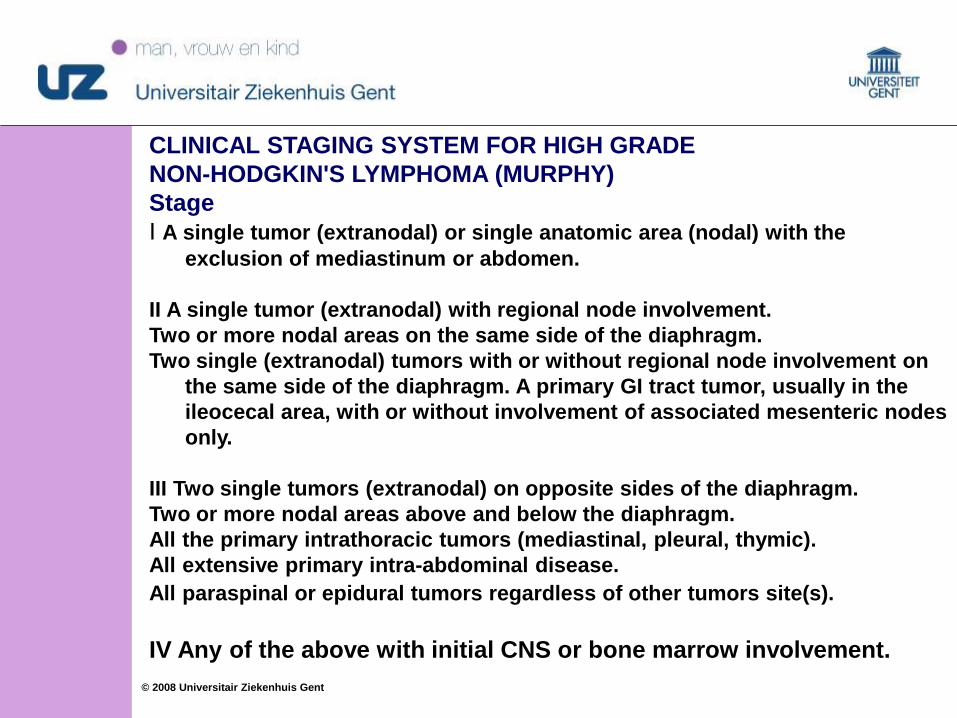
CLINICAL STAGING SYSTEM FOR HIGH GRADE
NON-HODGKIN'S LYMPHOMA (MURPHY)
Stage
I A single tumor (extranodal) or single anatomic area (nodal) with the
exclusion of mediastinum or abdomen.
II A single tumor (extranodal) with regional node involvement.
Two or more nodal areas on the same side of the diaphragm.
Two single (extranodal) tumors with or without regional node involvement on
the same side of the diaphragm. A primary GI tract tumor, usually in the
ileocecal area, with or without involvement of associated mesenteric nodes
only.
III Two single tumors (extranodal) on opposite sides of the diaphragm.
Two or more nodal areas above and below the diaphragm.
All the primary intrathoracic tumors (mediastinal, pleural, thymic).
All extensive primary intra-abdominal disease.
All paraspinal or epidural tumors regardless of other tumors site(s).
IV Any of the above with initial CNS or bone marrow involvement.
5252© 2008 Universitair Ziekenhuis Gent
Non Hodgkin Lymphoma in children
Epidemiology:
Burkitt lymphoma mature B-cell lymphoma:
15% of cases in Europe or the United States will have EBV
detectable in the tumor tissue
immunodeficiency, both congenital and acquired (human
immunodeficiency virus infection [HIV] or posttransplant
immunodeficiency),
Rare as secondary malignancy
PTLD
5353© 2008 Universitair Ziekenhuis Gent
• Non Hodgkin Lymphoma in children
1. Mature B-cell NHL (Burkitt and Burkitt-like lymphoma/leukemia
and diffuse large B-cell lymphoma).
40 à 50 %
Rapidly repeated dose-intense chemotherapy courses
5-y EFS: 90 %
2. Lymphoblastic lymphoma (LBL)
30 à 40 % (numbers may vary according to study/population/age
limit)
Therapeutic protocols cfr ALL, (Belgium: EORTC) based on the
principle of continual exposure to cytostatics over long period of
time
5-y EFS: 85 %
3. Anaplastic large cell lymphoma (mature T-cell or null-cell
lymphomas):
10 à 15 %
different therapeutic strategies? EICNHL-ALCL, 6 courses
5-y EFS: 75 %