product/technology strategy
TRANSCRIPT

5/15/2017
1
MSGERC First Biennial Meeting Asilomar, California, 2016Jack Edwards
Efforts to Develop A Vaccine for Candida:
Scientific and Developmental Challenges
Disclosure
One of six scientific co-founders who hold equity and consult for NovaDigmTherapeutics, Inc.
Biotechnology company established in collaboration with the LABiomedical Research Institute at Harbor/UCLA, the NIH, the DoD, and Domain Partners specifically to develop a Candidavaccine.
“A Scientist Over the Age of 60Does More Harm Than Good.”
Thomas Huxley1825-1895
Nick Name: “Darwin’s Bulldog”
5/15/2017
2
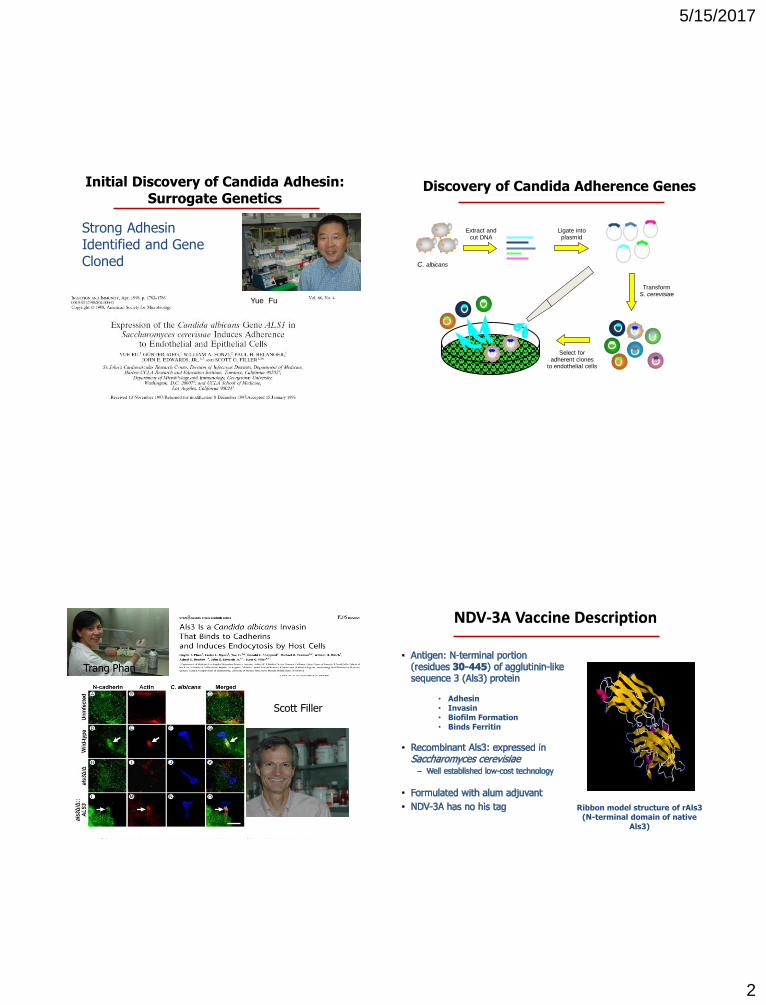
Strong AdhesinIdentified and Gene Cloned
Initial Discovery of Candida Adhesin:Surrogate Genetics
Yue Fu
Discovery of Candida Adherence Genes
Extract andcut DNA
C. albicans
Ligate intoplasmid
TransformS. cerevisiae
Select foradherent clones
to endothelial cells
Scott Filler
Trang Phan
Ribbon model structure of rAls3 (N-terminal domain of native
Als3)
NDV-3A Vaccine Description
• Adhesin• Invasin• Biofilm Formation• Binds Ferritin
5/15/2017
3
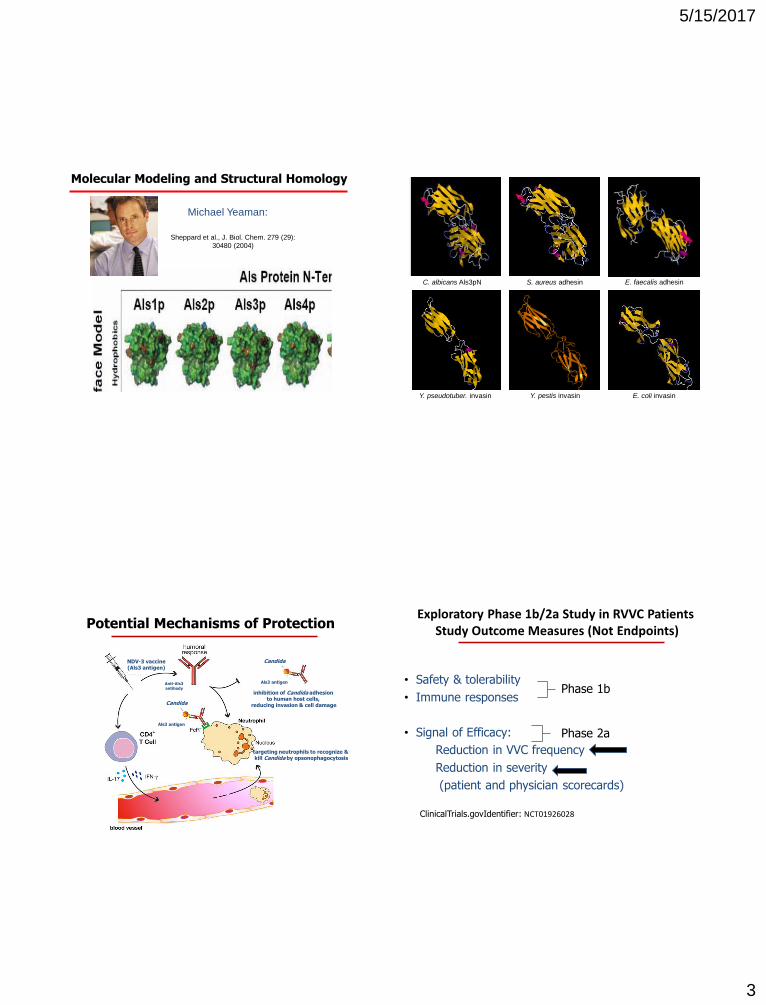
Molecular Modeling and Structural Homology
Michael Yeaman:
Sheppard et al., J. Biol. Chem. 279 (29):
30480 (2004)
C. albicans Als3pN S. aureus adhesin
Y. pseudotuber. invasin Y. pestis invasin E. coli invasin
E. faecalis adhesin
Potential Mechanisms of Protection
NDV-3 vaccine(Als3 antigen)
Candida
Anti-Als3 antibody
Als3 antigen
Als3 antigen
Candida
inhibition of Candida adhesion to human host cells,
reducing invasion & cell damage
targeting neutrophils to recognize & kill Candida by opsonophagocytosis
Exploratory Phase 1b/2a Study in RVVC PatientsStudy Outcome Measures (Not Endpoints)
• Safety & tolerability
• Immune responses
• Signal of Efficacy:
Reduction in VVC frequency
Reduction in severity
(patient and physician scorecards)
ClinicalTrials.govIdentifier: NCT01926028
Phase 1b
Phase 2a
5/15/2017
4
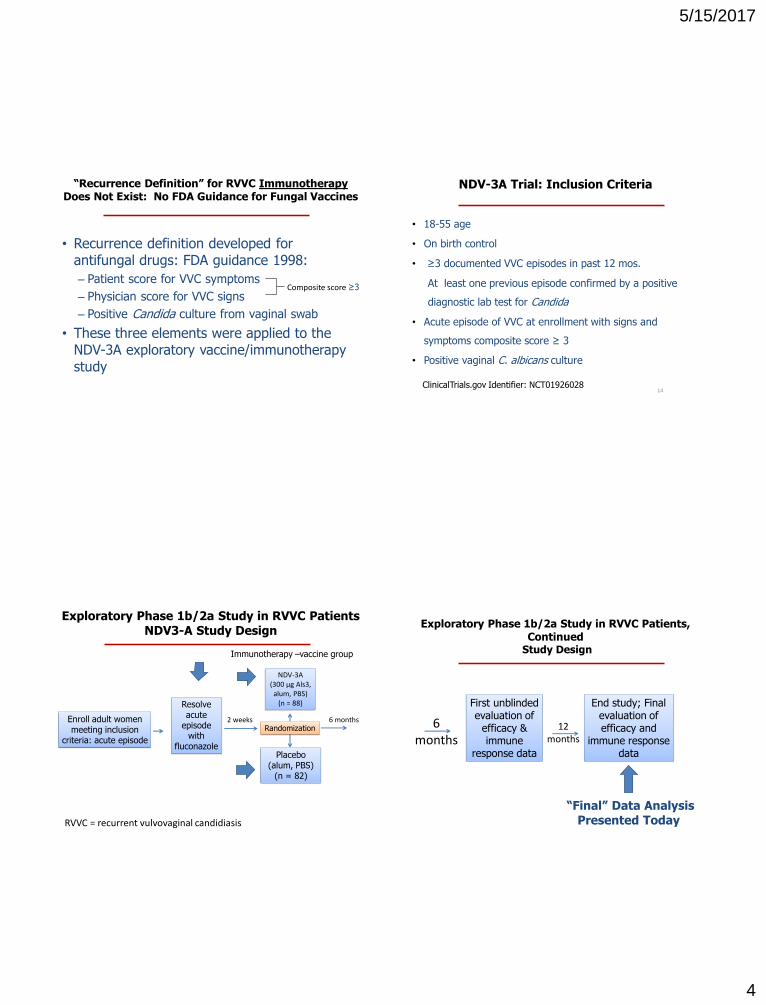
“Recurrence Definition” for RVVC ImmunotherapyDoes Not Exist: No FDA Guidance for Fungal Vaccines
• Recurrence definition developed for antifungal drugs: FDA guidance 1998:
– Patient score for VVC symptoms
– Physician score for VVC signs
– Positive Candida culture from vaginal swab
• These three elements were applied to the NDV-3A exploratory vaccine/immunotherapy study
Composite score ≥3
NDV-3A Trial: Inclusion Criteria
• 18-55 age
• On birth control
• ≥3 documented VVC episodes in past 12 mos.
At least one previous episode confirmed by a positive
diagnostic lab test for Candida
• Acute episode of VVC at enrollment with signs and
symptoms composite score ≥ 3
• Positive vaginal C. albicans culture
14ClinicalTrials.gov Identifier: NCT01926028
Exploratory Phase 1b/2a Study in RVVC PatientsNDV3-A Study Design
RVVC = recurrent vulvovaginal candidiasis
Enroll adult women meeting inclusion
criteria: acute episode
Resolve acute
episode with
fluconazolePlacebo
(alum, PBS)(n = 82)
NDV-3A(300 μg Als3, alum, PBS)
(n = 88)
Immunotherapy –vaccine group
6 monthsRandomization
2 weeks
Exploratory Phase 1b/2a Study in RVVC Patients, Continued
Study Design
First unblinded evaluation of
efficacy & immune
response data
6months
12 months
End study; Final evaluation of efficacy and
immune response data
“Final” Data AnalysisPresented Today
5/15/2017
5
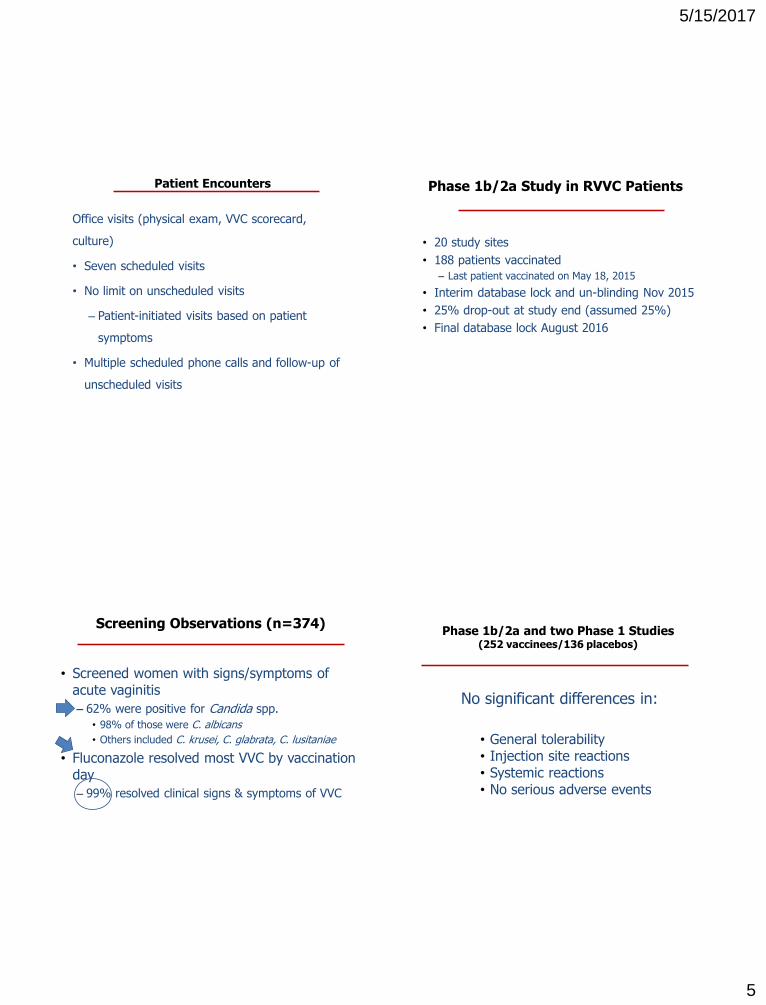
Patient Encounters
Office visits (physical exam, VVC scorecard,
culture)
• Seven scheduled visits
• No limit on unscheduled visits
– Patient-initiated visits based on patient
symptoms
• Multiple scheduled phone calls and follow-up of
unscheduled visits
Phase 1b/2a Study in RVVC Patients
• 20 study sites
• 188 patients vaccinated
– Last patient vaccinated on May 18, 2015
• Interim database lock and un-blinding Nov 2015
• 25% drop-out at study end (assumed 25%)
• Final database lock August 2016
Screening Observations (n=374)
• Screened women with signs/symptoms of acute vaginitis
– 62% were positive for Candida spp.
• 98% of those were C. albicans
• Others included C. krusei, C. glabrata, C. lusitaniae
• Fluconazole resolved most VVC by vaccination day
– 99% resolved clinical signs & symptoms of VVC
No significant differences in:
• General tolerability• Injection site reactions• Systemic reactions• No serious adverse events
Phase 1b/2a and two Phase 1 Studies(252 vaccinees/136 placebos)

5/15/2017
6
NDV-3A Induces Strong B and T Cell Responses in Women with RVVC
Seru
m I
gG
Titer
Seru
m I
gA
Titer
% IF
N-γ
Responses
% IL-1
7A
R
esponders
IFN-γ
IL-17
Study Days Study Days
“Final” Data Analysis Parameters
• ITT population for NDV-3A and placebo = 174
• Per protocol population = 165
• Evaluation of recurrences starts at Study Day 18
– All patients receive fluconazole on Study Days -14, -11, -8, 1, 7 and 14
– Three half-lives for fluconazole = 3.8 days
• Censure day for K-M plot limited to 374 days (per protocol)
– Applies to 12 patients (5 NDV-3A, 7 Placebo) that exited the study later than planned
• Included all women who had not reached their 40th birthday
Protocol violations: specifics (n)Composite score <3 at screening (2) No positive culture at screening (4)Composite score >=3 on Day 0 (2) Other (1)
Recurrence Free Percentages
Kaplan-Meier Curve: time to first recurrence: patients <40 (77% of total)
Recurrences: based on patient symptom scores ≥3
Placebo
NDV-3A/placebo
hazard ratio = 0.59
Difference in curves, p = 0.026
Pro
po
rtio
n w
ho
are
re
cu
rre
nce
-fre
e
Days following single dose of NDV-3A
NDV-3A
Efficacy Data: Patient Symptom ScoresNDV-3A Extends Recurrence-Free State vs Placebo
3 months 12 months
<40 years n=122
All agesn=159
<40 years n=107
All agesn=124
Recurrence(NDV-3A)
27% 32% 58% 62%
Recurrence(Placebo)
47% 44% 78% 75%
Efficacy 43% 28% 26% 17%
Odds Ratio NDV-3A/placebo(95% CI)
0.41(0.19-0.88)
p=0.02
0.58(0.30-1.14)
p=0.11
0.39(0.16-0.92)
p=0.03
0.55(0.26–1.14)
p=0.10
Recurrence defined by patient symptom score ≥3Efficacy = (placebo recurrence rate – NDV-3A recurrence rate)/placebo recurrence rateOdds ratio = relative odds of having first recurrence by 12 months, NDV-3A/placebo
5/15/2017
7
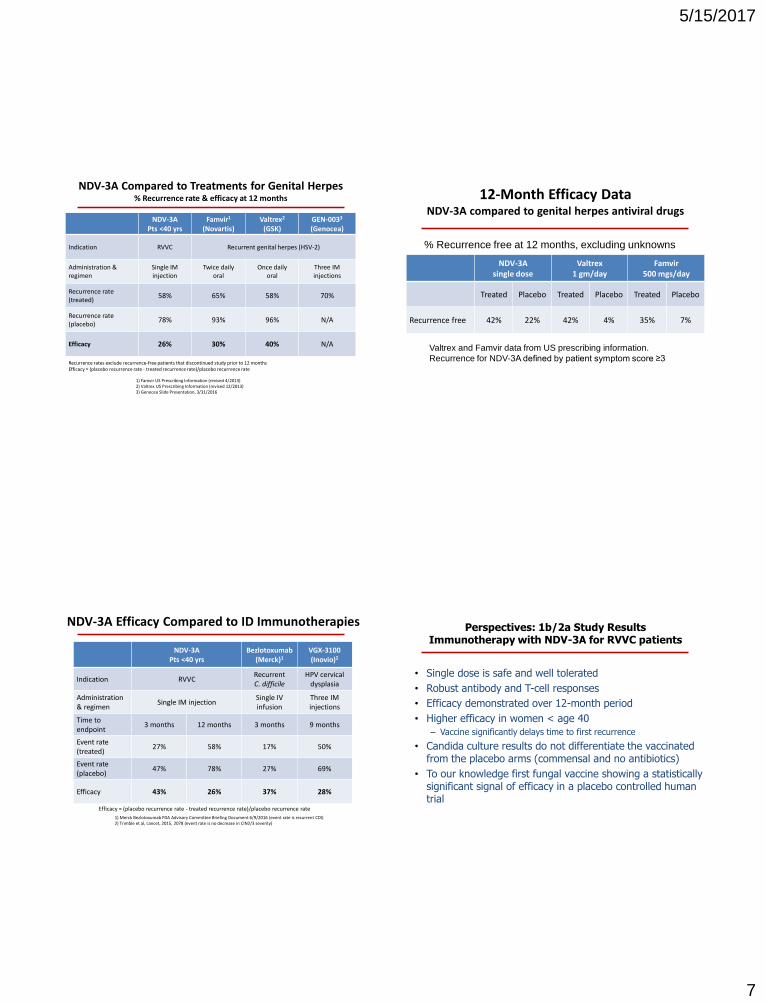
NDV-3APts <40 yrs
Famvir1
(Novartis)Valtrex2
(GSK)GEN-0033
(Genocea)
Indication RVVC Recurrent genital herpes (HSV-2)
Administration & regimen
Single IM injection
Twice daily oral
Once daily oral
Three IM injections
Recurrence rate(treated)
58% 65% 58% 70%
Recurrence rate(placebo)
78% 93% 96% N/A
Efficacy 26% 30% 40% N/A
1) Famvir US Prescribing Information (revised 4/2013)2) Valtrex US Prescribing Information (revised 12/2013) 3) Genocea Slide Presentation, 3/31/2016
NDV-3A Compared to Treatments for Genital Herpes% Recurrence rate & efficacy at 12 months
Recurrence rates exclude recurrence-free patients that discontinued study prior to 12 monthsEfficacy = (placebo recurrence rate - treated recurrence rate)/placebo recurrence rate
12-Month Efficacy DataNDV-3A compared to genital herpes antiviral drugs
NDV-3Asingle dose
Valtrex1 gm/day
Famvir500 mgs/day
Treated Placebo Treated Placebo Treated Placebo
Recurrence free 42% 22% 42% 4% 35% 7%
Valtrex and Famvir data from US prescribing information.
Recurrence for NDV-3A defined by patient symptom score ≥3
% Recurrence free at 12 months, excluding unknowns
NDV-3APts <40 yrs
Bezlotoxumab(Merck)1
VGX-3100(Inovio)2
Indication RVVCRecurrentC. difficile
HPV cervical dysplasia
Administration& regimen
Single IM injectionSingle IV infusion
Three IM injections
Time to endpoint
3 months 12 months 3 months 9 months
Event rate(treated)
27% 58% 17% 50%
Event rate(placebo)
47% 78% 27% 69%
Efficacy 43% 26% 37% 28%
NDV-3A Efficacy Compared to ID Immunotherapies
Efficacy = (placebo recurrence rate - treated recurrence rate)/placebo recurrence rate
1) Merck Bezlotoxumab FDA Advisory Committee Briefing Document 6/9/2016 (event rate is recurrent CDI)2) Trimble et al, Lancet, 2015, 2078 (event rate is no decrease in CIN2/3 severity)
Perspectives: 1b/2a Study ResultsImmunotherapy with NDV-3A for RVVC patients
• Single dose is safe and well tolerated
• Robust antibody and T-cell responses
• Efficacy demonstrated over 12-month period
• Higher efficacy in women < age 40
– Vaccine significantly delays time to first recurrence
• Candida culture results do not differentiate the vaccinated from the placebo arms (commensal and no antibiotics)
• To our knowledge first fungal vaccine showing a statistically significant signal of efficacy in a placebo controlled human trial
5/15/2017
8
• Use multiple doses of NDV-3A rather than single dose
• Refinement and focus on patient self-reported assessments
• Assess additional microbiological methods to explore “hard”
microbiological endpoint. May not be required
– Multiple hyphae-specific genes can be used to assess yeast & hyphae
forms (e.g., PCR, q-PCR, nanostring, gene expression)
• Limit to patients under 40 years of age
• Multiple antigens
Considerations for Future RVVC Studies
• Job’s Patients at NIH Clinical Center (CHI)
• DoD Military Recruits Fort Benning, Sept. 2017
• Collaboration with CDC on C. auris
• Detailed Evaluation of Multiple Antigens (HYR1,
SAP2, ALS3) Alone and Combined
• Healthcare-Associated (Nosocomial) Study (MSG)
Other Plans
“Progress always involves risk.
You can’t steal second base
and keep your foot on first.”
Frederick B. Wilcox
Three Rules for Successful InvestigatorsFrank DeSantis Circa 1990
1. Get the Money
2. Get the Money
3. Get the Money
5/15/2017
9
Acknowledgements
John P. Hennessey, Jr.*Clint S. Schmidt*
Terry CochraneMichael M. Schwartz* Erica MarchusMary Lizakowski
Elizabeth Ann DeMontignyJesse Hoeg
Tim Cooke*
Tuomas Holmberg*Holly JorudFred HaneySavery Nash
Will JosephAl JosephGordon Douglas
Hugh GeorgeJoe GerstnerPatrice DuboisFlorian Schodel
Jo WhiteEric Brass
Study Investigators
Dennis Dixon*
Rory Duncan*
Jim BlairTodd BradyPartners
Michael Augenbraun Khadra Osman
Liesl Bredeson Smith Rovena Reagan
Michael Drusano Allen Silanee
Lance Edwards Jack Sobel
Charles Eubank Valerie Sorkin-Well
Mark Jacobs Steven Sussman
Susan Jeanfreau Andrew Wagner
Helena Kirkpatrick Richard Wyatt
Stephen McCann Edward Zbella
Paul Nyirjesy Keila Hoover
Ashraf S. Ibrahim*Michael R. Yeaman
Scott G. Filler*Yue FuBrad Spellberg