procedural sedation in the pre-hospital setting antoinette eng, md albany medical center december...
TRANSCRIPT

Procedural Sedation in Procedural Sedation in the the
Pre-Hospital SettingPre-Hospital Setting
Antoinette Eng, MDAntoinette Eng, MD
Albany Medical CenterAlbany Medical Center
December 20, 2006December 20, 2006
EMS Procedural Sedation: EMS Procedural Sedation: OverviewOverview
DefinitionDefinition IndicationsIndications MedicationsMedications Recent ResearchRecent Research SummarySummary

SedationSedation
Controlled reduction of environmental Controlled reduction of environmental awarenessawareness

SedationSedation
DynamicDynamic

A Clinical SpectrumA Clinical Spectrum
Anesthesia
Anxiolysis
Moderate Sedation & Analgesia
Deep Sedation & Analgesia

Minimal SedationMinimal Sedation Drug-induced stateDrug-induced state Impaired cognitive function & coordinationImpaired cognitive function & coordination Responds to verbal commandsResponds to verbal commands Ventilatory and cardiovascular functions Ventilatory and cardiovascular functions
intactintact
Anxiolysis

Previously known as “conscious sedation”Previously known as “conscious sedation” Depression of consciousnessDepression of consciousness Respond purposefully to verbal commands Respond purposefully to verbal commands
alone or with light tactile stimulationalone or with light tactile stimulation Ventilation and cardiovascular function Ventilation and cardiovascular function
intactintact
Anxiolysis
Moderate Sedation & Analgesia

Depression of consciousnessDepression of consciousness Not easily aroused, but responds purposefully Not easily aroused, but responds purposefully
after repeated or painful stimulationafter repeated or painful stimulation May require airway and ventilatory supportMay require airway and ventilatory support Cardiovascular function maintainedCardiovascular function maintained
Anxiolysis
Moderate Sedation & Analgesia
Deep Sedation & Analgesia

Loss of consciousnessLoss of consciousness Patient cannot be aroused by painful Patient cannot be aroused by painful
stimulistimuli Requires airway and ventilatory supportRequires airway and ventilatory support Cardiovascular function may be impairedCardiovascular function may be impaired
Anesthesia
Anxiolysis
Moderate Sedation & Analgesia
Deep Sedation & Analgesia

IndicationsIndications
ProceduresProceduresCardioversionCardioversionTranscutaneous Transcutaneous PacingPacingPre/Post-IntubationPre/Post-IntubationTransportTransportExtricationExtrication
Primary TreatmentPrimary TreatmentAnxietyAnxietySympathomimetic OverdoseSympathomimetic OverdoseAlcohol WithdrawalAlcohol Withdrawal
Pain Management AdjunctPain Management AdjunctTraumaTrauma
Acute AbdomenAcute Abdomen
ACSACS
Patient RestraintPatient Restraint

IndicationsIndications
ProceduresProceduresCardioversionCardioversionTranscutaneous Transcutaneous PacingPacingPre/Post-IntubationPre/Post-IntubationTransportTransportExtricationExtrication
Primary TreatmentPrimary TreatmentAnxietyAnxietySympathomimetic OverdoseSympathomimetic OverdoseAlcohol WithdrawalAlcohol Withdrawal
Pain Management AdjunctPain Management AdjunctTraumaTrauma
Acute AbdomenAcute Abdomen
ACSACS
Patient RestraintPatient Restraint


Procedural Sedation: Procedural Sedation: MedicationsMedications
BenzodiazepinesBenzodiazepines EtomidateEtomidate OpiatesOpiates Nitrous OxideNitrous Oxide
BenzodiazepinesBenzodiazepines

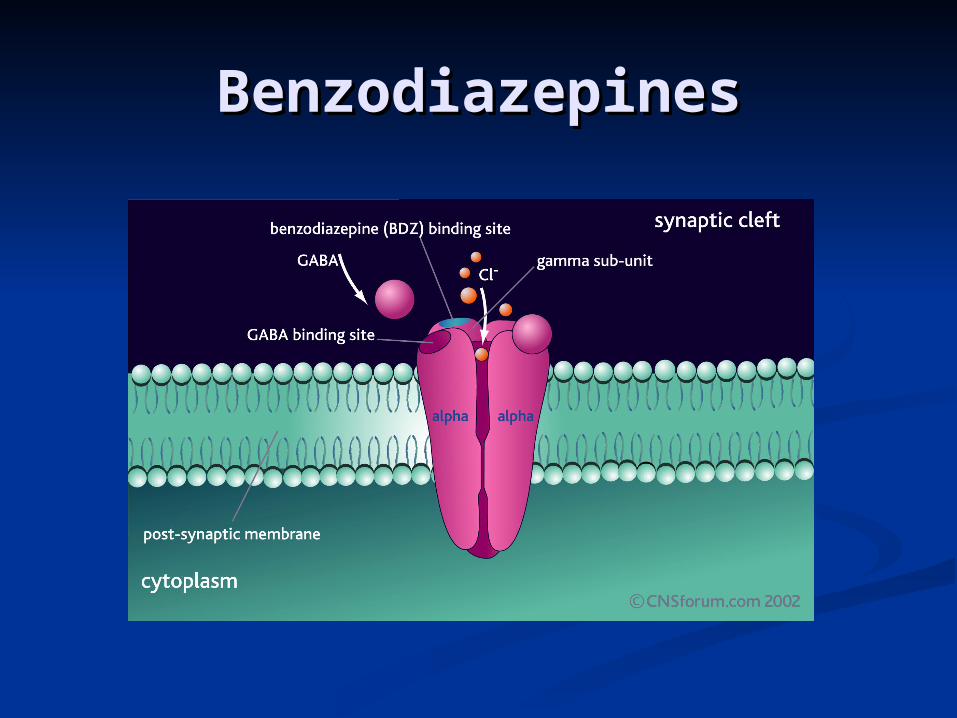
BenzodiazepinesBenzodiazepines GABA is major inhibitory neurotransmitter in CNSGABA is major inhibitory neurotransmitter in CNS 3 types of receptors: GABA-A, GABA-B, GABA-C3 types of receptors: GABA-A, GABA-B, GABA-C GABA-A overwhelmingly numerically dominant receptor GABA-A overwhelmingly numerically dominant receptor
in CNSin CNS BZO bind and allosterically modify receptorBZO bind and allosterically modify receptor Potentiate GABA responsePotentiate GABA response Increase hyperpolarizationIncrease hyperpolarization Increase neuronal inhibition at all levels of the neuraxis, Increase neuronal inhibition at all levels of the neuraxis,
including the spinal cord, hypothalamus, hippocampus, including the spinal cord, hypothalamus, hippocampus, substantia nigra, cerebellar cortex, and cerebral cortex substantia nigra, cerebellar cortex, and cerebral cortex
Sedation, amnesia, muscle relaxation, anesthesia, anti-Sedation, amnesia, muscle relaxation, anesthesia, anti-convulsant, anxiolyticconvulsant, anxiolytic

MidazolamMidazolam lipid soluble in bloodlipid soluble in blood Rapid GI absorption, Rapid GI absorption, Lipid solubility = prompt passage across blood-Lipid solubility = prompt passage across blood-
brain barrier, rapid redistribution and short brain barrier, rapid redistribution and short duration of actionduration of action
Large first-pass hepatic effectLarge first-pass hepatic effect Metabolism slowed in patients on cimetidine, Metabolism slowed in patients on cimetidine,
erythromycin, calcium channel blockers, erythromycin, calcium channel blockers, antifungal medications, fentanyl since they also antifungal medications, fentanyl since they also use P450 cytochrome systemuse P450 cytochrome system
1.0-2.5 mg IV1.0-2.5 mg IV Onset 30-60 secondsOnset 30-60 seconds Time to Peak Effect 3-5 minutesTime to Peak Effect 3-5 minutes Duration of Sedation 15-80 minutesDuration of Sedation 15-80 minutes

MidazolamMidazolam
Indications:Indications: Sedation prior to cardioversion and Sedation prior to cardioversion and
intubationintubation Maintenance of sedation in Maintenance of sedation in
mechanically ventilated patientsmechanically ventilated patients Pediatric seizure controlPediatric seizure control

MidazolamMidazolam
AdultsAdults Intubation adjunctIntubation adjunct: :
0.5-5mg IV/IM0.5-5mg IV/IM may repeat every 5-10 minutesmay repeat every 5-10 minutes max 10 mgmax 10 mg
Status, cardioversion, pacing, inner Status, cardioversion, pacing, inner ear problems, sedation, muscular ear problems, sedation, muscular spasmsspasms:: 0.5-2.5 mg IV, 5mg IM0.5-2.5 mg IV, 5mg IM may repeat every 5-10 mins may repeat every 5-10 mins max 5mgmax 5mg

MidazolamMidazolam
PediatricPediatric IntubationIntubation: :
0.1-0.2 mg/kg 0.1-0.2 mg/kg max 5 mg/dose, repeat PRN for sedation to max of 10 mgmax 5 mg/dose, repeat PRN for sedation to max of 10 mg
SeizuresSeizures: : 0.2-0.4 mg/kg IN/PR 0.2-0.4 mg/kg IN/PR IV/IM 0.05-0.2 mg/kgIV/IM 0.05-0.2 mg/kg repeat every 5 mins PRNrepeat every 5 mins PRN
Sedation for painful procedures, Sedation for painful procedures, cardioversion, pacing, muscular spasms, cardioversion, pacing, muscular spasms, hyperdynamic drug ingestion/exposurehyperdynamic drug ingestion/exposure:: 0.05-0.1 mg/kg IV/IM/IO 0.05-0.1 mg/kg IV/IM/IO every 5-10 min (2-5 mins if IV) max 2.5 mgevery 5-10 min (2-5 mins if IV) max 2.5 mg

Midazolam Side EffectsMidazolam Side Effects
Ventilatory Depression caused by Ventilatory Depression caused by decrease in hypoxic drivedecrease in hypoxic drive
Effects greater than for Lorazepam Effects greater than for Lorazepam and Diazepamand Diazepam
Exaggerated in presence of other Exaggerated in presence of other opioids and CNS depressants, COPD, opioids and CNS depressants, COPD, increasing ageincreasing age
DiazepamDiazepam Indications:Indications:
Seizures/status epilepticusSeizures/status epilepticus Sedation pre-cardioversionSedation pre-cardioversion Acute anxietyAcute anxiety Skeletal muscle relaxantSkeletal muscle relaxant Alcohol withdrawalAlcohol withdrawal VertigoVertigo

DiazepamDiazepam
SeizuresSeizures: : 2-10 mg slow IV2-10 mg slow IV 5-10 mg PR5-10 mg PR max 20 mgmax 20 mg
Sedation/cardioversion/pacing/Sedation/cardioversion/pacing/muscle muscle spasm/labyrinthitis/vertigospasm/labyrinthitis/vertigo: : 2-5 mg slow IV every 5-10 mins2-5 mg slow IV every 5-10 mins max 10mgmax 10mg
Midazolam vs DiazepamMidazolam vs Diazepam
More rapid onsetMore rapid onset Greater amnesiaGreater amnesia 2 to 3 times as potent2 to 3 times as potent Twice the affinity for benzodiazepine Twice the affinity for benzodiazepine
receptorreceptor Greater decrease in blood pressure and heart Greater decrease in blood pressure and heart
raterate Systemic vascular resistanceSystemic vascular resistance Less post-procedural sedationLess post-procedural sedation Same time to complete recoverySame time to complete recovery

BenzodiazepinesBenzodiazepines
OnsetOnset DuratioDurationn
DiazepaDiazepamm
IV 5 minIV 5 min
IM 15-IM 15-30m30m
15-60 m15-60 m
MidazolaMidazolamm
IV 1-3 IV 1-3 minmin
IM 5-15 IM 5-15 minmin
15-90 m15-90 m

BenzodiazepinesBenzodiazepinesSide Side EffectsEffects
MinorMinor MajorMajor
DiazepamDiazepam CNS CNS DepressionDepression
Resp DepressionResp Depression
ApneaApnea
HypotensionHypotension
Cardiac ArrestCardiac Arrest
““Valium rage”Valium rage”
MidazolaMidazolamm
CNS CNS DepressionDepression
CoughCough
HiccupsHiccups
see Diazepamsee Diazepam
Phlebitis @ IM Phlebitis @ IM sitesite
Etomidate: PropertiesEtomidate: Properties AnestheticAnesthetic Non-narcotic sedative hypnoticNon-narcotic sedative hypnotic Increases GABA receptors, enhancing Increases GABA receptors, enhancing
inhibitory neurotransmissioninhibitory neurotransmission Reticular activating system depressionReticular activating system depression Short actingShort acting Induces sedation & amnesiaInduces sedation & amnesia No histamine releaseNo histamine release Minimal cardiac & respiratory depressive Minimal cardiac & respiratory depressive
effectseffects

Etomidate: Adverse Etomidate: Adverse EffectsEffects
? Decreased ICP? Decreased ICP Nausea and vomitingNausea and vomiting MyoclonusMyoclonus Adrenocortical SuppressionAdrenocortical Suppression

EtomidateEtomidate
Indications:Indications:
Induction agent for intubationInduction agent for intubation
Pre-medication for cardioversionPre-medication for cardioversion

EtomidateEtomidate Adults & PediatricsAdults & Pediatrics
IntubationIntubation: 0.3 mg/kg slow IV over 30-: 0.3 mg/kg slow IV over 30-60 seconds, repeat as needed, 60 seconds, repeat as needed, maximum 0.6mg/kgmaximum 0.6mg/kg
Short painful proceduresShort painful procedures: 0.15 mg/kg : 0.15 mg/kg slow IV over 30-60 secondsslow IV over 30-60 seconds

Etomidate vs Midazolam for Etomidate vs Midazolam for Out-of-Hospital Intubation: Out-of-Hospital Intubation: A Prospective, Randomized A Prospective, Randomized
TrialTrialAnn Emerg Med. 47(6):525-30, 2006 JunAnn Emerg Med. 47(6):525-30, 2006 Jun Prospective, double blind, randomizedProspective, double blind, randomized 55 Versed, 55 Etomidate55 Versed, 55 Etomidate 75% success rate versed, 76% etomidate75% success rate versed, 76% etomidate No difference in success rates, incidence No difference in success rates, incidence
of hypotension, number of attempts, of hypotension, number of attempts, perceived difficultyperceived difficulty

OpiatesOpiates

MorphineMorphine
Central nervous system depressantCentral nervous system depressant Acts at mu receptors above and at Acts at mu receptors above and at
spinal cordspinal cord Decrease cardiac preload/afterloadDecrease cardiac preload/afterload Decreases myocardial oxygen Decreases myocardial oxygen
demanddemand Releases histamine Releases histamine can cause can cause
hypotensionhypotension

MorphineMorphine
Dose:Dose: 0.05-0.1 mg/kg IV0.05-0.1 mg/kg IV Peak:Peak: 10-30 minutes10-30 minutes Duration:Duration: 2-4 hours2-4 hours

MorphineMorphine
Adverse Reactions & Side EffectsAdverse Reactions & Side Effects CNS: Euphoria, sedation, respiratory CNS: Euphoria, sedation, respiratory
depressiondepression Cardiovascular: bradycardia, Cardiovascular: bradycardia,
hypotensionhypotension GI: decreased motility, nausea, vomitingGI: decreased motility, nausea, vomiting GU: urinary retentionGU: urinary retention Respiratory: bronchoconstriction, Respiratory: bronchoconstriction,
antitussiveantitussive

FentanylFentanyl
Synthetic opioid derivativeSynthetic opioid derivative 100x potency of morphine100x potency of morphine Highly lipid solubleHighly lipid soluble Stored in adipose tissue to create a Stored in adipose tissue to create a
“reservoir”“reservoir” Low complication rateLow complication rate Doesn’t release histamine, rarely Doesn’t release histamine, rarely
produces hypotensionproduces hypotension

FentanylFentanyl
Dose:Dose: 1 mcg/kg IV1 mcg/kg IV Onset:Onset: FastFast Peak:Peak: 2.5-10 minutes2.5-10 minutes Duration:Duration: 30-90 minutes30-90 minutes

FentanylFentanyl
Respiratory depression with alcohol Respiratory depression with alcohol or versedor versed
Chest wall rigidityChest wall rigidity dose dependentdose dependent not reliably antagonized by naloxonenot reliably antagonized by naloxone

Nitrous Nitrous OxideOxide

Nitrous OxideNitrous Oxide
Colorless gasColorless gas Mixed with 50% oxygen and inhaledMixed with 50% oxygen and inhaled Self-administered by patientSelf-administered by patient Mild intoxicant, potent analgesicMild intoxicant, potent analgesic Disspiates within 2-5 minutes after Disspiates within 2-5 minutes after
stoppingstopping

Nitrous OxideNitrous Oxide
Adverse ReactionsAdverse Reactions Light-headedLight-headed ConfusionConfusion DrowsinessDrowsiness Nausea/vomitingNausea/vomiting

Nitrous OxideNitrous Oxide Contraindicated:Contraindicated: Altered state of consciousnessAltered state of consciousness
Head injury, alcohol ingestion, drug ODHead injury, alcohol ingestion, drug OD COPDCOPD PneumothoraxPneumothorax Decompression sicknessDecompression sickness Air embolusAir embolus Abdominal pain with distensionAbdominal pain with distension Pregnancy, except during deliveryPregnancy, except during delivery Unable to self-administerUnable to self-administer

Nitrous OxideNitrous Oxide
ConsiderationsConsiderations Currently not on REMO protocol, but a Currently not on REMO protocol, but a
good drug to know aboutgood drug to know about Heavier than air, can accumulate at Heavier than air, can accumulate at
ambulance floor and affect EMS ambulance floor and affect EMS personnelpersonnel

Patient RestraintPatient Restraint
No standing ordersNo standing orders
Available through Medical Control:Available through Medical Control: Age < 70: Haloperidol 5mg mixed with Age < 70: Haloperidol 5mg mixed with
Midazolam 2mg IMMidazolam 2mg IM Age > 70: Haloperidol 5mg IMAge > 70: Haloperidol 5mg IM RepeatRepeat

Patient RestraintPatient Restraint
In 1998 California survey of 490 EMS In 1998 California survey of 490 EMS providers:providers:
61% recounted assault on the job61% recounted assault on the job 25% reported injury25% reported injury 37% of injured required medical attention37% of injured required medical attention 95% recounted restraining patient 95% recounted restraining patient
““Exposure of prehospital care providers to Exposure of prehospital care providers to violence.”violence.”Prehospital Emergency Care. 2(2):127-31, Prehospital Emergency Care. 2(2):127-31, 1998 Apr-Jun.1998 Apr-Jun.

Dangers to PatientsDangers to Patients ““Positional Asphyxia During Law Enforcement Positional Asphyxia During Law Enforcement
Transport.” Transport.” Am Jrnl of Forensic Med and Path. Reay DR. 13(2):90-7, 1992.Am Jrnl of Forensic Med and Path. Reay DR. 13(2):90-7, 1992.
““Met Acidosis in Restraint-Associated Cardiac Arrest: A Met Acidosis in Restraint-Associated Cardiac Arrest: A Case Series.” Case Series.” Acad Emerg Med. Hick, et al. 6(3):239-44, 1999.Acad Emerg Med. Hick, et al. 6(3):239-44, 1999.
““Sudden Death in Individuals in Hobble Restraints Sudden Death in Individuals in Hobble Restraints During Paramedic Transport.” During Paramedic Transport.” Ann of Emerg Med. Stratton SJ, et al. 25(5):710-12, May 1995.Ann of Emerg Med. Stratton SJ, et al. 25(5):710-12, May 1995.

Patient RestraintPatient Restraint
Indications:Indications: Patients at risk of causing physical Patients at risk of causing physical
harm to emergency responders, the harm to emergency responders, the public, and/or themselvespublic, and/or themselves
Considerations:Considerations: Cannot be transported face downCannot be transported face down If in police custody with handcuffs on, If in police custody with handcuffs on,
must beaccompanied by police officer in must beaccompanied by police officer in ambulance to hospitalambulance to hospital
EMS may only apply “soft restraints”EMS may only apply “soft restraints”

HaldolHaldol
Dopamine blockade in mesocortex and limbic Dopamine blockade in mesocortex and limbic system inhibits psychosessystem inhibits psychoses
Extrapyramidal effects (akathisia, dystonia, Extrapyramidal effects (akathisia, dystonia, pseudoparkinsonism) due to dopamine pseudoparkinsonism) due to dopamine blockade in niagrostriatal pathwaysblockade in niagrostriatal pathways
Sedative for psychomotor agitationSedative for psychomotor agitation Minor anticholinergic and antihistaminic Minor anticholinergic and antihistaminic
actionsactions rarely cardiovascular, anticholinergic rarely cardiovascular, anticholinergic effectseffects
May cause QT prolongation, lower seizure May cause QT prolongation, lower seizure thresholdsthresholds
HaldolHaldol Indications:Indications:
Acute and chronic psychosesAcute and chronic psychoses Agitation, aggressionAgitation, aggression
Contraindications:Contraindications: Parkinson’sParkinson’s SeizureSeizure Cocaine overdoseCocaine overdose AlcoholismAlcoholism Severe mental/CNS depressionSevere mental/CNS depression thyrotoxicosisthyrotoxicosis

HaldolHaldol
Dosage 5-10mg IMDosage 5-10mg IM

SummarySummary
Sedation is a dynamic spectrumSedation is a dynamic spectrum
Main EMS uses: Main EMS uses: Procedures Procedures RestraintRestraint Primary TreatmentPrimary Treatment Pain management adjunctPain management adjunct

Thank you for your attention!Thank you for your attention!