prime contractor model - king's fund · prime contractor model ... •msk conditions = most...
TRANSCRIPT
Prime Contractor ModelKing’s FundNick Boyle Consultant Surgeon27 March 2014

MSK Referral
Horizon
Musculoskeletal Triage &
Treatment
Treatment or Procedures,
1 New to 4 FU
Chronic PainTreatment or Procedures,
1 New to 4 FU
Injections
Secondary Care:
++ Direct Access Physiotherapy
BHT PhysioPhysio
1 New to 4 FUInjections
L&D PhysioPhysio
1 New to 4 FU
SEPT MSK Podiatry contacts
1 new to 4 FU Podiatric Surgery
Community Physiotherapy
1 New to 4 Follow Ups
-
No Triage
Sec. Care OP 1st:
T&O
Rheum
Plastics
576 Pain
Secondary Care FU
T&O
Rheum
Plastics
1,324 Pain
OP Procedures
Daycases
ElectivesNon
Attendances/Cancelled Referrals
Repeat referrals
1.Horizon Health Choices
2.Direct Access Physiotherapy
3.Direct Access to Consultant Out Patient Clinics
Current Referral Route options -Information

MSK Challenges
• There are over 200 musculoskeletal conditions affecting millions of people
• MSK conditions contribute to long-term disability
• The ageing population/technology increases demand
• MSK conditions = most common reason for repeat consultations with a GP (30%)
Source: The Musculoskeletal Framework: A joint responsibility, doing it differently, DH (2006)

MSK Challenges
• Up to 60% of people on long-term incapacity benefit
8–10 million people in the UK have arthritis
• 40% of people over 70 have osteoarthritis of the knee
• Low back pain is reported by about 80% of people at
sometime in their life
• By 2020, trauma caused by road traffic injury will become
the third highest ranked cause of disabling conditions.
Source: The Musculoskeletal Framework: A joint responsibility, doing it differently, DH (2006) -World Health Organization (WHO) and European Bone and Joint Health Strategies Project11

Problems
• Patient’s/GP’s perspective
• Un-coordinated
• Fragmented
• Inconsistent
• Variable quality
• Variable communication
• No central point of contact

Problems
• System view
• Variation in quality/clinical interventions
• Adherence to best practice inconsistent
• Hospital centric model
• Introduction of innovation such as self care/shared decision making slow
• High access times

Bedfordshire Hospital Waiting TimesDecember 2013
• 18 weeks Referral to Treatment (RTT) pathways (Target 90%)
• Trauma & Orthopaedics 80.5%
• The non-admitted pathway (Target 95%) with the exception of 2 specialties:
• Trauma & Orthopaedics 94.1%
• The incomplete pathway (Target 92%)• Trauma & Orthopaedics 87.8%
From Bedfordshire CCG March 2014 Governing Body Integrated Quality, Safety & Performance Report

Bedford Hospital NHS Trust Performance
Elective care:
• Failure to meet 18 week RTT consistently (for 18 months) with resulting subcontracting of private sector providers: 1 in 4 patients waits longer than 18 weeks for inpatient procedure
• Below average numbers of procedures being undertaken in some categories (e.g. hip and knee revisions)
• Low/no wound infection rates (in the 3 months audited)
• Average PROMs completion and outcomes data

NHS Annual MSK Spend is £6bn

What are the Problems?
System of Care
• Micro-commissioning complex care pathways
• Perverse incentives – PbR
• KPIs process drives neither population level improvement or patient experience
• No effective performance management of care
• Separation from clinical accountability from financial responsibility
• Lack of true clinical leadership

The current administrative micro-management approach to cost containment
11
Primary Care Assessment and
Treatment
Hospital Investigation and
Treatment
Referral Management
Prior Approval
New / FU ratios
Treatment Thresholds
LoS penalties
• Fragmented treatment for patients• Only deals with referred patients• Silo-driven hospital care
“Reduce activity” “Increase activity”

It all starts with the CredoThe beliefs that our partnership is founded on
Our Purpose
To build a great company dedicated to our patients.
Our Parameters
We focus our efforts exclusively on• What we are passionate about• What we can become best at• What drives our economic sustainability
Our Principles
• We are above all the agents of our patients. • We empower our people to do their best. • We are unrelenting in the pursuit of excellence.

Reducing per capita cost whilst maintaining quality
Re-design MSK Impact

Reducing per capita cost whilst maintaining quality
Re-design MSK Impact

The Circle Vision for MSK Services across BedfordshireIntegrating Services by:
• Managing the whole pathway for MSK patients
• Ensuring joined up care
• Improving access by moving services to the community
• Encompassing all MSK services (ex-Trauma)
• Ensuring Clinicians work in a truly integrated way
• Ensure consistent application of best practice clinical pathways
• Engaging patients in service development
• Empowering patients and facilitating self management

Bedford Prime Vendor model
Circle as Prime Contractor:
• Integrate all MSK providers into a programme of care
• System wide accountability for financial control and high quality delivery by managing the MSK supply chain

Primary care holistic assessment and care
COMMUNITY MULTIDISCIPLINARY SPECIALIST SERVICE
(Pathway Hub)
Prime contractor
Highly specialised, intensive, episodic
hospital care
Hub functions:• Referral triage• Skilling up 1’ care• Specialist Assessment• Specialist integrated care• Share Decision Making• Personal Health Planning• Supported Self Care• Patient & carer support• Voluntary sector
provision
PATHWAY MANAGEMENT
Referral triage
Referral
Subcontracting

Operational Model
Key aspects of the model include:
• Bedfordshire MSK model developed with Pennine MSK, based on their best practice model implemented in Oldham
• Clinical triage of all MSK referrals to ensure patients are placed on the right pathway first time
• Iterative development of services through clinical engagement
• Developing patients as partners e.g. patient participation group, shared decision making
• Supporting the CCG in driving up the quality of MSK care in General Practice e.g. training events on MSK conditions
• Shifting care from secondary care into community or primary care. Working with the commissioner to reduce contracted activity within secondary care
• Development of the community workforce to support the integrated care model, including development of Consultant Orthopaedic direct listing clinics

Operational Model
Key benefits:
• Application of best practice care pathways
• Reduction in secondary care referrals (c. 85% of cost base)
• Reduction in unnecessary diagnostics/interventions
• Improved patient experience and patient outcomes throughoptimum care pathways
• Overall system wide efficiency savings through consolidation offragmented service e.g. reduction in repeat treatments/OPAppts/investigations etc
• Improved secondary care efficiency = reduction in cost pertreatment

Beds MSK Services: Benefits To Providers
• Reduction of high volume – low income activity, allowing adoption of low volume high income activity.
• Increased OP capacity for repatriation of out of area work or alternative projects
• Increase in surgically ready patients worked up in primary care
• Improved margin performance through reduction of non value adding processes
• Increase in 18 week achievement rates for MSK
• Shared 18 week responsibility
• Reduction in Waiting List initiative cost risk
• Improved Financial rewards across the supply chain

Contract Structure
Circle as Prime Contractor• Integrate existing and other providers into a programme of care for the Bedfordshire MSK patient population• To take on the accountability for both financial control and the delivery of a high quality system of care by
managing the MSK supply chain
Strategic Partnership• Advised by long-term strategic partners Pennine MSK, National Rheumatoid Arthritis Society and Arthritis Care.
Pennine MSK has developed an integrated MSK service in Oldham over the last 8 years
Sub-Contracts• Circle to hold sub-contracts with secondary Care Providers and Horizon, which is a consortium of GP’s (representing
c. 50% of clinics in the region) currently delivering a proportion of MSK services in the market• Horizon will have responsibility for the provision of Community Care, and will hold sub-contracts with all other
Community Care Providers
Prime Contractor
Sub Contract Holders
Sub Contract Providers
Programme Budget
Horizon – Integrated Provider Hub
Secondary Care
Providers
Therapies
Podiatry
MSK Clinics
Direct Listing
Other Services
BCCG1
Circle
1. Bedfordshire Commissioning Group (BCCG)

MSK Referral
(done by GP)SPoA (Horizon)
Community PhysioDiagnostics
n < 20%
MuSTT
Bio Mechanical Assessment
Direct Listing
Day Case
Direct Listing
Electives
Procedures
Inflammatory Follow Ups
Chronic Pain Injection Follow Ups
SEPT MSK Podiatry Linked or Separate?
Podiatric Surgery
BHT Physio
L&D Physio
(Incremental End Point)Triage & Redirection
New Service Model - Integration

CURRENT KNEE PATHWAY BEDFORD
DISCHARGE / AFTERCARE
COMMUNITY / SECONDARY
PRIMARY CARE
GP referral
Bedford Hospital Triage Unit/
Diagnostics referral initiated
Direct to Community Services for Physio
Direct to Consultants
Direct to HospitalOrthopaedic Dept
Discharge no post operative care
Patient attends GP for post operative
care
Discharge with full discharge package
TREATMENT & DIAGNOSTIC PHASE
Patients enter Diagnostics and Knee
Surgery wait list
Patients referred for Physio go Bedford Physio Hospital
triage enter wait list to see a community
provider

INTEGRATED PROVIDER HUB
TREATMENT PHASEIPHPRIMARY CARE
GP referral
Triage
Knee Surgery with Hospital Provider
Informed Choice is offered to the Patient
Multidisciplinary Team “Shared Decision Making”
and Assessment
COMMUNITY/DISCHARGE
Post Operative Care plan with Community Physio
GP referral with Diagnostics
Pre Operative assessments and
Diagnostics if required
See and Treat Appointments & Minor
Surgical Procedures
Physio with Community
Provider
Self Management

1. Diagnostics - £ 180 (average cost per patient )Patients have the right diagnostics first time due to shared decision makingand the multidisciplinary team approach. Up to 25% of patients have inappropriate diagnostics!
2. Pre Operative Tests - £ 121 ( Cost per patient )The IPH employs nurse prescribers to complete these tests15,000 patient contacts
3. Post Operative Physio - £ 119 First and 3 x £ 70 Follow upsCommunity Physio Providers provide this at £ 103 for 1 and 4 sessions 15,000 patients
4. 90% Conversion rate target vs the current average conversion of 30 %Consultant appointment charges dramatically reduced due to only seeingThe most clinically appropriate patients that have been “ worked up “. This Also improves hospital efficiency.
Examples of Projected Financial Savings

Examples of Projected Financial Savings
• Activity growth managed in line with demographic growth of 1.9%
• Receive 100% of CQUINs – 2.5% of contract value, all of which is passed through to providers
• Moderate level of pathway redesign achieved, including:
a) Price – Sub-tariff prices with Secondary Care providers due to efficiency gains
b) Cost – Phased movement of Secondary Care outpatient appointments into Community at reduced local tariff. All activity moved into Community setting by Year 4
c) Cost – Movement of Bedford Hospital Trust Direct Access Physiotherapy into Community setting at reduced local tariff from Year 1
d) Volume – Stepped reduction in Orthopaedic First to Follow-up ratios, to 1.25 in Year 3 (from 1.93)

Overview of proposed programme budget Total programme budget of £169 across 5 years
27
• Annual programme budget in year 1 of £34.2m. The annual programme budget will be reduced over the course of the contract in line with savings.
• Total savings of £17m to be delivered across 5 years.• The programme budget includes £24m savings in surgical costs across 5 years. A quarter of these savings will be offset by an
increase in non-surgical costs as patients are treated in a different setting through pathway redesign.• Average underlying assumptions
• Demographic growth: 1.43%¹• Underlying growth: 1.90%²• Tariff deflator: (1.90%)³
¹ See Appendix for details
£32
£33
£34
£35
£36
£37
£38
£39
2013/2014 2014/2015 2015/2016 2016/2017 2017/2018 2018/2019
An
nu
al M
SK e
xpe
nd
itu
re (£
'm)
Projected CCG Baseline Expenditure Budget Proposal
£4.1m£3.4m£2.6m£1.9m £4.9m
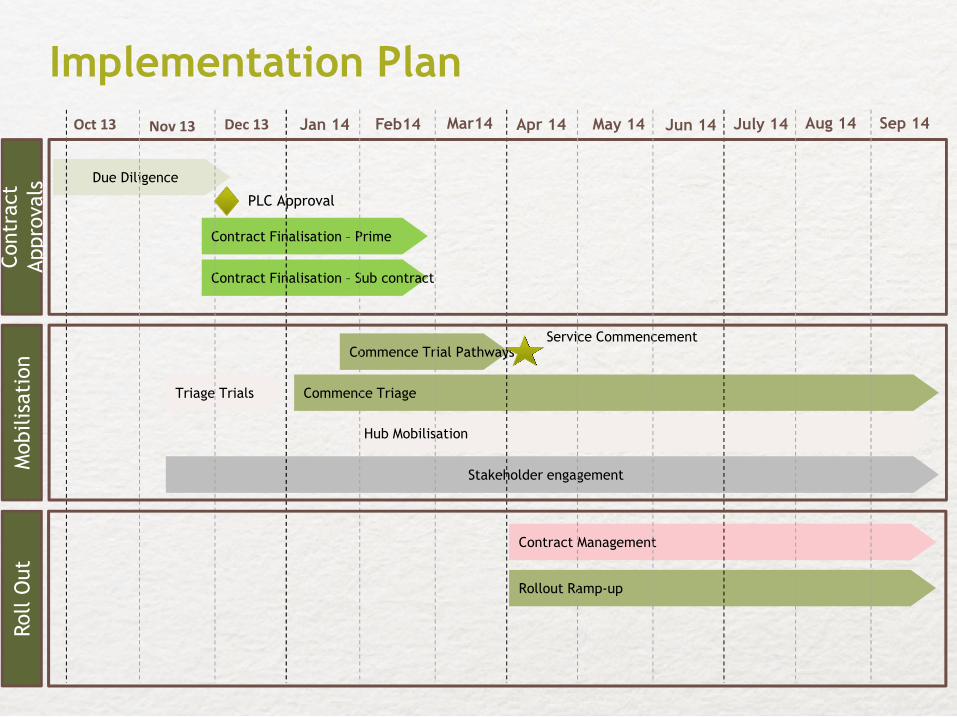
Contract Finalisation – Sub contract
Implementation PlanOct 13
Due Diligence
Jan 14
Stakeholder engagement
Apr 14
Contract Finalisation – Prime
Commence Trial Pathways
Commence Triage
Hub Mobilisation
Rollout Ramp-up
Triage Trials
Contract Management
Service Commencement
July 14
Contr
act
Appro
vals
Mobilis
ati
on
Roll O
ut
Nov 13 Dec 13
PLC Approval
Feb14 Mar14 May 14 Jun 14 Aug 14 Sep 14

Lessons Learnt/Key Success Criteria
• Early agreement of programme budget (PB)
• Assessment of PB requires clinical and assessment expertise
• Marginal analysis not universally available
• Availability and quality of data
• Cultural transformation and innovation take time
• Ability to engage with local organisation and especially with clinicians at early stage
• Contracting process is complex and requires time
• Commissioners require commitment. Good working relationship with Prime Contractor
is key
• Best practice pathway application is central to success
• Key enablers are independent clinical engagement, contracting and integrating IT
platform

Thank you