primary health care
DESCRIPTION
PRIMARY HEALTH CARE. HEALTH SYSTEM BASED ON PHC A Bogotá without Indifference. PRIMARY HEALTH CARE. COLOMBIA BOGOTA, District Secretariat of Health TRANSECTORALITY AND HEALTH DETERMINANTS. POPULATION. BOGOTA. - PowerPoint PPT PresentationTRANSCRIPT

PRIMARY HEALTH CARE PRIMARY HEALTH CARE
HEALTH SYSTEMBASED ON PHC
A Bogotá without Indifference

PRIMARY HEALTH CARE PRIMARY HEALTH CARE
COLOMBIABOGOTA, District Secretariat of
Health
TRANSECTORALITY AND HEALTH
DETERMINANTS

AreaUrban
AreaRural
BOGOTACOLOMBIA
2005: 42,090,502 inhabitants * 2005: 6,778,291 inhabitants *
POPULATIONPOPULATION
* Source DANE, 2005

TABLE OF CONTENTS TABLE OF CONTENTS
1. POLITICAL FRAMEWORK
2. MANAGING PRIMARY HEALTH CARE - Territory and Population
3. PHC AND FIRST LEVEL HOSPITALS4. PHC AND TRANSECTORALITY
– EDUCATION – HOUSING

1.POLICY FRAMEWORK

FOR-PROFIT INSURANCE SYSTEM
UNIVERSAL RIGHT TO HEALTH
FROM HEALTH TO QUALITY OF LIFE

THANKS

Sub
scrib
ers
to S
ubsi
dize
d R
egim
e
IPS
per
UP
Z

Transfer of population from the Paraíso Community from a contributivesystem to the primary care IPS
Transfer of population from the Paraíso Community from a subsidizedsystem to the primary care IPS

UNIVERSAL INSURANCE UNIVERSAL INSURANCE
INDIVIDUAL CONTRACTS ASSOCIATED WITH PAYMENT OF CLAIMS
ACCESS BARRIERS•Databases•Location of the first level of care•Limits of the Health Plan
COST CONTROL•Put off providing services to high-demand or high-cost populations •Forms of hiring and paying health providers, capitation and reports•Methods of payment and hiring health professionals

UNIVERSAL INSURANCE UNIVERSAL INSURANCE
INSURANCE IS NOT SYNONYMOUS WITH HEALTH SERVICES.
PERINATAL AND PERIOD MORTALITY RATES

HEALTH POLICY HEALTH POLICY “BOGOTÁ WITHOUT INDIFFERENCE”“BOGOTÁ WITHOUT INDIFFERENCE”
“Creating conditions for the effective, steady, and sustainable exercise of the human rights enshrined in the constitutional pact and international agreements and instruments.”

RIGHT TO HEALTH: RIGHT TO HEALTH:
““QUALITY OF LIFE AND HEALTH PROMOTIONAL QUALITY OF LIFE AND HEALTH PROMOTIONAL STRATEGY”STRATEGY”
• Population in territories• Eliminating social inequities• Quality of life, a transectoral matter• Needs-based services • Comprehensive social management• Participatory processes. Social mobilization for the
right to health

2. MANAGING PRIMARY HEALTH
CARE
Territory and Population

Integrating services with population-based perspective (life cycle and vulnerability)
Ways of organizing sectoral responses and bridging them with those of other sectors
Coordinating individual and joint actions in areas of everyday life (home, neighborhood, school, work)
PHC IN BOGOTÁPHC IN BOGOTÁ

PRIMARYPRIMARY CARE FLOW CHART CARE FLOW CHART
ENTRY POINTSENTRY POINTS
AREAS HEALTH SERVICES
ESE I-II-III Private IPS
COMPREHENSIVE SOCIAL MANAGEMENT - SOCIAL PARTICIPATIONCOMPREHENSIVE SOCIAL MANAGEMENT - SOCIAL PARTICIPATION
HEALTH IN YOUR HOME
The FamilySchools: Health in SchoolsKindergartensCommunity kitchens
Vulnerable Micro territories
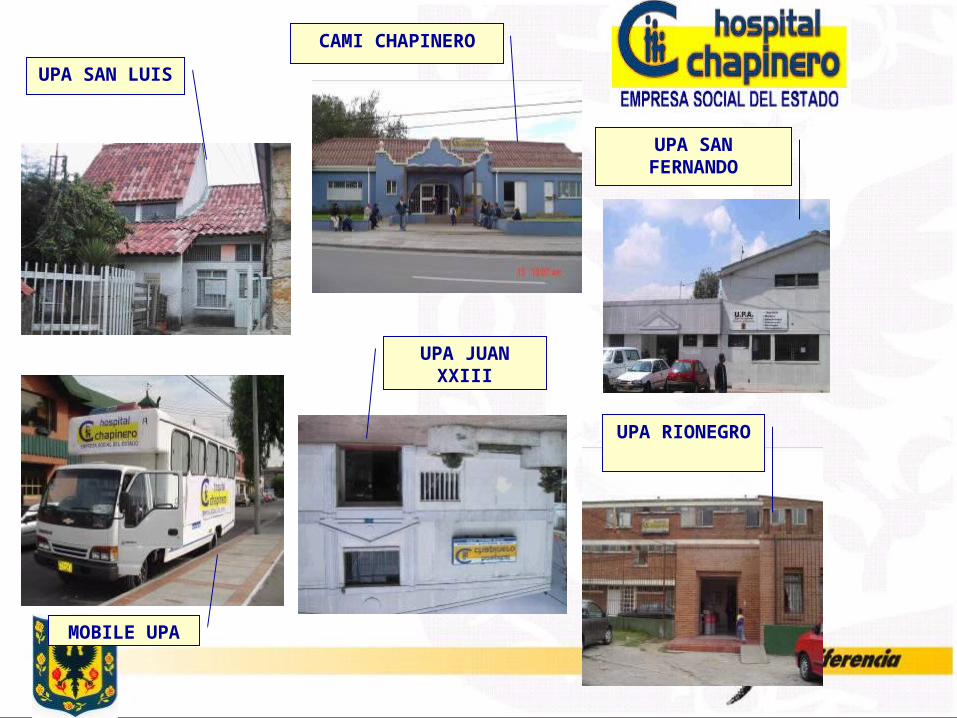
MOBILE UPA
UPA JUAN XXIII
UPA RIONEGRO
UPA SAN FERNANDO
CAMI CHAPINERO
UPA SAN LUIS

Contribute to an improvement in the quality of life and health of people who live in vulnerable territories, with an assignment of 1200 families, by lowering access barriers to sectoral, comprehensive, and transectoral care and community empowerment.
Health at HomeHealth at Home
PrioritiesPriorities
Pregnant WomenChildren under 5ElderlyDisabled Individuals diagnosed with diabetes and hypertensionWomen of childbearing ageIndividuals diagnosed with TB or leprosyCompulsory notification eventsFamilies living in vulnerable housing conditions

LIVABLE HOUSING CONDITIONS
UNLIVABLE HOUSING CONDITIONS
ASSOCIATED MORBIDITY
Privacy, enough space,Physically accessible
Overcrowding Sexual abuse, domestic violence, child abuse and ensuing problems Zoonotic diseases
Safe and secure enough Tenancy secured
Unsafe Violence in general
Adequate lighting TB, Skin diseases, COPD Adequate heating and ventilation
Housing unit is cold, damp, dark and is poorly ventilated TB, Skin diseases, COPD, ARD
Adequate walls, flooring and roofing
Presence of cracks, damage from moisture, holes,
Water seepage and leaks in roofs and walls Dirt floors, and inappropriate roofing materials
Superficial and Deep Mycosis (fungus on the skin, lungs and other organs), Acaridiasis (skin and respiratory parasites), Chronic Bronchial Allergic diseases(Asthma), COPD, TBC, ARD, pyodermitis.
Architectural conditions suited to disabilities
Architectural barriers to movement inside the home (it is difficult to access the home, bathroom, dining room, stairs, etc.)
Worsening of individuals’ disabilities
Water supply services Basic sanitation
No potable water ADD, ARD, Skin diseases
Unhealthy conditions ADD, ARD, Malnutrition, COPD, Zoonotic and parasitic diseases
Elimination of waste(Excreta)
Unhealthy conditions in and around the housing unit
ADD, ARD, Parasitic diseases Skin diseases
Appropriate factors for the quality of the environmentin the home
Inappropriate factors for thequality of environment in the home
COPD, ARD
Food security Lack of food securityand loss of beneficial traditional knowledge
Malnutrition (malnourishment, overweight, obesity, and dietary deficiencies)

Using sectoral management and health and environmental education to buttress the public health interventions that are moving forward through Health to Your Home, aimed at improving living and health conditions in the most vulnerable communities.
Healthy HousingHealthy Housing

METHODOLOGYMETHODOLOGY
1. Selecting the Health at Your Home territories
2. Housing assessment3. Establishing agreements and
commitments4. Follow-up, monitoring, and evaluation

Chart No. VS
NAME OF HEAD OF HOUSEHOLD No. inhabitants per housing unit
PHONE #
NAME OF MICROTERRITORY
101 102 103 104 105 FINAL 201 202 203 204 FINAL 301 302 303 304 305 FINAL 401 402 403 404 FINAL 501 502 503 504 FINAL 601 602 603
1. INITIAL ASSESSMENT
2.
3.
4. FINAL ASSESSMENT
Commitments:
1
2
3
4
5
6
1 2
3 4
NEIGHBORHOOD
DISTRICT SECRETARIAT OF HEALTH ON THE ROAD TO HEALTHLY HOUSING – FOR MY HOUSEHOLD TO LIVE
RECORD OF INTERVENTIONS PER FAMILY
PLACE
VISIT 200
Sips of Life – Drinking water in the Home
Signature of Sanitation Tech.
ADDRESS
DATE IF VISIT dd/mm/yyyy
VISIT 100
Housing as a vital space
ISSUES ADDRESSED
VISIT 300
Excrement and Sewerage in the open
VISIT 400
Solid Waste(Trash in the home)
VISIT 500
On the look out for Disease/pests
VISIT 600
Healthy & Sanitary Food & Housing
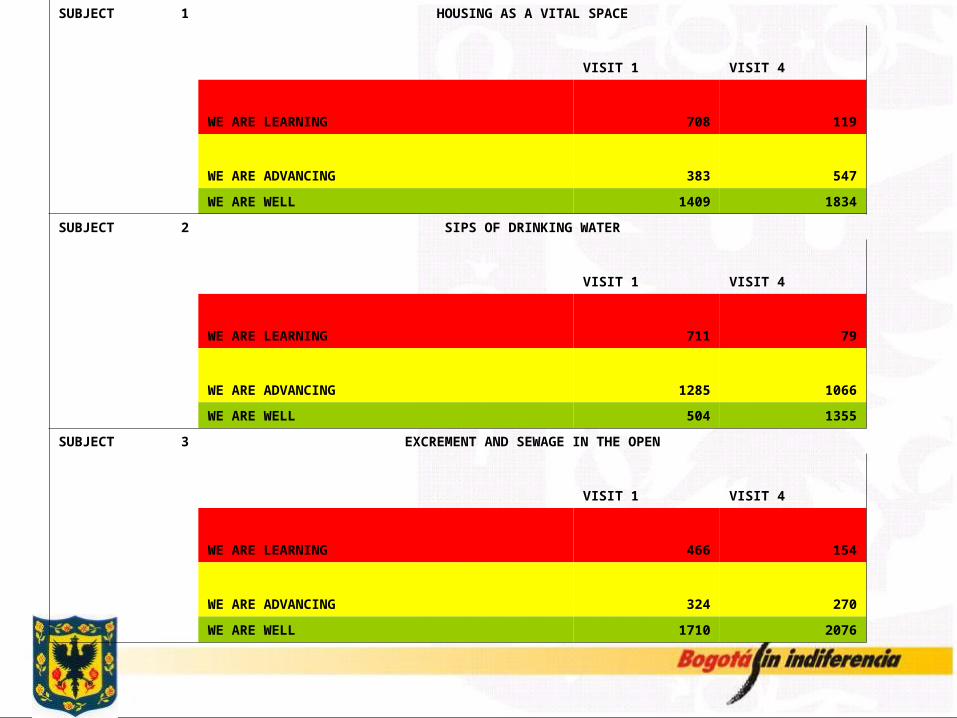
SUBJECT 1 HOUSING AS A VITAL SPACE
VISIT 1 VISIT 4
WE ARE LEARNING 708 119
WE ARE ADVANCING 383 547
WE ARE WELL 1409 1834
SUBJECT 2 SIPS OF DRINKING WATER
VISIT 1 VISIT 4
WE ARE LEARNING 711 79
WE ARE ADVANCING 1285 1066
WE ARE WELL 504 1355
SUBJECT 3 EXCREMENT AND SEWAGE IN THE OPEN
VISIT 1 VISIT 4
WE ARE LEARNING 466 154
WE ARE ADVANCING 324 270
WE ARE WELL 1710 2076

SUBJECT 4 SOLID WASTE IN THE HOME
VISIT 1 VISIT 4
WE ARE LEARNING 427 145
WE ARE ADVANCING 1387 907
WE ARE WELL 686 1448
SUBJECT 5 ON THE LOOK OUT FOR DISEASE/PESTS
VISIT 1 VISIT 4
WE ARE LEARNING 135 172
WE ARE ADVANCING 1202 1016
WE ARE WELL 1163 1312
SUBJECT 6 HEALTHY AND SANITARY FOOD AND HOUSING
VISIT 1 VISIT 4
WE ARE LEARNING 73 42
WE ARE ADVANCING 787 336
WE ARE WELL 1640 2122

Progress with Characterization: Identifying Needs
RISKS FOUND IN THE HOME DURING THE IDENTIFICATION AND CHARACTERIZATION OF
FAMILY GROUPS
5%7% 7%
16% 16%
0%2%4%6%8%
10%12%14%16%18%
Ove
rflo
win
g,
ris
ing
wa
ters
Flo
odi
ng o
f
pro
pert
y
Geo
log
ical
f
aul
ts
Ava
lan
ches
,C
olla
pses
, or
la
nd s
lides
Flo
ods

HEALTH AGREEMENT AND HABITAT HEALTH AGREEMENT AND HABITAT AS A LINCHIPINAS A LINCHIPIN
… mutually aid habitat development and improve the quality of life and health of the families of Bogotá, as part of the Primary Health Care strategy and the Health at Your Home program…
SUBSIDY FOR MAKING HOUSING MORE SUBSIDY FOR MAKING HOUSING MORE LIVABLE LIVABLE
Allocating resources for construction in the housing sector to improve basic health conditions, with priority given to improving bathrooms and kitchens or basic sanitation conditions.

INTERVENTION PROPOSAL
UNLIVABLE HOUSING CONDITIONS INTERVENTION PROPSOALOvercrowding Improve and/or redistribute living space inside
the homeImprove the conditions of bathrooms and kitchen
Lack of security Doors, windowsHome is cold, damp, dark and has poor ventilation Improve conditions with respect to ventilation,
lighting, kitchen, bathrooms, and the home’s non-structural materials
No potable water Connect to formal public services system or set up alternatepotable water systems
Improve kitchen and bathroom conditions
Unhealthy conditions Connect to sewage or set up alternate human waste and trashelimination systems
Provide toilets
Improve kitchen and bathroom conditionsCertain factors contributing to a poor quality homeenvironment
Improve kitchen and fuel use
Food insecurity and loss of traditional knowledge Promote use of vegetable gardens, medicinal and/or edible plants through urban agriculture
SUBSIDY SUBSIDY
up to 6.5 SMLMV
$2,800,000
1,400 dollars

COST OF CARE FOR BOYS AND GIRLS WITHCOST OF CARE FOR BOYS AND GIRLS WITH ACUTE RESPIRATORY DISEASESACUTE RESPIRATORY DISEASES
CARE APPROX. COST IN DOLLARS
FIRST-LEVEL EXPENSE US 200SECOND-LEVEL EXPENSE US 300THIRD LEVEL EXPENSE US 400INTENSIVE CARE UNIT (ICU) US 520

AVERAGE COST AVERAGE COST LIVABLE CONDITIONSLIVABLE CONDITIONS
Approximately US 1,500
SOURCE: CALCULOS CVP SOURCE: CALCULOS CVP NOTE: THIS AVERAGE DOES NOT INCLUDE STRUCTURAL NOTE: THIS AVERAGE DOES NOT INCLUDE STRUCTURAL INTERVENTIONSINTERVENTIONS

PRODUCTS
TECHNICAL ASSISTANCE FOR FAMILIESAPPLIYING FOR A SUBSIDY
HIRING BUILDERSASSISTANCE WITH PROPERTY TITLES
USME HOSPITAL
19 TECHNICAL TEAMS: ARCHITECT OR CIVIL ENGINEERSANITATION TECHNICIAN SOCIAL PROMOTER
TRAINING FOR THE TEAMS
APPLICATION OF FORMS: SANITATION, TECHNICAL, AND SOCIAL

POLITICAL RESULT
Notion of citizen health Inclusion of health in development plans. Decisionmakers.Organized mobilization of resources from other sectorsBetter quality of life for the population

POLITICAL RESULT
National debate on the insurance model, especially the national public health plan. Inclusion of structural health determinants. Organizational process and social mobilization. Bring other parts of the health sector into play, especially insurance companies in promotion and prevention.
A PHC-BASED HEALTH SYSTEM
PHC AND INSURANCE
HEALTH TO SCHOOL
I FEEL WELL I LEARN WELL

THANK YOU!