primary debulking for bulky advanced stage ovarian cancer ginger j. gardner, md director,...
TRANSCRIPT
Primary Debulking for Bulky Advanced Stage Ovarian Cancer
Ginger J. Gardner, MDDirector, Survivorship Program
Gynecology Service, Department of SurgeryMemorial Sloan-Kettering Cancer Center
Ovarian CarcinomaOvarian Carcinoma
Prognostic FactorsAgeAge
StageStageGradeGrade
HistologyHistologyAscitesAscites
ChemosensitivityChemosensitivityVolume of Residual DiseaseVolume of Residual Disease

Primary Debulking Surgery for Advanced Stage Disease Primary Debulking Surgery
for Advanced Stage Disease
Bristow, RE, JCO, 20:1248, 2002
• Meta-AnalysisMeta-Analysis• Medline database 1989 – 1998Medline database 1989 – 1998• Stage III-IV Ovarian CancerStage III-IV Ovarian Cancer• 6885 patients6885 patients• Multiple linear regression analysisMultiple linear regression analysis
****Each 10% increase in maximum Each 10% increase in maximum cytoreductive surgery was associated with a cytoreductive surgery was associated with a 5.5% increase in median overall survival5.5% increase in median overall survival

20
22
24
26
28
30
32
34
36
38
40
0 10 20 30 40 50 60 70 80 90 100
% Cytoreduction
Med
ian
Sur
viva
l (M
onth
s)
Significant survival advantagefor women optimally cytoreduced
Procedures may include: -En bloc resection of uterus ovaries and pelvic tumor -Omentectomy -Lymphadenectomy -Bowel resection -Diaphragm resection -Splenectomy, Appendectomy
Primary Debulking Surgery for Advanced Stage Disease Primary Debulking Surgery
for Advanced Stage Disease
Bristow, RE, JCO, 20:1248, 2002
Cytoreductive Surgery for Advanced Stage Disease
The Rationale
Cytoreductive Surgery for Advanced Stage Disease
The Rationale • Excision of large tumor mass of poorly perfused,
anoxic cells which would otherwise be exposed to sublethal concentration of drug
• Increase proliferating fraction of cells post-op
• Removal of 80-90% tumor burden favorable to "fractional cell kill hypothesis"
• Reduce the opportunity for drug resistance by start-stop chemotherapy approach with neoadjuvant therapy

Modified Posterior Pelvic Exenteration
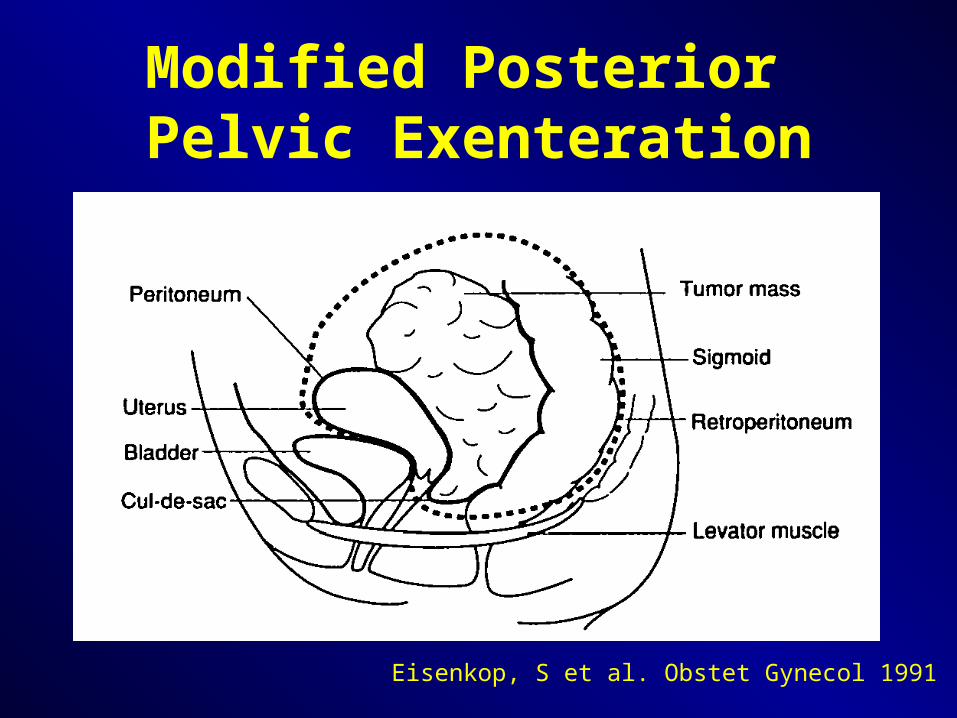
Eisenkop, S et al. Obstet Gynecol 1991
Modified Posterior Pelvic Exenteration
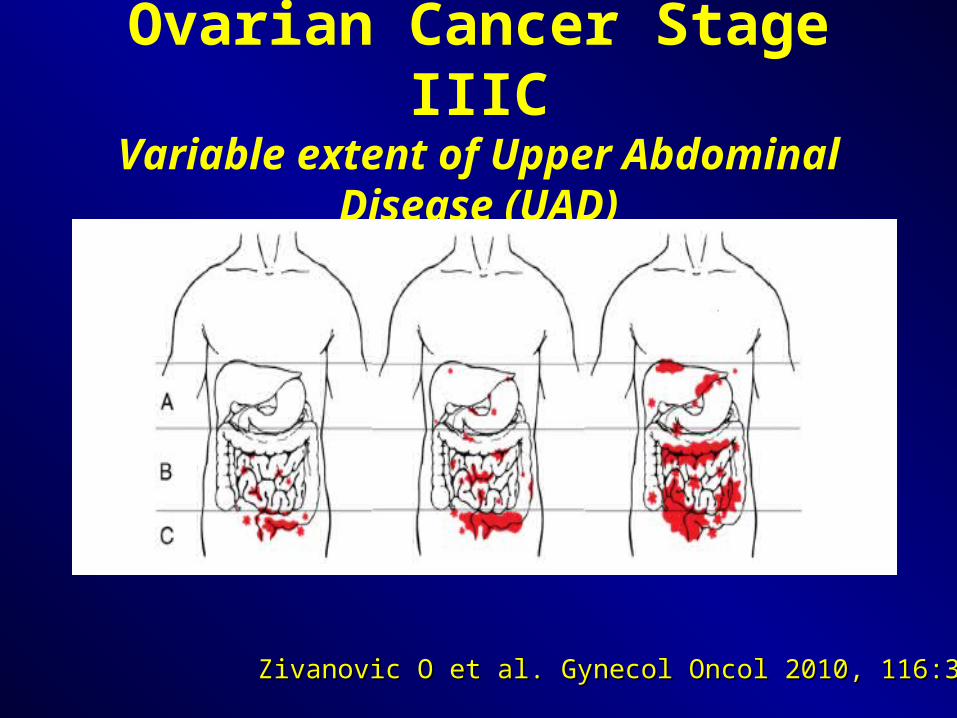
Ovarian Cancer Stage IIICVariable extent of Upper Abdominal
Disease (UAD)
Zivanovic O et al. Gynecol Oncol 2010, 116:351-7Zivanovic O et al. Gynecol Oncol 2010, 116:351-7

Bulky UAD Cephlad to the Greater Omentum
Zivanovic O et al. Gynecol Oncol 2010, 116:351-7Zivanovic O et al. Gynecol Oncol 2010, 116:351-7
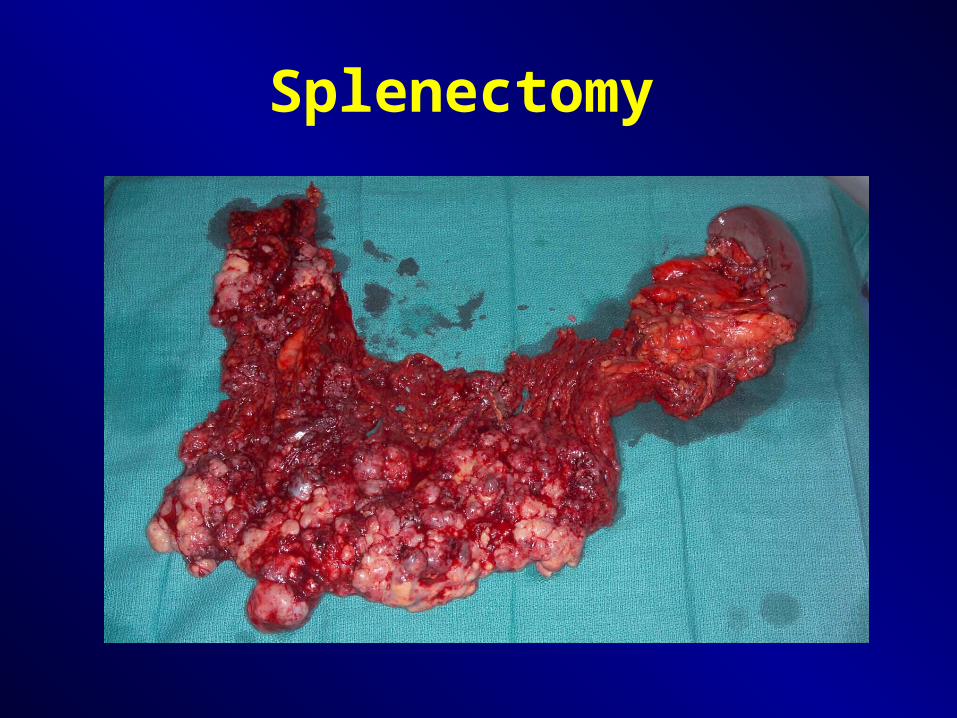
Splenectomy

Splenectomy with Distal Pancreatectomy
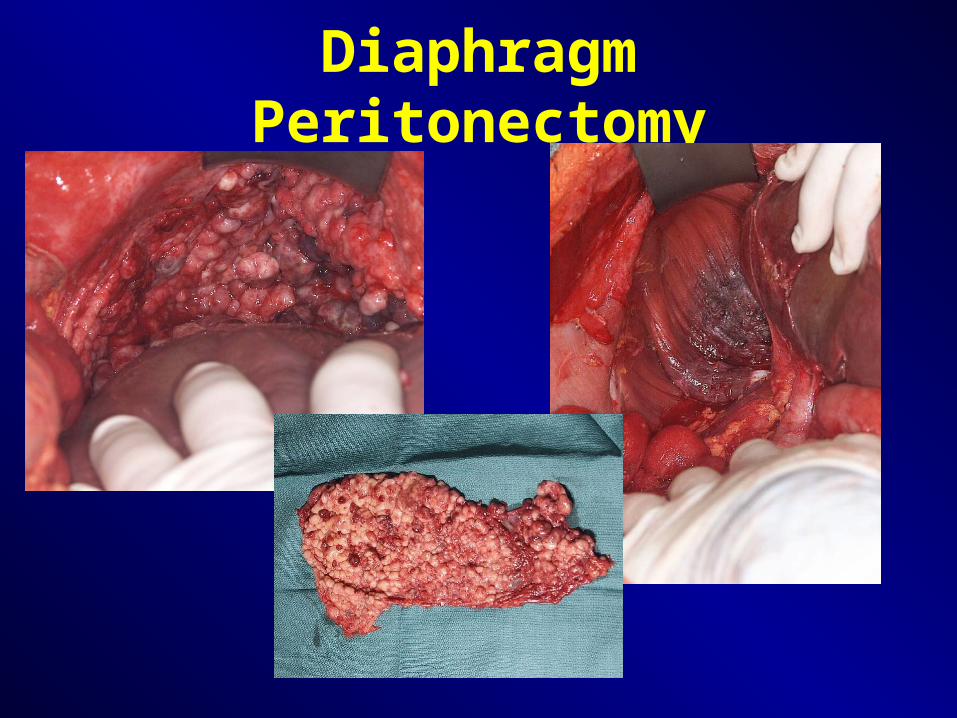
Diaphragm Peritonectomy
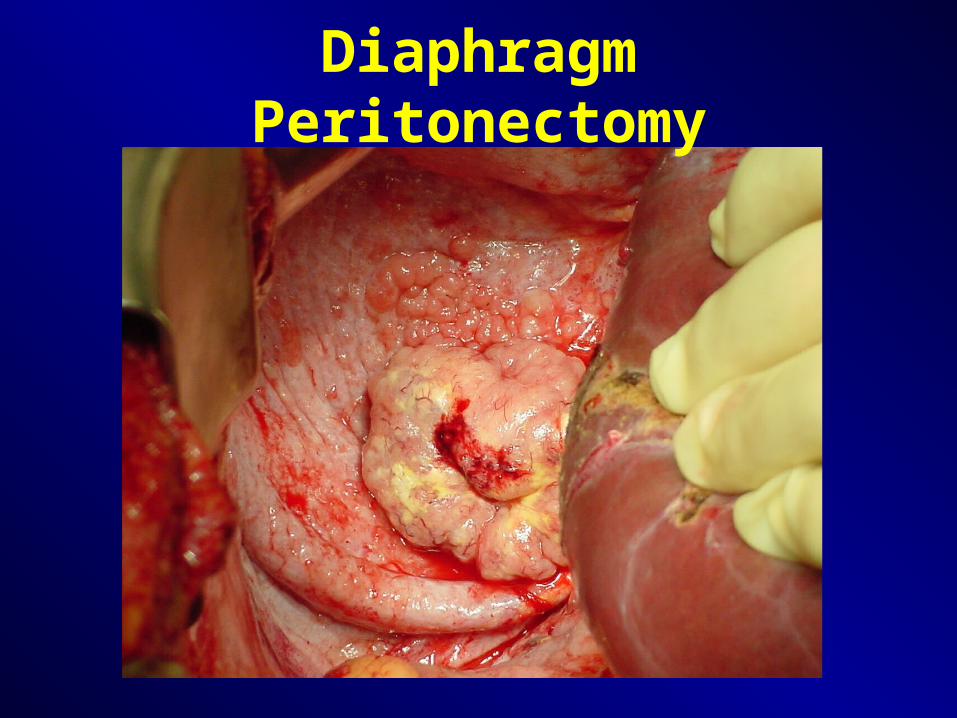
Diaphragm Peritonectomy

Liver and Diaphragm Resection
Cut edge of liver
Pleural Space


Randomized EORTC/NCIC Trial Randomized EORTC/NCIC Trial of NACT + IDS vs PDSof NACT + IDS vs PDS
Randomized EORTC/NCIC Trial Randomized EORTC/NCIC Trial of NACT + IDS vs PDSof NACT + IDS vs PDS

• Sept 1998 – Dec 2006Sept 1998 – Dec 2006• 670 pts randomized670 pts randomized• 59 institutions59 institutions• Eligible pts: Stage IIIC-IV disease with ≥2cm Eligible pts: Stage IIIC-IV disease with ≥2cm
upper abdominal diseaseupper abdominal disease• Optimal Debulking (≤1cm)Optimal Debulking (≤1cm)
• 41.6% PDS41.6% PDS• 80.6% IDS 80.6% IDS
NACT vs PDSNACT vs PDS
Vergote I, et al. NEJM 363:10
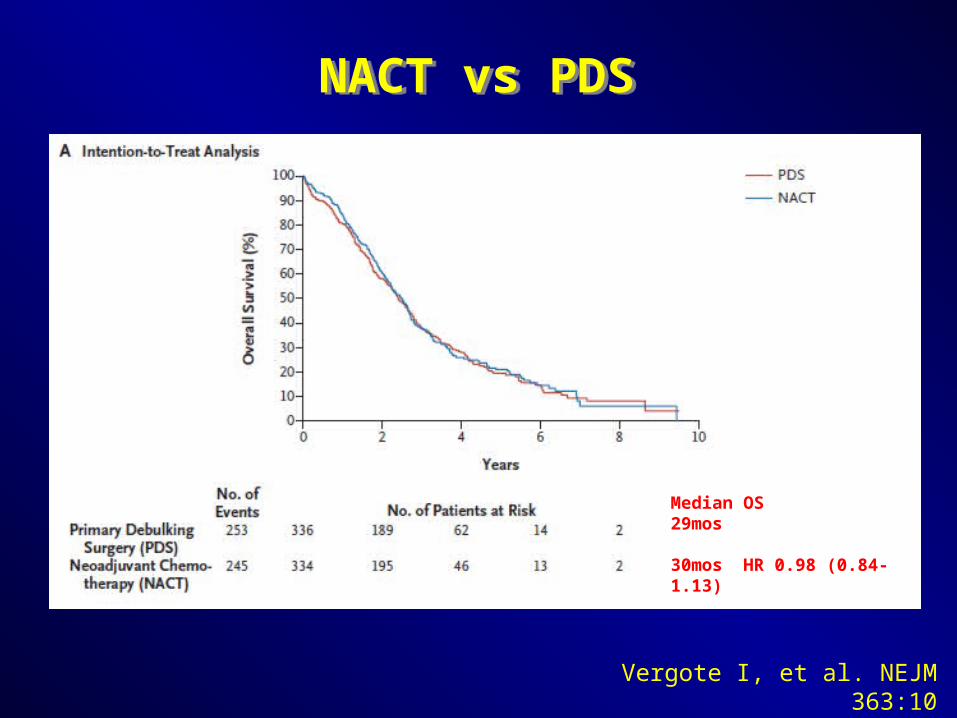
Vergote I, et al. NEJM 363:10
Median OS29mos
30mos HR 0.98 (0.84-1.13)
NACT vs PDSNACT vs PDS

• Complete resection of all macroscopic disease Complete resection of all macroscopic disease (PDS or IDS) was the strongest independent (PDS or IDS) was the strongest independent predictor of OS, p<0.001predictor of OS, p<0.001
• Followed by: Followed by: • Stage IIIC (vs stage IV), p=0.001 Stage IIIC (vs stage IV), p=0.001 • Small tumor size at randomization, p=0.001Small tumor size at randomization, p=0.001• Endometrioid histology, p=0.005Endometrioid histology, p=0.005• Younger age, p=0.005Younger age, p=0.005
Predictors of Prolonged SurvivalMultivariate Analysis
Predictors of Prolonged SurvivalMultivariate Analysis
Vergote I, et al. NEJM 363:10
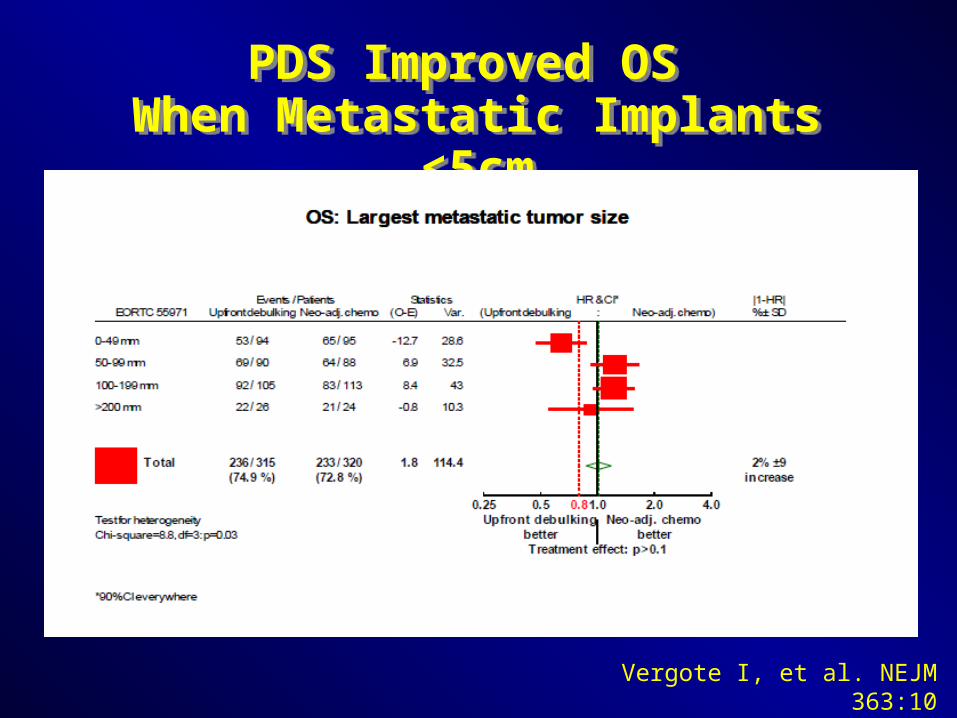
PDS Improved OS When Metastatic Implants <5cm
PDS Improved OS When Metastatic Implants <5cm
Vergote I, et al. NEJM 363:10

Summary from Vergote StudySummary from Vergote Study
• Complete gross resection associated with best Complete gross resection associated with best OS for both PDS and IDSOS for both PDS and IDS
• NACT may be an option for advanced stage NACT may be an option for advanced stage ovarian cancer with >5cm distant metastatic ovarian cancer with >5cm distant metastatic implants…implants…
Should NACT be the new standard of care?Should NACT be the new standard of care?

Questions Remain….Questions Remain….
• Low rate of primary optimal debulking: 41.6%Low rate of primary optimal debulking: 41.6%
• Median OS: 30mosMedian OS: 30mos• Difficult to enroll good operative candidates onto Difficult to enroll good operative candidates onto
the surgical trialsthe surgical trials• After debulking, the diagnosis changed in 11pts After debulking, the diagnosis changed in 11pts
(3.3%) PDS and 7 pts (2.1%) IDS: (3.3%) PDS and 7 pts (2.1%) IDS: carcinosarcoma, carcinosarcoma, endometrial ca, GI tumors, LMPs, cervical adenoca, endometrial ca, GI tumors, LMPs, cervical adenoca, teratoma, rhabdomyosarcoma, pseudomyxomateratoma, rhabdomyosarcoma, pseudomyxoma
• Histologic grade unknown in 35-45% of casesHistologic grade unknown in 35-45% of cases

Acceptance of NACT by SGO Members
Acceptance of NACT by SGO Members
Dewdney S et al. Gynecol Oncol 2010, 119:18-21
• 339/1137 (30%) responded339/1137 (30%) responded• 98.2% Gynecologic Oncologists98.2% Gynecologic Oncologists• 94.6% in United States94.6% in United States
• 59.2% Academic Practice59.2% Academic Practice• 66.7% Male66.7% Male
• Years in Practice: 39.8% (>15yrs), 22.8% (<5yrs)Years in Practice: 39.8% (>15yrs), 22.8% (<5yrs)

Acceptance of NACT by SGO Members
Acceptance of NACT by SGO Members
Dewdney S et al. Gynecol Oncol 2010, 119:18-21
• Rate of Optimal DebulkingRate of Optimal Debulking• 42% of GYOs report a 61-80% rate of optimal 42% of GYOs report a 61-80% rate of optimal
debulkingdebulking• 38.9% of GYOs report a >80% rate of optimal 38.9% of GYOs report a >80% rate of optimal
debulkingdebulking
• Rate of NACTRate of NACT• 60% of GYOs give NACT less for <10% of 60% of GYOs give NACT less for <10% of
casescases

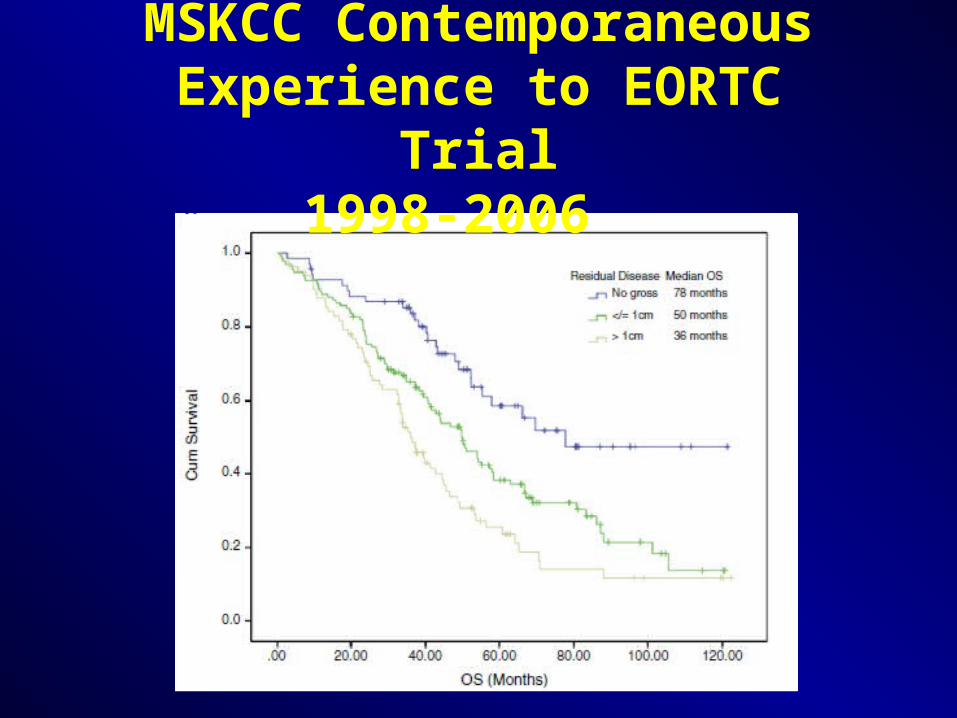
Conclusions
-Cytoreduction to > 1 cm residual has no benefit on overall survival
-There is a survival benefit associated with cytoreduction to < 1 cm residual
-Within the gross residual but < 1 cm category, no gross residual is associated with the longest median survival

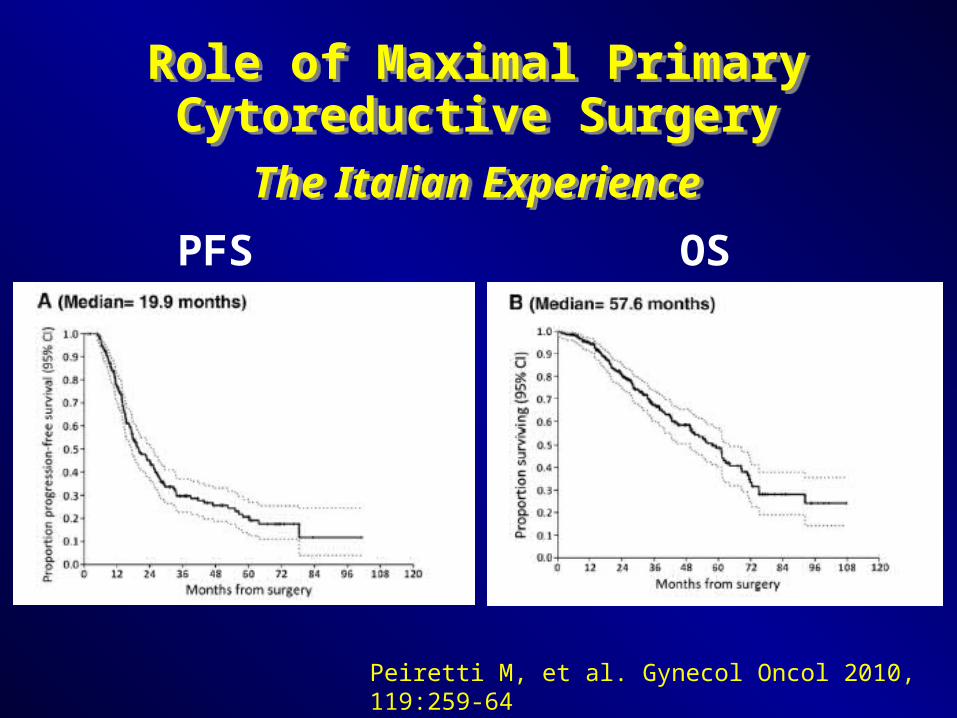
Role of Maximal Primary Cytoreductive Surgery
The Italian Experience
Role of Maximal Primary Cytoreductive Surgery
The Italian Experience
Peiretti M, et al. Gynecol Oncol 2010, 119:259-64
Peiretti M, et al. Gynecol Oncol 2010, 119:259-64
Role of Maximal Primary Cytoreductive Surgery
The Italian Experience
Role of Maximal Primary Cytoreductive Surgery
The Italian Experience
PFS OS

MSKCC Contemporaneous Experience to EORTC Trial
• Identical inclusion criteria for all patients undergoing primary surgery at MSKCC during same time period (9/98-12/06)
• Excluded patients with borderline, germ cell, stromal, and advanced carcinoma based solely on microscopic nodal metastasis
• All pts “eligible” for EORTC trial: 316
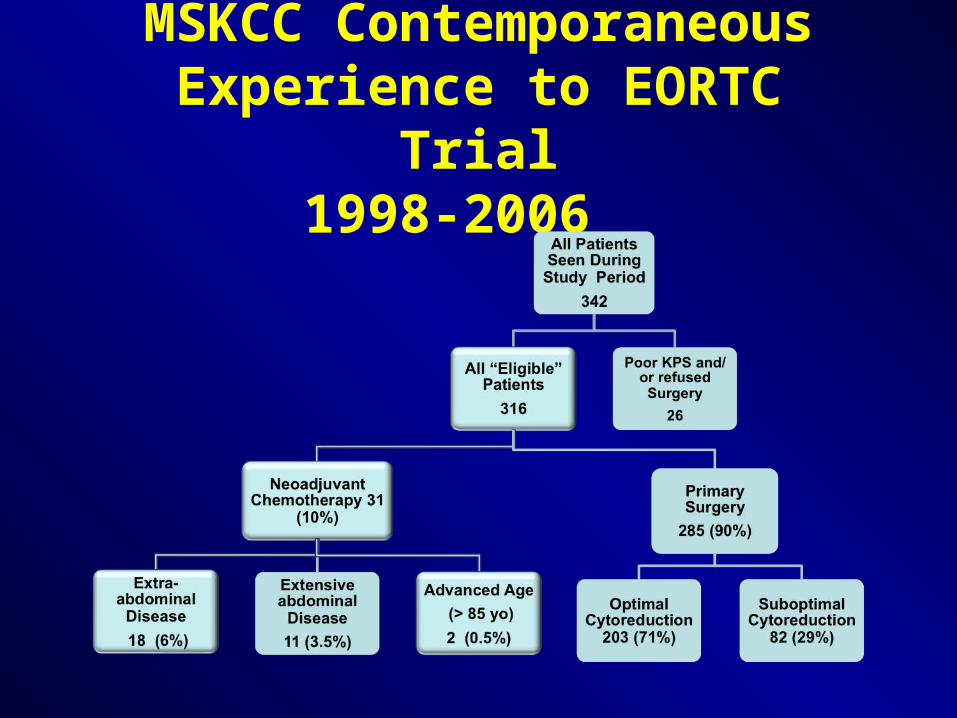
MSKCC Contemporaneous Experience to EORTC Trial
1998-2006
MSKCC Contemporaneous Experience to EORTC Trial
1998-2006
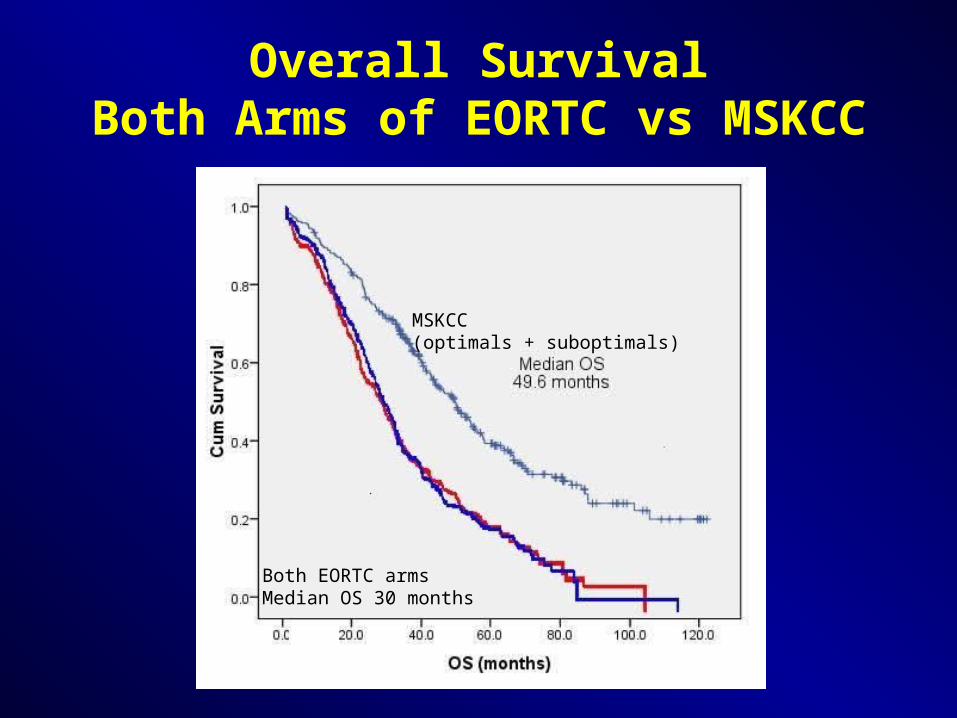
Overall Survival Both Arms of EORTC vs MSKCC
MSKCC (optimals + suboptimals)
Both EORTC armsMedian OS 30 months
• Quality of Life, Vergote 2010Quality of Life, Vergote 2010• QLQ-C30 global health scores were not QLQ-C30 global health scores were not
significantly different between the NACT and significantly different between the NACT and PDS groups at any of the 5 time points PDS groups at any of the 5 time points evaluatedevaluated
Even if we consider PDS and NACT OS equivalent,…what about factors?
Even if we consider PDS and NACT OS equivalent,…what about factors?

• Cost Effectiveness, Aletti 2009Cost Effectiveness, Aletti 2009• Surigcal Complexity Score (SCS): 1-3Surigcal Complexity Score (SCS): 1-3• Inpatient costs $21k, $27k, $33k; p<0.001Inpatient costs $21k, $27k, $33k; p<0.001• $4950 / life yr gained for SCS 2 vs 1$4950 / life yr gained for SCS 2 vs 1• $8912 / life yr gained for SCS 3 vs 1$8912 / life yr gained for SCS 3 vs 1
Even if we consider PDS and NACT OS equivalent,…what about factors?
Even if we consider PDS and NACT OS equivalent,…what about factors?

Intraperitoneal (IP) ChemotherapyImproves Survival
Intraperitoneal (IP) ChemotherapyImproves Survival
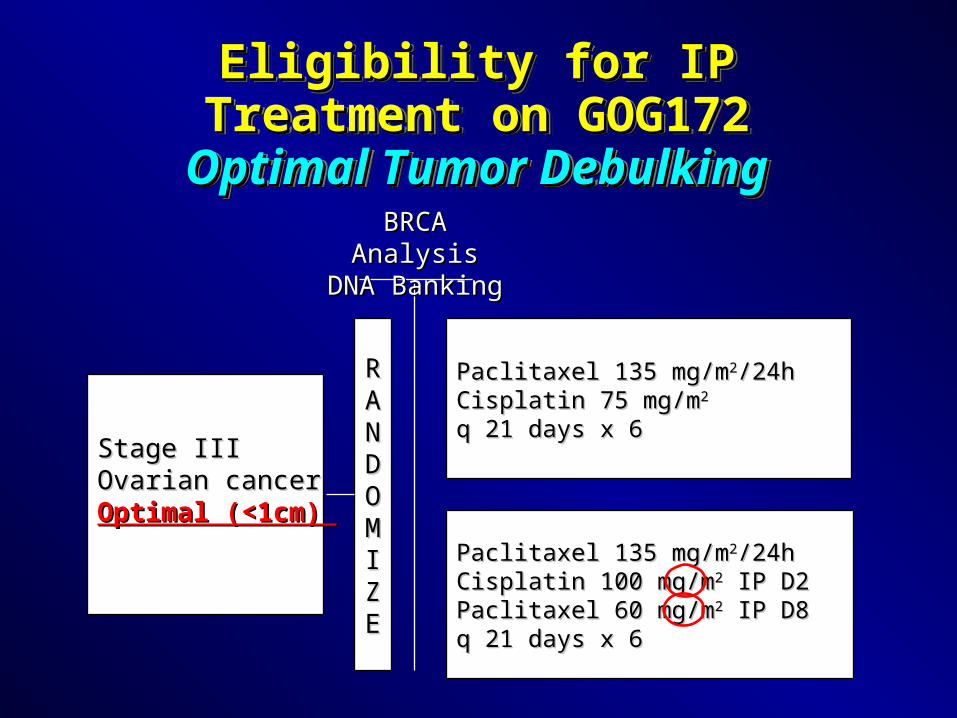
Stage IIIStage IIIOvarian cancerOvarian cancerOptimal (<1cm) Optimal (<1cm)
RRAANNDDOOMMIIZZEE
BRCA AnalysisBRCA AnalysisDNA BankingDNA Banking
Paclitaxel 135 mg/mPaclitaxel 135 mg/m22/24h/24hCisplatin 75 mg/mCisplatin 75 mg/m22 q 21 days x 6q 21 days x 6
Paclitaxel 135 mg/mPaclitaxel 135 mg/m22/24h/24hCisplatin 100 mg/mCisplatin 100 mg/m22 IP D2 IP D2Paclitaxel 60 mg/mPaclitaxel 60 mg/m22 IP D8 IP D8q 21 days x 6q 21 days x 6
Eligibility for IP Treatment on Eligibility for IP Treatment on GOG172GOG172
Optimal Tumor DebulkingOptimal Tumor Debulking
Eligibility for IP Treatment on Eligibility for IP Treatment on GOG172GOG172
Optimal Tumor DebulkingOptimal Tumor Debulking

GOG 172 SurvivalPatient Eligibility: Completed Primary
Optimal Debulking (≤1cm)
Regimen 1
Intravenous
Regimen 2
Intraperitoneal
Progression-free 18.3 mos 23.8 mos
Overall Survival 49.5 mos 66.9 mos

Advanced Ovarian Cancer
CisplatinCisplatin PaclitaxelPaclitaxelMulti-drugMulti-drug AlkeranAlkeran
Improving Overall SurvivalImproving Overall Survival
IP therapyIP therapy
(optimal)(optimal)
(optimal)(optimal)
mon
ths
mon
ths
1212 14142424
3737
5252 57.457.465.665.6
00
2020
4040
6060
8080
19751975 19831983 19861986 19961996 19981998 20032003 20052005

Primary Debulking for Advanced Ovarian Cancer
Summary
Primary Debulking for Advanced Ovarian Cancer
Summary• Large body of retrospective data supports primary Large body of retrospective data supports primary
debulking surgery, now with median 5yr overall debulking surgery, now with median 5yr overall survival.survival.
• Survival benefit includes resection of bulky upper Survival benefit includes resection of bulky upper abdominal disease located cephalad to the abdominal disease located cephalad to the greater omentum.greater omentum.
• One RCT shows non-inferiority of NACT for large One RCT shows non-inferiority of NACT for large volume distant metastasis (>5cm), but had low volume distant metastasis (>5cm), but had low median survival, and no benefit for QOL or cost.median survival, and no benefit for QOL or cost.

Primary Debulking for Advanced Ovarian Cancer
Summary
Primary Debulking for Advanced Ovarian Cancer
Summary• MSKCC analysis using the same eligibility criteria MSKCC analysis using the same eligibility criteria
demonstrates a longer overall survival.demonstrates a longer overall survival.
• Eligibility for adjuvant IP chemotherapy is based Eligibility for adjuvant IP chemotherapy is based on optimal tumor debulking status.on optimal tumor debulking status.
• We should prioritize optimal primary debulking We should prioritize optimal primary debulking surgery, and use NACT only in selected cases.surgery, and use NACT only in selected cases.
• Our goal is to provide our patients excellence in Our goal is to provide our patients excellence in surgical technique as we continue to expand our surgical technique as we continue to expand our chemotherapy repetoire for ovarian cancer.chemotherapy repetoire for ovarian cancer.
