primary care trigger tool manaia health pho linda holman quality leader
TRANSCRIPT

Primary Care Trigger Tool
Manaia Health PHO
Linda Holman Quality Leader
Background•F
ew studies on trigger tool use in primary care
•Primary care trigger tools have been used in Scotland and England NHS
•Sensitivity and specificity of primary care trigger tool in identifying harm not known
Method• 37 triggers used initially
• 170 patients in one large general practice identified
• 50% of cohort Māori
• Included children
• Record for one year reviewed looking for presence of triggers and associated harm
• Record also reviewed for harm without any trigger
• 2 review teams (GP + nurse/pharmacist)
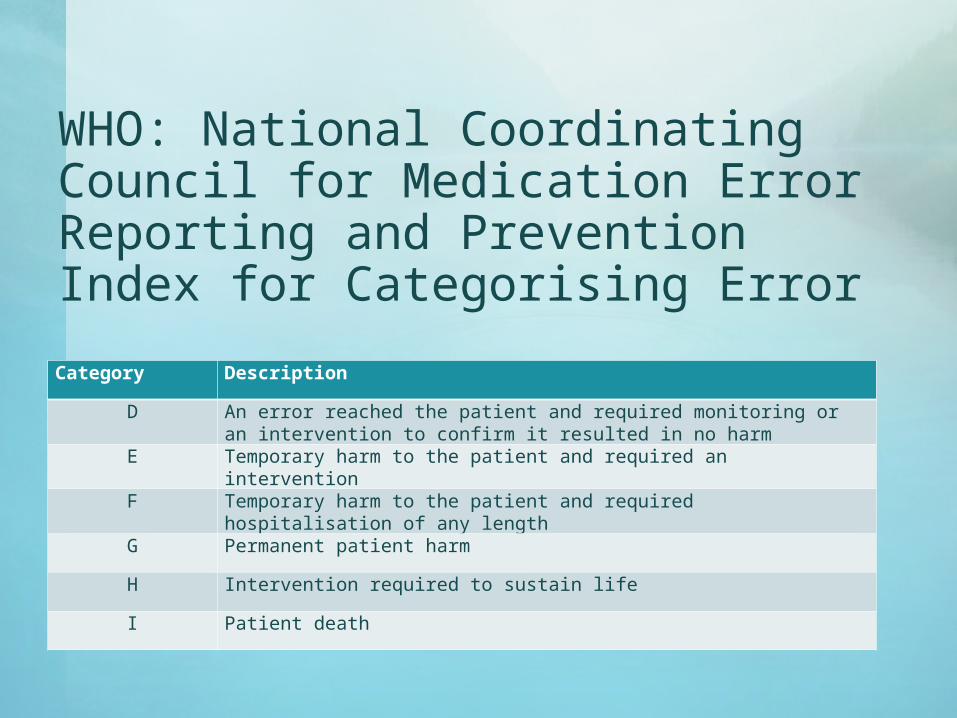
WHO: National Coordinating Council for Medication Error Reporting and Prevention Index for Categorising Error
Category Description
D An error reached the patient and required monitoring or an intervention to confirm it resulted in no harm
E Temporary harm to the patient and required an intervention
F Temporary harm to the patient and required hospitalisation of any length
G Permanent patient harm
H Intervention required to sustain life
I Patient death
Findings•1
034 triggers initially identified
•40 030 days of follow-up
•637 consultations
•Harm found in 63 of these triggers + 1 outside of the defined triggers(corresponding to 45 individual events)
•Harm categories: E = 48, F = 11, G = 3, H = 0, I = 1
Rates of Harm•R
ate of harm: 0.07 (95% CI 0.05-0.09)
•Rate of harm per 100 patient years = 41 (95% CI 29-55)
•Rate of harm between Māori and non-Māori no difference (adjusting for age and sex)
•Rate of harm if male 0.53 (95% CI 0.29-0.98) adjusting for age and ethnicity
Triggers refined & reduced to 8
Adverse reaction documented in PMS ≥ consultations with a GP in 1 week Cessation of medication Reduction in medication dose ≥6 medications prescribed Seen in ED/A+M within 2 weeks of seeing
GP eGFR < 35 Death
Efficacy of Refined Tool•O
dds ratio of harm occurring is refined trigger tool used (adjusting for age, sex and ethnicity) 6.3 (95% CI 2.7-14.8)
•Sensitivity of refined trigger tool 0.88
•Specificity of refined trigger tool 0.48
Discussion•R
ates of harm comparable to published literature in primary care
•Predominant cause of harm from medication
•Small number of harms that could be linked to an actual error
•Value in pharmacist being involved
•Qualitative information gained during process valuable
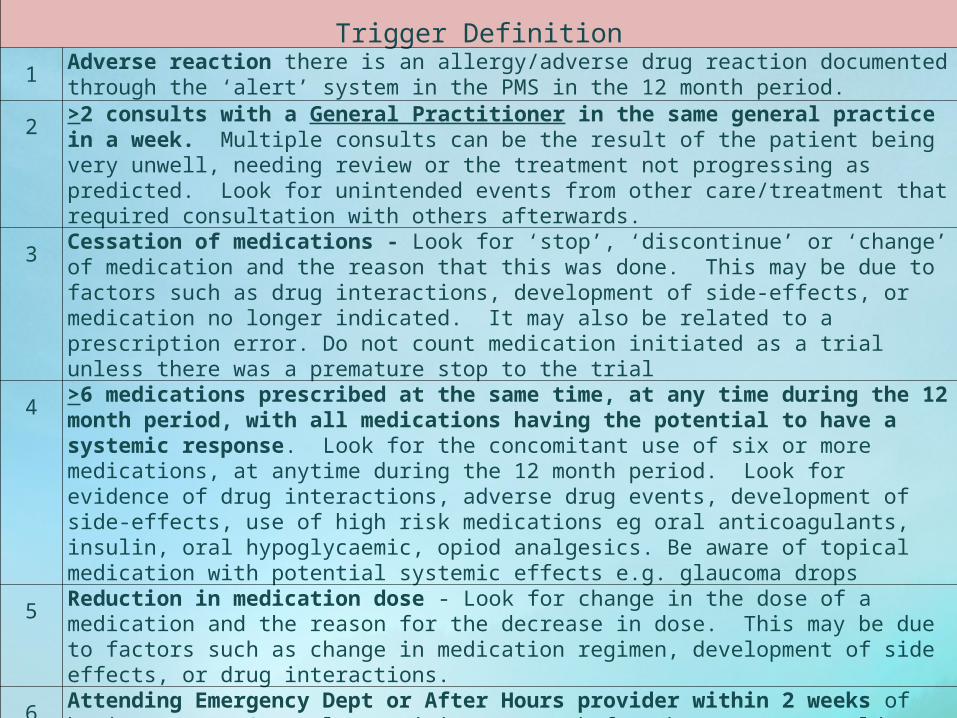
Trigger Definition1 Adverse reaction there is an allergy/adverse drug reaction documented through the ‘alert’ system in
the PMS in the 12 month period.
2 >2 consults with a General Practitioner in the same general practice in a week. Multiple consults can be the result of the patient being very unwell, needing review or the treatment not progressing as predicted. Look for unintended events from other care/treatment that required consultation with others afterwards.
3 Cessation of medications - Look for ‘stop’, ‘discontinue’ or ‘change’ of medication and the reason that this was done. This may be due to factors such as drug interactions, development of side-effects, or medication no longer indicated. It may also be related to a prescription error. Do not count medication initiated as a trial unless there was a premature stop to the trial
4 >6 medications prescribed at the same time, at any time during the 12 month period, with all medications having the potential to have a systemic response. Look for the concomitant use of six or more medications, at anytime during the 12 month period. Look for evidence of drug interactions, adverse drug events, development of side-effects, use of high risk medications eg oral anticoagulants, insulin, oral hypoglycaemic, opiod analgesics. Be aware of topical medication with potential systemic effects e.g. glaucoma drops
5 Reduction in medication dose - Look for change in the dose of a medication and the reason for the decrease in dose. This may be due to factors such as change in medication regimen, development of side effects, or drug interactions.
6 Attending Emergency Dept or After Hours provider within 2 weeks of having seen a General Practitioner. Look for the reasons, could indicate for example an inadequate response to GP initiated treatment, incorrect diagnosis, inability to access GP review or deterioration of the patients health.
7 eGFR (<35) Patients with results outside of range have a greater risk of experiencing an adverse event. The lab value is only a trigger, so look for evidence of harm.
8 Death during the 12 month period.