prezentace aplikace powerpoint · isotonic hypotonic more hypotonic a/ isotonic solutions –the...
TRANSCRIPT
Blood Physiology
Practical 3
© Katarína Babinská, MD, PhD. MSc., 2018
ContentsBlood plasma, osmotic pressure and oncotic
pressure. Erythrocyte osmotic resistance.
Blood density and its determinants.
Haemostasis
Practical tasks1. Determination of erythrocyte osmotic resistance
2. Determination of blood density
3. Blood coagulation time determination by the
Lee – White method
4. Determination of bleeding time by the Duke
method
5. Determination of the thromboplastin time by the
Quick test
Determination of the erythrocyte osmotic resistance
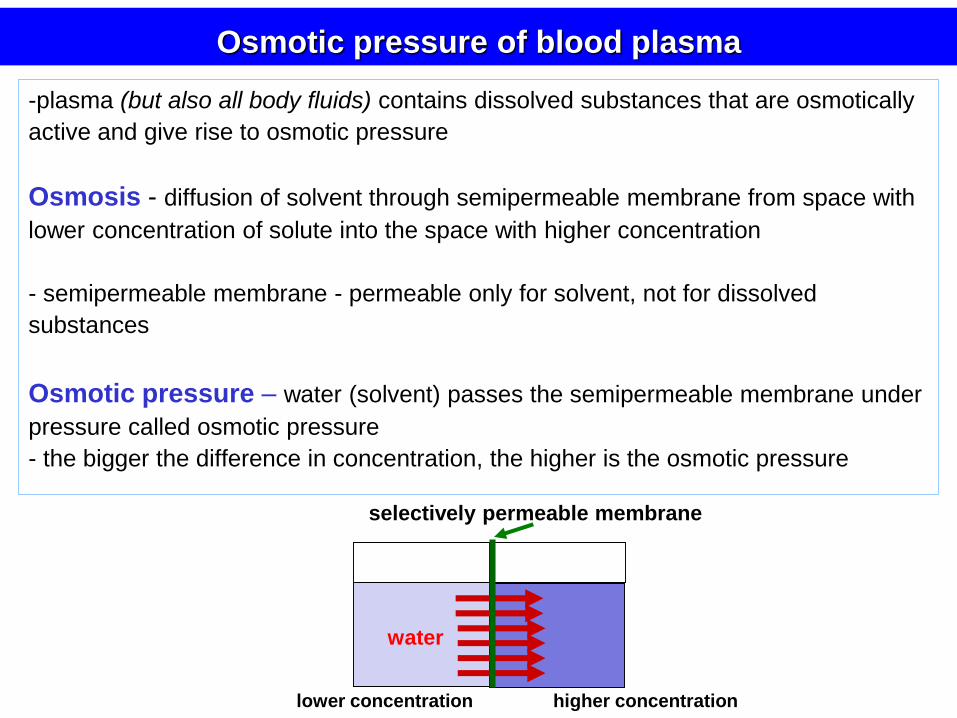
-plasma (but also all body fluids) contains dissolved substances that are osmotically
active and give rise to osmotic pressure
Osmosis - diffusion of solvent through semipermeable membrane from space with
lower concentration of solute into the space with higher concentration
- semipermeable membrane - permeable only for solvent, not for dissolved
substances
Osmotic pressure – water (solvent) passes the semipermeable membrane under
pressure called osmotic pressure
- the bigger the difference in concentration, the higher is the osmotic pressure
selectively permeable membrane
Osmotic pressure of blood plasma
lower concentration higher concentration
vodap
water

- normal value 690 kPa
- depends on concentration od osmotically active substances
- osmolarity of plasma (concentration of osmotically active substances):
290 - 300 mmol.l-1
- osmotic forces are generated mainly by Na+, Cl-, glucose, albumin
Osmotic pressure of blood plasma
Some functions in human body are based on osmotic pressure, e.g.:
• regulation of water balance - hypothalamus monitors osmolarity of plasma
• absorption in gut
• water reabsorption in kidney
• osmotic pressure needs to be considered when patient is given an infusion, or in
laboratory experiments with blood
water plasma
690 kPa
- blood plasma and blood elements – are isoosmotic (isotonic)
= osmotic equilibrium – no water gain/loss

isotonic
hypertonic
hypotonic
Osmotic resistance of erythrocytes – the ability to
resist small changes in osmotic pressure
lysisisotonic hypotonic more hypotonic
A/ Isotonic solutions
– the same osmotic pressure as plasma, optimum for function
of Ery
B/ Hypertonic solutions
– higher osmotic pressure
– if a cell („isotonic solution“) is put into a hypertonic solution,
it loses water, shrinks and may malfunction or die due to
rupture of its membrane (haemolysis)
C/ Hypotonic solutions
– lower osmotic pressure
– water flow is directed into the erythrocyte
– cause expansion of cells, their malfunction and eventually
destruction and death (haemolysis)

In intravenous administration of solutions
(fluids, nutrients, drugs)
• their concentration of osmotically active substances is adjusted to isotonicity
• isotonic solutions:
– 0,9 % NaCl (physiological solution)
– 5 % glucose
– they can be infused without danger of disturbing osmotic equilibrium
• non – isotonic solutions may be used in
special circumstances
– e.g. hypertonic solution in cerebral
oedema – water is attracted from
brain tissue into the circulation
osmotic equilibrium can be broken in dehydration, after infusion of non-isotonic solution

- a component of osmotic pressure
- exerted by plasma albumins
- normal value: 3,7 kPa
(out of 690 kPa of the total osmotic pressure)
proteinwater
tissue blood capillary
Function:
- plays significant role in water reabsorption in capillaries
- it prevents water loss from circulation
Oncotic pressure (colloid-osmotic
pressure of plasma proteins)

1. are permeable for low molecular weight
substances (e.g. ions)
- ions freely cross the capillary membrane in
both directions (tissue - capillary)
- the osmotic pressure of low-molecular weight
substances in capillaries = 0
- no net changes in water volume
Na+
Cl-
HCO3-
proteins
Na+
Cl-
HCO3-
proteins
tissue blood capillary
2. are impermeable for plasma proteins (macromolecules)
- plasma proteins exert oncotic (colloid-osmotic) pressure on capillary wall
- concentration of proteins in plasma >> concentration of proteins in tissue fluid
- water moves from tissues (interstitial fluid) into capillaries
Blood capillaries
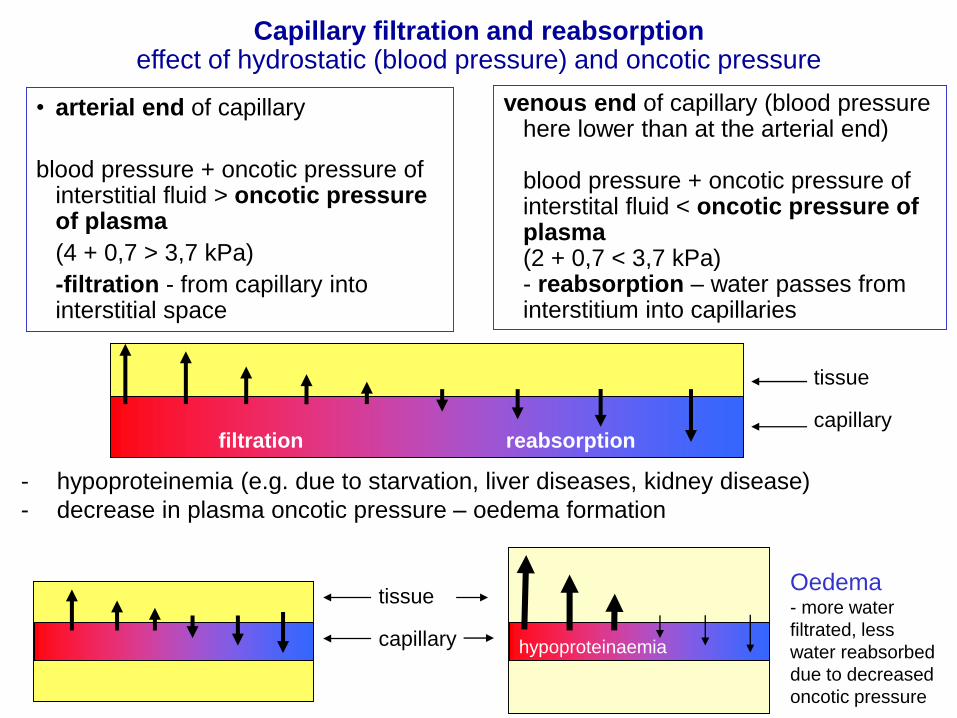
venous end of capillary (blood pressure here lower than at the arterial end)
blood pressure + oncotic pressure of interstital fluid < oncotic pressure of plasma(2 + 0,7 < 3,7 kPa)- reabsorption – water passes from interstitium into capillaries
• arterial end of capillary
blood pressure + oncotic pressure of interstitial fluid > oncotic pressure of plasma
(4 + 0,7 > 3,7 kPa)
-filtration - from capillary into interstitial space
- hypoproteinemia (e.g. due to starvation, liver diseases, kidney disease)
- decrease in plasma oncotic pressure – oedema formation
tissue
capillary
Oedema- more water
filtrated, less
water reabsorbed
due to decreased
oncotic pressure
filtration reabsorption
hypoproteinaemia
tissue
capillary
Capillary filtration and reabsorption effect of hydrostatic (blood pressure) and oncotic pressure
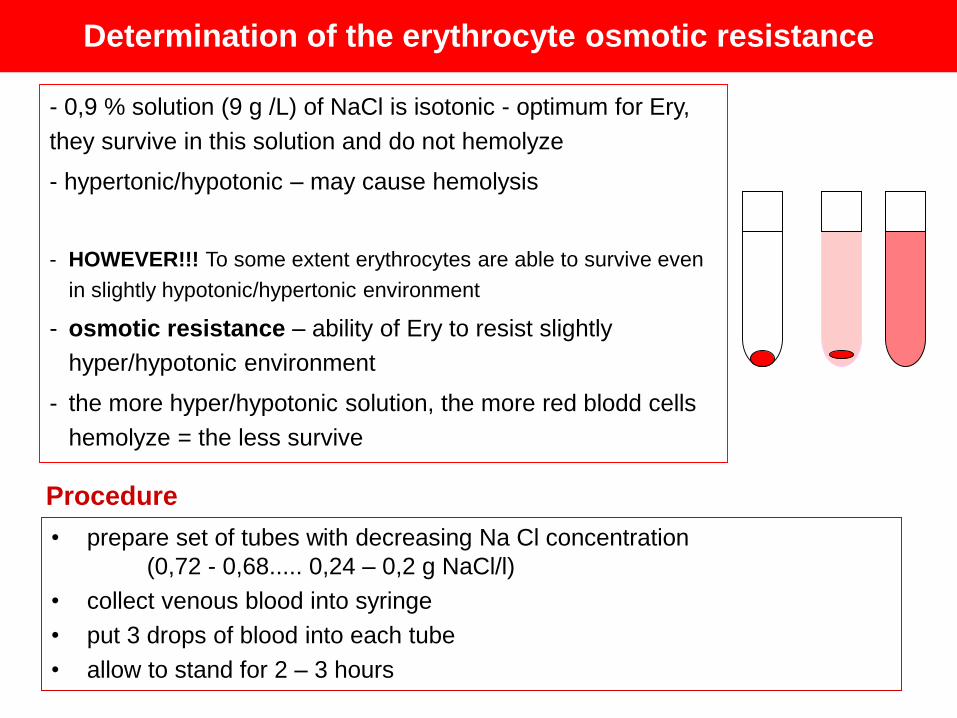
- 0,9 % solution (9 g /L) of NaCl is isotonic - optimum for Ery,
they survive in this solution and do not hemolyze
- hypertonic/hypotonic – may cause hemolysis
- HOWEVER!!! To some extent erythrocytes are able to survive even
in slightly hypotonic/hypertonic environment
- osmotic resistance – ability of Ery to resist slightly
hyper/hypotonic environment
- the more hyper/hypotonic solution, the more red blodd cells
hemolyze = the less survive
• prepare set of tubes with decreasing Na Cl concentration
(0,72 - 0,68..... 0,24 – 0,2 g NaCl/l)
• collect venous blood into syringe
• put 3 drops of blood into each tube
• allow to stand for 2 – 3 hours
Determination of the erythrocyte osmotic resistance
Procedure

Read the results
solution in the tube is clear = no hemolysis
sediment of Er at the bottom of the tube (settle down because they are
heavier than water)
Result 1. Read the minimum osmotic resistance
Start to read the results from the tube with highest NaCl concentration
= Find the first tube with pinkish content and sediment of erythrocytes
Minimum osmotic resistance
= NaCl concentration in which red blood cells begin to hemolyze
the colour of the solution turns pink (indication of hemolysis)
usually in concentration: 0,44-0,4 g .l-1 NaCl
some Er remain unhemolyzed – settle down at the bottom of the tube
Result 2. Read the maximum osmotic resistnace
= find the 1st tube with dark pink content without sediment
Maximum osmotic resistance
NaCl concentration in which all red blood cells hemolyze
the first tube with no sediment at the bottom
(i.e. all erythrocytes are hemolyzed)
normal value 0,34-0,30 g.l-1 NaCl

SPECIFIC GRAVITY (DENSITY)
- in a healthy human – a constant value
blood 1,052 – 1,063 g.cm-3 (ml)
blood elements 1,090 g.cm-3 (ml)
plasma 1,026 – 1,031 g.cm-3 (ml)
depends mainly on:
erythrocyte count
plasma protein concentration
Determination of the blood densityIntroduction
1 ml
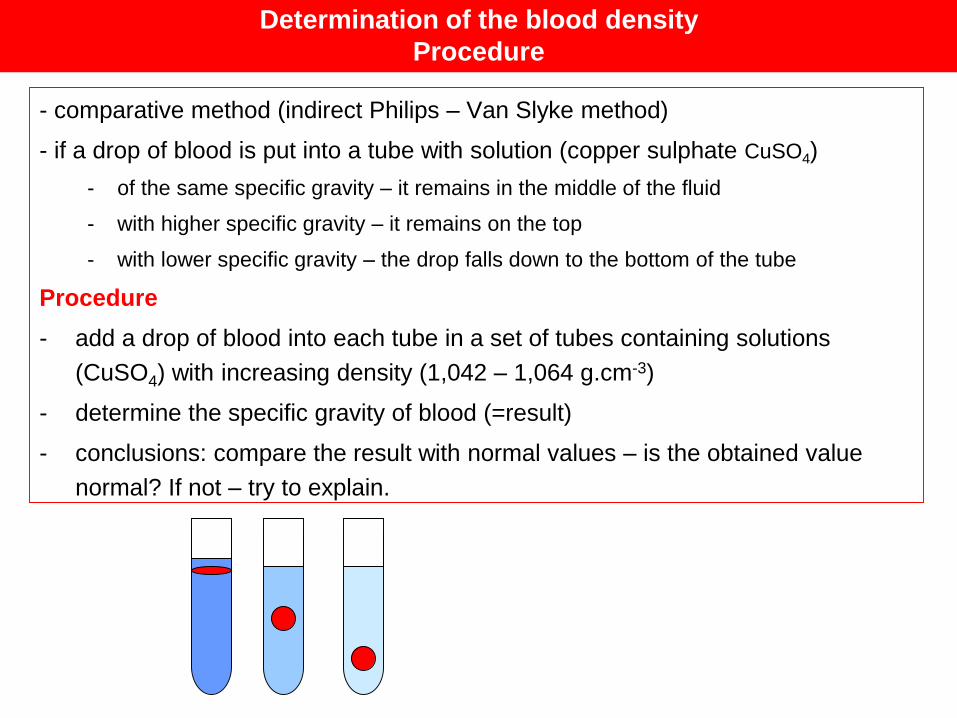
- comparative method (indirect Philips – Van Slyke method)
- if a drop of blood is put into a tube with solution (copper sulphate CuSO4)
- of the same specific gravity – it remains in the middle of the fluid
- with higher specific gravity – it remains on the top
- with lower specific gravity – the drop falls down to the bottom of the tube
Procedure
- add a drop of blood into each tube in a set of tubes containing solutions
(CuSO4) with increasing density (1,042 – 1,064 g.cm-3)
- determine the specific gravity of blood (=result)
- conclusions: compare the result with normal values – is the obtained value
normal? If not – try to explain.
Determination of the blood density
Procedure

Haemostasis – bleeding arrest
- a complex process which makes a bleeding to stop
• maintenance of normal blood volume – vital
• massive bleeding may lead to cardiovascular collapse and death
- haemostasis includes 3 simultaneous interrelated processes
1/ reaction of the injured vessel
2/ activity of the platelets (platelet plug formation)
3/ blood clotting (haemocoagulation)
https://encrypted-tbn1.gstatic.com/images?q=tbn:ANd9GcQb2izwqoBOH84Gwb_-qwRpr_LBr5jnUrLOccz15CtqAtFR43oD9Q

1. Vascular constriction
Effects
- a decrease of the vessel diameter
- diminished blood flow through the ruptured vessel
- a decrease of the blood loss
- contraction of the smooth
muscle in the vessel wall
(circular muscle)
http://images.radiopaedia.org/images/21153/3c503a80bfd516413a65ac8d3aae8d_gallery.jpg

- includes several steps:
A/ Adhesion of platelets
(normal smooth endothelial lining of vessels – repels platelets)
- vessel trauma – damage to endothelium - subendothelial tissue (collagen) has
receptors for platelets – the platelets stick to the vessel wall (to collagen)
2. Formation of the platelet plug
B/ Change of the shape and releasing reaction
▪ thrombocytes swell (become spheric) and form pseudopods
▪ releasing reaction - platelets release substances active in
hemostasis into the blood
C/ Aggregation of platelets
- several layers of platelets stick together
Result: platelet activity results in formation of the platelet plug
- it is sufficient for temporary blocking the blood loss, especially in small vessels
- it does not contain fibrin threads, therefore loose, fragile

- series of enzyme reactions following in definite and rapid sequence
- the reactions involve activation of clotting factors (12 substances)
Result of haemocoagulation:
- formation of fibrin threads - strengthen and stabilize the platelet plug
- net of fibrin threads + platelet plug + trapped blood elements = blood clot
- blood clot - seals the broken vessel until the tissue is repaired
3. Haemocoagulation (blood clotting)

Blood clotting factors
I. fibrinogen
II. prothrombin
III. tissue thromboplastin
IV. Ca2+ ions
V. proaccelerin
VII. proconvertin
VIII. antihemophilic factor
VIII C - antihemophilic globulin
VIII A – von Willebrand factor
IX. Plasma thrombopastin component - Christmas factor
X. Stuart – Prower factor
XI. PTA – Plasma thromboplastin antecedent
XII. Hageman factor
XIII. fibrin stabilising factor
- present in blood
- inactive forms of proteolytic
enzymes (majority)
- blood clotting = a cascade of
chemical reactions leading to
conversion to active forms
..............
- synthesized in liver
- vitamin K – required for
synthesis of factor II, VII, IX, X
F1 F1A
F2 F2A
•HK - High molecular weight kininogen
•PK - Prekallikrein

1. damage of endothelium and
exposure of collagen in the
vessel wall
activates a stepwside (cascade)
activation of clotting factors
referred to as
intrinsic pathway of blood clotting
2. damage of the perivascular
tissue and release of tissue
thromboplastin
activates a stepwside (cascade)
activation of clotting factors
referred to as
extrinsic pathway of blood clotting
Blood clotting - activation
following reactions of both intrinsic
and extrinsic pathway are the same
and they are referred to as
=common pathway
Result of haemocoagulation:
formation of fibrin thread
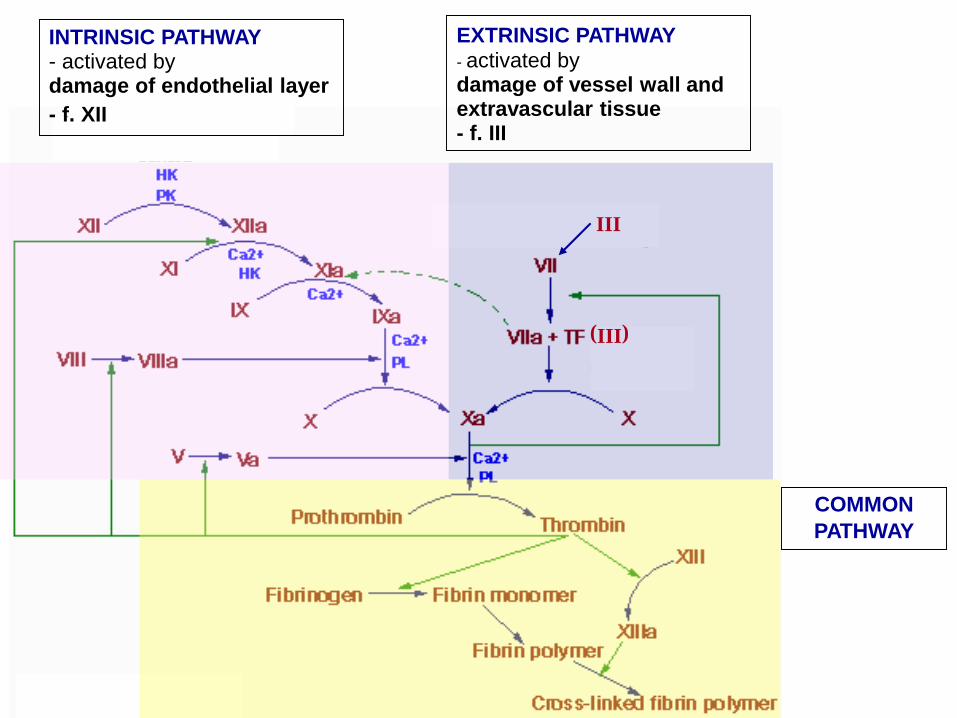
INTRINSIC PATHWAY- activated bydamage of endothelial layer
- f. XII
COMMON
PATHWAY
EXTRINSIC PATHWAY
- activated bydamage of vessel wall and extravascular tissue- f. III
III
(III)

INTRINSIC PATHWAY- activated bydamage of endothelial layer
- f. XII
EXTRINSIC PATHWAY
- activated bydamage of vesel wall and extravascular tissue- f. III
III
(III)
EXTRINSIC PATHWAY
activated bydamage of vesel wall and extravascular tissue
III
(III)
1. fibrin monomer
2. fibrin polymer
3. cross-linked fibrin polymer
4. stabilization of the cross
linked fibrin polymer
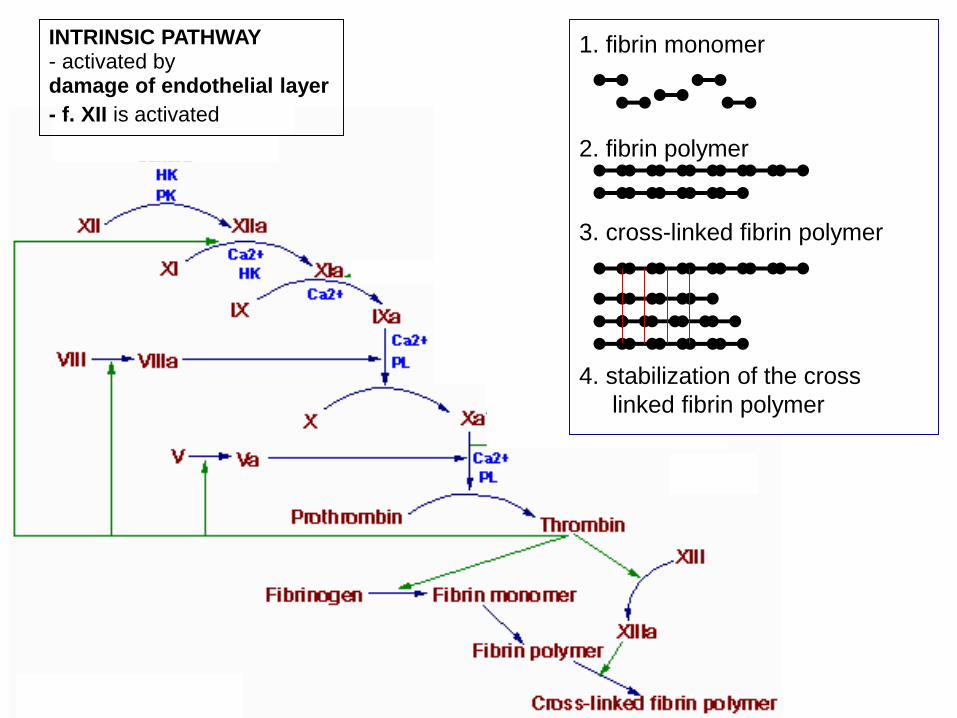
INTRINSIC PATHWAY- activated bydamage of endothelial layer
- f. XII is activated
EXTRINSIC PATHWAY
- activated bydamage of vesel wall and extravascular tissue- f. III
III
(III)
1. fibrin monomer
2. fibrin polymer
3. cross-linked fibrin polymer
4. stabilization of the cross
linked fibrin polymer
In bleeding mostly both pathways are activated
Extrinsic pathway - fast (seconds), is first activated
= initiation phase the hemocoagulation
- causes formation of minute amounts of thrombin
- amplification phase
- thrombin activates factor V, VIII, IX
- propagation phase reactions of intrinsic pathway take
place
- Intrinsic pathway – delayed activation/proceeds slower
New fundamentals in haemocoagulation

Blood clot
▪ network of fibrin threads running in all directions -
adhere to damaged surfaces of vessels
▪ contains trapped blood elements
Retraction of the clot
- occurs 20 - 60 minutes after formation of the clot
- caused by the contraction of thrombocytes
(contain contractile fibres – actin, myosin)
- liquid (serum) is extruded from the clot
- wound surfaces are drawn together, tissue repair is
promoted
clot
clot
serum
IN VIVO – Intravascular anticoagulants
- endothelial factors- that prevent blood coagulation and platelet plug formation
- endothelial layer – non-wettable surface
- glycocalyx - layer of mucopolysaccharides on the surface of endothelium
- repels clotting factors and thrombocytes
- thrombomodulin – protein bound to endothelial cells, binds thrombin
- blood flow – homogenously dispels clotting factors, prevents their local
concentration
- anticoagulant substances
- antithrombin III – binds thrombin, inactivates clotting factors
- heparin – produced in basophils and mast cells
- a weak anti-clotting agent
- its anticoagulant effect increases in complex with antithrombin III
(100 – 1000 x) – inactivates thrombin and f. XII, XI, IX, X
- heparin and its derivatives - used for anticoagulant therapy
- fibrin – adsorbs thrombin, prevents further conversion of fibrinogen to fibrin
Anticoagulants – substances that prevent blood clotting

Anticoagulants for clinical use
▪ tubes from special „non-wettable“ materials (silicone)
▪ non-wettable surface = a surface that does not start the blood clotting
▪ decalcification – binding of Ca2+ ions - oxalate, citrate
▪ defibrination – removal of fibrin (e.g. snake toxins)
▪ coumarin derivates (e.g. warfarin)
- block the effect of vitamin K in liver (long-term effect)
- production of vitamin K dependent factors is affected – lack of Ca2+
receptor in their molecule
- are used also as medicaments in anticoagulation therapy
- effective within 12 hours
▪ heparin

Determination of bleeding time by the Duke method
• Test of platelet function and/or vascular function

Procedure
- disinfect the tip of the 4th finger and puncture it
- at the moment of puncturing turn on the stop watch
- wipe off the first drop
- suck off the blood with a strip of filter paper every 30 seconds
- stop the watch when you cannot see any more blood on the filter paper
- normal value 2-5 minutes
Report
A. Write down the time
B. Is the time within the interval of normal values?
0 30´´ 60´´ 90´´ 120´´ 150´´

Blood coagulation time determination
by the Lee – White method
• test of the intrinsic pathway of blood coagulation
• glass tube
– wettable surface = mimics the effect of collagen (starts the intrinsic
pathway of blood clotting)
• in clinical settings Activated Partial Thromboplastin Time (APTT) is
used to test the intrinsic pathway
Procedure
- collect venous blood – 3 ml
- place the last 1 ml of blood into a tube
- by using the last 1 ml the tissue factor III is eliminated (in this way it
remains in the bottom of the tube – i.e. the intrinsic pathway will not
get activated)
- turn on the stop watch
- check every 30 - 60 sec if the blood has coaglulated or not
- stop the watch when the blood is clotted
- normal value 4 -10 minutes (in 37° C), in a room temperature
up to 15 minutes)
Report
A. Write down the time.
B. Is the value normal? Compare measured results with standards
tissue
factor
Determination of prothrombin time by Quick
• test of the extrinsic pathway of blood clotting
• tissue thromboplastin (togehter with Ca ions) is added to blood serum
• tissue thromboplastin activates the extrinsic pathway of
haemocoagulation
• in clinical settings the PT (prothrombin time) test or international
normalized ratio (INR) is used to test the extrinsic pathway

Procedure
• collect a sample of venous blood – 0,3 ml citrate + 2,7 ml blood
• put the blood into a tube, centrifuge
• put the tube with plasma into the water bath (37º C)
• keep other reagents in water bath
• put into a clean tube
– 0,1 ml of plasma
– 0,2 ml of thromboplastin + CaCl
• immediately turn on the stop watch
• with a glass hook try to pick fibrin clots
• when you find fibrin clot stop the watch
• normal time 11 – 16 sec
Report:
A. Describe your observation of fibrin clot formation.
B. Write down the result
C. Compare your result to standard values - evaluate if the time is normal
Questions to study
• Haemostasis – 3 main processes and their end-results
• Haemocoagulation – extrinsic and intrinsic pathway, common pathway
• Events that activate the intrinsic/extrinsic pathway, sequence of activation of
the factors
• Haemocoagulation factors and their general description and function, the
role of vitamin K in haemocoagulation
• Tests used for assessment of intrinsic and extrinsic pathways
• Platelets – normal count, activity in haemostasis, event that activates the
platelets
• Haemopoiesis – definition, site, characteristics, stem cells, lineages
• Main nutritional factors of haemopoiesis.
• Stimuli for erythropoiesis (erythropoietin, stimuli for its synthesis and
secretion)
• Plasma components and their functions.
• Plasma osmotic and oncotic pressure and their clinical implications.
• Hypoalbuminemia, decreased oncotic pressure and edemas.