preview only · 2013-05-16 · preview only these notes are a preview. slides are limited. full...
TRANSCRIPT
16/05/2013
1
Be sure to convert to your own time zone at www.worldhealthwebinars.com.au
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Need technical support for this live event?
Please call 1800 006 293, then press 1
NOTE: You will be initially asked for the email address associated with this webinar account – “Say I’m a webinar attendee – I don’t have an account”
Be sure to convert to your own time zone at www.worldhealthwebinars.com.au
Low Back Pain Triage: Identification of Serious Spinal Pathology
Presented by: Dr Debra Shirley FACP PhD BSc
Specialist Musculoskeletal Physiotherapist
Will commence LIVE from Sydney, Australia at 7:30pm AEST
Andrew Ellis BSc (Ex. Sci), M. Phty
World Health Webinars CEO
World Health Webinars (Australia/NZ) Host
Need technical support?
Please call 1800 006 293, then press 1
You will need to tell them that you are a webinar attendee and do not have an email account with Citrix.
Click red button to minimise
You will be muted
during every webinar.
Make as much noise
as you like :)
Dodgy computer
speakers? Select
Telephone and call in
toll - FREE to hear the
presentation
Questions? We’ll
answer them all at
the end
Dr Debra Shirley
• Specialist Musculoskeletal Physiotherapist and Fellow of the
Australian College of Physiotherapy.
• Senior Lecturer in Musculoskeletal Physiotherapy
• Director of Social Inclusion at the Faculty of Health Sciences at the
University of Sydney.
• Extensive experience in teaching musculoskeletal physiotherapy at
entry level and post graduate Masters in Manipulative
Physiotherapy.
• Presented on international manipulative physiotherapy courses at
the University of Birmingham and the DVMT in Germany.
• Debra is a co author of the APA Clinical Guidelines for Assessing
Vertebrobasilar Insufficiency in the Management of Cervical Spine
Disorders (2006).
• Member the NSW Physiotherapy Council and previously served
as Deputy President of The NSW Physiotherapists Registration
Board and as a Director of the Australian Physiotherapy Council.
Specialist Musculoskeletal Physiotherapist

16/05/2013
2
Low Back Pain Triage:
Identification of serious spinal pathology
Learning Outcomes
1. Describe a selection of specific/serious pathology affecting the lumbar spine that need to be differentiated from non-specific low back pain.
2. Identify the information (red flags) from the history and physical examination that might signal the risk of a specific/serious pathology.
3. Evaluate the diagnostic utility of red flags and discuss how this influences clinical reasoning.
4. Discuss when it is necessary to refer a patient for further medical evaluation.
Where is my pain coming from?
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Diagnostic Triage for LBP
Idiopathic = non-specific Spinal nerve/nerve root compromise
Acute Chronic
Syndrome Idiopathic / NSLBP
~90%
The Back Pain Revolution, G. Waddell (2004)
Diagnostic Triage for LBP
<1%
Benign (e.g. OA) Serious
serious (red flags) eg tumour, cauda equina, fracture, myelopathy, infection
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Serious Pathologies
Fracture
Cancer
Infection
Inflammatory conditions
– eg ankylosing spondylitis
Cauda equina syndromes
Myelopathy

16/05/2013
3
Red flags for possible serious spinal pathology
Consider prompt referral (less than 4 weeks)
Presentation under age 20 or onset over 55
Non-mechanical pain
Thoracic pain
Past history - carcinoma, steroids, HIV
Unwell, weight loss
Widespread neurological symptoms or signs
Structural deformity
(Waddell 2001 RCGP acute LBP guidelines )
Cauda Equina syndrome
Immediate referral
Sphincter disturbance
Gait disturbance
Saddle anaesthesia
Waddell 2001 RCGP acute LBP guidelines
Red flags for Serious Pathology
<20, >50 yrs
trauma / unwell / RUWL / +’ve investigations
Structural deformity
History of Ca, steroids, drug abuse, HIV
Constant
Non mechanical pain
S&S inflammatory disorders
family history of inflammatory disorders
Need to use clinical reasoning and investigate further if concerned
Waddell (2004): p 12
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Age and Red Flags
Older age: Pre-test probability of a GP patient with back pain having cancer -
<50years - 0.14%
>50years - 0.56%
Back pain in young person < 20, potential red flag conditions (cancer, inflammatory back disease, stress fracture)
Dr J Bleasel 2005
Red Flags
Significant weight loss
Fevers
IV drug use
Constant pain, nocturnal pain
Pre existing Carcinoma
Additional symptoms in other systems
Neurological impairment
Severe, highly localised pain
Red Flags
Appear throughout the history but we actively search
for them in the SPECIAL / SPECIFIC QUESTIONS
Purpose;
To alert the PT to possible serious pathology
Alert PT to precautions or contraindications to treatment
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
16/05/2013
4
Special Questions (all conditions)
General health
PH Cancer
Unexplained weight loss
Recent X-rays or investigations
Medications
Oral steroids (osteoporosis)
Other Joints
Special Questions
Lumbar spine
Cord signs
• Bilateral non-dermatomal Sx and ataxia
Cauda Equina syndrome
• Changed bowel or bladder function, saddle anesthesia
Cervical spine
Dizziness (vertibrobasilar insufficiency)
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Debate: “To Screen or Not to Screen?” Ross 2010
Challenge: Identify which red flags are representative of specific pathological conditions Ross 2010
Eg night pain
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Specific pathology/Serious Spinal Pathology
Henschke et al 2008
• Many suggested but none with good sens and spec in isolation and poorly investigated
• >80% prevalence of one red flag
• 11/1172 (serious pathologies, 8 fractures)
• 6/11 identified by clinician
BUT
• Mean age for sample population was 44
Conclusion
• Most patients at least 1 red flag finding
• Individually red flags uninformative
Debate: “Time to Lower the Red Flags?” Underwood 2009
Clinicians should consider a small number of disorders
CE syndrome
Major IA pathology
Focal infections
Fractures
Time as a diagnostic tool for the remainder
Concern screening will lead to increased costs from investigations
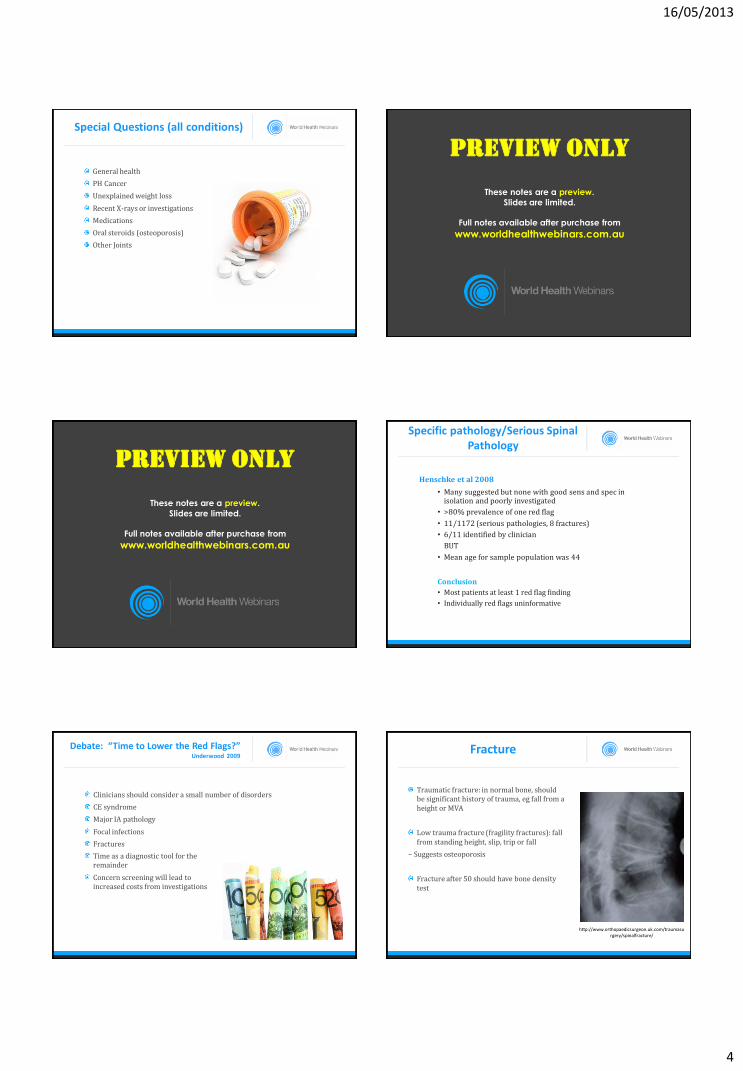
Fracture
Traumatic fracture: in normal bone, should be significant history of trauma, eg fall from a height or MVA
Low trauma fracture (fragility fractures): fall from standing height, slip, trip or fall
– Suggests osteoporosis
Fracture after 50 should have bone density test
http://www.orthopaedicsurgeon.uk.com/traumasurgery/spinalfracture/

16/05/2013
5
Osteoporosis
Decrease density of bone, increase risk of fracture
Risk factors
− Female, post- menopausal
− Increasing age male and female
− Family history
− Medical conditions eg liver, kidney disease, RA, thyroid/parathyroid disease
− Drugs: steroids, alcohol
http://imaging.consult.com/image/chapter/Interventional?title=Vertebral%20Height%20Restoration&image=fig1&locato
r=gr1a&pii=S1933-0332%2808%2973352-4
Vertebral Fractures
Incidence x 3 hip fractures
1 in 3 will come to medical attention
Female : Male 2:1
In Europe, one in eight men and women over the age 50 years have evidence of vertebral deformity (EVOS)
3 fold variation across Europe and up to 2 fold variation within individual countries (EVOS)
White women = Asians > African-American and Hispanic
Woolf Fragility Fractures 2011
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Prevalence of vertebral deformity
In Europe for Age and Gender
Woolf Fragility Fractures 2011
Increased Risk of Second Fracture
Prevalent vertebral fracture and new vertebral fracture in next year (Lindsay et al JAMA 2001)
1 prevalent fracture RR 2.6
≥1 RR 5.1
≥2 RR 7.3
Woolf Fragility Fractures 2011
Woolf Fragility Fractures 2011
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Diagnosis of Osteoporotic Fracture
Xray
Bone scan: will differentiate old vs new fractures
Bone densitometry:
– measure of bone density at hip and lumbar spine
– Does not diagnose fracture
http://www.ajnr.org/cgi/content/full/21/10/1807/F1
16/05/2013
6
Osteoporosis risk factors
Area of pain
Family history
Weight loss
Family history of op or hip fracture
Early menopause hormone deficiencies etc
Establish amount of height loss since age 25 (+ tsp pain)
Any fractures since age 45-50
Bleicher K, Naganathan V, Cumming RG, Seibel MJ, Sambrook PN, Blyth FM, et al. Prevalence and treatment of osteoporosis in older Australian men: Findings from the CHAMP study. Med J Aust. 2010;In press ; accepted for publication 01/07/2010
Likelihood Ratio
+LR sensitivity/1-specificity
-LR 1-sensitivity/specificity
Eg for Ca previous Hx Ca sens 0.31 sp 0.98
+LR 0.31/1-0.98 = 0.31/0.02 = 15.5
-LR 1-0.31/0.98 = 0.69/0.98 = 0.70
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Screening for spinal fracture
Henschke et al 2008
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
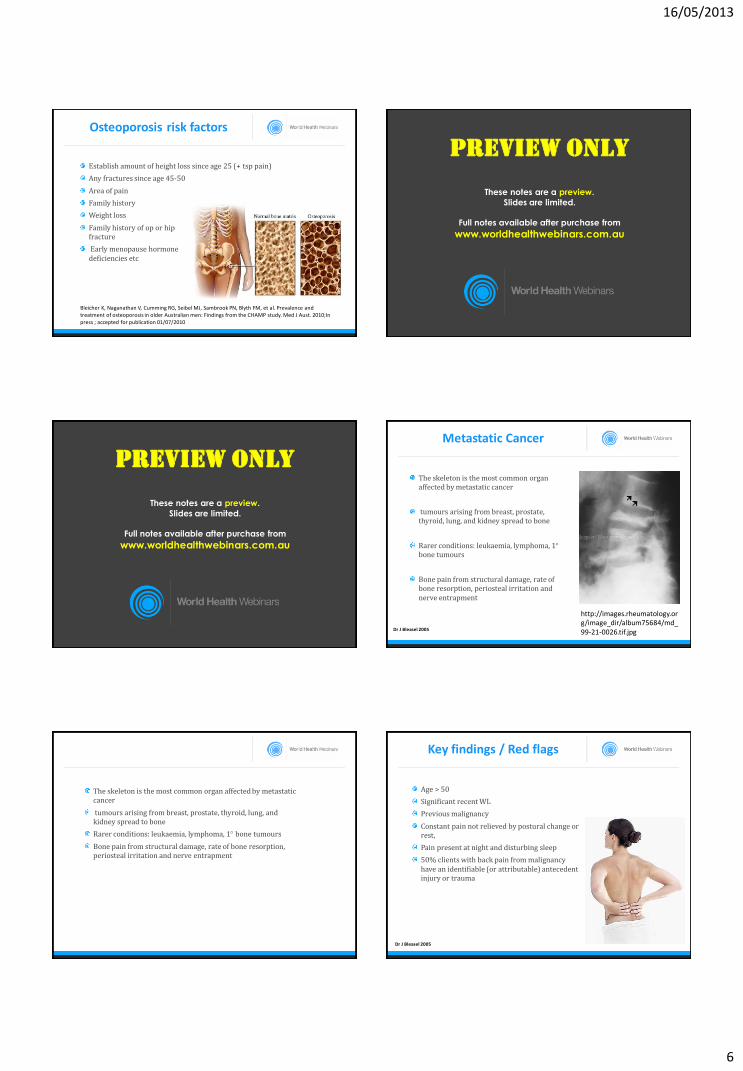
Metastatic Cancer
http://images.rheumatology.org/image_dir/album75684/md_99-21-0026.tif.jpg
The skeleton is the most common organ affected by metastatic cancer
tumours arising from breast, prostate, thyroid, lung, and kidney spread to bone
Rarer conditions: leukaemia, lymphoma, 1 bone tumours
Bone pain from structural damage, rate of bone resorption, periosteal irritation and nerve entrapment
Dr J Bleasel 2005
The skeleton is the most common organ affected by metastatic cancer
tumours arising from breast, prostate, thyroid, lung, and kidney spread to bone
Rarer conditions: leukaemia, lymphoma, 1 bone tumours
Bone pain from structural damage, rate of bone resorption, periosteal irritation and nerve entrapment
Key findings / Red flags
Age > 50
Significant recent WL
Previous malignancy
Constant pain not relieved by postural change or rest,
Pain present at night and disturbing sleep
50% clients with back pain from malignancy have an identifiable (or attributable) antecedent injury or trauma
Dr J Bleasel 2005

16/05/2013
7
Screening for Malignancy
Henschke et al 2007 Eur Spine J (2007) 16:1673–1679
Screening for malignancy
Henschke et al 2007 Eur Spine J (2007) 16:1673–1679
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Case 45 year old male
Quality control manager
Aggs: lying supine, coughing and sneezing, prolonged walking, and sitting >1 hour
Ease: heat, Ibuprofen
PM: pain, difficulty sleeping
CH: 2/12 no incident, p&n 1/52
PH: L LBP no limitation
GH , CE , Nil other SQ
Ross MD. J Orthop Sports Phys Ther. 35(10): 651-58. 2005
Case 45 year old male
PE
Slight antalgic gait
Ext and LLF sl back and thigh
Neuro L2 and L3 strength, Reflexes
L SLR 45 thigh pain
Ross MD. J Orthop Sports Phys Ther. 35(10): 651-58. 2005
Ross MD. J Orthop Sports Phys Ther. 35(10): 651-58. 2005
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
FIGURE 3. Anterior-posterior radiograph of the lumbar spine demonstrating mottled lucencies overlying the left sacroiliac wing
(oriented to the right in this image).
Ross MD. J Orthop Sports Phys Ther. 35(10): 651-58. 2005
16/05/2013
8
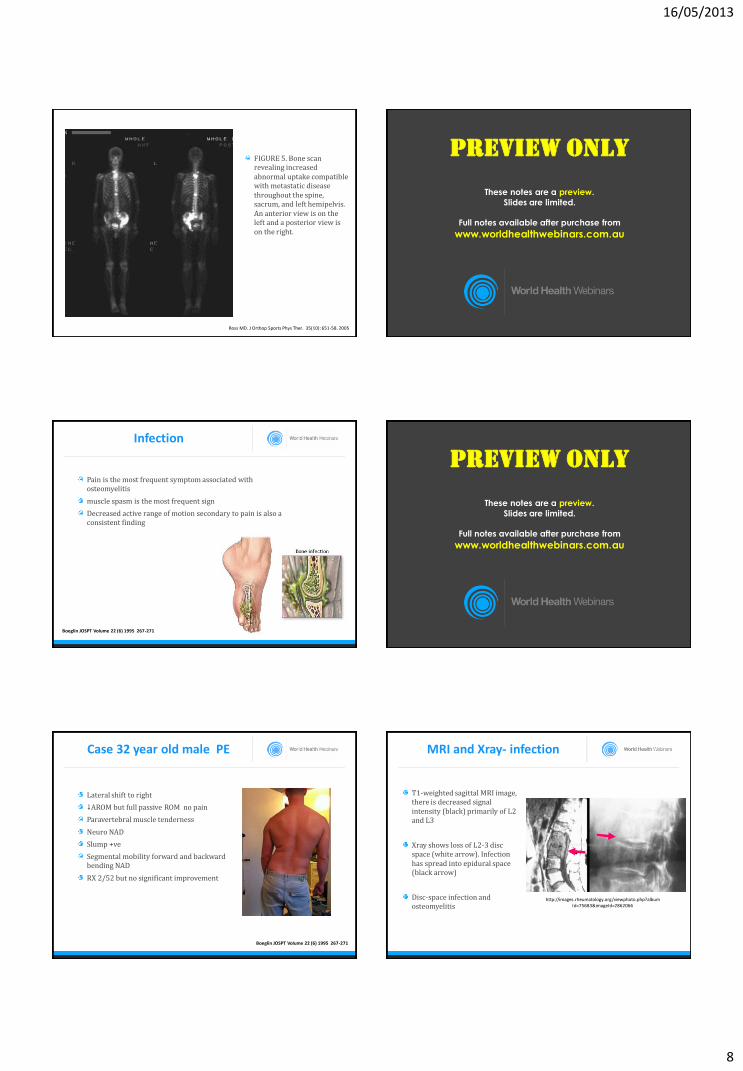
FIGURE 5. Bone scan revealing increased abnormal uptake compatible with metastatic disease throughout the spine, sacrum, and left hemipelvis. An anterior view is on the left and a posterior view is on the right.
Ross MD. J Orthop Sports Phys Ther. 35(10): 651-58. 2005
Infection
Osteomyelitis of the spine is rare (2-4% osteomyelitis)
Mortality 1 to 20%
Vertebral osteomyelitis children, ages 1-15, adults 50-70
Usually two vertebrae and a disc are involved
The lumbar spine has of osteomyelitis with the thoracic and cervical regions being affected to a lesser extent.
The most common area for spinal osteomyelitis is in the vertebral body
The primary etiology of contamination is from distant infections, often emanating from the respiratory or urinary tract
Boeglin JOSPT Volume 22 (6) 1995 267-271
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Pain is the most frequent symptom associated with osteomyelitis
muscle spasm is the most frequent sign
Decreased active range of motion secondary to pain is also a consistent finding
Infection
Boeglin JOSPT Volume 22 (6) 1995 267-271
Case 32 Year old male
CH Insidious LBP for 2/52 ??due to prolonged sitting
ED Pain meds home GP toradol pain
PH 10 years LB and leg pain
Boeglin JOSPT Volume 22 (6) 1995 267-271
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Case 32 year old male PE
Lateral shift to right
AROM but full passive ROM no pain
Paravertebral muscle tenderness
Neuro NAD
Slump +ve
Segmental mobility forward and backward bending NAD
RX 2/52 but no significant improvement
Boeglin JOSPT Volume 22 (6) 1995 267-271
MRI and Xray- infection
T1-weighted sagittal MRI image, there is decreased signal intensity (black) primarily of L2 and L3
Xray shows loss of L2-3 disc space (white arrow). Infection has spread into epidural space (black arrow)
Disc-space infection and osteomyelitis
http://images.rheumatology.org/viewphoto.php?albumId=75683&imageId=2862066

16/05/2013
9
Infection as a cause of Back Pain
Suspected primarily on history
Cardinal feature is fever
Other important risk factors
– Previous infection eg UTI
– IVDU
– Skin lesions
– IV catheters and urinary catheters
– Occupational exposure
Dr J Bleasel 2005
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Lumbar Osteomyelitis
Commonest organism (60% of cases) Staphylococcus aureus
Gram negative organisms in elderly and from IVDU
Workers in the meat processing industry - Brucellosis infection
Tuberculous and fungal infections
Elderly
Immunocompromised individuals
May be present for years before diagnosis
http://radiopaedia.org/images/25251
Dr J Bleasel 2005
Sepsis in other sites
Disciitis- localised pain in back
Sacroiliac joint- Pain in low back, buttock
Any septic patient- red flags
– Fever, sweats, night pain
– IVDU, skin lesions
– invasive procedures (IV lines, Urinary catheters
– Recent infection
http://emedicine.medscape.com/article/340211-overview Dr J Bleasel 2005
Septic Sacroiliitis
Right sacroiliac joint-
Increased sclerosis,
joint space widening,
irregular joint margin
left sacroiliac joint is normal.
Joint aspiration:
Staph aureus
Symptoms include acute onset severe right lower back pain associated with high fever.
http://imaging.consult.com/imageSearch?query=joints&qyType=AND&global_search=Search&modality=&thes=true&normalVariantImage=false&groupByNode=none&anatomicRegion=&modalityFilter=Conventional%20Radiography
Dr J Bleasel 2005
Seronegative Spondyloarthropathies
Inflammatory arthropathies
– Axial skeleton
– Sacroiliac joints
– +/- Peripheral joints
Prominent enthesopathy (inflammation at insertion of tendon or ligament)
Extra-articular manifestations eg. skin and gut
http://www.aafp.org/afp/2004/0615/p2853.html Dr J Bleasel 2005
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Disease
Ankylosing spondylitis
Psoriatic arthritis
Reactive arthritis (Reiters Disease)
Ulcerative Colitis, Crohns disease: inflammatory bowel disease may have associatedc Arthritis
Juvenile ankylosing spondylitis
http://homepages.which.net/~ks.burrell/nassdb/Spinal%20xray.htm
16/05/2013
10
AS Incidence and Prevalence
0.5-2.0% prevalence
– Higher in selected ethnic groups
5:1 male:female ratio
Incidence 6-7 cases per 100,000 per year
Natural history
– Progression towards ankylosis - may be over many decades, some cases asymptomatic - found on x-rays
Dr J Bleasel 2005
Red flags Inflammatory disease
Onset before age 40
Insidious onset
Morning stiffness lasting >30 mins
Persisting beyond 3 months
Not responsive to conservative treatment
Peripheral joint involvement
In combination are suggestive of sero negative arthridities
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Ankylosing Spondylitis
Medical History Sensitivity Specificity LR+ LR-
Ankylosing Spondylitis
4 out of 5 0.23 0.82 1.28 0.94
Onset <40 1 0.07 1.08 0
Pain not relieved supine 0.8 0.49 1.57 0.41
Morning stiffness 0.64 0.59 1.56 0.61
Pain duration >3/12 0.71 0.54 1.54 0.54
Case 32 year old female
Commercial Pilot
10/12 LBP L buttock and thigh
GP after 2/12 LB strain
Sev month later worse MRI L4/5 degen disc
Agg “twisting”, lying down to sitting and sit to standing, walking for exercise, and coughing or sneezing,
Ease changing positions and gentle exercise, but not with prolonged rest.
AM pain few mins moving eases
Day with increasing levels of activity, not as active as usual.
GH NAD meds
Seif and Elliott Physiotherapy Theory and Practice, 28(1):2012, 63–70
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
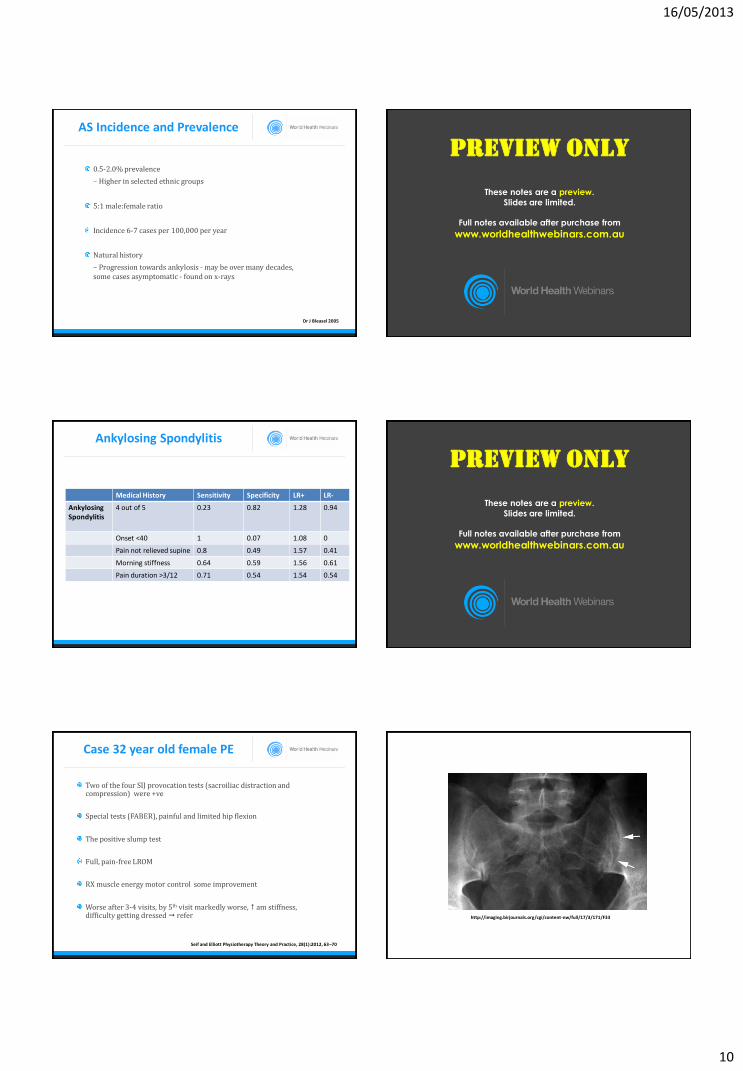
Case 32 year old female PE
Two of the four SIJ provocation tests (sacroiliac distraction and compression) were +ve
Special tests (FABER), painful and limited hip flexion
The positive slump test
Full, pain-free LROM
RX muscle energy motor control some improvement
Worse after 3-4 visits, by 5th visit markedly worse, am stiffness, difficulty getting dressed refer
Seif and Elliott Physiotherapy Theory and Practice, 28(1):2012, 63–70
http://imaging.birjournals.org/cgi/content-nw/full/17/3/171/F33
16/05/2013
11
Seif and Elliott Physiotherapy Theory and Practice, 28(1):2012, 63–70
Radiology
Sacroiliitis
– Erosions
– Subchondral sclerosis
– Ankylosis
Spine
– Anterior erosions
– Squaring
– Syndesmophytes- anterior border to anterior border
– Fusion- Bamboo spine
http://homepages.which.net/~ks.burrell/nassdb/Spinal%20xray.htm
Dr J Bleasel 2005
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Syndesmophytes
http://www.nature.com/nrrheum/journal/v8/n1/full/nrrheum.2011.183.html
http://wiki.cns.org/wiki/index.php/Ankylosing_spondylitis
http://www.radrounds.com/photo/1791588:Photo:9383?context=top
KATARIA et al Am Fam Physician. 2004 Jun 15;69(12):2853-2860
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
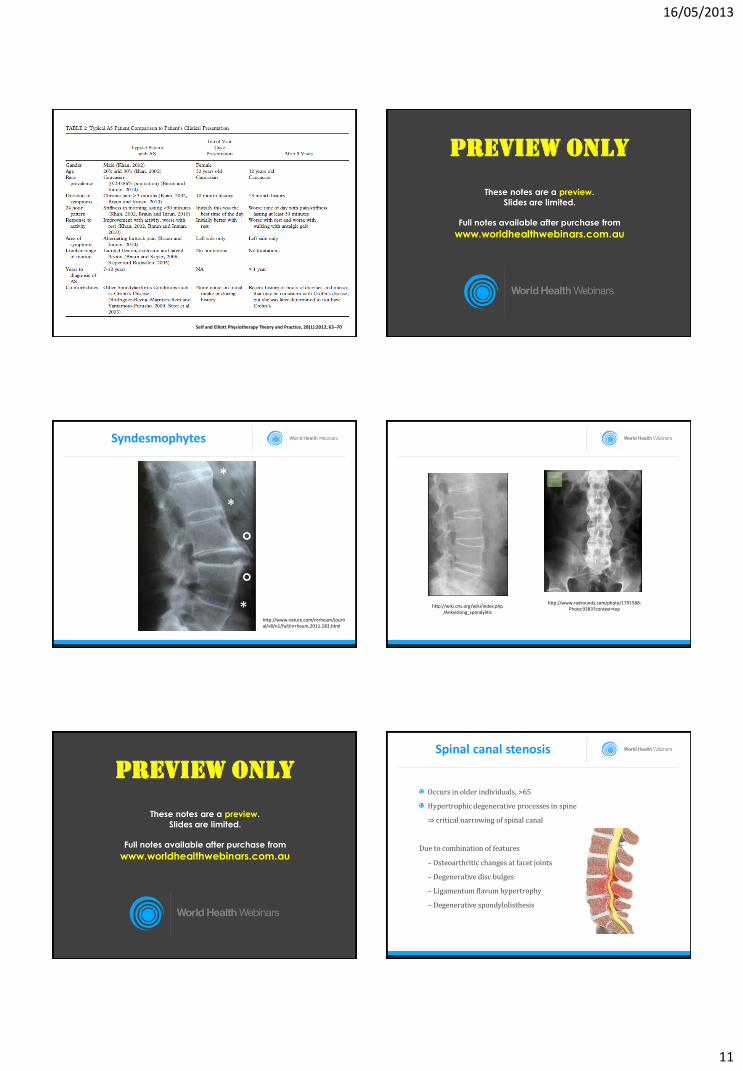
Spinal canal stenosis
Occurs in older individuals, >65
Hypertrophic degenerative processes in spine
⇒ critical narrowing of spinal canal
Due to combination of features
– Osteoarthritic changes at facet joints
– Degenerative disc bulges
– Ligamentum flavum hypertrophy
– Degenerative spondylolisthesis

16/05/2013
12
Clinical Presentation
?? Burning pain (neurogenic)
No change to pulse
No trophic changes
symptoms with spinal Ext
symptoms with spinal Fl
symptoms standing
Symptoms may respond to rest
Vascular claudication
Throbbing pain
Diminished or absent pulses
Trophic changes
Pain not related to spinal positions
No pain on standing
symptoms with activity, promptly relieved by rest or cessation of activity
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Red Flags in a child with back pain
Progressive pain not responding to analgesia Pain that awakes the child at night Fever Weight loss Severe constipation Adoption of abnormal postures Development of scoliosis Reduction in mobility & abnormalities of gait Sphincter dysfunction
Dr J Bleasel 2005
Spine injury in young athletes
Lumbar spine # less common than c spine
Compression fractures most common
Disc herniation (associated with fracture of the ring apophyses)
Spondylolysis (47% of adolescents with back pain), 85-95% L5
Maxfield. Radiol Clin N Am 48 (2010) 1237–1248
Spondylolysis in children with LBP
Presents as LBP
Agg by activity
Minimal physical findings
Misdiagnosis common
Up to 45% of LBP in athletic adolescents
Early diagnosis important to prevent progression
Plain xrays not always helpful
Treatment with activity restriction
Ralston and Weir 1998
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Summary

16/05/2013
13
Red Flags requiring evaluation
Back pain or symptoms not improving
Steady pain irrespective of activity
Symptoms increasing
Development of new or progressive neurological deficits
Identifying Serious pathology
Sound Clinical reasoning
Knowledge of red flags
May not be apparent on first visit
Monitor progress
Develop expectation from treatment ie expected outcome and timeframe
Reassessment really important
Clinical Judgment shouldn’t be underestimateed
http://gal3.piclab.us/key/lower%20back%20pain%20cartoons
PREVIEW ONLY
These notes are a preview.
Slides are limited.
Full notes available after purchase from
www.worldhealthwebinars.com.au
Live Q & A With Debra Shirley
Join US on Facebook
Coming up next week
Live Q & A With Debra Shirley

16/05/2013
14
Thank you
From Debra Shirley
&
World Health Webinars Australia / NZ
http://worldhealthwebinars.com.au