preventing sudden cardiac death in youth sports · 2019-07-15 · preventing sudden cardiac death...
TRANSCRIPT

Preventing Sudden Cardiac Death in Youth Sports
Victoria L. Vetter, M.D., MPH
Professor of Pediatrics
Perelman School of Medicine at the University of Pennsylvania
Division of Cardiology, The Children’s Hospital of Philadelphia

Sudden Cardiac Arrest (SCA) is a condition in which the heartbeat
stops suddenly and unexpectedly. It is the immediate loss of
electrical heart function. This usually is caused by ventricular
fibrillation (VF), an abnormality in the heart's electrical system
which causes the heart to quiver and blood flow to the body and
brain to stop.
Sudden Cardiac Death (SCD) occurs if emergency treatment with
CPR/AED or spontaneous recovery does not occur.

Scope of the Problem
SCA is the leading cause of death in young athletes – accounting for 75% of all deaths.
Maron; Circulation 2006


Who is At Risk?
2010-2011 High School Sports Participants
7,667,955
60 % of HS Students
Females 3,173,549 41%
Males 4,494,406 59%
Athlete: A participant in a sport, exercise, or game requiring physical skill. Dictionary.com
>30 million US children not on school sports teams
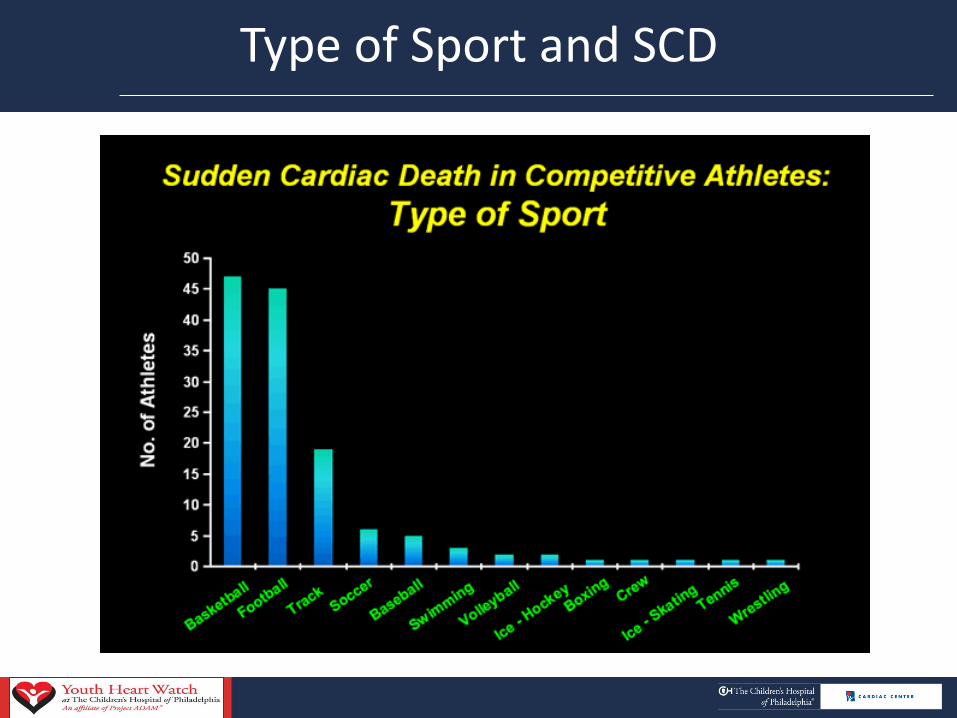
Type of Sport and SCD

Epidemiology of SCD in Children
• Incidence: 3-6/100,000 per-yrs
~1,000 deaths/yr in USA
• Greatest in 10-19 yr age group
• Male: Female 4:1
• Two-thirds occur with exercise
or activity
• Estimated 1:9000 (Military 18-
35 yrs) to 1:27,000 (Atkins) to
1:200,000 (Maron)
4.4
6.37
0.6
4.9
13
2.7
6.2
2.8
0 5 10 15
Drezner
Atkins
Maron
Liberthson
Eckart
Corrado
Shen
Winkel
Only % of cases found in media reports

Death Rates 2005-2007: 5-17 yrs/100,000
SCD 3-6/100,000 person-years

High School/College Basketball Players

Etiology of Sudden Cardiac Death in Children
• Cardiomyopathy
HCM, ARVC , DCM, LVNC
• Primary Electrical Disease
LQTS, SQTS, Brugada
CPVT, Primary VF
WPW
• Congenital Heart Disease
– AF, VT/VF, SSS, CHB
• Coronary Artery Anomalies
• Acquired Heart Disease
Myocarditis
Drugs
Marfan Syndrome
Commotio Cordis/Blow to chest
HCM
43%
LQT/Electrical
Disease
15%
Marfan
5%
WPW
2%
CHD
8%
ARVD/CM
5%
Cor Art
12%
Myocarditis
5%
Commotio
Cordis
5%
Parent Heart Watch Database 2007
Prevalence: 1:500- 1:3000

What We Don’t Know about SCA in the Young
• We don’t know how often these conditions result in death.
• We don’t know how prevalent the SCA high risk conditions are in the young.
• So…are we just looking at the tip of the iceberg with our current information?
There is no required reporting or Registry for SCA/SCD in the US
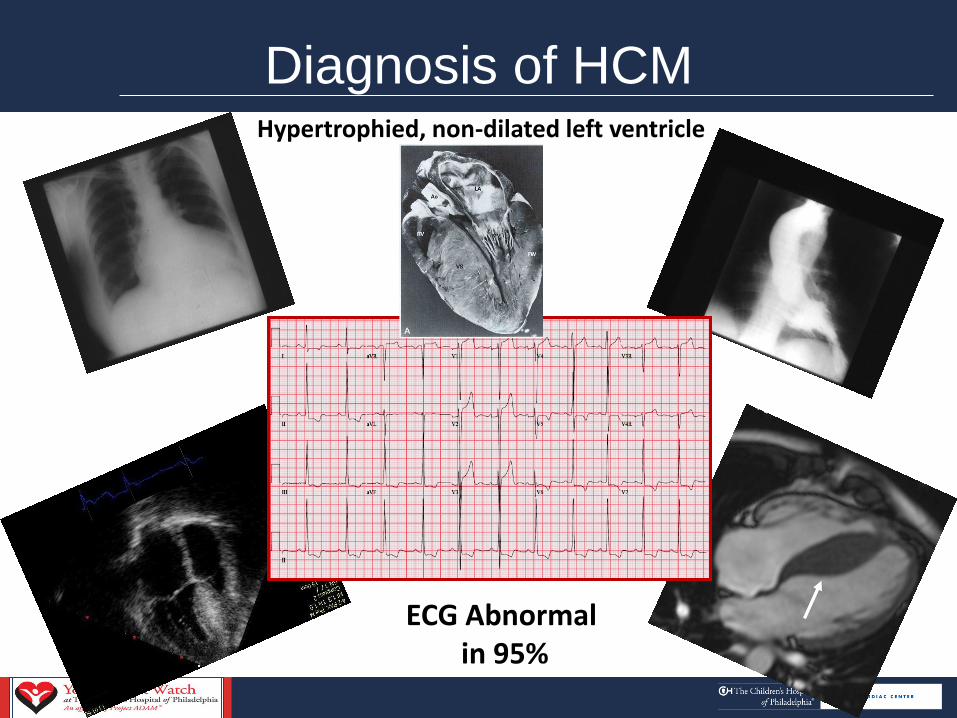
ECG Abnormal in 95%
Diagnosis of HCM Hypertrophied, non-dilated left ventricle

Long QT Syndrome Characteristics
• Prolonged QT Interval
• Syncope/Fainting
• Malignant Ventricular Arrhythmias Torsades de Pointes
• Sudden Death

Survival Following Sudden Cardiac Arrest
• SCA in athletes is a catastrophic event with a low survival rate (11-16%)
•Low survival rate demands re-evaluation of our current screening and prevention practices.

How Can We Prevent Sudden Cardiac Death
Primary Prevention Preparticipation Evaluation/PPE
–Goal of Screening is to detect potentially life-threatening conditions (Prevalence 0.2-0.4% by estimate, or 1:250-500 young persons).
–Risk stratification to determine who will have a SCA is imperfect.

Methods of Preparticipation Evaluation
• History
– Personal and Family
• Physical Exam
– Murmurs
– Hypertension
– Stigmata of Marfan Syndrome
– Femoral Pulses
• ECG • Echocardiogram • Genetic testing

Preparticipation Physical Evaluation –4th Edition
• Provides a uniform comprehensive history and physical form
• Endorsed by 6 national organizations
• Describes the important questions
AAFP, AAP, ACSM, AMSSM, AOSSM, AOASM

Have you ever passed out or nearly passed out during or after exercise?
Have you ever had discomfort, pain, pressure, or tightness in your chest during exercise?
Do you get lightheaded or feel more short of breath than expected during exercise?
Does your heart ever race or skip beats (irregular beats) during exercise?
Has a doctor ever told you that you have: any heart problem, high blood pressure, high cholesterol, a heart murmur, a heart infection, or an unexplained seizure disorder?
Has a doctor ever ordered a test for your heart (for example, ECG or echocardiogram)?
Has any family member or relative died of heart problems or had an unexpected or unexplained sudden death before age 50 (including drowning, car accident, or sudden infant death syndrome)?
Has anyone in your family had unexplained fainting, seizures, or near drowning?
Does anyone in your family have a heart problem, pacemaker, or implanted defibrillator?
Does anyone in your family have: hypertrophic cardiomyopathy, Marfan syndrome, arrhythmogenic right ventricular cardiomyopathy, long QT syndrome, short QT syndrome, Brugada syndrome, or catecholaminergic polymorphic ventricular tachycardia?
PPE 4th Edition Recommended Personal & Family History Questions
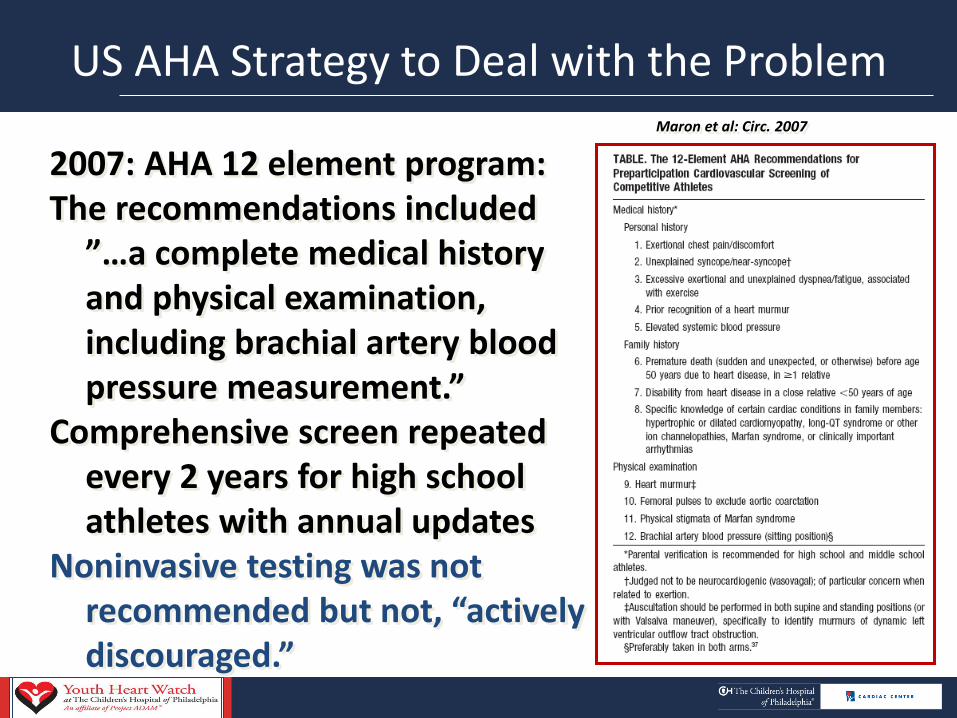
US AHA Strategy to Deal with the Problem
2007: AHA 12 element program: The recommendations included
”…a complete medical history and physical examination, including brachial artery blood pressure measurement.”
Comprehensive screen repeated every 2 years for high school athletes with annual updates
Noninvasive testing was not recommended but not, “actively discouraged.”
Maron et al: Circ. 2007

Problems with Identification of Conditions that Cause SCA
• Symptoms
Occur in 30-50%
May not be present prior to the SCA
SCA 1st symptom: 30-80%
• Family History
Often not known
Positive family history: 20-30%
• Physical Exam
The conditions that cause Sudden Cardiac Arrest may be subtle and not apparent on routine physical exam.
No study has shown that History & Physical can adequately find athletes at risk and prevent SCD.

Methods of Preparticipation Evaluation
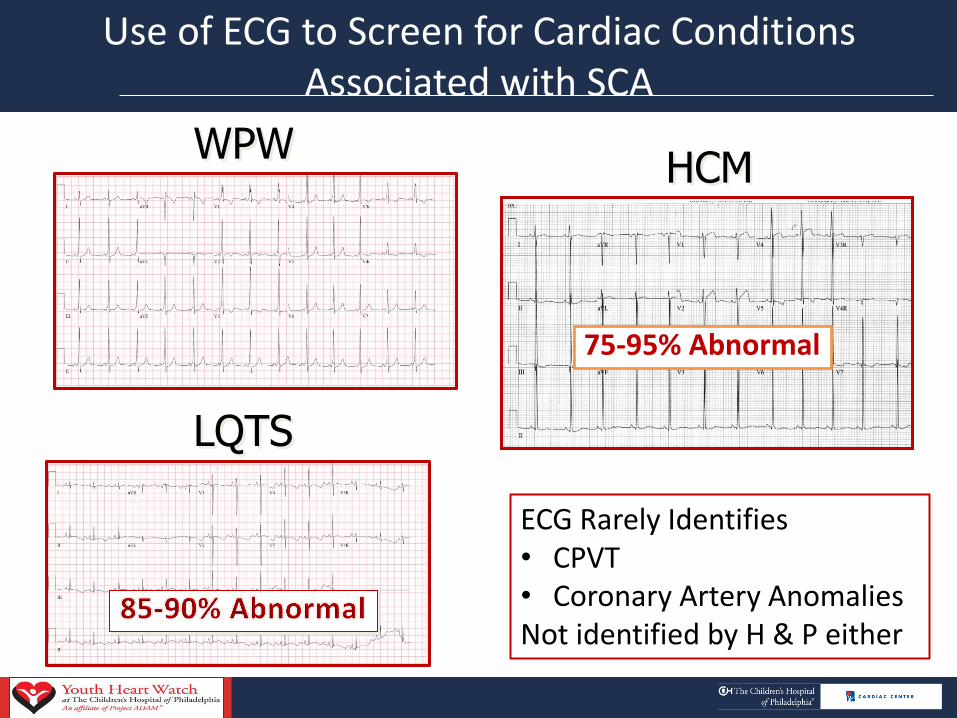
Use of ECG to Screen for Cardiac Conditions Associated with SCA
WPW HCM
LQTS
75-95% Abnormal
ECG Rarely Identifies • CPVT • Coronary Artery Anomalies Not identified by H & P either

Who Uses the ECG to Screen for SCD?
Japan 1973 1st, 7th, 10th graders
Italy 1979 12-35 yo athletes
12 EU countries
IOC

Italian Athletic Screening Program
Medical Protection Athletes Act – 1979
All 12-35 yo who compete in
sports History ,Physical Exam, and ECG • More cases found with ECG than
history & physical exam • ECG had 77% greater power to
detect HCM than History and Physical Exam alone
22
82%
23%
0
5
10
15
20
25 # HCM
ABNECG
Pos.FH/M
0.07%
Corrado NEJM 1998

Would Identifying the Condition Make a Difference?
Italian Athletic Screening Program
Corrado, JAMA 2006
1979-2004: 42,386 athletes screened in Padua, Italy
89% Decrease in Sudden Cardiac Death

Concerns Regarding ECG Screening
• Low disease prevalence, Low PPV
• Current ECG standards may not correctly identify all abnormalities.
Develop more specific new reference standards with norms for race, ethnicity and gender.
• False positives anxiety and costs
Improve test characteristics
• Athletic training affects ECG
Recent data suggests this can be distinguished from pathologic changes
• Limited manpower to interpret ECG:
Use remote reading and computers
• Disqualification concerns: 2%0.2%
Corrado 2009
•Lack of proof for ID of conditions and prevention of SCA Same for ECG and History and Physical

ECG Screening Cost Effectiveness/Year of Life Saved
$0
$5,000
$10,000
$15,000
$20,000
$25,000
$30,000
$35,000
$40,000
$45,000
$50,000
$8,800
$15,926
$44,000 $42,900 $40,855
Japan Italy Neo Nevada HS Wheeler Anderson

Cost Effectiveness Analysis
Fuller et al. , Med Sci Sports Exerc 2000

Am Heart J 2011
Previously undiagnosed CV abnormalities 10.75% –Hypertension >98th % 5% (20) –Important CV Abnormalities 2.5% (10)
400 healthy children –Ages 5-19 years recruited from pediatric practices in Philadelphia area –Questionnaire with patient medical and family history –Physical Exam, ECG, Echocardiogram

Community School Screening Model CHOP Heart Health Screening Study
• 2781 children 5-19 years screened
• Conditions requiring treatment:17
• 2 Atrial Septal Defects
• 7 LQTS
• 7 WPW
• 1 Marfan Syndrome
• 2 Potential cardiomyopathies for follow-up
• Other potentially significant
• Ventricular couplets, 2AV block, Aortic root dilation

Prevention of Sudden Cardiac Death
–Secondary Prevention
•Lifestyle modification, Medication, ICD implants
•Implement CPR/AED Programs –AEDs can be safely placed in schools

National Registry for AED Use in Sports Survey
Total Schools 1710 high schools with on-site AED programs
Interval 2006-07
Emergency Response Plan 83%
Practice Plan Annually 40%
SCA 36 (2.1%)
14 student athletes (16, 14-17 yrs)
22 non-students (57, 42-71 yrs)
Witnessed SCA 35 (97%)
Bystander CPR 34 (95%)
AED shock 30 (83%)
Survival to Hospital Discharge 23 (64%)
9 of 15 students
14 of 22 non-students Drezner et al, Circulation 2009; 120: 518-525

Who Has Laws for AEDs in Schools?
• 24 states have some type of legislation regarding AEDs in schools but only 17 mandate AEDs on a continuing basis
• 7 provide a lower level of coverage
• Other states have laws on CPR, AED teaching
STATE SCHOOL AED LEGISLATION
Ongoing Programs Al, AR, CT, FL, DE, GA, IL, MD,ME, NV, NY, OH, OK, OR,SC,TN,TX
One time Program or limited by funds or group (e.g. College only)
CA, CO, MI, ND, NH,PA,RI
CPR/AED Instruction WI, IA

What happens next? It’s up to YOU……………………
Make a difference in YOUR community. Thank you!