pressure ulcer prevention and care - ostomy wound … · impact on the standards for pressure ulcer...
TRANSCRIPT

Pressure Ulcer Prevention and Care:Incorporating New Federal Guidelines for Assessment,Documentation, Treatment, and Prevention
OstomyWoundManagement
Supplement to April 2005
This activity is made possible by a sponsorship from ConvaTec, A Bristol-Myers Squibb Company, and by HMP Communications.
HMP Communications
C1_ConvaTecCVR_0405.qxd 3/29/05 3:31 PM Page 1

DuoDERM Signal® DuoDERM® Extra Thin DuoDERM® CGF®
DuoDERM®
Hydroactive Gel
Innovatively designed to be people friendly
DuoDERM Signal® dressing, the newest advancementfrom DuoDERM®, the world’s leading family of clinicallyproven hydrocolloid dressings.
DuoDERM is a registered trademark of E.R. Squibb & Sons, L.L.C. ©2005 E.R. Squibb & Sons, L.L.C. US-05-381 www.convatec.com
ConvaTec_DuoDerm_0405.qxd 3/11/05 11:41 AM Page 1

Lia van Rijswijk, RN, MSN, CWCN, is clinical editor, Ostomy WoundManagement; and an adjunct faculty member and public health nurse, LaSalle University School of Nursing and Neighborhood Nursing Center,Philadelphia and Newtown, Pa. Please address correspondence to: Lia vanRijswijk, RN, MSN, CWCN, 210 S. Chancellor Street, Newtown, PA 18940;email: [email protected].
Courtney H. Lyder, RN, ND, GNP, FAAN, is Professor and Chairman,Department of Acute and Specialty Care, University of Virginia MedicalCenter, University of Virginia School of Nursing, Charlottesville, Va. Pleaseaddress correspondence to: Courtney H. Lyder, RN, ND, University ofVirginia Medical Center, University of Virginia School of Nursing, McLeod Hall,Charlottesville, Virginia 22908; email: [email protected].
Meet the Authors
01_MeetAuthors.qxd 3/29/05 4:46 PM Page 2

2
Since the establishment ofMedicare in 1965, providing qualitycare to residents in long-term carefacilities has been a priority for the USDepartment of Health and HumanServices. Much of the oversight fornursing home quality has been dele-gated to the Centers for Medicareand Medicaid Services (CMS). Asadministrator of the Medicare TrustFund, the CMS has had a profoundimpact on the standards for pressureulcer prevention in long-term carefacilities. Through Federal Regulation314 — Pressure Ulcers, CMS guidesfederal and state surveyors on theessentials of pressure ulcer care.Hence, long-term care facilities mustfollow strict guidelines for both preven-tion and treatment of pressure ulcersor risk exposure to financial penaltiesand/or closure by the government as
a result of federal and state mone-tary withholdings. Unquestionably,CMS, through its federal mandates,has a significant impact on long-term care facilities.
Presently, the federal prevalencerate for pressure ulcers in long-termcare is approximately 8.9%.1 This is amajor concern of CMS, which believesthat expected significant reductions inpressure ulcers in long-term care facili-ties have not been realized. A reduc-tion in pressure ulcers is one of twogoals that have been established in2004 for CMS through theGovernment Performance and ResultsAct (GPRA) in nursing homes.2 Thus,the GPRA sets internal goals that theCMS must attempt to achieve over aperiod of time. The actual pressureulcer goal set by the GPRA has notbeen released. However, what is
known is that the current 8.9% is notseen as an acceptable rate for long-term care facilities.
The Centers for Medicare andMedicaid Services has several strate-gies to help decrease the pressureulcer prevalence rate. One such strat-egy is reinterpreting the F-314 regula-tion.3 To this end, CMS embarked ona 3-year process of reinterpreting itspressure ulcer regulation. The revisedinterpretation of the regulation was notonly officially released on November12, 2004, but also took effect on thatday. Thus, a long-term care facilitywould be held accountable for thenew interpretation of the regulationwithout any grace period, potentiallyplacing it at a disadvantage if it hadbeen scheduled for a state or federalsurvey within weeks of the revisedregulation. The purpose of this article
Pressure Ulcer Prevention and Care:Preventing and Managing Pressure Ulcers inLong-Term Care: An Overview of the RevisedFederal Regulation
Courtney Lyder, RN, ND, GNP, FAAN; Lia van Rijswijk, RN, MSN, CWCN
Although the Centers for Medicare and Medicaid Service’s Federal Regulation as it relates to pressure ulcer preven-tion and care in long-term care facilities has not changed, the Guidance to Surveyors (F-314) has been expandedsignificantly. In addition to more clearly defining commonly used terms, the new guidance document emphasizes theuse of pressure ulcer risk assessment and prevention strategies, pain assessment and treatment, and monitoringthe care outcomes. The Centers for Medicare and Medicaid Service has clearly raised the bar on pressure ulcercare. Based on currently available evidence, the guidance document is clear in its intent to encourage all long-termcare facilities to adopt evidence-based pressure ulcer protocols of care. This transition, and the development andimplementation of this guidance document, may present considerable challenges to some long-term care facilities.However, the lack of ambiguity in the F-314 document and its consistency with currently available evidence may behelpful to staff and improve outcomes of care.
Keywords: CMS, surveyor guidance, pressure ulcers
02-06_Lyder.qxd 3/29/05 4:52 PM Page 2

is to highlight some of the essentialcomponents of the revised F-314 andhow a long-term care facility mayimplement the requisite pressure ulcerprevention and treatment componentsso the next survey related to the newF-314 may lead a positive outcome.
Development of the Revised F-314First, it is important to understand
that the Federal regulation for pressureulcers has not changed. The federalregulation simply states the following:
Based on the ComprehensiveAssessment of a resident, the facilitymust 1) ensure that a resident thatenters the facility without pressuresores does not develop pressuresores unless the individual's clinicalcondition demonstrates that they wereunavoidable; 2) promote the preven-tion of pressure ulcer development; 3)promote the healing of pressure ulcersthat are present (including preventionof infection to the extent possible);and 4) prevent development of addi-tional pressure ulcers.3 What haschanged is the interpretation of theregulation. The process of reinterpret-ing F-314 and bringing it to fruitiontook more than 2.5 years to com-plete. Thus, CMS was quite deliberatein taking its time to ensure the docu-ment was well crafted and reflectedcurrent research and professionalopinion related to pressure ulcer pre-vention and treatment.
The CMS created a panel compris-ing federal officers, federal and statesurveyors, national clinical/academicexperts, and key professional groups(National Pressure Ulcer Advisory Panel[NPUAP], American Medical DirectorsAssociation, and similar organizations)to help reinterpret F-314. The panelmet approximately four times and con-ducted numerous teleconferences toreview materials and engage in healthyintellectual discourse. Once the initial
reinterpretation was completed, thedocument was released for publiccomment in 2002. At that juncture,any person or organization was able tocomment on the document.Subsequently, every comment wasread and discussed by the CMSpanel. Based on initial public com-ments, the document was revised andsent out again for a second round ofpublic comment in 2003. Once thesecond public comment period wascompleted, the document was refinedand reviewed by the committee forfinal changes. Once the committee'swork was completed, the documentwas circulated internally at CMS forthe appropriate sign-offs. The finalrevised F-314 document can be readin its entirety at:www.cmshhs.gov/manuals/pm_trans/R4SOM.pdf.3
Highlights of the Revised F-314The 40-page, revised F-314
includes references and the investiga-tive protocol for surveyors. The inves-tigative protocol directs the surveyprocess for residents at risk and/orwith pressure ulcers, as well as helpsthe surveyor determine the level ofdeficiency, if one exists. The mainbody of F-314 is divided into threesections: 1) definitions, 2) prevention,and 3) treatment. Of note: in this revi-sion, the prevention section precedesthe treatment section, suggesting thatCMS may be paying closer attentionto prevention strategies. It is writtenconcisely, providing the surveyor com-munity with sufficient detail to assessany aspect of pressure ulcer preven-tion or treatment.
Definitions. A series of definitionsare provided to the surveyor to clarifyclinical terms related to pressureulcers, their evaluation, and their treat-ment. Hence, the surveyor communityhas a common language that should
be utilized in the medical record for theresident when referring to pressureulcer care.
Avoidability and unavoidability aredefined at the beginning of the defini-tion section. Interestingly, both sets ofdefinitions highlight “recognized stan-dards of practice.” This suggests thatit is imperative for long-term care facili-ties to both understand and implementcurrent standards of practice. TheCMS defines pressure ulcer avoidabili-ty: “The resident developed a pressureulcer and the facility did not do one ormore of the following: evaluate the res-ident's clinical condition and pressureulcer risk factors: define and imple-ment interventions that are consistentwith resident needs, resident goals,and recognized standards of practice;monitor and evaluate the impact of theinterventions; or revise the interven-tions as appropriate.” Unavoidability isdefined as: “The resident developed apressure ulcer even though the facilityhad evaluated the resident's clinicalcondition and pressure ulcer risk fac-tors; defined and implemented interven-tions that are consistent with residentneeds, goals, and recognized stan-dards of practice; monitored and evalu-ated the impact of interventions; andrevised the approaches as appropriate.”
Definitions also are provided for aseries of common ulcer characteris-tics and treatments, including cleans-ing, irrigation, colonized versusinfected, and various debridementmethods. New to the guidance is theuse of maggots as a viable debride-ment strategy. Definitions to delineatesinus tracts from tunneling andundermining and eschar from sloughalso are included.
Prevention. New to the revised F-314 is a plethora of resources (includ-ing websites) that were used to guideits development, such as the NPUAP;Wound, Ostomy and Continence
3
02-06_Lyder.qxd 3/29/05 4:52 PM Page 3

Nurses Society; American GeriatricsSociety; American Medical DirectorsAssociation; and quality improve-ment organizations.
Assessment. The prevention sec-tion underscores F-314's attention toassessment. A series of risk factorsand comorbid conditions are listed.However, the Guidance to Surveyorsclearly stipulates that the list providedis not exhaustive — identifying factorsthat may place a specific resident atrisk for the development of pressureulcers remains the responsibility of theclinicians at the long-term care facility.Of particular interest, and new to F-314, is the explicit suggestion thatalthough a risk assessment instrument(eg, the Braden Scale or Norton Scale)may not place a resident at risk forpressure ulcers, this does not meanthe clinician can ignore single risk fac-tors and refrain from actively attempt-ing to address them, independent ofthe overall score on a pressure ulcerrisk instrument.
Location, tissue tolerance, nutri-tion. The revised F-314 pays a greatdeal of attention to reviewing severalkey concepts related to pressuredevelopment. In addition to identify-ing the more common anatomicallocations for pressure ulcer develop-ment, the document addresses theconcept of tissue tolerance and itsrelationship to pressure ulcer devel-opment. The issues of undernutritionand hydration also are covered in therevised F-314. Little specificity is pro-vided in this section except for notingthat if the resident has a pressureulcer or is at risk for developing one,protein intake should be provided atapproximately 1.2 to 1.5 g/kg bodyweight daily. Moreover, the documentrecommends that the use of a simplemultivitamin is appropriate, butunless specific vitamin or mineralsare depleted, supplementation with
additional vitamins and minerals maynot be helpful.
Skin moisture. The role of skinmoisture and its subsequent sequelaealso are included in the revised survey-or guidance. More importantly, efforthas been made to delineate pressureulcers caused by moisture (increasesfriction and shear forces) versus per-ineal dermatitis. It appears that thetrue distinction lies within the clinician'sability to assess and place into contextthe source of the observed skin irrita-tion and the anatomical site.
Directives. A thoughtful discussionon the role of the resident's right torefuse one or more aspects of pres-sure ulcer care also has been addedto the guidance document. However,the guidance is clear that a resident'sadvanced directives do not absolvethe long-term care facility from provid-ing quality pressure ulcer care. For thefirst time, the Guidance provides clarityon end-of-life care, noting “If the facilityhas implemented individualizedapproaches for end-of-life care inaccordance with the resident's wishes,and has implemented appropriateefforts to try and stabilize the resi-dent's condition and to provide care toprevent and treat the pressure ulcer,then the development, continuation, orprogression of a pressure ulcer maybe consistent with regulatory require-ments. Hence, care must be providedeven though the resident may be athis/her end-of-life, as long as that careis congruent with resident's wishesand is documented as such.”1
Positioning. The usefulness of repo-sitioning also is reviewed and issuessurveyors should consider are listed.Specific care caveats the long-termcare facility should be institutingdependent on mobility status of a resi-dent and time frequency for reposition-ing (eg, offloading a resident sitting in achair once every hour) are addressed.
The concept of pressure redistributionis introduced for the first time in theguidance — ie, when pressure isreduced in one anatomical location, itmay increase the pressure gradient inanother anatomical location; hence,clinicians must remain vigilant, select-ing the most appropriate supportsurface and remaining mindful inorder to safeguard high-risk anatomi-cal locations by providing adequatepressure redistribution.
At-risk patients. Finally, the preven-tion section focuses on monitoring res-idents who may be at risk. TheGuidance suggests that staff shouldbe vigilant as to potential skin integritychanges on a daily basis. Moreover,the guidance recommends weeklydocumentation of complete skinassessment, especially when the resi-dent is using a medical device thatmay cause pressure.
Treatment. Pressure ulcer treatmentcontinues to be a complex processorchestrated by the clinical staff. TheGuidance to Surveyors suggests thatduring the assessment of the ulcer, it iscritical to 1) differentiate the type ofulcer (pressure- versus non-pressure-related ulcer); 2) determine the ulcer'sstage; 3) describe and monitor theulcer's characteristics; 4) monitorprogress toward healing and for poten-tial complications; 5) determine if infec-tion is present; 6) assess, treat, andmonitor pain, if present; and 7) monitordressings and treatments.
A good discussion on a residentrights and end-of-life wound carealso is included. For the first time, theCMS recognizes a resident's right torefuse treatments if that is in accor-dance with the overall plan of care.However, having a Do-Not-Resuscitate order does not relievethe long-term care facility from pro-viding quality pressure ulcer preven-tion or treatment.
4
02-06_Lyder.qxd 3/29/05 4:52 PM Page 4

Monitoring. The Guidance is clear— when a pressure ulcer is present,daily monitoring is needed. Thismonitoring can be quite benign, suchas identifying that the dressing is dry,intact, and not leaking, or mayinclude a description of the ulcerbed. Clarifying the differencebetween monitoring and assessingwill most likely be helpful and serveas a reminder that daily dressingchanges are not required to monitorthe ulcer. Pain appears to be animportant factor in the newGuidance. Reference is made to clini-cian assessment and adequate man-agement of pain when it is present.
Dressing change frequency.Discussion regarding the frequency ofdressing changes is ample. Pressureulcers should be evaluated at leastweekly. Minimum documentationincludes ulcer location, ulcer stage(using the NPUAP staging system),size, exudate amount, pain, woundbed characteristics, and a descriptionof ulcer margins. The Guidance alsosuggests that photographs be taken ifthe facility has a protocol consistentwith accepted standards for photo-graphing wounds.
Healing. Pressure ulcer healing isdiscussed at length. It is the facility'sresponsibility to measure the pres-sure ulcer on a weekly basis.Moreover, the Guidance recognizesvalidated pressure ulcer healinginstruments such as the NPUAPPressure Ulcer Scale for Healing. TheGuidance provides surveyors with atime frame of 2 to 4 weeks for thelong-term care facilities to observesome healing of the pressure ulcer.The document suggests that if noprogress is observed within a 2- to4-week time frame, the long-termcare facility should re-evaluate theresident and the plan of care. TheGuidance also addresses the need
for long-term care facilities to ade-quately assess for the presence ofinfections and adequate pain relief.
Dressings and treatment. The finalsection of the Guidance focuses ondressings and treatment. The focus foreffective wound healing appears to bethe clinician's ability to manage exu-date and promote a moist woundenvironment. No specific dressings arerecommended because no optimaldressing exists for every pressureulcer. The Guidance suggests thatproduct selection should be based ona combination of factors, such asmanufacturer suggested use, pressureulcer characteristics, and goals forhealing. Finally, a brief discussiondescribes the use of wet-to-dry dress-ings. According to the new Guidance,this dressing regimen is associatedwith debridement and even though itmay be appropriate to use in limitedcircumstances, repeated use mayslow the healing process and causepain. Hence, wet-to-dry dressingsshould be used judiciously.
Investigative Protocol andDeficiency Categorization
Investigative protocol. The inves-tigative protocol is used by federaland state surveyors to determine theavoidability or unavoidability of pres-sure ulcers as well as to determinethe effectiveness of the long-termcare facility in preventing and treatingpressure ulcers. The surveyors deter-mine compliance with acceptableprevention or treatment standards ofpractice through direct observation,resident/staff interviews, medicalrecord review, care plan review, andinterviews with healthcare practition-ers and professionals. If the surveyteam concludes that the long-termcare facility has been deficient, thesurvey team must determine the levelof deficiency.
Deficiency categorization. Todetermine the level of deficiency, thesurvey team must consider threeimportant elements: 1) presence ofharm/negative outcome(s) or potentialfor negative outcomes because of lackof appropriate treatment and care; 2)degree of harm (actual or potential)related to the noncompliance; and 3)the immediacy of correction required.Once these three elements have beenconsidered by the team, the surveyteam determines the level of severity.This section contain perhaps the mostsignificant change in the revised F-314. Historically, there were four levelsof severity — now there are three (seeTable 1).
Level 1 deficiencies have been elim-inated from the revised F-314. This ispredicated on CMS's belief that thedevelopment of a pressure ulcer con-stitutes more than minimal harm.Thus, when the surveyors determinethat the long-term care facility hasbeen noncompliant, they must cite thefacility at, minimally, Level 2. The sec-ond major change to the deficiencycategory is the use of sample deficien-cy descriptions to aid surveyor deter-mination of the appropriate level ofseverity. This approach decreases thevariability between surveyor deficien-cies within and between states forsimilar noncompliance infractions.
Impact for Long-Term CareFacilities
Based on the new F-314, long-termcare facilities will need to increase theirsurveillance of residents at risk forpressure ulcers and an increasedfocus on the quality of pressure ulcerprevention plans will be paramount.For example, are the facilities' compo-nents of risk assessment, skin assess-ment, pressure redistribution, supportsurface, nutrition, and skin care inplace and, more importantly, based on
5
02-06_Lyder.qxd 3/29/05 4:52 PM Page 5

current standards of practice?4,5 Theuse of validated tools and algorithmsshould be utilized. In 2003, Lyderand colleagues4 found that the imple-mentation of a comprehensive proto-col to prevent pressure ulcers notonly significantly (P = 02) decreasedthe incidence of pressure ulcers by87% and 76% in two long-term carefacilities, respectively, but it also pro-vided a mechanism to reduce pre-vention costs in both facilities.Similarly, for residents who havepressure ulcers, providing evidence-based wound care that encompass-es the principles of moist woundhealing and includes regular, accu-rate, and comprehensive assess-ments will be imperative. Moreover,remaining vigilant on monitoring the
progress of pressure ulcers will becritical. Managing the entire resident,not just the pressure ulcer, also willbe important. Implementation of thenew guidelines also means that facili-ties will need to consider a variety ofdressings beyond wet-to-dry gauze,which is (correctly) considered adebridement strategy by the CMS.Finally, in order to provide evidence-based care, staff must remaininformed about new developmentsand research findings and periodical-ly re-evaluate their protocols of care.
ConclusionThe process to revise F-314 was a
monumental task for CMS. The doc-ument provides the surveyor com-munity with more information on how
to better evaluate appropriate pres-sure ulcer care. The document isinterdigitated with current evidence tosupport the Centers' probes of long-term care facilities. This is new to theInterpretative Guidance and sends aclear message that the CMS isfocusing on current standards ratherthan old remedies. With the elimina-tion of Level 1 deficiency, the CMSalso indicates that the prevention ofpressure ulcers is paramount in 2005and beyond. The challenge for thelong-term care community to meetthe new regulation will be great butwith careful, thoughtful planning, thisgoal can be achieved. The CMS hasclearly raised the bar in pressureulcer prevention and treatment.
References1. Centers for Medicare and Medicaid
Services. CMS Manual System,Pub.100-07 State Operations,Provider Certification. DepartmentHealth and Human Services,.November 12, 2004. Available atwww.cmshhs.gov/manuals/pm_trans/R4SOM.pdf
2. Centers for Medicare and MedicaidServices. Action Plan for FurtherImprovement of Nursing HomeQuality. Department Health andHuman Services. December 2004.Available at: www.cms.hhs.gov/quali-ty/nhqi/NHActionPlan.pdf.
3. Centers for Medicare and MedicaidServices. Progress in Nursing HomeQuality. Department Health andHuman Services. December 2004.Available at:www.cms.hhs.gov/quality/nhqi/.
4. Lyder C, Shannon R, Empleo-Frazier,O, McGee D, White C. A compre-hensive program to prevent pressureulcers: Exploring cost and outcomes.Ostomy Wound Manage.2003;48(4):52-62.
5. van Rijswijk L, Lyder C. Pressureulcer and care: Implementing therevised guidance to surveyors forlong term care facilities. OstomyWound Manage. 2005;51(4suppl):7–19.
6
Category
Level 1
Level 2
Level 3
Level 4
Previous F-314 severity description
No actual harm withpotential for minimal harm
No actual harm withpotential for more thanminimal harm that is notimmediate jeopardy
Actual harm that is notimmediate jeopardy
Immediate jeopardy to resident health or safety
Pertinent new F-314 severity leveldescriptions and examples
No longer exists
No actual harm with potential formore than minimal harm that is notimmediate jeopardy. For example:a) The development of an avoidable
Stage I pressure ulcerb) Failure to recognize or address
the potential for developing apressure ulcer
Actual harm that is not immediatejeopardy. For example:a) Failure to implement the compre-
hensive care plan for a residentwho has a pressure ulcer
b) The development of recurrent ormultiple avoidable Stage II pres-sure ulcer(s)
Immediate jeopardy to residenthealth or safety. For example: a) Development of avoidable Stage
IV pressure ulcerb) Admitted Stage IV pressure ulcer,
but shows signs of deteriorationor failure to progress due to facili-ty noncompliance
Table 1. Previous and Current F-314 Deficiency SeverityCategorization
02-06_Lyder.qxd 3/29/05 4:52 PM Page 6

Pressure ulcers, defined as “anylesion caused by unrelieved pressurethat results in damage to the underly-ing tissue,”1,2 remain a major concernin all healthcare environments, partic-ularly long-term care facilities. Despiteconcerted efforts by, among others,the Agency for Healthcare Researchand Quality (AHRQ), the NationalPressure Ulcer Advisory Panel, andthe American Medical DirectorsAssociation, as well as the publicationof numerous research and consensusreports related to the effects of opti-mal prevention and treatment ofthese wounds, implementation ofavailable best practice guidelinesremains sparse.1,3 For example, com-prehensive and risk-assessment-based prevention protocols of carehave been found to reduce the inci-dence of pressure ulcers4-6 while treat-ment protocols utilizing optimalwound care strategies reduce healingtime and costs.7,8 The revised guide-lines for surveyors by the Centers forMedicare and Medicaid Services(CMS) link the existing pressure ulcer
prevention and treatment evidencebase with federal guidelines.9 As aresult, it is now imperative that long-term care facilities implement evi-dence-based protocols of preventionand care. The guidance documentrecommendations are summarizedand their rationale and pertinentbackground information are providedto help administrators and cliniciansdevelop and implement these proto-cols of care in preparation for theirnext survey.
Pressure Ulcers: Etiology andComponents of Care
While it is common knowledge thatpressure, and the resultant obstruc-tion of capillary flow, is the main causeof these wounds and hinders theirability to heal, a variety of factorsincrease or decrease resident suscep-tibility to the adverse effects of pres-sure. Some risk factors, such as skinexposure to moisture, can be modi-fied. However, the potential deleteri-ous effects of other factors cannot bemodified at all or only partially
addressed. For example, in personswith diabetes mellitus, supportive caremust be supplemented with improvedglucose control to help reduce thepotential complications of this dis-ease. Although pressure ulcers com-monly occur at the end of life and thegoal of a resident’s plan of care maynot be healing an existing ulcer, manypressure ulcer prevention and treat-ment strategies are consistent withpalliative care strategies10 — eg, com-passionate care often includes imple-menting measures to prevent thedevelopment of pressure ulcers orprevent worsening of existing woundsto prevent increased suffering.
Regardless of the ultimate goal ofcare, components of care that affectevery facet of pressure ulcer preven-tion and treatment are interdiscipli-nary teamwork and education of allstaff members, residents, and familymembers.3,11 A successful pressureulcer program always involves a vari-ety of disciplines, facility staff at alllevels, dedication to excellence, andoptimal communication.
Pressure Ulcer Prevention and Care:Implementing the Revised Guidance toSurveyors for Long-Term Care Facilities
Lia van Rijswijk, RN, MSN, CWCN; and Courtney H. Lyder, ND
The revised guidelines for long-term care surveyors by the Centers for Medicare and Medicaid Services link theexisting pressure ulcer prevention and treatment evidence base with federal guidelines. The guidance document isdetailed and attempts to ensure that residents receive optimal care to help prevent and manage these wounds.Implementation of the guidance document recommendations requires a complete review, and possibly revision, ofexisting policies and procedures. Understanding the background, rationale, and methods to implement these rec-ommendations will help administrators and clinicians develop protocols of care that are effective, cost efficient, andcomply with the new guidelines.
Keywords: pressure ulcers, long-term care, CMS, guidelines
7
07-19_Lia.qxd 3/29/05 4:47 PM Page 7

8
PreventionMonitoring and assessment.
Before developing and implement-ing any pressure ulcer prevention ortreatment protocol of care, the dif-ference between monitoring andassessing/evaluating a resident,skin condition, and/or wound mustbe understood. An assessment orevaluation always includes verifica-tion and interpretation of the obser-vations made; whereas, monitoringor inspecting simply means “keep-ing track” or “watching.”12 Forinstance, daily monitoring of a resi-dent's skin while providing routinecare may reveal that a reddenedarea has developed. This observa-tion is recorded and may warrant acomplete assessment by a staffmember who has the skills and
knowledge needed to interpret thesignificance of the observation.Assessments are also more time-consuming than monitoring proce-dures. Fortunately, the revisedGuidance to Surveyors for Long-Term Care Facilities related to thefederal regulation for pressureulcers also makes this distinction;hence, no conflict exists betweensuggested monitoring andreassessment intervals and therevised F-314.2
Optimal pressure ulcer preventionstrategies are based on an individualresident assessment and must focuson ameliorating or reducing theeffects of the underlying etiology.Clinical studies most frequentlyreport the following individual pres-sure ulcer risk factors: reduced
mobility, nutritional deficiencies,incontinence, diabetes mellitus,decreased mental status, and a his-tory of pressure ulcers.13 In additionto obtaining a complete assessment— including a skin inspection — andhistory on admission, the most expe-dient way to assess a resident's riskof developing pressure ulcers is byusing the Braden Scale for predictingpressure ulcers because this scalehas been shown to be both valid andreliable.14,15 The Braden scale is prob-ably the most widely used riskassessment tool in the world.16
Studies have found that long-termcare resident risk assessments arebest performed within 48 hours fol-lowing admission, weekly for the firstfour weeks after admission, and atregular intervals thereafter, or whenthe resident's condition changes.15
The Braden scale contains sixsubscales, designed to assess intrin-sic and external risk factors; potentialtotal score ranges from 6 to 23 withhigher scores indicating a higher levelof functioning17 (see Table 1).Although cut-off scores must beevaluated in light of a resident's gen-eral health condition and factors thatmay not be captured by the Bradenscale (eg, impaired blood flow, end-stage renal disease, diabetes melli-tus), residents with a Braden scalescore of 18 or below are generallyconsidered to be at risk for develop-ing pressure ulcers.15 Specifically, res-idents with a score of 18 to 15 areconsidered to be at mild, 12 to 14 atmoderate, and ≤11 at high risk fordeveloping pressure ulcers.
Regardless of risk level, daily skininspection of residents with limitedmobility is crucial to detecting thefirst signs of a pressure ulcer. Skinmarkings from medical devices andreddened, tender, cool, indurated,or warm areas should be noted,
Subscale ItemSensory perception: abilityto respond meaningfully topressure related discomfort
Moisture: degree to whichskin is exposed to moisture
Activity: (degree of physicalactivity
Mobility: ability to changeand control body position
Nutrition: usual food intakepattern
Friction and shear: degreeto which assistance withmovement is needed
Item BackgroundLimited sensory perceptionincreases risk of notresponding to and relievingthe discomfort of prolongedpressure
An extrinsic risk factor, pro-longed exposure to moistureand/or irritants such as urineor feces increases risk of skinirritation and breakdown
Activity enhances circulationand influences metabolism
While mobility may be limited(eg, bedfast), residents whoare able to move frequentlyhave a lower pressure ulcerrisk than those who areunable to change positions
Poor nutritional status is anintrinsic risk factor for pres-sure ulcer development andassessed by rating intakepatterns
Friction and shear, from slidingduring transfer or slidingdown in bed or chair, is anextrinsic risk factor for pres-sure ulcer development
Score Range1 (= high risk) to 4 (= low risk)
1 (= high risk) to 4 (= low risk)
1 (= high risk) to 4 (= low risk)
1 (= high risk) to 4 (= low risk)
1 (= high risk) to 4 (= low risk)
1 (= high risk) to 3 (= low risk)
Table 1. Braden Scale Items and Scoring
07-19_Lia.qxd 4/29/05 11:32 AM Page 8

especially when found on high-riskareas such as the occiput, sacrum,heel, coccyx, tuberosity, ischial area,or trochanter. The above-mentionedpressure-related skin changes arereferred to as Stage I pressureulcers.1 These changes may be diffi-cult to assess, especially in personswith darkly pigmented skin. When indoubt about the potential presenceof a Stage I ulcer, the residentshould be positioned off the areaand re-assessed after 30 or 45 min-utes. If changes persist, a preventionprotocol should be implemented.2
Implementation of a comprehensiveprevention protocol must be initiatedfor all residents who have intact skinand are at risk for developing, or whoalready have, a pressure ulcer.
Finally, documentation of pressureulcer risk, individual risk factors,assessment findings, and protocolsof care is crucial, yet reported to befrequently overlooked.18
Interventions. While most meas-ures to prevent the development ofpressure ulcers also provide comfortand may improve resident quality oflife, some may be inconsistent withthe overall goal of resident care. Forexample, in the terminally or chroni-cally ill, a pressure ulcer may be acomorbid pathologic process andindicative of impending death.19 If theoverall goal of care is to providecomfort and breathing is difficultwhen the head of the bed or chair ispositioned at a low angle of elevationto reduce pressure on the sacralarea, the option of keeping the headof the bed raised should be dis-cussed with the resident and/or theresident's legal representative.Similarly, in malnourished residents,regardless of prognosis, the potentialpositive effects of enteral feeding onpressure ulcer prevention and healingmust be considered in light of the
high rate of complications associatedwith long-term tube feeding.20 All caredecisions and exceptions, particularlythose that may increase the risk ofcomplications such as pressureulcers, should be noted in the resi-dent’s chart.
Pressure ulcer prevention strate-gies consist of addressing the riskfactors identified during assessment(see Table 2). Most residents requireimplementation of multiple interven-tions. For example, use of a specialsupport surface does not replace theneed to reposition residents who areunable to shift positions by them-selves. In one pressure ulcer preven-
tion study, turning patients placed ona support surface every 4 hours wasfound to be more effective than turn-ing patients every 6 hours.21
Comprehensive prevention programsfor elderly persons that includeimplementation of risk assessmenttools, support surfaces, skin careprotocols, repositioning schedules,nutritional support, and staff educa-tion have been shown to reduce theincidence of pressure ulcers and arecost-effective.4,5
Support and positioning surfaces.1. Support surfacesStandard foam mattresses are not
appropriate for persons with limited
Risk FactorReduced mobilityand activity
Shear and fric-tion (secondaryto reduced mobility/activity)
Nutritional/hydration deficit
Skin exposed tomoisture
Intervention- if possible, teach resident tochange positions frequently
- place resident on pressure-reduc-ing mattress/bed and chair cushion
- implement turning/repositioningschedule
- assess resident position (alignment,stability, pressure redistribution) andpotential pressure points, includingdevices (eg, catheters)
- position resident to avoid “sliding”in bed (eg, keep head of bed atlowest degree of elevation)
- use lifting devices to help move/reposition resident
- develop nutritional care plan - encourage increased dietary intake(particularly protein)
- monitor fluid intake/output- multivitamin may be appropriate
- establish bladder/bowel programand/or select absorbent productsthat wick moisture away from skin
- gently cleanse and dry skin aftereach incontinence episode
- apply skin barrier products- consider temporary use of fecalmanagement system or urinarycatheter
Comments- If possible, regularlylower head of bed/back of chair to <30degree angle
- Keep written records ofturning/repositioningschedule
- Pay particular attentionto heels and elbowsand use pillows toposition/elevate
- A trapeze may helpresidents who are ableto assist with reposi-tioning
- Involuntary weight loss,poor dietary intake,and/or low albumin orpre-albumin levels arecommon signs of mal-nutrition
- Urinary/fecal inconti-nence can cause der-matitis and skin break-down
- Use pH-balancedcleansers, avoid friction
Table 2. Interventions to Reduce the Risk of PressureUlcers
9
07-19_Lia.qxd 3/29/05 4:47 PM Page 9

10
mobility and who are at risk fordeveloping pressure ulcers.22
Support surfaces are generally clas-sified according to their Medicarereimbursement group: Group 1 (stat-ic devices such as air, foam, gel, andwater overlay or mattresses); Group2 (dynamic, or powered overlays ormattresses); or Group 3 surfaces(dynamic air-fluidized beds). Group 1static devices are most commonlyused for residents who are at mild ormoderate risk and those who have aStage I ulcer. Study results suggestthat overlays and replacement mat-tresses reduce the incidence ofpressure ulcers when compared tostandard hospital mattresses andsome evidence shows that solidfoam overlays are more effectivethan convoluted foam mattresses.22,23
Regular assessment of these prod-ucts and making sure that they arein good condition are important. Forexample, if a 4-inch foam mattress iscompressed to 1 or 2 inches in anylocation, the mattress is “bottomingout” and not effective.
Dynamic or powered overlays ormattresses are generally used forpersons with pressure ulcers andresidents at moderate or high risk fordeveloping ulcers. Even thoughmany powered support surfacestudies have been conducted, theirvariability makes it difficult to ascer-tain their relative merits and users
may decide to choose a surfacebased on performance characteris-tics such as surface life expectancy,service requirements, moisture con-trol, and shear/friction reduction.22,23
Because pressure on the heels rarelycan be sufficiently relieved on aGroup 1 or 2 surface, measures toelevate the heels (eg, using pillowsor foam wedges) must be taken. Group 3 surfaces provide more pres-sure reduction and are more costlyto rent or purchase than Group 1 or2 surfaces. Therefore, they are usu-ally reserved for persons with verylimited mobility and deep pressureulcers. A recent long-term-carestudy found that residents on Group3 surfaces had a higher illness scoreand were more likely to have StageIII or Stage IV pressure ulcers thanthose on Group 2 or Group 1 sur-faces.24 Stage III/IV ulcers of resi-dents on Group 3 surfaces also werefound to have statistically significant-ly greater healing rates than thoseon Group 1 or 2 surfaces.24
Choosing the right support sur-face remains a challenge, in partbecause manufacturers continue touse a wide variety of methods to testbasic performance characteristicsand use different terminology todescribe product features.23,25 Untilclinicians are able to compare theresults of clinical studies and productfeatures and characteristics are stan-
dardized, few specific product usagerecommendations can be made.
2. PositioningIf at all possible, residents should
not be positioned on existing red-dened areas or pressure ulcers andthey should be repositioned regular-ly. If consistent with the overall goalof care, a 2-hour turning scheduleshould be implemented. Foamwedges and pillows can be useful toposition residents and protect par-ticularly vulnerable areas such asheels and elbows. To reduce the riskof skin damage from shear and fric-tion, the head of the bed or chairshould be kept at a low angle (30degrees or lower) and lifting devicesshould be used to transport or repo-sition residents.3
Nutritional/hydration deficits.Nutritional and hydration deficits arecommon among institutionalized eld-erly and an important risk factor forthe development of pressure ulcersand delayed healing.26 One studyfound that a combination of immobili-ty, loss of lean body mass, andimmune system challenges increasesthe risk of pressure ulcers by 74%.27
Although nutritional intake is a com-ponent of the Braden Scale, assess-ing the nutritional and hydration sta-tus of all residents is crucial.2 Dietaryneeds change with increasing age —older adults generally need fewercalories but more nutrients and fluids.When an ulcer develops, nutritionalneeds (particularly protein) increaseeven more.26 Residents at high risk fordeveloping pressure ulcers or thosewho already have an ulcer generallyrequire supplementation. Becauseexisting health conditions (eg,impaired renal or hepatic function,anemia of chronic disease, dialysis)may contraindicate the administrationof certain supplements, a dietitianconsult is advisable.
Figure 1. The effect of moisture and incontinence on the skin.
07-19_Lia.qxd 3/29/05 4:48 PM Page 10

Skin moisture. Moist skin, particu-larly if the source of moisture is urineor feces, is more vulnerable to thepotential effects of shear, friction, andpressure than dry skin (see Figure 1).Perineal dermatitis, characterized byintense erythema, scaling, itching,papules, weeping, and eruptions, ispainful and may progress to ulcera-tion and bacterial (Staphylococcus)or yeast (Candida albicans) infec-tions.28 The Wound Ostomy andContinence Nurses Society 2003Guidelines29 include the following rec-ommendations for managing inconti-nence to prevent pressure ulcer for-mation: 1) establish a bowel andbladder program, 2) cleanse skingently at each time of soiling withpH-balanced cleansers, 3) use incon-tinence skin barriers,4) select under-pads, diapers or briefs that areabsorbent and wick moisture away,5) consider use of a pouching sys-tem or collection device to containurine or stool, and 6) consider appro-priateness of short-term indwellingcatheter use to prevent pressureulcer contamination.
If consistent with the overall goalof care, bowel and bladder pro-grams may reduce the number ofincontinent episodes; thus, reducingskin exposure to moisture andpotential friction and irritation fromcleansing. Most soaps and syntheticsurfactants are anionic — ie, theyhave a negative electrical charge,rendering them more irritating thancleansers without a charge (nonion-ic).30 Studies have shown that clean-ing the skin can lead to changes inthe skin's surface pH, which, in turn,may affect the resident (normal) skinflora. Because the skin of olderadults is vulnerable and cleansing isneeded following each incontinenceepisode, the area should be gentlywiped using a pH-balanced cleanser
or special pH-balanced perinealcleanser and a product to protectand moisturize the skin should beapplied. Results of a recent studysuggest that the ability of special skinprotection creams to fulfill all threeproduct requirements (protectagainst irritants, protect against mac-eration, moisturize) varies as a resultof their ingredients.31 Products con-taining petroleum provide protectionagainst irritants and maceration andprovide some moisturization; prod-ucts with a zinc oxide base are effec-tive barriers against irritants but areless effective at preventing macera-tion and moisturizing the skin.
Sometimes, when skin irritation issevere, the resident has diarrhea, oran existing wound continues to becontaminated by urine or feces, itmay be necessary to temporarily usea fecal management system or uri-nary catheter (see Figure 2). A fecalpouching system also can be used ifa skin wafer can be attached.
Meticulous incontinence care isindicated for all residents regardlessof the overall goal of care to increasethe resident's comfort and help pre-vent painful irritation and skin break-down. Such diligence may make itunnecessary for staff to face the addi-tional challenges of managing pres-sure ulcers in incontinent residents.
Assessment and treatment.Most pressure ulcer prevention rec-ommendations described — includ-ing pressure redistribution, moisturemanagement, and nutritionalassessments — also need to beimplemented for residents withpressure ulcers because variablesthat cause the formation of theseulcers also delay their healing.Further, the underlying physiologicalcauses (eg, appropriate manage-ment of diabetes or peripheral vas-cular disease) that may place the
resident at risk or impede the heal-ing process must be addressed.32
In addition, residents who alreadyhave a pressure ulcer are atincreased risk for developing addi-tional ulcers.33 All wounds increaseresident nutritional needs. Once anulcer has developed, a resident's riskfor under-nutrition, particularly pro-tein-energy malnutrition, increases. Anutritional consult and implementa-tion of a nutrition care plan, includingprotein and vitamin supplementation,should be considered for all residentswith pressure ulcers.26 When assess-ing the ulcer itself, the Guidance toSurveyors2 emphasizes the impor-tance of ulcer diagnosis and differen-tiation, ulcer staging and assess-ment, monitoring of ulcer progress,assessment of complications includ-ing the presence of infection, assess-ment, treatment and monitoring ofpain, and monitoring of dressingsand treatments.
Ulcer differentiation and location.Pressure ulcers usually occur over abony prominence, (eg, the sacrumand coccyx area, trochanter, ischialtuberosity, ankles, heels, scapula, orocciput). Occasionally, a pressureulcer may be observed in anotheranatomical location as a result ofpressure from a device (eg, cast,catheter). In the absence of an obvi-ous source of pressure and when the
Figure 2. Fecal containment system.
11
07-19_Lia.qxd 3/29/05 4:48 PM Page 11

12
ulcer does not appear over a bonyprominence (eg, lower leg), a differen-tial diagnosis must be made becausethe wound could be the result of vas-cular or arterial insufficiency.
The Guidance documentdescribes venous insufficiencyulcers as “open lesions of the skinand subcutaneous tissue of thelower leg, usually occurring in thepretibial area of the lower leg orabove the medial ankle”2 (seeFigure 3). These wounds are usual-ly shallow and are associated withmoderate or heavy amounts of exu-date because many residents withvenous ulcers also have lower legedema. Obtaining a differentialdiagnosis before starting treatmentis crucial — the most importanttreatment component of venousulcers, compression bandages, iscontraindicated in residents witharterial ulcers.34
Venous and arterial ulcers areoften painful. However, residents witharterial ulcers, which are usually the
result of arterial occlusive disease,frequently experience intermittentclaudication as well. A completephysical examination, clinical history,and vascular laboratory tests willhelp clinicians diagnose the causeof lower leg ulcers. Most of theother principles of local wound care,such as frequent assessments andmaintaining a moist wound environ-ment, as well as general supportivecare measures to maintain orimprove the resident's overall health,nutritional, and hydration status, arethe same as those described forpressure ulcers.
A special note should be madeabout ulcers on the feet of residentswith diabetes mellitus. Depending onthe location of the wound, arterialinsufficiency or unrelieved pressureas a result of loss-of-sensation (neu-ropathy) may be the culprit (seeFigure 4). While optimal wound careand glucose control are crucial tohelping these wounds heal, addition-al wound assessments, diagnosticstudies, and/or pressure offloadingtechniques may be needed.35 Thelocation of the ulcer should be docu-mented in the Minimum Data Set(MDS) and resident's chart.
Ulcer staging. Pressure ulcers arecommonly “staged.” The F-314 andMDS use the National Pressure UlcerAdvisory Panel ulcer staging defini-tions1 (see Table 3). Although not anexact science, pressure ulcer stagingdefinitions help healthcare profes-sionals use the same language todescribe ulcer depth and the extendof damage to the skin. If the ulcer iscovered with necrotic tissue, thewound is usually deep, but accurate-ly assessing the extent of tissuedamage is not possible (see Figure5). In these instances, the MDSinstructions must be followed forcoding purposes — ie, the RAI
Figure 3. Venous ulcer: Note charac-teristic change in skin pigmentation.
Figure 4. Diabetic neuropathic ulcer.
StageI
II
III
IV
DefinitionAn observable, pressure-related alteration of intact skin, whose indica-tors as compared to an adjacent or opposite area on the body mayinclude changes in one or more of the following parameters: skin tem-perature, tissue consistency, sensation, and or a defined area of per-sistent redness in lightly pigmented skin, whereas in darker skin tones,the ulcer may appear with persistent red, blue, or purple hues
Partial-thickness skin loss involving epidermis, dermis, or both. Theulcer is superficial and present clinically as an abrasion, blister, or shal-low crater
Full-thickness skin loss involving damage to, or necrosis of, subcuta-neous tissue that may extend down to, but not through, underlyingfascia. The ulcer presents clinically as a deep crater with or withoutundermining of adjacent tissue
Full-thickness skin loss with extensive destruction, tissue necrosis, ordamage to muscle, bone, or supporting structures (eg, tendon, jointcapsule). Undermining and sinus tracts also may be associated withStage IV pressure ulcers
Table 3. National Pressure Ulcer Advisory PanelPressure Ulcer Definitions/Staging System*
* From NPUAP. Available at: http://www.npuap.org
07-19_Lia.qxd 3/29/05 4:48 PM Page 12
User's Manual Version 2 instructsassessors to code these ulcers as aStage IV.
Ulcer monitoring, assessment,and progress. The F-314 has fol-lowed NPUAP consensus panelsuggestions related to pressureulcer assessments and monitoring,including daily monitoring of all resi-dents with a pressure ulcer.2,12 TheF-314 suggests that monitoring canoccur independent of the presenceof a dressing. Thus, the CMS doesnot support dressing removals tomonitor the pressure ulcer. If nodressing is present (eg, residentswith a Stage I pressure ulcer), theulcer should be evaluated andobservations documented. If thewound is dressed and a dressingchange is not indicated, the statusof the dressing (leakage of woundexudate, adhesion), the surroundingskin condition, and pain should bemonitored. Increased pain, swelling,or redness of the surrounding skinmay indicate the presence of infec-tion.29,36 Redness or pain also maysuggest less-than-optimal pressureredistribution. For example, if painand redness subside when the resi-dent is repositioned and there is nopressure on the area, pressure-redistribution protocols must be re-evaluated. Similarly, shear and fric-tion may be the culprits if a dressingdesigned to remain in place for 4 or5 days is dislodged almost daily or ifthe edges continue to “roll up.” Dailymonitoring will help spot these prob-lems early and prevent long-termexposure of the wound to the dele-terious effects of pressure, shear,and friction.
A complete ulcer assessmentshould be performed at each dress-ing change or at least weekly.2 Ulcerassessments provide the foundationfor the resident's plan of care and
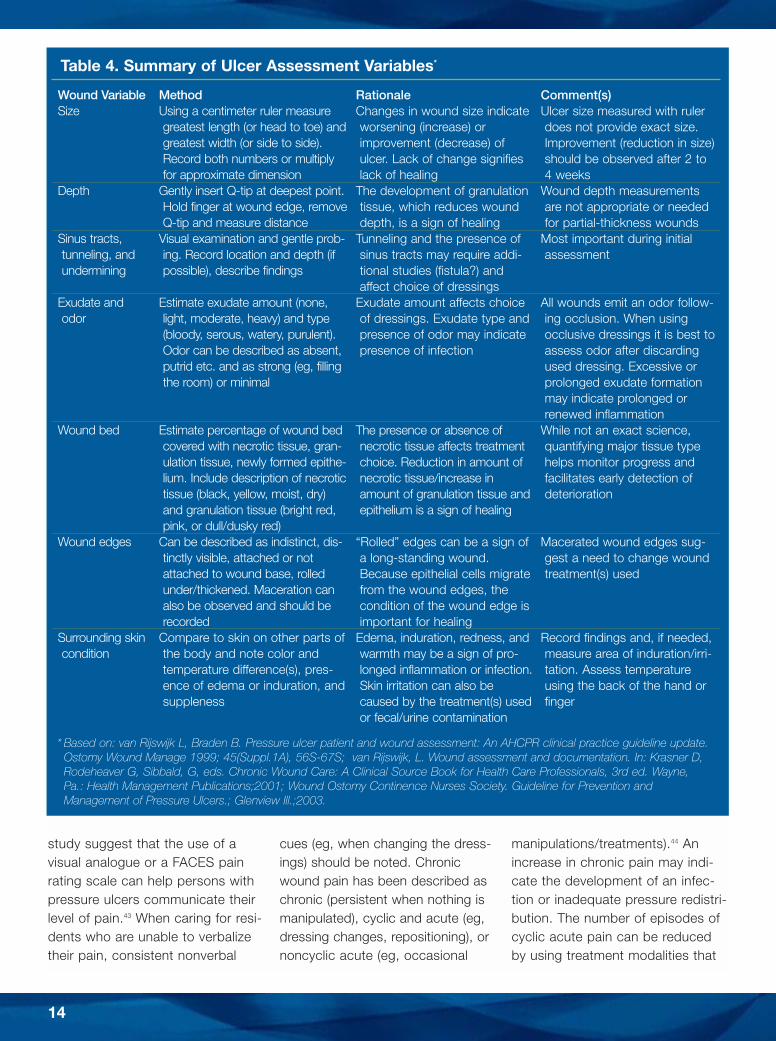
are crucial to monitoring the effec-tiveness of that plan.36 In addition toassessing wound depth throughstaging, ulcer characteristics used toasses these wounds include size,exudate, pain, and wound bed andsurrounding skin characteristics (seeTable 4, Figures 6 and 7). With theexception of wound pain, all woundvariables described in the guidancedocument are included in thePressure Sore Status Tool; whereas,the National Pressure Ulcer AdvisoryPanel's Pressure Ulcer Scale forhealing (or PUSH tool) contains threeof the above-mentioned wound vari-ables.37,38 Both tools have been thesubject of validation studies but atthis time which instrument is mostlikely to help predict healing isunknown. Some but not all variableshelp determine which treatmentshould be used. For example, exu-date amount is generally the first vari-able to consider when choosing awound treatment modality; whereas,change in ulcer size is an importantvariable to help evaluate progresstowards healing.2,29,39 Specifically, theresults of pressure ulcer and otherchronic wound studies have shownthat a reduction in ulcer size after 2to 4 weeks of care is a predictor oftreatment outcome and/or healing.40-
42 The guidance document also sug-gests the use of photographs fordocumentation, providing the facilityhas a protocol for taking quality pho-tographs. To maximize their useful-ness, photographs should include ameasuring tape, resident identifica-tion, and date.2
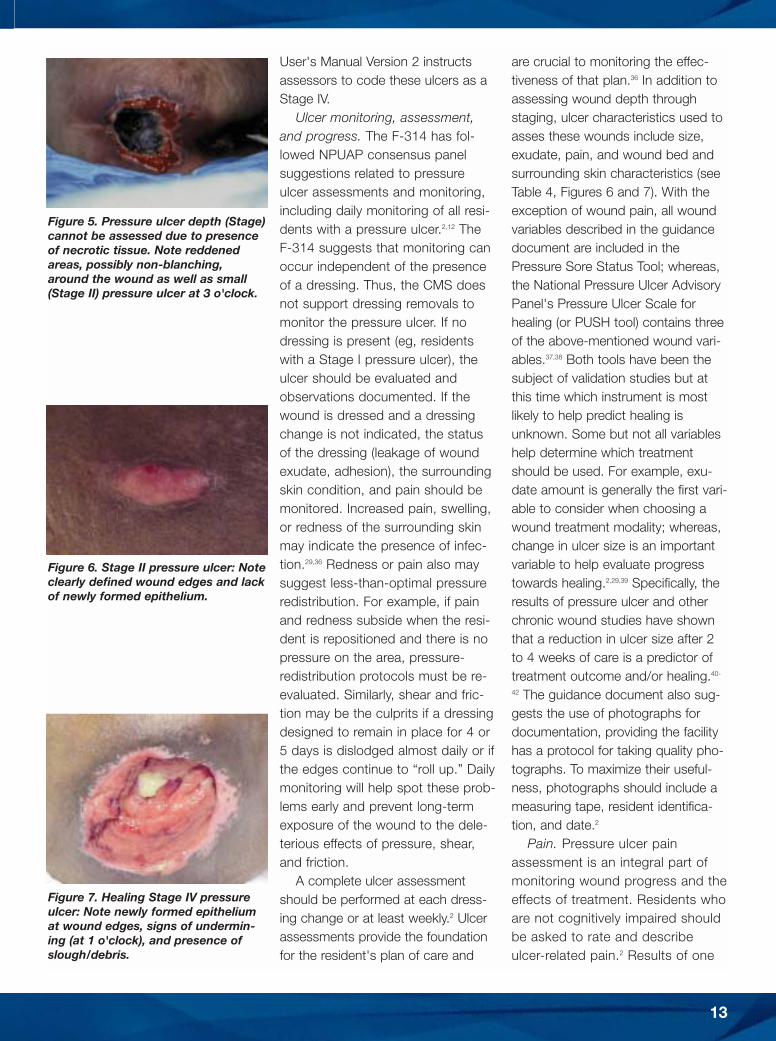
Pain. Pressure ulcer painassessment is an integral part ofmonitoring wound progress and theeffects of treatment. Residents whoare not cognitively impaired shouldbe asked to rate and describeulcer-related pain.2 Results of one
Figure 5. Pressure ulcer depth (Stage)cannot be assessed due to presenceof necrotic tissue. Note reddenedareas, possibly non-blanching,around the wound as well as small(Stage II) pressure ulcer at 3 o'clock.
Figure 6. Stage II pressure ulcer: Noteclearly defined wound edges and lackof newly formed epithelium.
Figure 7. Healing Stage IV pressureulcer: Note newly formed epitheliumat wound edges, signs of undermin-ing (at 1 o'clock), and presence ofslough/debris.
13
07-19_Lia.qxd 3/29/05 4:48 PM Page 13
14
study suggest that the use of avisual analogue or a FACES painrating scale can help persons withpressure ulcers communicate theirlevel of pain.43 When caring for resi-dents who are unable to verbalizetheir pain, consistent nonverbal
cues (eg, when changing the dress-ings) should be noted. Chronicwound pain has been described aschronic (persistent when nothing ismanipulated), cyclic and acute (eg,dressing changes, repositioning), ornoncyclic acute (eg, occasional
manipulations/treatments).44 Anincrease in chronic pain may indi-cate the development of an infec-tion or inadequate pressure redistri-bution. The number of episodes ofcyclic acute pain can be reducedby using treatment modalities that
Wound VariableSize
Depth
Sinus tracts, tunneling, andundermining
Exudate and odor
Wound bed
Wound edges
Surrounding skincondition
MethodUsing a centimeter ruler measuregreatest length (or head to toe) andgreatest width (or side to side).Record both numbers or multiplyfor approximate dimension
Gently insert Q-tip at deepest point.Hold finger at wound edge, removeQ-tip and measure distance
Visual examination and gentle prob-ing. Record location and depth (ifpossible), describe findings
Estimate exudate amount (none,light, moderate, heavy) and type(bloody, serous, watery, purulent).Odor can be described as absent,putrid etc. and as strong (eg, fillingthe room) or minimal
Estimate percentage of wound bedcovered with necrotic tissue, gran-ulation tissue, newly formed epithe-lium. Include description of necrotictissue (black, yellow, moist, dry)and granulation tissue (bright red,pink, or dull/dusky red)
Can be described as indistinct, dis-tinctly visible, attached or notattached to wound base, rolledunder/thickened. Maceration canalso be observed and should berecorded
Compare to skin on other parts ofthe body and note color andtemperature difference(s), pres-ence of edema or induration, andsuppleness
RationaleChanges in wound size indicateworsening (increase) orimprovement (decrease) ofulcer. Lack of change signifieslack of healing
The development of granulationtissue, which reduces wounddepth, is a sign of healing
Tunneling and the presence ofsinus tracts may require addi-tional studies (fistula?) andaffect choice of dressings
Exudate amount affects choiceof dressings. Exudate type andpresence of odor may indicatepresence of infection
The presence or absence ofnecrotic tissue affects treatmentchoice. Reduction in amount ofnecrotic tissue/increase inamount of granulation tissue andepithelium is a sign of healing
“Rolled” edges can be a sign ofa long-standing wound.Because epithelial cells migratefrom the wound edges, thecondition of the wound edge isimportant for healing
Edema, induration, redness, andwarmth may be a sign of pro-longed inflammation or infection.Skin irritation can also becaused by the treatment(s) usedor fecal/urine contamination
Comment(s)Ulcer size measured with rulerdoes not provide exact size.Improvement (reduction in size)should be observed after 2 to4 weeks
Wound depth measurementsare not appropriate or neededfor partial-thickness wounds
Most important during initialassessment
All wounds emit an odor follow-ing occlusion. When usingocclusive dressings it is best toassess odor after discardingused dressing. Excessive orprolonged exudate formationmay indicate prolonged orrenewed inflammation
While not an exact science,quantifying major tissue typehelps monitor progress andfacilitates early detection ofdeterioration
Macerated wound edges sug-gest a need to change woundtreatment(s) used
Record findings and, if needed,measure area of induration/irri-tation. Assess temperatureusing the back of the hand orfinger
Table 4. Summary of Ulcer Assessment Variables*
* Based on: van Rijswijk L, Braden B. Pressure ulcer patient and wound assessment: An AHCPR clinical practice guideline update.Ostomy Wound Manage 1999; 45(Suppl.1A), 56S-67S; van Rijswijk, L. Wound assessment and documentation. In: Krasner D,Rodeheaver G, Sibbald, G, eds. Chronic Wound Care: A Clinical Source Book for Health Care Professionals, 3rd ed. Wayne,Pa.: Health Management Publications;2001; Wound Ostomy Continence Nurses Society. Guideline for Prevention andManagement of Pressure Ulcers.; Glenview Ill.;2003.
07-19_Lia.qxd 3/29/05 4:48 PM Page 14

require less frequent wound manip-ulation; the pain intensity of unavoid-able procedures can be addressedby administering systemic or localpain medication before the proce-dure.44 Non-pharmacologic painreduction strategies may includereducing shear, friction, and pressurethrough positioning and pressure-redistribution; gentle removal ofdressing materials; use of lukewarminstead of cold wound cleansing flu-ids; providing “time-outs”; and usingtreatments that do not cause pain.Controlled clinical studies ofpatients with acute wounds haveshown that wounds covered with ahydrocolloid dressing, which pro-vides a moist wound environment,(eg, DuoDERM®: DuoDERM® is aregistered trademark of E.R. Squibband Sons, L.L.C.) exhibited lesspain during dressing changes thanwounds covered with gauze-typedressings.45,46 Finally, the pain ofoccasional interventions such assurgical debridement must beaddressed before the procedure.While much remains unknownabout the intensity, nature, frequen-cy, and types of pressure ulcerpain, the vast majority of personswith pressure ulcers experienceboth constant pain and pain duringdressing changes.47 Pressure ulcerpain can and must be assessed,documented, and alleviated.
Dressings and treatments. Giventhe plethora of treatment choicesavailable today, it is helpful toremember the basics: 1) woundcleansing is the first step in thedressing process, 2) all treatmentchoices must be based on woundand resident assessment findingsand the goals of care, and 3) thetreatment must be safe and effective.With respect to the latter, data tosupport the safety and effectiveness
of many wound care modalitiesavailable today are limited; hence,practitioners are encouraged toreview all available evidence beforemaking a product selection. Forexample, when the literature wassearched for reported outcomesdata of various chronic wound treat-ment studies, only three pressureulcer protocols of care were found tohave detailed aggregate data on 100wounds or more — representingapproximately 1% of all dressingsavailable at that time.7
The Surveyor Guidance documentdoes not contain specific recommen-dations for practice, beyond discour-aging prolonged use of wet-to-drygauze dressings.2 This recommenda-tion is in agreement with a plethoraof research findings and conclusionsmade by the National Institute onClinical Excellence for the treatmentof difficult-to-heal surgical wounds aswell as the US Food and DrugAdministration Wound Healing Focusgroup that has stated: “Maintenanceof a moist wound environment is agenerally accepted standard of carefor all chronic cutaneous ulcers.”48,49
Although the number of controlledclinical studies to evaluate the effec-tiveness of pressure ulcer manage-ment strategies remains limited, pro-tocols of care that include the use ofa hydrocolloid dressing have beenfound to have improved rates ofhealing as compared to protocols ofcare that include traditional gauze-type dressings.7,50 Thus, an evidence-based protocol of care shouldinclude maintenance of a moistwound environment using a dressingthat has been shown to be safe,effective, and able to maintain amoist environment.
With regard to wound cleansing,procedures should be implementedthat minimize trauma to the wound
yet effectively remove debris, regard-less of the dressing selected. In mostcases, normal saline, delivered withenough pressure to dislodge debris,will accomplish both. The most com-monly recommended methodincludes using a 35-mL syringe witha 19-gauge needle or angiocathwhich delivers 8-psi irrigation pres-sure.29 Specially formulated, non-toxic wound cleansing products areavailable and may be helpful for dis-solving and removing slough adher-ing to the wound bed.
In terms of dressing selection, aparticular selection process that hasbeen found to be valid and providegood outcomes starts with assess-ment of wound exudate amounts,followed by an assessment ofnecrotic tissue and fibrin slough,wound depth, surrounding skin con-dition, and status of the woundedges.8,39 If the wound bed is dry, ahydration product (eg, gel) should beapplied. If the wound is moist, anappropriate moisture retentive dress-ing should be selected. If the woundis wet, an absorption product, suchas a Hydrofiber® dressing(Hydrofiber® is a registered trademarkof E.R. Squibb and Sons, L.L.C.) orcalcium alginate dressing, is used. Amoist wound environment facilitatesthe process of autolytic debridement(the body's own enzymes digest thenecrotic tissue). The principles ofautolytic debridement can be usedfor wounds with limited amounts offibrin slough or necrotic tissue that isnot too dry and/or adherent to theedges of the wound. If this is thecase, sharp/surgical debridementmay be indicated. Limited data areavailable to compare the effective-ness of various debridement meth-ods in the management of pressureulcers. However, the general consen-sus is that stable, dry, adherent, and
15
07-19_Lia.qxd 4/1/05 12:13 PM Page 15

16
intact eschar on the foot/heel shouldnot be debrided unless signs andsymptoms of local infection or insta-bility are detected.2,29
Deep wounds and wounds withundermined edges may benefit fromthe application of a wound filler prod-uct to reduce wound dead space.39
The type of wound filler useddepends on the amount of exudatepresent in the wound. For example, adry deep wound should be managedwith a gel and covered with a mois-ture retentive dressing; whereas, awet wound would benefit from anexudate absorption dressing coveredwith a moisture-retentive dressing.Finally, the condition of the surround-ing skin and wound edges may pro-vide important information about theeffectiveness of the treatment select-ed. Maceration would indicate thatwound exudate has not been man-aged effectively and/or the dressinghas been in place too long (see Table4). Particularly when managing deep,Stage III or Stage IV pressure ulcers,the optimal dressings are likely tochange as healing progresses andwound assessment variables change.
With regard to managing the riskof infection, the Guidance documentcites current literature findings thatinclude the observation that all pres-sure ulcers contain bacteria (are col-onized) but their presence does notmean that the wound is infected.2
Whether bacteria invade the tissuesand cause an infection depends on avariety of factors, including the typeof bacteria, the condition of thewound bed, and the overall health ofthe resident.51 The presence ofnecrotic tissue in the wound increas-es the risk of infection; hence,debridement is a crucial step in thehealing process. Some bacteria aremore virulent and likely to invade tis-sues; whereas, others may become
virulent when combined with, forexample, Escherichia coli.52 Infectionsin acute wounds are relatively easy toassess. Infected acute wounds usuallyexhibit one or more of the followingsymptoms: periwound warmth,swelling, induration or erythema,increasing pain or tenderness, andpurulent exudate.2 In chronic wounds,these symptoms may or may not bepresent; sometimes, the only indica-tion of infection is delayed healing orwound deterioration. Other clinicalsigns of a chronic wound infectionmay include the presence of friablegranulation tissue or a foul odor.53 Aquantitative or semi-quantitative cul-ture may help diagnose an infectionand guide systemic antibiotic treat-ment but the results must be inter-preted with caution. The presence oflarge quantities of some bacteria maybe meaningless; whereas, small quan-tities of a virulent bacterial strain foundin the wound of a resident with acompromised immune status cancause a serious infection and sepsis.52
In addition to addressing theoverall health of the resident, localwound care measures to preventinfection include debridement,wound and periwound skin cleans-ing, prevention of tissue desiccation,and protection of the wound againstcontamination. The latter is particu-larly important in light of evidencerelated to the potential role of E coliin causing infections and the obser-vation that bacteria are frequentlypresent on periwound skin.52,54
The bacterial barrier properties ofsome, but not all, dressings havebeen studied. Clinicians can usuallyfind information about the barrierproperties of a dressing in the prod-uct package insert. With respect toprimary dressings (eg, exudateabsorption products), laboratorystudies suggest that products such
as Hydrofiber® (Hydrofiber® is a reg-istered trademark of E.R. Squibband Sons, L.L.C.) dressings with sil-ver may play a role in managing therisk of infection by absorbing, immo-bilizing, and killing a broad spectrumof wound bacteria in the dressing.55
In summary, wound assessmentrecommendations included in theGuidance document will go a long waytoward helping clinicians identifywounds that may be infected whilemeasures to optimize the resident'soverall health status and wound envi-ronment will help control the invasion ofsurface bacteria and prevent infection.
Additional treatment modalities.The Guidance document does notcontain any recommendations relat-ed to the use of so-called adjunctivetreatment modalities (eg, therapeuticultrasound, growth factors, negativepressure wound therapy). This maybe attributed to the variability inresearch findings using these meth-ods for managing recalcitrantwounds.32 Their use is generally rec-ommended for highly refractivewounds and remains limited to facili-ties that have access to thesemodalities; their effectiveness hasbeen compared to gauze-typedressings only. Data about theireffectiveness compared to acceptedstandards of care using moistureretentive dressings remain sparse.
Goals and Outcomes of Care Results from a recent study, which
showed that the 180-day mortalityrate of long-term care residents whoacquired a pressure ulcer was 67%,56
serve as an important reminder thathealing may not always be the goalof pressure ulcer care. Yet, most rec-ommendations discussed would stillapply when, for example, preventionof deterioration, prevention of infec-tion, or reduction of pain was the
07-19_Lia.qxd 4/1/05 12:15 PM Page 16

goal of care. Gauze-type dressingsnot only delay healing, but they alsodry out the wound bed, require fre-quent (and sometimes painful) dress-ing changes, and fail to protectwounds against contaminants, bac-teria, or viruses.557
If the goal of a resident's plan ofcare is healing, what can/shouldproviders monitoring the ulcerexpect? In addition to expectedchanges in wound area observedafter 2 to 4 weeks of care, the litera-ture provides some insights thatmay help determine whether theresident's plan of care should be re-evaluated. Information from agrouped analysis, using data from519 pressure ulcers of whichapproximately half were Stage II andhalf were Stage III/IV, suggests thatmore than 50% of pressure ulcerscan be expected to be healed after12 weeks of care.7 Specifically, theweighted average proportion ofulcers healed after 12 weeks rangedfrom 41% to 65%, depending onthe type of dressing used. Also, ascan be expected, partial-thickness(Stage II) pressure ulcers heal moreexpediently than full-thickness(Stage III/IV) ulcers. Results fromone large, prospective, longitudinalstudy showed that, using standard-ized assessments and protocols ofcare incorporating moisture-retentivedressings, 61% of Stage II pressureulcers and 36% of Stage III/IV ulcerswere healed after 12 weeks of care.8
In this study, the average time tohealing was 31 days for partial-thickness and 57 days for full-thick-ness pressure ulcers. These num-bers are remarkably similar to earlierreports using a smaller sample sizeon the outcomes of using a hydro-colloid dressing to manage full-thickness pressure ulcers.41 In thisstudy, 37% of ulcers were healed
after an average of 56 days. Mostimportantly, however, data from thisstudy illustrate that healthcareproviders should not wait 2 or 3months to assess the effectivenessof their protocol of care. In this study,ulcers that healed showed a 44%reduction in ulcer area after 2 weeksand a 76% reduction after 4 weeksof care; whereas; ulcers that did notheal had an increase in ulcer sizeafter 2 weeks and a decrease of only17% after 4 weeks of care.41
The Costs of Care Even though costs of care are
not included in the Guidance docu-ment, administrators and cliniciansmay be concerned about the poten-tial costs of implementing the rec-ommendations. The initial costs ofimplementation will vary greatly anddepend on current facility policiesrelated to obtaining products andservices, dietary consults and sup-plements, and resident skin andwound assessment procedures. Inaddition, administrator and stafftime to review and update existingpolicies and procedures may be sig-nificant. Furthermore, the purchaseprice of moisture-retentive dressingsis higher than the price of gauzeand for some facilities the costs ofbuying or renting support surfacesalso may increase. However, the ini-tial increased costs are most likelyto be offset by substantial cost sav-ings after the recommendationshave been implemented. For exam-ple, although the costs of supportsurfaces and skin protection prod-ucts may be high, use of a validatedprediction tool and protocol of carewill reduce the incidence of pres-sure ulcers and their associatedcosts of care. In one long-term carestudy,4 implementation of such aprevention protocol was found to
cost an average of $ 519.73 permonth but the incidence of newulcers decreased from 13.2% to1.7%. Because the cost to treatone pressure ulcer may be morethan $50,000,58 optimal preventionprotocols will save money.
With respect to treatment proto-cols, caregiver time has been foundto be more costly than the purchaseprice of products used and totalcosts of care are determined by theoutcomes.4,7,59,60 In one study7 thatused published outcomes data from102 pressure ulcers managed withgauze-type dressings and 281ulcers managed with one type ofhydrocolloid dressing, it was calcu-lated that the average cost perpatient healed was $2,179 for gauzeprotocols of care compared to $910for the hydrocolloid dressing, eventhough the average purchase priceof gauze was three times lower thanthe price of the hydrocolloid dress-ing. The reduced rates of healingand increased labor costs whenusing gauze make this seeminglyinexpensive product costly to use.
Thus, Guidance document rec-ommendations to limit the use ofwet-to-dry type dressings and moni-tor wound outcomes are likely toreduce the overall costs of care.Instead of using caregiver time tochange dressings one, twice, oreven three times a day, caregiverswill simply monitor the dressing andthe wound once a day. Most mois-ture-retentive dressings are changedonce every 3 to 7 days, at whichtime a complete wound assessmentcan be completed. The latter helpscaregivers intervene promptly if thewound is not exhibiting signs ofhealing. This approach will helpreduce the overall costs of care sim-ply because ineffective care isalways expensive.
17
07-19_Lia.qxd 3/29/05 4:48 PM Page 17

18
ConclusionPressure ulcer prevention and care
remain a challenge throughout thehealthcare system and especially forall long-term care providers. The newGuidance to Surveyors documentcontains many suggestions that mayhelp facilities develop and adoptappropriate policies and proceduresthat may improve outcomes andreduce their costs of care. Althoughmuch remains to be learned aboutthe prevention and treatment ofthese wounds, evidence to substan-tiate safe and effective protocols ofcare has increased substantially dur-ing the past few decades.Fortunately, the most substantialimprovements healthcare providerscan make do not require expensiveequipment or technology. Rather,meticulous assessments, team work,an understanding of the underlyingcause of these wounds and thewound healing process and a holisticapproach to the care of residentswith limited mobility will improve careand reduce costs.
References1. Cuddigan J, Ayello EA, Sussman C,
Baranoski S, eds. Pressure Ulcersin America: Prevalence, Incidence,and Implications for the Future.National Pressure Ulcer AdvisoryPanel (NPUAP) Monograph.NPUAP, Reston, Va. 2001.
2. Centers for Medicare and MedicaidServices. CMS Manual System,Pub.100-07 State Operations,Provider Certification. DepartmentHealth and Human Services, 2004:November 12, 2004.
3. Panel for the : Prediction andPrevention of Pressure Ulcers inAdults. Pressure ulcers in adults:prediction and prevention. AHCPRPublication No.92-0047. Rockville,Md. Agency for Health Care Policyand Research, US Department ofHealth and Human Services. 1992.
4. Lyder CH, Shannon R, Empleo-Frazier O, McGeHee, D, White C. A
comprehensive program to preventpressure ulcers in long-term care:exploring costs and outcomes.Ostomy Wound Manage.2002;48(4):52–62.
5. Xakellis GC, Frantz RA, Lewis A,Harvey P. Cost-effectiveness of anintensive pressure ulcer preventionprotocol in long term care. AdvWound Care. 1998;11:22–29.
6. Regan MB, Byers PH, MayrovitzHN. Efficacy of a comprehensivepressure ulcer prevention programin an extended care facility. AdvWound Care. 1995;8(3):51–55.
7. Kerstein MD, Gemmen E, vanRijswijk L, et al. Cost and costeffectiveness of venous and pres-sure ulcer protocols of care. DisManage Health Outcomes.2001;9(11):651–663.
8. Bolton LL, McNees P, van RijswijkL, et al. Wound healing outcomesusing standardized assessmentand care in clinical practice.JWOCN. 2004;31(2):65–71.
9. Lyder C, van Rijswijk L. Preventingand managing pressure ulcers inlong-term care: An overview of therevised federal regulation. OstomyWound Manage.2005;51(4suppl);2–6.
10. Alvarez OM, Meehan M, Ennis W,et al. Chronic wounds: palliativemanagement for the frail popula-tion. WOUNDS.2002;14(8):5S–27S.
11. Maklebust JA, Braden B.Computer-based testing of theBraden Scale for PredictingPressure Sore Risk. OstomyWound Manage. 2005;51(4):40–52.
12. van Rijswijk L. Frequency ofreassessment of pressure ulcers.In: Proceedings National PressureUlcer Advisory Panel meeting onpressure ulcer healing. Adv WoundCare. 1995;8(4):28/1928/24.
13. van Rijswijk L. Epidemiology. In:Morrison M, ed. The Preventionand Treatment of Pressure Ulcers.New York, NY: Mosby;2001.
14. Bergstrom N, Braden B. Aprospective study of pressure sorerisk among institutionalized elderly.J Am Geriatr Soc.1992;40:747–758.
15, Braden BJ, Bergstrom N. Riskassessment and risk-based pro-grams of prevention in various set-tings. Ostomy Wound Manage.
1996;42(10A):6S–12S.16. Lyder, C. Pressure ulcer prevention
and management. In: Archibold P,Stewart B, eds. Annual Review ofNursing Research. 2002:3561.
17. Bergstrom N, Braden BJ, LaguzzaA, Holman V. The Braden Scale forPredicting Pressure Sore Risk. NursRes. 1987;36(4):205210.
18. Lyder CH, Preston J, Grady JN,Scinto J, et al. Quality of care forhospitalized Medicare patients atrisk for pressure ulcers. Arch InternMed. 2001;161:1549–1554.
19. Kennedy K. The prevalence ofpressure ulcers in an intermediatecare facility. Decubitus.1989;2(2):44–45.
20. Mathus-Vliegen E. Nutritional sta-tus, nutrition, and pressure ulcers.Nutrition in Clinical Practice.2001;16:286–291.
21. Defloor T. Less frequent turningintervals and yet less pressureulcers. Tijdschr voor Gerontol enGeriatr. 2001;32(4):174–177.
22. Cullum N, McInnes E, Bell-SyerSEM, Legood R. Support surfacesfor pressure ulcer prevention(Cochrane Review). In: TheCochrane Library, Chichester, UK:John Wiley & Sons, Ltd; Issue 3,2004.
23. Maklebust JA. An update on hori-zontal patient support surfaces.Ostomy Wound Manage.1999;45(1A suppl):70S–77S.
24. Ochs, RF, Horn, SD, van Rijswijk, L,Pietsch, C, Smout, RJ. Comparisonof air-fluidized therapy with othersupport surfaces used to treatpressure ulcers in nursing homeresidents. Ostomy Wound Manage.2005;51(2)38–68.
25. Sprigle S. The NPUAP SupportSurface Standards Initiative.Ostomy Wound Manage.2004;50(8):6–8.
26. Harris CL, Fraser C. Malnutrition inthe institutionalized elderly: theeffects on wound healing. OstomyWound Manage.2004;50(10):54–63.
27. Horn SD, Bender SA, FergusonML, et al. The national pressureulcer long-term care study: pres-sure ulcer development in long-term care residents. JAGS.2004;52(3):359-–67.
28. Lyder CH. Perineal dermatitis in theelderly. A critical review of the litera-
07-19_Lia.qxd 3/29/05 4:49 PM Page 18

ture. J Gerontol Nurs.1997:23(12):5–10.
29. Wound Ostomy Continence NursesSociety. Guideline for preventionand management of pressureulcers. Glenview, Ill.;2003.
30. Kirsner RS, Froelich CW. Soapsand detergents: understanding theircomposition and effect. OstomyWound Manage.1998;44(3A):62S–70S.
31. Hoggarth A, Waring M, AlexanderJ, Greenwood A, Gallaghan T. Asingle-blind, single centre, three-part trial to investigate the barrierfunction and moisturizing propertiesof five skin protectant products.Ostomy Wound Manage. In press.
32. Lyder, C. Exploring pressure ulcerprevention and management.JAMA. 2003;289: 223–226.
33. Lyder, C. Pressure ulcers. In:American Geriatrics Society, ed.Geriatrics Review Syllabus: A CoreCurriculum in Geriatric Medicine,6th ed. New York, NY: AmericanGeriatrics Society. In press.
34. Sieggreen MY, Kline RA.Recognizing and managing venousleg ulcers. Adv Skin Wound Care2004;17(6):302–311.
35. American Diabetes Association.Consensus development confer-ence on diabetic foot wound care.Diabetes Care.1999;22(8):1354–1360
36. van Rijswijk L, Braden B. Pressureulcer patient and wound assess-ment: an AHCPR clinical practiceguideline update. Ostomy WoundManage.1999;45(suppl.1A)56S–67S.
37. Bates-Jensen B. Indices to includein wound healing assessment. AdvWound Care. 1995;8:25–33.
38. National Pressure Ulcer AdvisoryPanel. PUSH tool. Available at:http://www.npuap.org. AccessedDecember 12, 2004.
39. Beitz JM, van Rijswijk L. Usingwound care algorithms: a contentvalidation study. JWOCN.1999;26:238–249.
40. Bates-Jensen B. The Pressure SoreStatus Tool a few thousand assess-ments later. Adv Wound Care.1997;109(5):65–73.
41. van Rijswijk L. Full-thickness pres-sure ulcers: patient and woundhealing characteristics. Decubitus.1993;6:16–21.
42. Margolis DJ, Gross EA, Wood CR,Lazarus GS. Planimetric rate ofhealing in venous ulcers of the legtreated with pressure bandage andhydrocolloid dressing. J Am AcadDermatol. 1993;28:418–421.
43. Dallam L, Smyth C, Jackson BS, etal. Pressure ulcer pain: assessmentand quantification. JWOCN.1995;22:211–218.
44. Krasner D. The chronic wound painexperience: a conceptual model.Ostomy Wound Manage.1995;41(3):20–27.
45. Madden M, Nolan E, Finkelstein JL,et al. Comparison of an occlusiveand a semi occlusive dressing andthe effect of the wound exudateupon keratinocyte proliferation. JTrauma. 1989;29(7):924–930.
46. Nemeth AJ, Eaglstein WH, TaylorJR, Peerson LJ, Falanga V. Fasterhealing and less pain in skin biopsysites treated with an occlusivedressing. Arch Dermatol.1991;127:1679–1683.
47. Szor JK, Bourguignon C.Description of pressure ulcer painat rest and at dressing change.JWOCN. 1999;26:115–120.
48. National Institute for ClinicalExcellence (N.I.C.E). Guidance onthe use of debriding agents andspecialist wound care clinics for dif-ficult to heal surgical wounds.Technology Appraisal GuidanceNo.24. April 2001. Available at:http://www.nice.org.uk/pdf/wound-careguidance.pdf. AccessedAugust 1, 2002.
49. US Department of Health andHuman Services, Food and DrugAdministration. Guidance forIndustry: Chronic cutaneous ulcerand burn wounds: developingproducts for treatment. June 2000.Available at:http://www.fda/cber/guidelines.htm. Accessed: August 2, 2002.
50. Bradley M, Cullum N, Nelseon EA,et al. Systematic reviews of woundcare management (2) Dressingsand topical agents used in the
healing of chronic wounds. HealthTechnology Assessment.1999;3(17), Pt.2. Available at:http:// www.cochrane.org.Accessed January 2, 2005.
51. McGuckin MM, Goldman R, BoltonL, Salcido R. The clinical relevanceof microbiology in acute and chron-ic wounds. Adv Skin Wound Care.2003;16:12–25.
52. Bowler PG. The 105 bacterialgrowth guideline: reassessing itsclinical relevance in wound healing.Ostomy Wound Manage.2003;49(1):44–53.
53. Gardner SE, Frantz RA, DoebbelingBN. The validity of the clinical signsand symptoms used to identifylocalized chronic wound infection.Wound Rep Regen.2001;9:178–186.
54. Konya C, Sanada H, Sugama J etal. Skin debris and micro-organ-isms on the periwound skin ofpressure ulcers and the influence ofperiwound cleansing on microbialflora. Ostomy Wound Manage.2005;51(1):50–59.
55. Bowler PG, Jones SA, Walker M,Parrons D. Microbicidal propertiesof a silver-containing hydrofiberdressing against a variety of burnpathogens. J Burn Care Rehabil.2004;25:192–196.
56. Brown, G. Long-term outcomes offull-thickness pressure ulcers: heal-ing and mortality. Ostomy WoundManage. 2003;49(10):42–50.
57. Ovington, LG. Hanging wet-to-drydressings out to dry. Home HealthcNurse. 2001;19(8):477–483.
58. Pompeo MQ. The role of “woundburden” in determining the costsassociated with wound care.Ostomy Wound Manage.2001;47(3):65–71.
59. Xakellis GC, Chrischilles, EA.Hydrocolloid versus saline-gauzedressings in treating pressureulcers: a cost effectiveness analy-sis. Arch Phys Med Rehab.1992;73:463–469.
60. Bolton LL, van Rijswijk L, ShafferFA. Quality wound care equalscost-effective wound care: a clinicalmodel. Nurs Manage.1996;27(7):30,32–33,37.
19
07-19_Lia.qxd 3/29/05 4:49 PM Page 19

The ConvaTec Line of Skin Care Products…
Helping Skin Win!®
© 2005 E. R. Squibb & Sons, L.L.C. March 2005 US-05-333 CVT0052
Helping Skin to Win, Solutions, Aloe Vesta and Sensi-Care are registered trademarks of E.R. Squibb & Sons, L.L.C.
Appropriate skin care can help reduce the incidence of pressure ulcers1
• A clinical study conducted by Yale University
researchers using the Solutions® validated
protocols of care and ConvaTec skin care
products demonstrated a reduction in the
incidence of pressure ulcers by up to 87%1*
• Our comprehensive prevention program—including the ConvaTec skin care line—may actually help prevent skin breakdown
The product line that benefits both patients and nurses
• ConvaTec offers a wide range of quality
products specially formulated for at-risk skin
• Our new skin care packaging helps caregivers
meet each patient’s needs by following the
new convenient numbering system
- 1 and 2 for routine bathing and moisturizing
- 1 for incontinence cleansing, 2 for skinmoisturizing, and 3 for incontinenceprotection
• Each product is easy to use, helping to
reduce nursing time
• A reduction in incidence of skin breakdown
results in more cost-effective care
*Study conducted at two long-term care facilities where incidence of pressure ulcers was reduced from 13.2% to 1.7% and from 15.0% to 3.5%,respectively, following implementation of Solutions ® standardized protocols of care.
Reference: 1. Lyder CH, Shannon R, Empleo-Frazier O, McGeHee D, White C. A comprehensive program to prevent pressure ulcers in long-term care:exploring costs and outcomes. Ostomy Wound Manage. 2002;48:52-62.
US-05-417
ConvaTec_SkinCare_0405.qxd 4/1/05 12:06 PM Page 1