presented by: jennifer birt, ot reg(mb)csmc.ca/docs/archives/2013_archive/hnd/ws 13 best practices...
TRANSCRIPT

Presented By: Jennifer Birt, OT Reg(MB)Specialized Seating & Mobility
Clinical Specialist© 2013

1. Define and understand the concept of practical pressure management and categorizing individuals at different levels of risk from a practical perspective
2. Identify a minimum of 6 factors that commonly contribute to pressure ulcer development from a 24 hour perspective
3. Identify a minimum of 4 assessment techniques that can be utilized when evaluating these pressure factors
4. List a minimum of 4 recommendations guided by best practice to resolve these pressure factors
© Jennifer Birt 2013

© Jennifer Birt 2013

© Jennifer Birt 2013

© Jennifer Birt 2013

© Jennifer Birt 2013

© Jennifer Birt 2013

© Jennifer Birt 2013

Occipu t
Scapulae
Sacrum
Coccyx
Greater Trochanter
Ischial Tuberosity
Epicondyle
Spinous Processes
Malleolus & Heel
Elbow
© Jennifer Birt 2013

General CPG’s
Winnipeg Regional Health Authority (WRHA) updated 2012
Registered Nurses of Ontario (RNAO) updated 2011 & 2007
National Pressure Ulcer Advisory Panel/European Pressure Ulcer Advisory Panel (NPUAP/EPUAP) 2009
Canadian Association of Wound Care (CAWC) updated 2006
SCI-Specific CPG’s
Rick Hansen Institute (RHI) 2013
Spinal Cord Injury Rehabilitation Evidence (SCIRE) updated 2009
New South Wales Agency for Clinical Innovation (NSW ACI) 2008
Paralyzed Veterans of America (PVA) 2000
© Jennifer Birt 2013

© Jennifer Birt 2013

© Jennifer Birt 2013
© Jennifer Birt 2013

What makes OT’s key clinicians in the role of practical pressure management?
Applying pressure management best practices into the functional context of
an individual’s daily life and environment
Holistic (24 hour) approach Adaptive approach
Activity analysis Assistive device & equipment specialists
Practical Problem solving P-E-O Model
© Jennifer Birt 2013

Cognitive Issues
© Jennifer Birt 2013
PURPOSE
To provide a clinical evaluation tool, based on best practice, that offers a systematic way of evaluating pressure management from a practical perspective
The PMAT provides a structural framework that investigates the causative factors that contribute to the functional aspects of pressure ulcer development from a 24 hour perspective
© Jennifer Birt 2013

Working knowledge of clinical practice guidelines for pressure ulcer prevention & treatment
Working knowledge of pressure ulcer stages as well as additional signs & symptoms of pressure-related damage to skin
Ability to reliably landmark and palpate key bony areas that are most susceptible to pressure-related damage in a variety of positions
Working knowledge of proper support surface terminology and principles
Awareness of pressure-posture relationship
Understand team roles in addition to your own role
© Jennifer Birt 2013

© Jennifer Birt 2013

© Jennifer Birt 2013

REFERRAL TO OCCUPATIONAL THERAPYDiagnosis: • Multiple Sclerosis
Associated medical
conditions:
• Spasticity• Incontinence
Pressure Issue identified:
• Skin breakdown on “buttocks”
Other issues flagged:
• Sliding in the wheelchair
• Postural deformities
Purpose of Referral:
• Needs a cushion • Needs a seating
assessment
Client ‘X’
© Jennifer Birt 2013

© Jennifer Birt 2013

© Jennifer Birt 2013

© Jennifer Birt 2013

© Jennifer Birt 2013

© Jennifer Birt 2013

© Jennifer Birt 2013

© Jennifer Birt 2013

© Jennifer Birt 2013

© Jennifer Birt 2013

© Jennifer Birt 2013

© Jennifer Birt 2013

FUNCTIONAL WOUND EVALUATION
• Visual inspection of skin over primary weight bearing surfaces
• Remove dressings whenever possible – involve nursing
• Side lying in “mocked” sitting position
• Rule of thumb when evaluating wounds:
• What do you see?• What do you feel?• What do you smell?
• Understand signs of pressure, shear, friction, & microclimate
• Digital photos
© Jennifer Birt 2013

© Jennifer Birt 2013

© Jennifer Birt 2013

POSITIONING EVALUATION
• Palpation to correlate ulcer with each position
• Evaluate whether pressure ulcer is weight bearing, partial weight bearing, or fully offloaded for:
• All positions, on• All support surfaces• 24 hour perspective
• Mock up modified and/or additional positions with client as alternative solutions
• Understand PRESSURE- POSTURE relationship
© Jennifer Birt 2013

© Jennifer Birt 2013

POSTURAL SCREEN IN SITTING
• PRESSURE-POSTURE relationship
• What happens in the wheelchair is a good indication of what will happen on other sitting surfaces
• Influence of gravity• Bodies will go in 3 general
directions under the influence of gravity:
• Anterior• Posterior• Lateral
© Jennifer Birt 2013

© Jennifer Birt 2013

REPOSITIONING EVALUATION
• Evaluation of repositioning movements in:
• Bed• Wheelchair• Other sitting surfaces
• Goal is to determine whether:
• Client is capable of the movement
• Movement is effective• Palpate ulcer area during
movement to decide:• Effective offloading?• Shear, friction or trauma
during movement?
© Jennifer Birt 2013

© Jennifer Birt 2013

SUPPORT SURFACE EVLAUTION
• Visually inspect every support surface used over a 24 hour period
• Ensure equipment is:• Set up properly• In good condition
• Understand impact of support surface on:
• Stability• Microclimate• Shear & friction• Function
• Support surface performance may change when position changes
• Correlate ulcer location to support surface features
© Jennifer Birt 2013

© Jennifer Birt 2013

MOBILITY, FRICTION & SHEAR EVALUATION
• Watch transfer and repositioning movements and screen for signs of:
• Trauma• Shear & friction
• Palpate ulcer area during transfer and repositioning movements
• Mock up alternative methods of movement
• Confirm trauma, shear & friction are eliminated or minimized with alternative methods
© Jennifer Birt 2013

© Jennifer Birt 2013

COGNITIVE SCREEN
• Indirect evaluation gathered from Part 1 & 2 results
• Appropriate pressure management requires:
• Insight & awareness• Problem solving• Motivation• Ability to retain
information and apply new learning
• Sometimes people make BAD lifestyle choices and decisions
© Jennifer Birt 2013

© Jennifer Birt 2013

© Jennifer Birt 2013

TOP 10 TIPS FOR PROVIDING PRACTICAL RECOMMENDATIONS
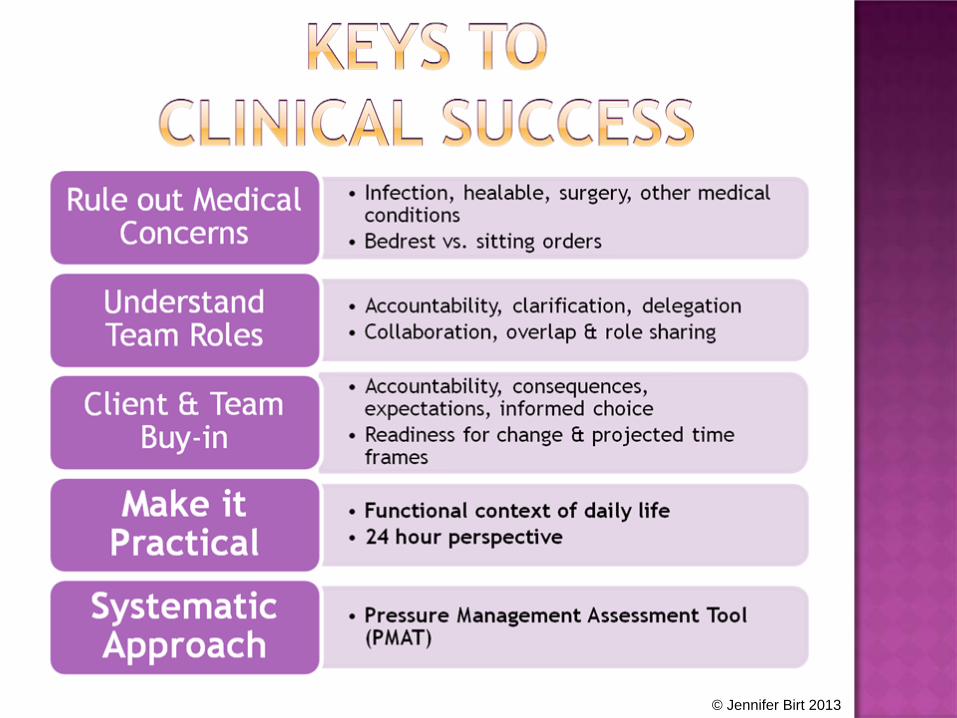
1 Initiate consult to physician for unresolved medical concerns
2 Initiate cross referrals as indicated & at transition points in care
3 Clarify & collaborate regarding bedrest vs. sitting orders
4 Prioritize repositioning schedules & support surface use based on bedrest vs. sitting orders
5 Prioritize what to do for the interim vs. long-term
6 Prioritize interventions for essential functional tasks: eating, sleeping, toileting & bathing
7 Think outside the box for practical solutions to these core tasks
8 Frame recommendations to create clear expectations & accountability
9 Provide clients with the opportunity to choose whether or not they will follow recommendations
10 Be clear on trade-offs & consequences if clients choose not to follow recommendations
© Jennifer Birt 2013

RECOMMENDATIONS
1 Pressure ulcer should be offloaded 100% of the time to help determine capacity to heal
2 Recommend medical re-evaluation for:(a) Ruling out need for surgical intervention(b) Spasticity management
3 Recommend a period of bedrest for 4-6 weeks if appropriate therapeutic sleep surface and repositioning schedule can be implemented to allow for full offloading
4 Upgrade to a low air loss mattress
5 Alternate client’s position in bed between right and left side-lying; rotate 30 degrees over from supine and use a wedge to maintain this angle, and place pillows between knees and feet
6 Due to low tolerance in side-lying positions, initiate a turning schedule every hour to start and gradually build to 2 hours as tolerance increases
© Jennifer Birt 2013

RECOMMENDATIONS
7 Check skin after each turn in bed to evaluate tissue tolerance over weight bearing areas – gradually increase turn intervals by 1 hour each week based on tissue response
8 Consult Home Care about increasing frequency of services to facilitate bed rest and turning schedule during the day
9 Use a slider sheet for repositioning in bed and remove after repositioning occurs
10 Use an alarm clock overnight to implement turning schedule and consult to Home Care to problem-solve day time turns
11 Evaluate client in side-lying with the head of the bed raised to 30 degrees as an alternative position to eat meals while on bed rest; place a wedge under knees in this position to minimize sliding and do not stay in this position any longer than 1 hour
© Jennifer Birt 2013

RECOMMENDATIONS
12 Consult to nursing about alternative solutions for bladder management – catheter good or bad idea? Consult to Home Care about increasing frequency of brief changes
13 Eliminate use of soaker pads on sleep surface especially if briefs cannot be discontinued
14 Consult to nursing about bowel management for bed rest
15 Provide education to client’s husband about performing skin checks and proper methods for assisting with bed mobility & bed positioning
16 Consult to dietitian re: intake requirements; additional consult to Home Care to assist with meal provision during the day
17 If client demonstrates wound healing after 4-6 weeks and no further medical interventions are required, re-initiate seating consult and re-evaluate mobility & function on sitting surfaces
© Jennifer Birt 2013

© Jennifer Birt 2013

Ontario Neurotrauma Foundation (ONF): www.onf.org (can download Canadian Best Practice Guidelines for SCI Pressure Ulcer Prevention & Treatment)
Winnipeg Regional Health Authority (WRHA): www.wrha.mb.ca (‘for health professionals’ ‘evidence informed practice tools’ ‘wound care’ ‘pressure ulcer’
Registered Nurses of Ontario (RNAO): www.rnao.ca
International review. Pressure ulcer prevention: pressure, shear, friction and microclimate in context. A consensus document. London: Wounds International, 2010.
National Pressure Ulcer Advisory Panel (NPUAP): www.npuap.org
Spinal Cord Injury Rehabilitation Evidence (SCIRE): www.scireproject.com
New South Wales Agency for Clinical Innovation (Spinal seating online education program, module 8): www.aci.health.nsw.gov.au/networks/spinal-seating
Canadian Association of Wound Care (CAWC): www.cawc.net
Wound Care Canada (Official publication of CAWC): www.woundcarecanada.ca
Paralyzed Veterans of America (PVA): www.pva.org© Jennifer Birt 2013

1. Define and understand the concept of practical pressure management and categorizing individuals at different levels of risk from a practical perspective
2. Identify a minimum of 6 factors that commonly contribute to pressure ulcer development from a 24 hour perspective
3. Identify a minimum of 4 assessment techniques that can be utilized when evaluating these pressure factors
4. List a minimum of 4 recommendations guided by best practice to resolve these pressure factors
© Jennifer Birt 2013

PLEASE PLEASE
REMEMBER REMEMBER TO VISIT THE TO VISIT THE
EXHIBIT EXHIBIT HALL HALL

Jennifer Birt, OT Reg(MB)Specialized Seating and Mobility
Clinical Specialist(p) 204-787-4266(f) 204-787-8637
Email: [email protected]