presented by: dr/ gamal adel.. for non cardiac surgery tetralogy of fallot
TRANSCRIPT

presented by: Dr/ Gamal Adel
.. For non cardiac surgery
TETRALOGY OF Fallot

Case I
• A 4 years old female with uncorrected Tetrology of Fallot, was to be operated upon for fronto-parietal SOL in the brain with associated midline shift .
• Examination showed pulse:97/min; BP: 135/81mmHg; RR:20/min; SpO2:89-92% with O2 mask at 2L/min.
• Patient’s ECG showed
normal sinus rhythm with tachycardia, T-wave inversions in lead III and V1, strain pattern in anterior chest leads, right ventricular hypertrophy.
• Physical examination
detected Clubbing in both hands, mild peripheral and central cyanosis.
• The development of convulsions, focal neurologic abnormalities or clinical symptoms and signs of raised ICP are the alarming signs of presence of..
Brain abscess

Approach ….
1. Define cardiovascular pathology
2. Predict pathophysiology
3. Determine haemodynamic goals
4. Anticipate emergency treatments

• Pathophysiological classification of congenital heart disease
- Shunt lesions
- Mixing lesions
- Obstructive lesions
- Regurgitation lesions

- Assess functional status - daily activities - exercise tolerance
- ↓ cardiac reserve - cyanosis - respiratory distress with feeding
- Dyspnea- Fainting attack- Fatigue- Palpitations- chest pain- Syncope - Abdominal fullness- Leg swelling- Medications
Vital signs Airway abnormality Associated extracardiac
congenital anomalies Tachypnea, dyspnea, cyanosis Squatting Clubbing of digits Heart murmur (s) CHF:
- Jugular venous distention.
- Hepatomegally
- Ascitis
- Peripheral edema
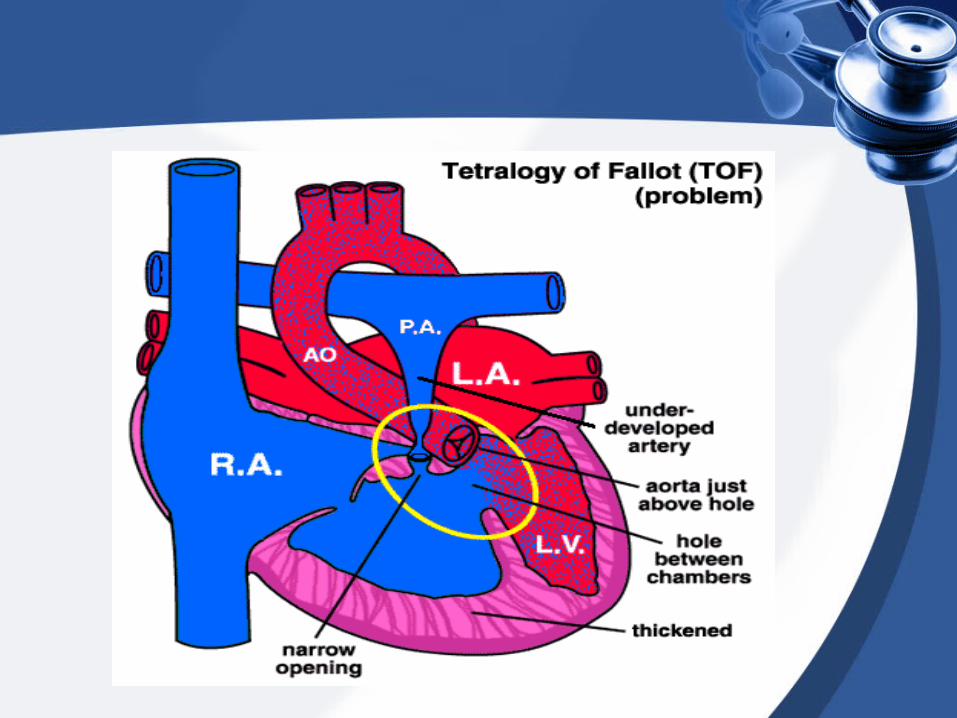
Pathophysiology of Fallot’s tetralogy :
Essentially :
1. severe RVOT obstruction plus
2. nonrestrictive VSD
With anatomic consequences of:
1. RVH
2. Overriding aorta
And physiologic consequences of :
1. Rt to Lt shunt
2. Diminished pulmonary blood flow
..Shunt lesions.. (continued)
Rt-to-Lt shunt• Most common cyanotic lesion
• NB: cyanosis plus quiet heart
• Diminished pulmonary blood flow
• Hypercyanotic “tet” spells
-↓ Pulmonary blood flow = hypoxemia
- Pressure overload of the Rt. ventricle

Preoperative Anesthetic Management:
A- History
B- physical examination
C- Investigations
D- Premedications
E- Fasting Guidelines

INVESTIGATIONSINVESTIGATIONS
MRI
Laboratory Evaluation
Cardiac Catheterization
12 Lead ECG
Echocardiography chest X – Ray


Preoperative Anesthetic Considerations
1- Complete history and physical examination.
2- Review investigations.
3- Hydration should be maintained ??
4- Premedication should be given to patients
at risk for right to left shunt ??
5- Antibiotic prophylaxis against endocarditis must be given ??

Continuing Education in anesthesia, Critical care & Pain | Volume 12 Number 1 - 2012
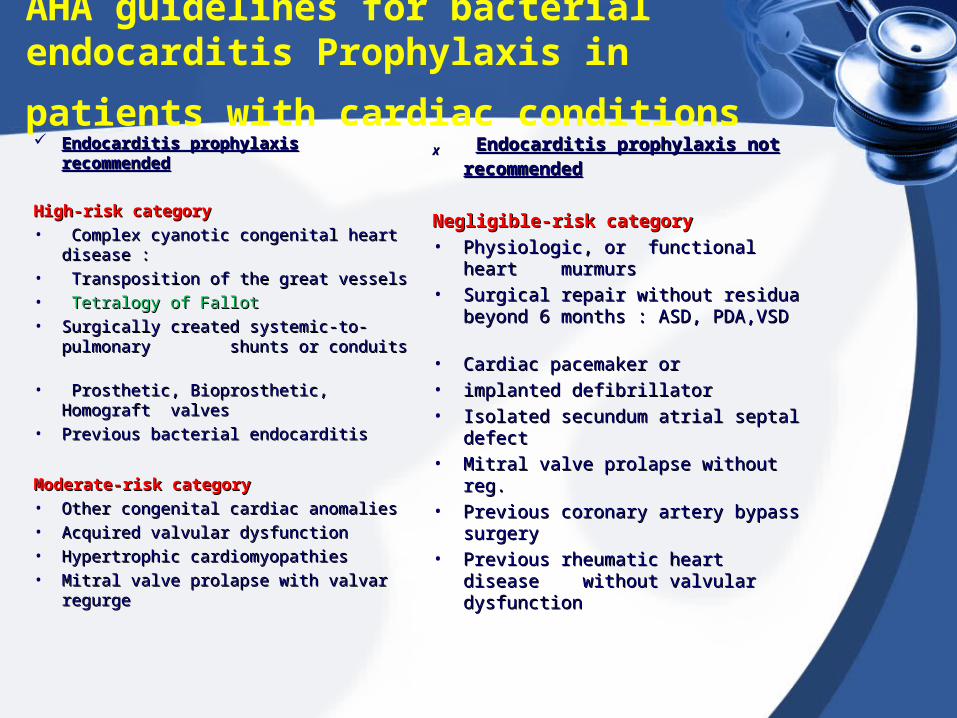
AHA guidelines for bacterial endocarditis
Prophylaxis in patients with cardiac conditions Endocarditis prophylaxis Endocarditis prophylaxis
recommendedrecommended
High-risk category High-risk category • Complex cyanotic congenital heart Complex cyanotic congenital heart
disease :disease :• Transposition of the great vessels Transposition of the great vessels • Tetralogy of Fallot Tetralogy of Fallot • Surgically created systemic-to-Surgically created systemic-to-
pulmonary shunts or conduits pulmonary shunts or conduits • Prosthetic, Bioprosthetic, Homograft Prosthetic, Bioprosthetic, Homograft
valvesvalves• Previous bacterial endocarditis Previous bacterial endocarditis
Moderate-risk categoryModerate-risk category• Other congenital cardiac anomaliesOther congenital cardiac anomalies• Acquired valvular dysfunctionAcquired valvular dysfunction• Hypertrophic cardiomyopathiesHypertrophic cardiomyopathies• Mitral valve prolapse with valvar regurgeMitral valve prolapse with valvar regurge
XX Endocarditis prophylaxis not Endocarditis prophylaxis not
recommendedrecommended
Negligible-risk categoryNegligible-risk category• Physiologic, or functional heart Physiologic, or functional heart
murmursmurmurs• Surgical repair without residua Surgical repair without residua
beyond 6 months : ASD, PDA,VSD beyond 6 months : ASD, PDA,VSD
• Cardiac pacemaker or Cardiac pacemaker or • implanted defibrillatorimplanted defibrillator• Isolated secundum atrial septal Isolated secundum atrial septal
defectdefect• Mitral valve prolapse without reg. Mitral valve prolapse without reg. • Previous coronary artery bypass Previous coronary artery bypass
surgerysurgery• Previous rheumatic heart disease Previous rheumatic heart disease
without valvular dysfunction without valvular dysfunction

AHA guideline for antibiotic prophylaxis for genitourinary procedures:
- High risk Child patient:
Ampicillin 50 mg/kg & gentamicin 1.5 mg/kg IM or IV
- High risk child allergic to penicillin:
Vancomycin 20 mg/kg i.v bolus

Premedication
• Oral Premedication: - Midazolam 0.25 -1.0 mg/kg - Ketamine 2 - 4 mg/kg
• IV Premedication: - Midazolam 0.02 - 0.05 mg/kg titrated in small increments - Ketamine 1-2 mg/kg
• IM Premedication: - Uncooperative or unable to take orally
- Ketamine 5 – 10 mg/kg - Midazolam 0.2 mg/kg
N.B. Propranolol should be continued up to and including the day of surgery

Anesthetic Management
A - Preoperative Management
B - Intraoperative Management :
1- Monitoring
2- Choice of anesthetic agent
3- Maintenance of anesthesia
4- Emergence from anesthesia

• Anesthesia was induced with :
- Thiopentone sodium (4mg/kg)
- Fentanyl (2microgram/kg)
- Atracurium (0.5mg/kg)
• Preoperative antibiotics :
- Cefazoline and Vancomycin.

Monitoring
Non-invasive• Clinical observation.• ECG • NIBP• Pulse oximetry on two different
limbs. • Precordial stethoscope• Continuous airway manometry. • Multiple site temperature
measurement.
Invasive• Volumetric urine
collection. • Arterial catheterization • CVP• PAC• TEE

Choice of anesthetic Regimen
Development of anesthetic regimen is
based on various factors such as:
- Presence and direction of shunts.
- HF.
- Arrhythmia.
- Pulmonary circulation and lowering or maintenance of PVR.

• Inhalational anaesthetic (Isoflurane) was given at 1-1.5% with 100% O2. At the same time systemic venous resistance (SVR) was maintained by using intravenous phenylephrine boluses. (As, reduction in SVR increases right to left shunt). In addition patient was kept adequately hydrated in order to avoid hypotension.
• Blood loss during the procedure was 450ml which was replaced with equal amount of packed cells.

Tetralogy Of Fallot =Maintain adequate tissue oxygenation
• Avoid increasing O2 demand.
• Maintain SVR, systemic BP.• Minimize PVR.• Avoid dehydration especially if polycythemic• Oral premedication/induction(midazolam +
ketamine).• Since patient had VSD with right to left shunt
so all the intravenous lines were kept air free to prevent paradoxical air embolism.
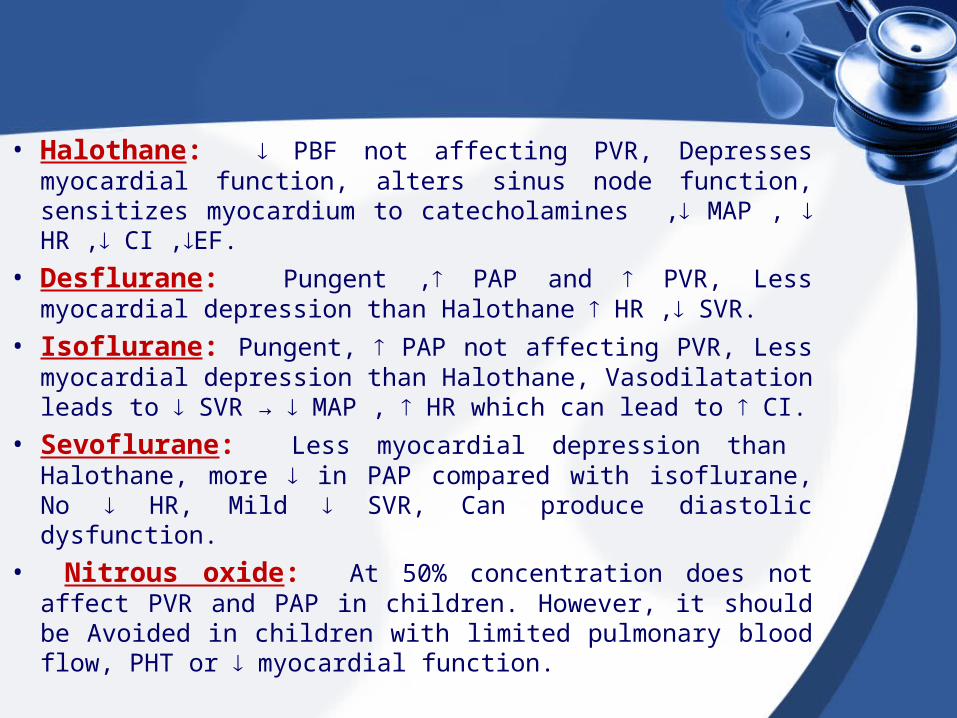
• Halothane: PBF not affecting PVR, Depresses myocardial function, alters sinus node function, sensitizes myocardium to catecholamines , MAP , HR , CI ,EF.
• Desflurane: Pungent , PAP and PVR, Less myocardial depression than Halothane HR , SVR.
• Isoflurane: Pungent, PAP not affecting PVR, Less myocardial depression than Halothane, Vasodilatation leads to SVR → MAP , HR which can lead to CI.
• Sevoflurane: Less myocardial depression than Halothane, more in PAP compared with isoflurane, No HR, Mild SVR, Can produce diastolic dysfunction.
• Nitrous oxide: At 50% concentration does not affect PVR and PAP in children. However, it should be Avoided in children with limited pulmonary blood flow, PHT or myocardial function.
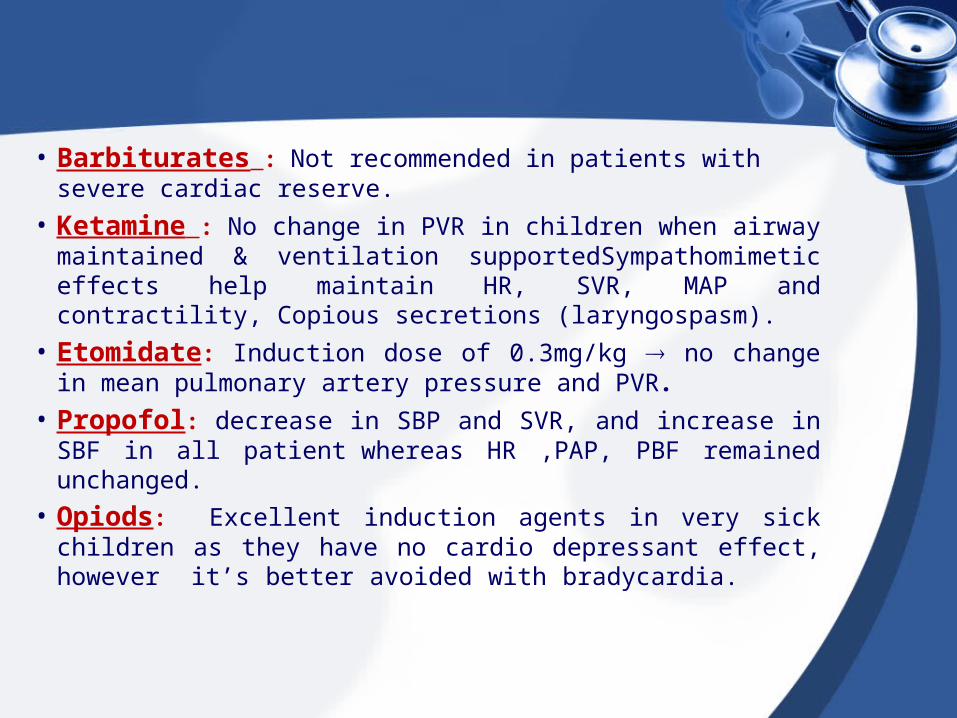
• Barbiturates : Not recommended in patients with severe cardiac reserve.
• Ketamine : No change in PVR in children when airway maintained & ventilation supportedSympathomimetic effects help maintain HR, SVR, MAP and contractility, Copious secretions (laryngospasm).
• Etomidate: Induction dose of 0.3mg/kg no change in mean pulmonary artery pressure and PVR.
• Propofol: decrease in SBP and SVR, and increase in SBF in all patient whereas HR ,PAP, PBF remained unchanged.
• Opiods: Excellent induction agents in very sick children as they have no cardio depressant effect, however it’s better avoided with bradycardia.

• Choice of Induction Agents– Intravenous
• Ketamine: maintaining SVR• Nacrotics: good hemodynamic stability • Barbiturate: ↓both SVR and PVR
– Inhalation• Sevoflurane: least effect on SVR• Halothane• Desflurane dose-dependent ↓SVR• Isoflurane pungent odor• Nitrous oxide

Neuromuscular Blocking Drugs
Non-depolarizing• Atracuruim and vecronium
have few cardiovascular side effects in children when given in recommended doses.
• Pancuronuim if given slowly doesn't produce HR or BP changes. if given as bolus doses it can produce tachycardia , ↑BP (through sympathomimetic effect )
• Cisatracuruim and Rocuroinuim: safe
Depolarizing• Succinylcholine in
pediatric is controversial
• Should be used with Atropine to avoid associated bradycardia or sinus arrest
• Also, if used with potent narcotic , atropine should be used to avoid severe bradycardia in children with CR

Case II
• A male baby, born at 39 weeks of gestational age TOF with a birth body weight of 3050 g, was admitted at 4 days old for progressive abdominal distention and vomiting.
• An emergent loop ileostomy and multiple biopsies of the rectum and colon proved a diagnosis of long-segment Hirschsprung’s disease.
• General anesthesia was induced using sevoflurane with oxygen by facemask.
• Rocuronium bromide (0.6 mg/kg) was used to facilitate the tracheal intubation.

• The patient’s condition remained stable until the surgeon pulled out all of the intestinal loops, at which point the oxygen saturation shown on pulse oximetry (SpO2) abruptly decreased, and the arterial blood pressure also gradually decreased.
• SPO2 was noted and dropped to only 23%. The intestine showed poor perfusion and the heart rate rose to 180 beats/min.
• Blood gas analytical data showed metabolic acidosis, which was corrected by sodium bicarbonate. Concomitant hypothermia (35.5°C at the nasopharynx) was detected.

OR preparation
• Included bolus syringes of phenylephrine and epinephrine along with epinephrine infusion.
• In addition, Bicarbonate was also available in the room.

Cyanotic spells
Flexing the legs or Squatting position compressing abdominal aorta Volume administration α-adrengeric agonist β-blockers Deepening anesthesia Morphine

REGIONALREGIONAL ANESTHESIA ANESTHESIA &ANALGESIA&ANALGESIA
• Regional blocks could be used safely in TOF in pediatric age group as sympathectomy doesn’t occur following these blocks.
• VD : which can Cause oxyhemoglobin saturation in R-L shunts

Postoperative Anesthetic Management of CHD patients:
• Need for supplemental O2 and maintain patent airway
• Pain infundibular spasm in TOF RVOT obstruction cyanosis, hypoxia, syncope, seizures, acidosis and death

Therefore, it is common for patients with CHD to present for non-cardiac surgery, and even in patient with corrected CHD significant residual problems such as arrhythmias, ventricular dysfunction, shunts, valvular stenosis, and PH may exist.

Thank you