presentazione di powerpoint - trivenetachirurgica.it filedr. angelo parello catholic university,...
TRANSCRIPT

Dr. Angelo Parello Catholic University, Rome, Italy
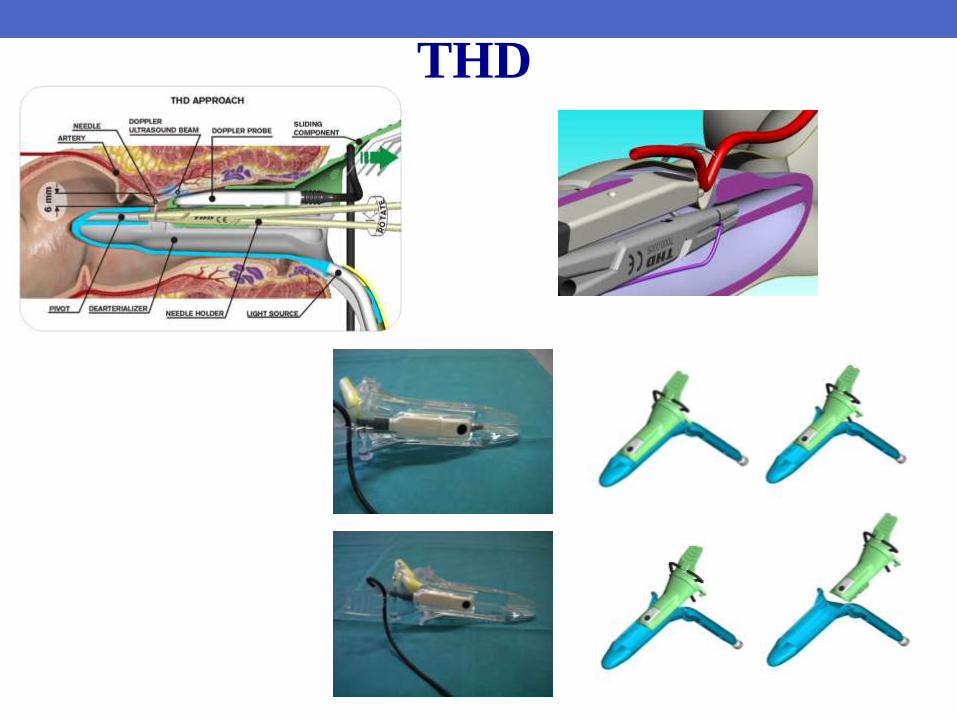
T H D

THD
• Transanal • Through the anus into the rectum
• Only mild stretch of anal sphincters
• Hemorrhoidal • … arteries, not cushions, identified by Doppler
• Dearterialization • ligation of main hemorrhoidal arteries
• reduction of overflow
THD

Sphincter hypertone
Anal cushions hypertension
(overflow)
Venous drainage impairment
Increased cushions pressure
Stress on connective tissue
Abnormally high anal pressure
Increased straining during defecation
Increased congestion and slippage of the
anal cushions
Degeneration of connective
tissue
Pathophysiology
THD
Dearterialization
THD
Mucopexy

Pathophysiology
- Higher artery caliber
- Increased arterial flow
- Incresed arterial flow velocity
- Lower arterial resistivity index
Echo-color Doppler features in
Hemorrhoidal Disease
Aigner et al. 2006
Aigner et al. 2009
Aigner et al. 2010
Ratto et al. 2007

Healthy volunteers
Patients with hemorrhoidal disease
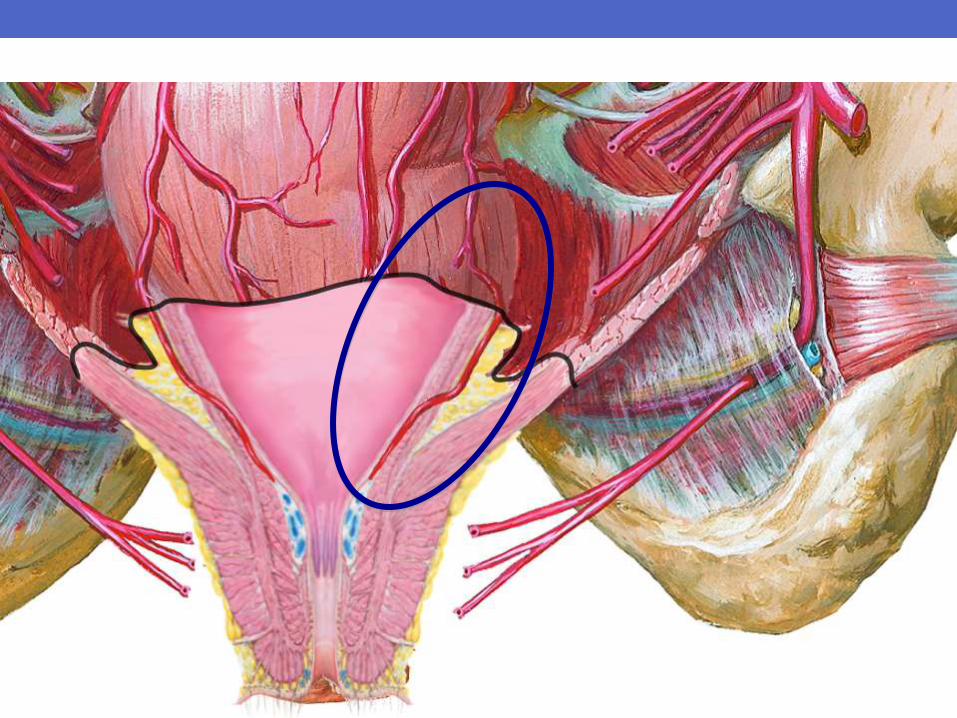
Hemorrhoidal Arteries
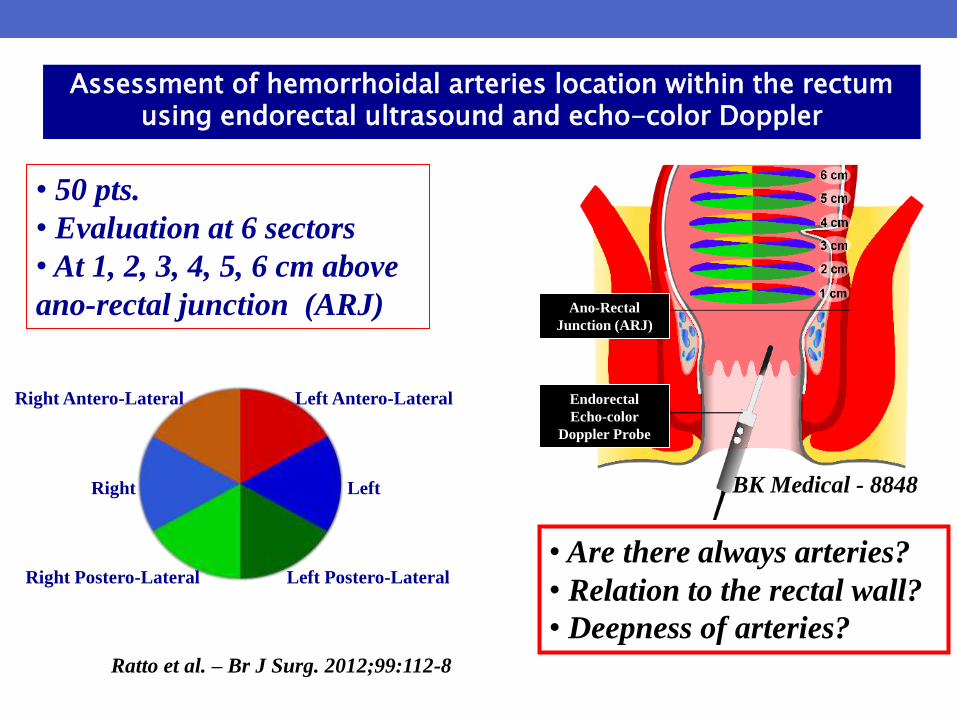
Assessment of hemorrhoidal arteries location within the rectum using endorectal ultrasound and echo-color Doppler
• 50 pts.
• Evaluation at 6 sectors
• At 1, 2, 3, 4, 5, 6 cm above
ano-rectal junction (ARJ)
Ratto et al. – Br J Surg. 2012;99:112-8
Ano-Rectal
Junction (ARJ)
Endorectal
Echo-color
Doppler Probe
• Are there always arteries?
• Relation to the rectal wall?
• Deepness of arteries?
Right Antero-Lateral
Right
Right Postero-Lateral
Left Antero-Lateral
Left
Left Postero-Lateral
BK Medical - 8848

F F
F-M M-SM
M-SM SM
Echo-color Doppler of
Hemorrhoidal Arteries
(HAs)
Ratto et al.
Br J Surg. 2012;99:112-8

- in almost all 6 sectors there are arteries (99.3 – 99.7 %)
- the arteries are into the submucosa (98.3 – 100 %)
- the arteries are very superficial (2.4-1.9 mm)
Close to the Ano-Rectal Junction (within 2 cm):
Assessment of hemorrhoidal arteries location within the rectum using endorectal ultrasound and echo-color Doppler
Ratto et al. – Br J Surg. 2012;99:112-8
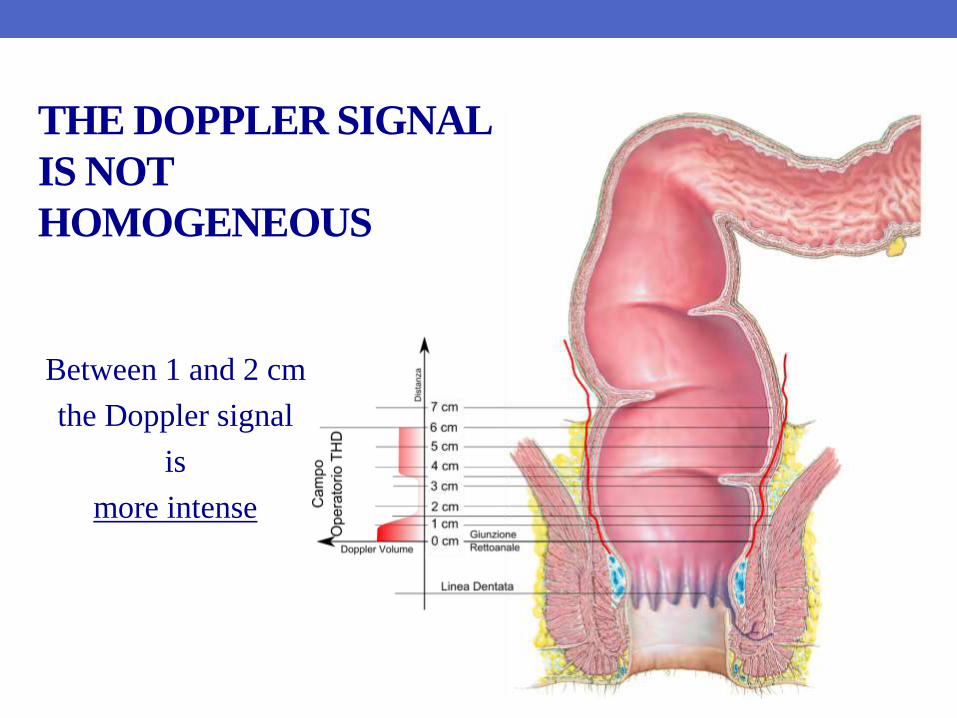
THE DOPPLER SIGNAL
IS NOT
HOMOGENEOUS
Between 1 and 2 cm
the Doppler signal
is
more intense

Distal Doppler-guided Dearterialization

THD
Distal Doppler-guided Dearterialization
& Structured Hemorrhoid-sparing Mucopexy
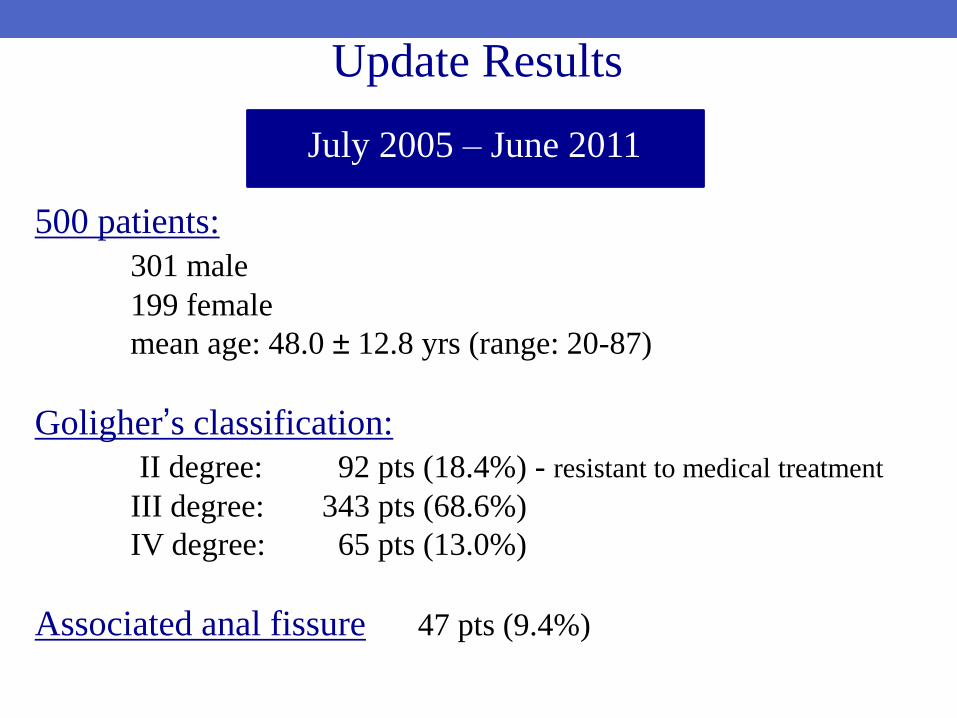
500 patients:
301 male
199 female
mean age: 48.0 ± 12.8 yrs (range: 20-87)
Goligher’s classification:
II degree: 92 pts (18.4%) - resistant to medical treatment
III degree: 343 pts (68.6%)
IV degree: 65 pts (13.0%)
Associated anal fissure 47 pts (9.4%)
July 2005 – June 2011
Update Results
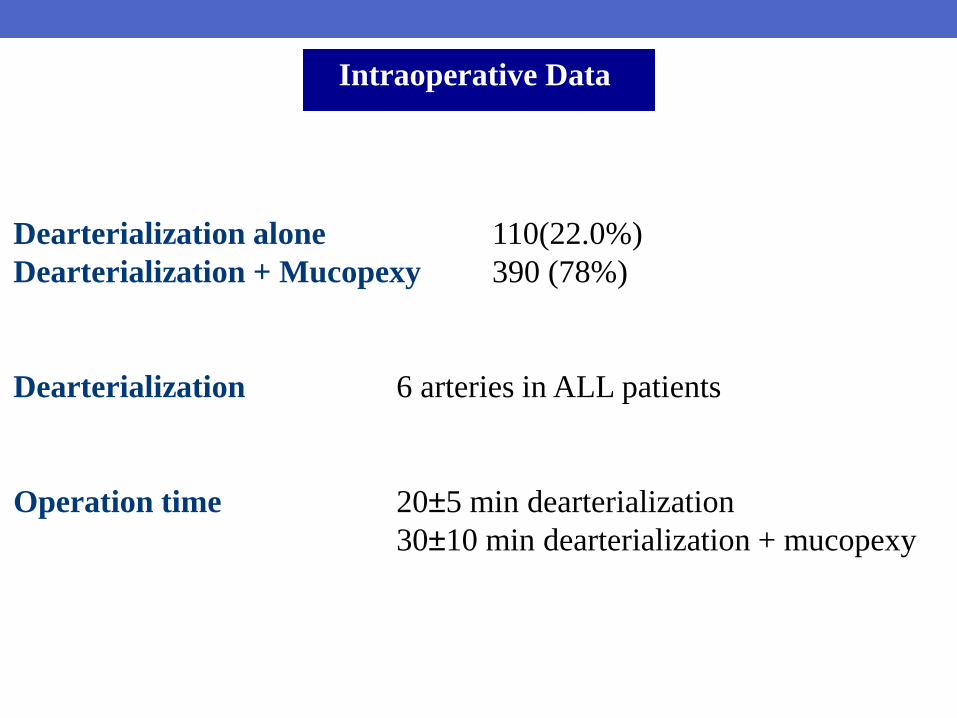
Intraoperative Data
Dearterialization alone 110(22.0%)
Dearterialization + Mucopexy 390 (78%)
Dearterialization 6 arteries in ALL patients
Operation time 20±5 min dearterialization
30±10 min dearterialization + mucopexy

27 pts. 41 pts. 57 pts. 375 pts.
1st year 2nd year 3rd year 4-6th years
Traditional
proctoscope THD Surgy THD Slide
THD instruments over the time

Post-operative Symptoms
SYMPTOMS EARLY (< 10 days) LATE (30 days)
Dearterializ.
alone
Dearterializ.
+ Pexy
Dearterializ.
alone
Dearterializ.
+ Pexy
n. % n. % n. % n. %
Tenesmus - - 123 31.5 - - - -
Significant bleeding
• Surgery - -
15
5
3.8
1.3 - - - -
Fecal Incontinence - - - - - - - -
Anorectal pain
• Prolonged analgesics
5
-
4.5
-
46
16
11.8
4.1 - - - -
Urinary retention 6 5.5 44 11.3 - - - -
Thrombosis 2 1.8 8 2.1 - - - -

Follow up
Recurrences 58 pts (11.6%)
Symptoms
Bleeding 0 pts
Prolapse 36 pts (7.2%)
Bleeding + Prolapse 22 pts (4.4%)
Mean Follow-up: 10.3±9.4 months (range 3-57)
Schedule: 2 weeks, 1 and 3 months, once a year after operation

Follow up
%
Recurrences

Bleeding Recurrence
Follow up %

Dearterialization with “intention to treat”
Bleeding Recurrence
20 / 461 cases (4.3%)
Follow up %
6.3% 2.8%
Follow up %
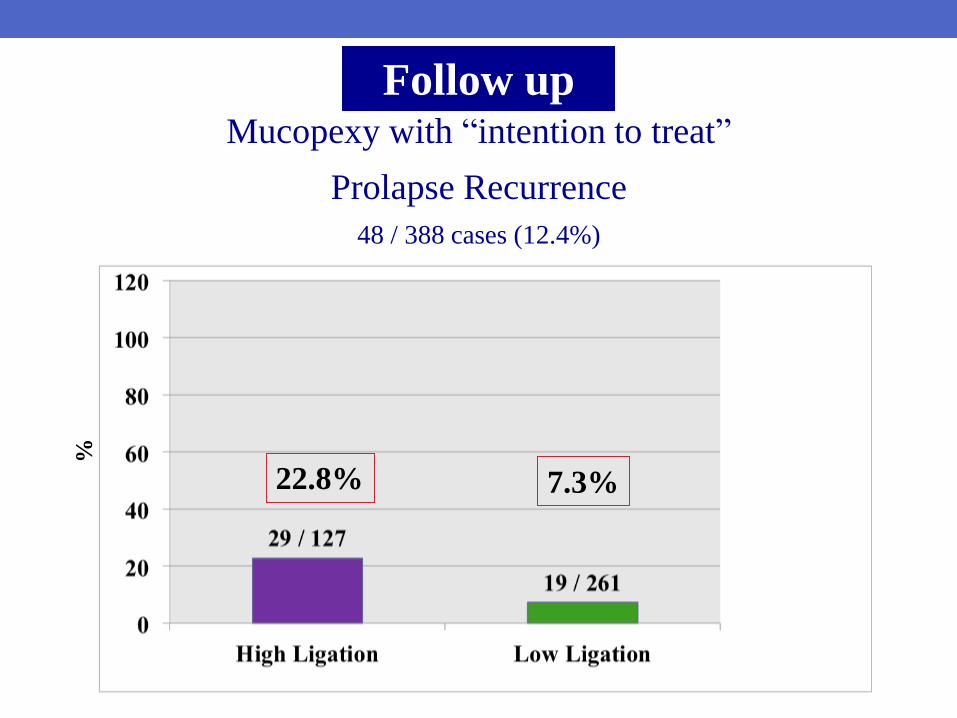
Mucopexy with “intention to treat”
Prolapse Recurrence
48 / 388 cases (12.4%)
22.8% 7.3%

Follow up %
Mucopexy with “intention to treat”
Prolapse Recurrence
48 / 388 cases (12.4%)
28.6% 26.8% 10.3%

Mucopexy with “intention to treat”
Prolapse Recurrence
48 / 388 cases (12.4%)
Follow up %
28.6% 26.8% 20.3% 7.3%

Re-operation 26 pts (5.2%) THD 16 pts (3.2%) Prolapse 13 pts (2.6%) Bleeding + Prolapse 3 pts (0.6%) MM 10 pts Prolapse 6 pts (1.2%) Bleeding + Prolapse 4 pts (0.8%)
Follow up
• Locations of arteries are not always the same
• Find the best ! Be selective !
• Not time-expensive
• Precision and reliability are of great value
Why Doppler ?

• To “modulate” the treatment of prolapse
• No any resection
• Save the hemorrhoids ! Away from the pecten !
• Safe procedure (no major complications)
Why Mucopexy ?

Why would a surgeon want to utilize this technique ?
SUMMARY
Together
A reliable method to treat hemorrhoidal disease