presentations on sustainability - shopsplusproject.org · the impact of nhif accreditation on...
TRANSCRIPT

Presentations on Sustainability
• Global Workshop for Social Franchising in Health – Jeanna Holtz, Abt Associates
• Strategic Purchasing of Quality Health Services from Private Providers in Myanmar –Han Win
Htat, PSI
• Linking Social Franchising Clinics to Health Financing Mechanisms – Joyce Wanderi-Maina, PSI
• The Impact of NHIF Accreditation on Sustainability and Contraceptive Uptake – MSK
• Vouchers in Uganda: An Accelerator of Access to Quality FP Services
• Masterclass: The Essentials of Contracting to Provide Family Planning and Reproductive
Health Services – Jeanna Holtz, Abt Associates
• Growing Businesses to Grow Health Impact – Sylvia Wamuhu, PSI
• Improving Business Skills – Miguel Antonio S. Lindo, PSPI
• Social Franchising in Lima: Expanding the Value Proposition
• Sustainability and Affordability in Low-Income Countries – Alexis Aimé Miharimanana, MSI
• Enhancing Sustainability of Social Franchising Supervision through Decentralization –Genet
Mengistu, IPPF
• Sustaining Sun Quality Health Network through Linkage with Health Financing Schemes –
Socheat Chi, PSI
• The Philippines’ Evolving Health Financing Landscape - Miguel Antonio S. Lindo, PSPI

Unlocking Sustainability
Understanding expectations and tradeoffs

Linking social franchising into broader health financing
mechanisms

Linking social franchising into broader
health financing mechanisms:
Overview of health financing
Jeanna Holtz
Abt Associates
28 September 2017
Global Workshop on Social Franchising
Accra, Ghana

5
We need a common language
mCPR
Method-
mix
Unmet
need
Risk
pooling
Purchasing
Mobilizing
resources
Health Financing Family Planning

6
Universal health coverage
Definition: People can access the care they
need without financial hardship
• UHC is an aspiration,
and not:
– a program
– insurance

7
Health financing is part of HSS

8
Health financing functions
Revenue
collection
Pooling
Purchasing• What will be purchased? (benefits)?; Who to
purchase from (public, private)? What payment mechanism to use?
• The accumulation of pre-paid revenues on behalf
enrolled members, whether privately or publically…to
enable transfer of risks between healthy and sick,
and wealthy and poor.
• Need source of funds, collection mechanism and collector. Examples:
– Government collects taxes from citizens
– Employer pays premiums to an insurer on behalf of employees
9
Financing UHC
• Countries pursue UHC using a mix of financing mechanisms
– Publicly financed services
– Insurance
Publicly-financed: social health insurance, national health insurance, government-sponsored insurance
Privately-financed:
– Products for the wealthy/formal sector
– Products for low income households/informal sector: community-based (mutuelles), microinsurance
• Majority of population in many LMICs relies on out of pocket spending
– Result: financial hardship/forgo care


Strategic Purchasing of Quality Health Services
From Private Providers In MyanmarHan Win Htat, National Director
Sun Quality Health Network, Population Services International Myanmar

12
3.8 Achieve universal health coverage, including financial risk
protection, access to quality essential health-care services and
access to safe, effective, quality and affordable essential medicines
and vaccines for all
2
13
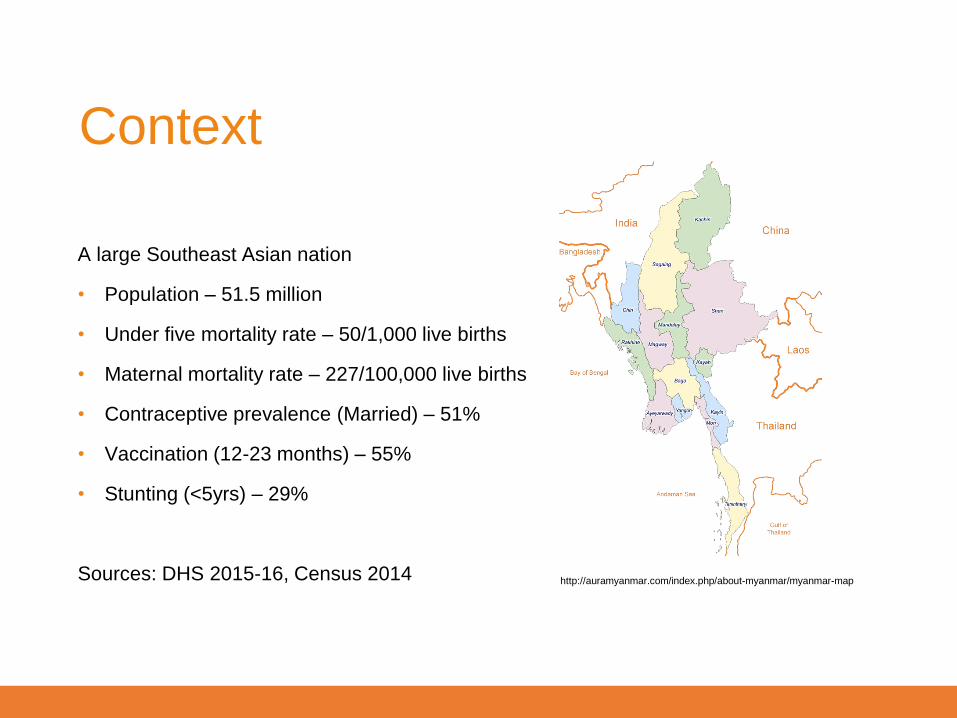
A large Southeast Asian nation
• Population – 51.5 million
• Under five mortality rate – 50/1,000 live births
• Maternal mortality rate – 227/100,000 live births
• Contraceptive prevalence (Married) – 51%
• Vaccination (12-23 months) – 55%
• Stunting (<5yrs) – 29%
Sources: DHS 2015-16, Census 2014 http://auramyanmar.com/index.php/about-myanmar/myanmar-map
Context

14
Myanmar’s UHC 2030 Vision

15
NHP Conceptual Framework

16
• Sun Quality Health Network: A social franchise network of 1,200+ general practitioners
• Mainly urban and peri-urban
• Focuses on reproductive health, HIV, malaria, tuberculosis, and maternal and child health
• Sun offers the government of Myanmar the opportunity and mechanism to commission services from private sector providers to compliment the public sector at predictable costs and quality
Sun Quality Health

17
Being at the table consistently is
important

18
Strategic
Purchasing Pilot
19
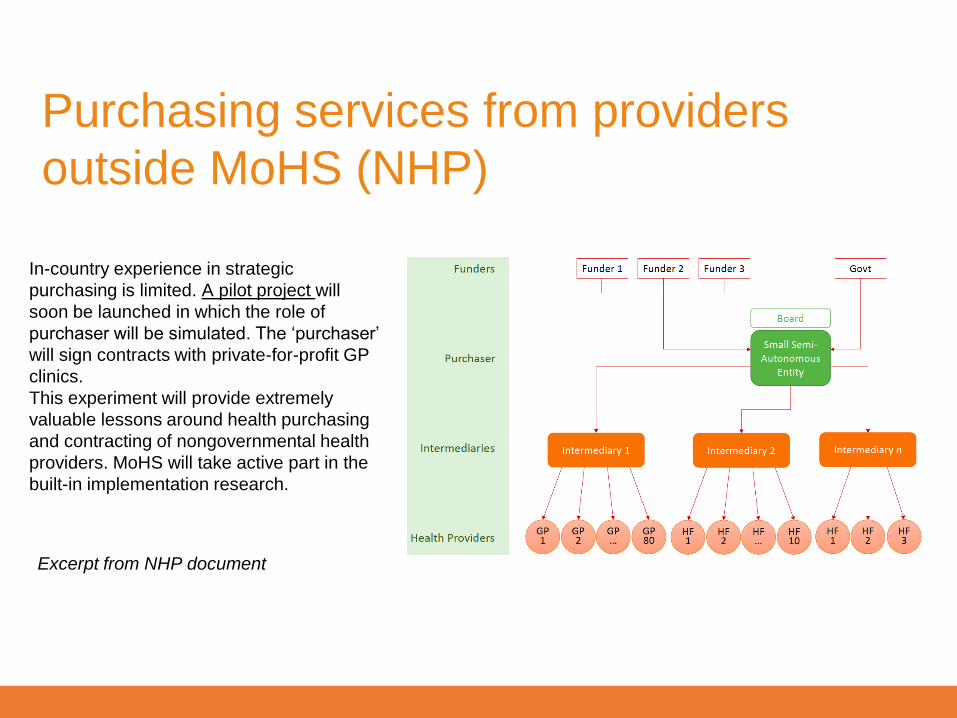
Purchasing services from providers
outside MoHS (NHP)
Excerpt from NHP document
In-country experience in strategic
purchasing is limited. A pilot project will
soon be launched in which the role of
purchaser will be simulated. The ‘purchaser’
will sign contracts with private-for-profit GP
clinics.
This experiment will provide extremely
valuable lessons around health purchasing
and contracting of nongovernmental health
providers. MoHS will take active part in the
built-in implementation research.

20
Under strategic purchasing arrangements, this model of care can increase access by
low-income consumers and achieve good value for money for public subsidy.
Project Objectives
In particular the project aims to:
• Increase the range of services
provided
• Decrease out of pocket payments
• Decrease the time to seek
treatment at a qualified provider
from the start of signs and
symptoms

21
Package of services
Inclusion criteria for
beneficiaries
Monthly capitation amount
Pay for performance
targets
Medical records
Critical Planning Steps
http://www.jointlearningnetwork.org/uploads/files/resources/UHC_Learning_Brief_Series_-_No1_Package_of_Services_FINAL_(1).pdf
http://www.jointlearningnetwork.org/uploads/files/resources/UHC_Learning_Brief_Series_-_No2_Strategic_Purchasing_FINAL_(1).pdf

22
• 2-year longitudinal study
• Base-line, mid-line and end-line
• 2 sites in peri-urban Yangon
• 11,000 study population
• 5 Sun Quality Health providers
• MOHS joined the project as the
Co-investigator.
Methodology
2,797 Potential
households
Screened
291 households
rejected
2,506 households registered
(10,881 eligible beneficiaries )
1,049 households eligible for
health surveys (41.9%)
1,334 individuals reported
seeking health
1,108 women reported
seeking health for FP or
fertility reasons

23
Five Categories
• Child health – IMCI approach, nutrition, immunization
• Reproductive health – short-term and long-term family planning methods, AN care, PN care, delivery support, ARH, Gender-based violence screening
• Communicable diseases – HIV, TB, Malaria
• Non-communicable diseases – Hypertension, Diabetes, Cervical cancer
• General illnesses - Minor Injuries (Abscess, Stitch), Aches and Pains, Alcoholism, Mental illness, Fever, Neuropathy, General weakness, Abdominal pain, Cough and URTI, Dengue (Grade I), Eyes (Conjunctivitis), Asthma, COPD (Primary Care Level), Fits, Epilepsy
The Package

24
Socio-economic Profiles
0%
15%
30%
45%
60%
Poorestquintile
2nd quintile Middlequintile
4th quintile Best-offquintile
Socio-Economic Profile_DB (N=1243)
(Reference: Yangon Population)
0%
15%
30%
45%
60%
Poorestquintile
2nd quintile Middlequintile
4th quintile Best-offquintile
Socio-Economic Profile_SPT (N=1263)
(Reference: Yangon Population)

25
Project Status (As of August 2017)
5 SQH doctors signed the provider contracts 7,287 beneficiaries received medical check-up
Each beneficiary received a health card MoHS team visited project clinics
UNiD generated by iris scan
Scale-up Management met 2 times

So what exactly does this look like for Su Su?
Access to low cost quality health care
• at a clinic of her choice
• close to her community
• for a wide range of FP options and illnesses
• from a friendly provider
• without financial hardship

27
• Negotiation with general practitioners to join the program
and accept the capitation model
• Lengthy identification process for poor households
• Prolonged baseline study due to temporary migrant
households
• Higher research cost due to higher burden of diseases
• Only 64% of eligible beneficiaries came to clinics for
medical screening (March-June 2017)
• Most beneficiaries are coming for “general illnesses"
Challenges


Linking Social Franchising Clinics to Health
Financing Mechanisms
Joyce Wanderi- Maina – PS Kenya

Context – Kenya
30
• Universal health coverage is a government priority in Kenya
• Decision made to anchor the country’s UHC aspirations on the
National Hospital Insurance Fund (NHIF)
• Only 1 in every 5 Kenyans has some form of health insurance
coverage
• NHIF covers 88% of those insured, private insurance – 9%, while
community based/other 3% of the population
• High out of pocket spending denying poor access to health care

▪ Approximately 41% of all outpatient
services are through private sector
▪ UHC commitments require wider
geographical foot print
▪ Social insurance traditionally biased
towards accrediting public sector
facilities
▪ Organized private sector – (social
franchising) provides an opportunity
to achieve scale and quality
Private sector role
44.10%41.60%
55.90%58.40%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
Inpatient Outpatient
Providers of outpatient and inpatient Services
Private Public

Our contribution towards meeting Kenya’s
UHC goals
32
Creating demand for enrolment into social health insurance
Facilitating empanelment and quality assurance
Advocating on policy issues with the public sector

• Uptake of social insurance is a behavior change
issue requiring intensive consumer education
• Development and implementation of a marketing
strategy to drive awareness of social insurance &
product benefits
• Improve product accessibility by simplifying
registration process
• Business case for providers
Creating demand for enrollment into
social insurance
33

Key Successes - National
scheme (Supacover)
34
370,000
New H/Holds registered in
12 months
Ease of
Registration
✓ Mobile phone registration
✓ NHIF e-wallet App
Online/NHIF website
✓ Premium remittance
through mobile money
• Enrolment numbers continue to grow at an
average of 50,000 new members per month
• Ownership of marketing strategy and
communication by NHIF beyond the initial
catalytic phase
• Integrating demand creation and enrolment into
other health outreach activities
• Use of feedback for continued improvement of
the product offering

87%Attended to by medical staff
74%Got prescribed drugs at facility
92%Described staff at facility as friendly
• Franchise providers contracted to provide
services to the indigents in priority regions
• Customer education, push for registration and
utilization stimulation in 8,500 households in 17
counties
• 96% of households registered by end of pilot
• Service utilization at 63%
• Customer feedback to NHIF to advice scale up
Beneficiary perception HISP
Key Successes – Health Insurance Subsidy
program (HISP)
35

Demystification of accreditation for providers
Quality improvement plans geared towards
improving facility readiness
Application of comprehensive quality tools to
assure quality of services and accelerate
accreditation process
Collaboration with national and regional
branches to pitch franchises on premise of
quality services
Facilitating empanelment and quality
assurance
36
36

Progress to date: Tunza
37
of Tunza facilities are
NHIF empaneled
• 173 providers empaneled to NHIF
• Target is to get 60% of Tunza
facilities empaneled by 2019
• Working towards fast tracking
contracting for various schemes
46%

NHIF members registered in Tunza facilities
for OP services
$ 1,003,562 Capitated value

“
• Contracting of small private sector providers –
preference was larger facilities
• Systems to measure and regulate service quality
• Recognition of other QA systems such as
franchise standards and external accreditation
• Balanced tariffs and efficient payment
mechanisms e.g. capitation amounts
• Advocacy for inclusion of comprehensive FP/RH
services and creating awareness of benefits
Advocating on policy issues
39
Growing recognition
of franchises and
notable readiness to
work with organized
private sector
39
“

▪ Increasing registration of dependents - lack of required documents
results to partial registration
▪ Clear communication on penalties and how they accrue to reduce
attrition as well as exclusions
▪ Simplification of benefits package to reduce subjective
interpretation by providers and clients
▪ Significance of the membership cards at the point of service
Opportunity: Using provider and customer
feedback to strengthen national schemes

▪ Government in the process of rollout FMS in
2,458 private and faith based (FBOs) facilities
in a phased approach
▪ Linda Mama comprises of an expanded
package of benefits to pregnant women and
their newborns for periods of one year
▪ The cover expires 90 days after delivery
Opportunity: Public sector contracting (Linda
mama) – skilled delivery
41
One on One Household sessions

Network Management Organization :An organization that
aggregates healthcare providers into a structured network
and presents this network to payers and healthcare
consumers.
• Customers: access to a panel of
quality providers, lower premiums or
lower out-of-pocket costs.
• Providers: Increased client volumes
(profitability)
• Insurance Companies: healthcare
services which meet a pre-defined set
of standards, lower administration fee
42
The future - Aggregation of providers

Thank You!Thank you

The impact of NHIF accreditation on
sustainability and contraceptive uptake
MSK
SEPTEMBER 2017

Marie Stopes International45
MSK’s value proposition• MSK set up the Amua social franchise network in 2004.
• Offer private providers a relevant and compelling ‘value proposition’ in order to:
• Motivate them to provide SRH services.
• Build their capacity to provide quality SRH services.
• MSK supports franchisees with NHIF accreditation, e.g.
• Acquisition of necessary licences and certificates.
• Support with SLAs for waste disposal, pharmacies and lab companies.
• Navigation of the process - NHIF Compliance Code/Certificate; Board
approvals; facility gazettment and tracking.

Marie Stopes International46
NHIF accreditation of Amua facilities
0
20
40
60
80
100
120
140
160M
ay-1
5
Ju
n-1
5
Ju
l-1
5
Au
g-1
5
Se
p-1
5
Oct-
15
No
v-1
5
De
c-1
5
Ja
n-1
6
Fe
b-1
6
Mar-
16
Ap
r-1
6
Ma
y-1
6
Ju
n-1
6
Ju
l-1
6
Au
g-1
6
Se
p-1
6
Oct-
16
No
v-1
6
De
c-1
6
Ja
n-1
7
Fe
b-1
7
Ma
r-1
7
Ap
r-1
7
Ma
y-1
7
Ju
n-1
7
Cu
mu
lati
ve
Da
ta
Month

Marie Stopes International47
NHIF’s impact on franchisee sustainability
Positive:
• Created opportunities for cross ‘selling’ services
• Improved provider reputation in their communities
• Improved provider status with other companies (e.g. insurance, workplaces, etc.)
• Client member volumes increasing, promoted through word-of-mouth by existing
members
• Utilisation increasing, cited as a benefit but also a challenge
• Client confidence - NHIF as a sign of service quality
• NHIF management information system (MIS) - providers like the automated
reporting and verification of client membership.

Marie Stopes International48
NHIF’s impact on franchisee sustainability
Negative:
• Increasing utilisation, including unnecessary visits (the Patient Moral Hazard).
• Influx of high risk clients / adverse selection i.e. chronic clients.
• Length of time to get empaneled
• Slow release of the capitation payments.
• Membership verification
• Provider changes
• Lack of scheme specificity

Marie Stopes International49
NHIF’s impact on contraceptive uptake
• Capitation covers all but permanent methods.
• NHIF guidelines on FP is vague and contradictory.
• Situation exacerbated by branch offices:
• Some branch managers unsure of the methods themselves.
• Others specify that implants are too expensive to be included.
• Consequently most providers are not providing FP services under capitation.
• Women are paying fees even if enrolled.
• This is probably impacting on method choice – e.g. chose OCP over more
expensive implants
• Providers benefit from Gov’t supplies of FP commodities but this is unreliable and
implants they are ‘last in the queue’ over public health facilities.
• Providers do not think it’s feasible to provide FP, esp. LARC, under capitation.

THANK YOU

51

- Meyer C, Bellows N, Campbell M, Potts M (2011)
52

Population
34.6 million people
34.6%
$1.90
28.4%
Fertility Rate
5.4
53
60%

Working through 220 private sector BlueStar franchisees,
using vouchers to target valuable subsidies to the most
vulnerable populations, reducing unmet need amongst
the lower wealth quintiles
.
Community Based Distributors trained and equiped to conduct community based mobilization, counseling and referral using
vouchers
Health workers trained to provide Quality counselling an
FP services to the most vulnerable populations
BLUESTAR
Improving access to affordable quality FP services including LARCs & PMs at health facility and community levels in the Private Sector
54

Family Planning Voucher (220), Youth Voucher (53). A client gets a service at any franchisees at no extra cost.

Vouchers distributed to
clients through the Community
Based Distributors
56
Clients reached with FP services
through Franchisees
rred ARC/PM
ervice
Voucher Redemption,
the highest ever in the 6year existence of
Voucher programme
Under the age of 24years
JULY, 2015 – JULY 2017Trends and Performance
202,218 172,075 91% 81% 44%

57 57
Learning

Perceiving Quality as a driver of business growth
Learning
58

Vouchers empower young people to demand for services at the health facility without fear of being judged
A driver of Business Growth
Infrastructure of the Franchisees improved as a result of reimbursement realized from offering services.
59
Learning

60

Neal Creative | click & Learn moreNeal Creative ©
Then 2014 Now 2017
SEE HOW FAR WE HAVE COME

Masterclass:
The Essentials of Contracting to Provide
Family Planning and Reproductive Health
Services
Jeanna Holtz
Abt Associates
28 September 2017
Global Workshop on Social Franchising
Accra, Ghana

63
QUIZ!

64
1. Which of these entities might purchase services from private providers?
a) Government
b) Private Employers
c) Private Insurance Companies
d) Donors
e) All of the above
QUIZ: Contracting basics

65
1. Which of these entities might purchase services from private providers?
a) Government
b) Private Employers
c) Private Insurance Companies
d) Donors
e) All of the above
QUIZ: Contracting basics
ANSWER

66
2. Why might private providers contract with governments?
a) Expand their client base
b) Improve their legal expertise
c) Tap into new revenue streams
d) A and C
e) All of the above
QUIZ: Contracting basics

67
2. Why might private providers contract with governments?
a) Expand their client base
b) Improve their legal expertise
c) Tap into new revenue streams
d) A and C
e) All of the above
QUIZ: Contracting basics
Contracts can help providers gain new clients and
access additional, stable sources of funding to expand
their practices and service offerings.
ANSWER

68
QUIZ: Contracting basics
3. Why might a government contract a private provider to deliver FP services?
a) Increase the number of service delivery sites in underserved areas
b) Help government avoid controversial or culturally sensitive issues
c) Improve efficiency in the health system
d) All of the above

69
QUIZ: Contracting basics
3. Why might a government contract a private provider to deliver FP services?
a) Increase the number of service delivery sites in underserved areas
b) Help government avoid controversial or culturally sensitive issues
c) Improve efficiency in the health system
d) All of the above
ANSWER

70
QUIZ: Contracting, UHC, and FP
4. Three common dimensions of UHC include:
a) Financial protection, facilities included, payment mechanisms
b) Payment mechanisms, health management information systems, services covered
c) Population covered, financial protection, services covered
d) Population covered, financial protection, facilities included

71
QUIZ: Contracting, UHC, and FP
4. Three common dimensions of UHC include:
a) Financial protection, facilities included, payment mechanisms
b) Payment mechanisms, health management information systems, services covered
c) Population covered, financial protection, services covered
d) Population covered, financial protection, facilities included
UHC focuses on increasing the number of people able to
access a greater range of services with increased
financial protection.
ANSWER

72
5. Insurance programs that support achieving UHC
always include benefits for FP.
True or False?
QUIZ: Contracting, UHC, and FP

73
5. Insurance programs that support achieving UHC
always include benefits for FP.
True or False?
QUIZ: Contracting, UHC, and FP
False. Benefits are often limited, and may focus on
inpatient services
ANSWER

74
6. Purchasers might face challenges contracting with private providers because:
a) Private sector is large and fragmented
b) Providers are accredited
c) Purchasers lack sufficient resources to pay private providers enough to cover their costs and make a reasonable return
d) A and C
e) All of the above
QUIZ: Contracting, UHC, and FP

75
6. Purchasers might face challenges contracting with private providers because:
a) Private sector is large and fragmented
b) Providers are accredited
c) Purchasers lack sufficient resources to pay private providers enough to cover their costs and make a reasonable return
d) A and C
e) All of the above
QUIZ: Contracting, UHC, and FP
ANSWER

76
7. Government contracting with private sector may support UHC by:
a) Encouraging efficient use of financing resources
b) Establishing a range of services that each provider must offer
c) Expanding access to subsidies and reducing financial barriers for underserved groups
d) Increasing the number of health facilities delivering covered services
e) All of the above
QUIZ: Contracting, UHC, and FP

77
7. Government contracting with private sector may support UHC by:
a) Encouraging efficient use of financing resources
b) Establishing a range of services that each provider must offer
c) Expanding access to subsidies and reducing financial barriers for underserved groups
d) Increasing the number of health facilities delivering covered services
e) All of the above
QUIZ: Contracting, UHC, and FP
ANSWER
78
Session agenda
• Overview of SHOPS contracting lifecycle
• Group activity on contracting
• Wrap up

79
Session Objectives
• Articulate how contracting supports objectives of
purchasers and providers
• Understand contracting lifecycle
• Identify obstacles/solutions to create and sustain
contracts for FP services
• Know where to go for additional resources

80
Contracting within the health sector
• Specify “gives and gets”
• Examples: service agreement,
lease, grant, franchising
• Focus today: service agreements
(purchaser and provider)
Contracts are legal instruments that set forth obligations,
rights, and duties of the partners involved.

81
Why contract?
• What motivates a government purchaser of health care
to contract with a health provider?
• What motivates a private provider to contract with a
government purchaser?

82
Objectives of purchasers (e.g. government)
• Improve access, relieve pressure on public facilities
• Harness private sector expertise and resources
• Improve efficiency
• Avoid controversial, culturally sensitive issues

83
Objectives of providers
• Increase revenue; establish regular income
source
• Expand and maintain client base
• Increase operating efficiency
• Fulfill social mission

84
The Contracting Lifecycle

85
The Contracting Lifecycle
Contracts can follow a “one cycle” pathway

86
The Contracting Lifecycle
…or a repeating cycle

87
Stage One: Evaluate Feasibility

88
Stage One: Evaluate Feasibility
• Assess internal, external environment
• Analyze strengths, weaknesses, opportunities, and
threats
• Understand payment mechanisms
• Fixed rates, results-based, or capitation are replacing grants, input-based, cost-based agreements

89
Stage Two: (Re)Design the Contractual
Relationship

90
Stage Two focuses on negotiation
• Payment mechanism and rates
• Covered services (including LA/PM)
• Monitoring and reporting
• Accreditation (quality)
• Dispute resolution
• Termination terms
Stage Two: (Re)Design the Contractual
Relationship

91
Stage Three: Implement the Contract

92
FP service providers need to
• Train staff for new roles and procedures
• Ensure adequate resources
• Staff
• Supplies
• Equipment
• Educational materials
Relationship management is key!
Stage Three: Implement the Contract

93
Stage Four: Manage, Monitor, Evaluate

94
Purchasers and providers will monitor:
• Volume, quality, efficiency, cost, client feedback
Providers should additionally monitor:
• Timeliness, accuracy of
payments
• Profitability
Stage Four: Manage, Monitor, Evaluate

95
Providers should establish procedures to track indicators
and prepare for audits:
• Clinical, utilization indicators
• % of target population reached
• # of FP services provided
• # of women counseled on FP
• # of adverse FP incidents
• # of CYPs
Stage Four: Manage, Monitor, Evaluate

96
Providers should establish procedures to track indicators
and prepare for audits:
• Non-clinical indicators
• Client satisfaction
• Costs
• Timeliness of reports
Stage Four: Manage, Monitor, Evaluate

97
Stage Five: Close the Contractual
Relationship

98
Contracts can end in two ways:
• Closure: Contract ends as planned
• Termination: Action taken to end contract before its
full performance (unplanned)
NOTE: Providers should understand their
obligations under termination, including
length of time to continue service delivery.
Stage Five: Close the Contractual
Relationship
99
Tips to avoid/manage termination:
• Establish a formal dispute resolution
process
• Stay on top of (outstanding) payments
• Maintain cash reserves
• Establish late fee provisions in
contract, and ability to suspend
services
Stage Five: Close the Contractual
Relationship

100
The Contracting Lifecycle

101
Small group work
Case study:
• Takes place in country of Manyland
• Involves the Ministry of Health and the Health Association of Manyland
Instructions:
30 minutes
• Read case study provided on tables
• Discuss based on prompts
• Prepare brief response to question
20 minutes
• Groups report out

102
Group report out

103
Key Takeaways
• Trend toward contracting for FP services to access
patients and revenue streams
• Success in contracting occurs at all stages of the
contracting lifecycle.
• Variety of skills needed to succeed under contracting
• Invest in relationships
• It’s a learning process!

104
SHOPS Plus has resources on contracting
• Published 2 primers on contracting for FP/RH
• One for policymakers, donors
• One for providers
• online FAQ tool to complement primers at: https://www.shopsplusproject.org/contractingfaq
• eLearning course at USAID Global Health eLearning
Center: https://www.globalhealthlearning.org/course/contracting-family-
planning-and-reproductive-health-services


Tables
Innovations in Social Franchising
Creating Sustainable Businesses
Improving business skills and creating linkages to business
improvement loans

Sylvia Wamuhu – PS Kenya
Growing businesses to grow health impact
108

Program Overview
Objectives of the overall program
• Offer holistic quality improvement leading to SafeCare
accreditation
• Help in bridging provider gap in business skills
• Provide access to affordable financing
173Tunza Providers Implementing
Business Skills

General Business Operations:
• Business registration, tax and statutory compliance, risk
management, general facility layout and client satisfaction
Financial Management:
• Setting up financial systems, bank accounts, managing debts, using
data for decision making
Stock Management:
• Manual and automated
Marketing and Demand Creation:
• Basic / community marketing techniques to spur growth

How the business program works
Sensitization, Recruitment
Business Assessment
Business Improvement Plan
Training / Continuous Support supervision and linkage to credit

Stepwise Business Improvement
Using business levels to help clinics grow & improve…
• Segment the providers into different levels to target resources and create efficiencies.
• Do not implement a “one size fits all” model (due to different sized clinics with varying capability to take on new services)
Business Level
Score Bracket Business Description
Level 1 0% - 25% No Business Skills
Level 2 26% - 50% Limited Business Skills
Level 3 51% - 75%Good Business
Management
Level 4 76% - 100%Excellent Business
Management

• Client Flow: Increased by an avg. of 35%!!!!!
• Revenue: Up by 28%
• Improved systems: 41 facilities have Clinic
Management Systems (up from 15)
• 59% - have moved from one level to another
• 29% - accessed credit
Tunza facility Levels
Level 1: 24 facilities Level 3: 78 facilities
Level 2: 60 facilities Level 4: 12 facilities
Impact
0
500
1000
1500
2000
2500
Level 1(0-25%) Level 2( 26-50%) Level 3( 51-75%) Level 4( 76-100%)
Business Level Vrs Average Patient No.s
Average Number of patients

Impact
What has worked?• Providers receptive to learning new business skills e.g.
Improved business systems, improved inventory management, cash management, data use etc.
• The program often led to rapid business growth/facility expansion e.g. lab
Sara (our PSI client archetype!)• Improved customer service (exit survey – 95% satisfied)• Increased scope of services (continuum of care)• Access to quality and affordable drugs
What has not worked?
Lessons learnt• Facilities in the business program perform better in
other quality related assessments e.g. NHIF, JHIC• Considerable effort initially required as providers
need hand holding
• Some providers are reluctant to share revenue data

`
Loans for growth
What worked?
• Access to financing led to improved quality of
services, increased clients and revenue
• Linkage to banks and facilitation of loans application
process
Lessons learnt• Assumption that providers lack other sources of
funding is not entirely true!
What happened?• Provides became credit worthy and banks
became more willing to lend to providers• 29% of providers accessed formal credit
through this program

• On joining the business
program, she
transformed her
approach to doing
business. Within the
first 1 year, Patients
increased from 20 to 45
per day.
Grace Wanjiku’s clinic
“The Tunza Business team
gave me business legs to stand on.’’Grace Wanjiku Masila,
Registered Nurse
I urge other clinics to
take up the advice of
the Tunza business
team and watch how
your business will
grow.

THANKYOU

Improving Business SkillsIs it a Zee or a Zor Question?Miguel Antonio S. Lindo
Friday, 29 September 2017

Marie Stopes International119
Who we are in the Philippines
To provide sustainable sexual and reproductive health services of the highest quality to Filipinos Nationwide
Successful Franchisees Lead to Family Planning
BlueStar Operational Excellence
Clinical Standards Execution
Active Demand Generation Activities

Marie Stopes International120
The challenge of managing two bottom lines
“[We] must effectively manage two bottom lines when operating a social
franchise; mission results and financial results.”
Benjamin C. Litalien, CFE
“[The manager] must be committed to the mission of the nonprofit and
motivated to control cost of goods, provide good training and supervision
for employees and constantly monitor and market sales.”
Judi Bishop, executive director of the Fort Worth YWCA

Marie Stopes International121
Understanding our client – the franchiseeGraduate of a 2 year course
Primarily a Service Provider
Ages between 40-60 years old
Before BlueStar either called for home service
Assistants of Doctors in Maternity Hospitals
No established professional fees
Earned by daily wage or by tips
Mothers and Home Makers
No formal graduate or post graduate education
Computer skills limited to Facebook and Facetime
Deliver babies according Philippine DOH Standards
Provide FP according to Philippine and MSI Standards
Manage employees (DOLE), facilities (PHIC), and supplies
Engage with Governing Bodies (LGU, DOH, PHIC, BIR, Bank)
Reportorial Duties of Data Validation, QTA, MDT, and others
Run a business that should gross $ 20,000.00 annually
Demand Generation
Behavior Modification
Cooking
Cleaning
Rearing Children
Husband-Wife Duties

Marie Stopes International122
Three Simple Tools to Improve Business Skills
Marie Stopes International123
The Franchise E-Factor• Model developed by Greg Nathan of the Franchise Relationships Institute
(Australia) to help franchisees and franchisors better understand their
relationship.
• Explains why dealings become strained and how both parties might use this
tension to enhance the relationship.

Marie Stopes International124
The Franchise E-Factor
GleeFranchisee
nervous but
excited and
optimistic
FeeFranchisee
feeling more
sensitive and
concerned
about return on
fees
MeFranchisee
concludes their
success is due
mainly to their
own efforts
FreeFranchisee tries
to assert their
independence
SeeMutual
understanding
and respect
grows after
frank and open
discussions
WeFranchisee
recognises
value of
collaborating
with franchisor
Dependence Independence Interdependence
AVOID:Reckless
optimismConfusion Fear Revenge Greed
COMMUNICATE:Cautious
optimismClarity
Confidence
and valueEmpathy Commitment
Fra
nc
his
ee s
ati
sfa
cti
on

Marie Stopes International125
Establishing basic financial KPI’s
• Sales
• Expenses
• Total Operating Expenses
• Net Profit
• Net Sales
• MCP Clients
• IUD Clients
• Implant Clients
• PSP Clients
• MCP 79:21
• If with PPIUD 65:35
• Interval IUD 30:70
• Implant 22:78
• Pap Smear 27:73
• MCP 80:20
• FP 60:40
• Separating Clinic Money from Personal Money
• Post Dated Check
• Giving oneself a salary
• Schedule of Payments
Develop an easy to use
Income Statement
Figure Out How Many Customers They Need
Per Month to Break Even
Maintain Per Service Cost to Revenue
Ratio
Maintain PHIC to
OOP Service Ratio
Develop Cash
Discipline

Marie Stopes International126
Continued education
The Certified Franchise Executive Program (CFE) is a career development program offered by the
Institute of Certified Franchise Executives (ICFE) of the International Franchise Association (IFA)
Education Foundation. It offers franchise professionals the opportunity to learn, grow
professionally and reach a recognized standard of excellence in the franchise community.
Franchise Asia Philippines is Asia’s biggest international Franchise Conference loaded with powerhouse international and local experts and
speakers discussing Global Best Practices, Latest Trends, and Innovations and Disruptive Strategies. It presents unparalleled educational, professional
development , and networking opportunities
Certified and Professional
Learn from the Best

40 años con bienestar
Red Plan SaludSocial Franchising in Lima: Expanding the value proposition

Red Plan Salud: Develop, Launch, Grow
Baseline Study
Market Study
MVP Study/Lean Experimentation
Franchise ModelDeveloped.
Signing of 7 agreementswith obstetric privateproviders
Adjustments to franchisemodel
Implementation of pilotwith 7 franchisees
Expansion of franchisenetwork

Expanding the Value Proposition forProviders: Business Management Training
Strategic Planning Marketing
Financial Planning Business Planning
Technical assistance
and accompaniment in
the development of
business planning and
training in business
management that
enables franchisees
to build business
skills to strengthen the
sustainability of their
clinics and reduce
overall costs of the
network, therefore also
increasing the
sustainability of the
network

Business Planning Training Topics
Business Description
Background
Actual Context
Vision, Mission, Goals
SWOT Analysis
Market Study- Marketing
Market
Client
Marketing Plan – Commercial
Strategy
Competition
Business Structure
Staff Required
Responsibilitiesof each position
OrganizationalChart
OperationsPlan
List of requirements
Classification of Direct and
Indirect Costs
Standard Costs
Break-evenPoint
FinancialPlan
Seeking and obtainingfinancial
resources
InvestmentRequired
Cash Flow
Activity Plan

Achievements
7 franchisees have strengthenedtheir business managementcapacities and have a businessplan
As part of the implementation of their business plans they have improved the infrastructure and adaptation of their clinics.
Focus on the user has improvequality of care
These factors lead to increased client demand, increased revenue, and increased provider sustainability. As the provider becomes more self-sustainable, there is less reliance on the franchising network to subsidize operating costs, thus the network becomes more sustainable as well.
Difficulties
Time to meet with all franchisees
Internet bandwidth within a franchisee clinic
Availability of commercial products
Referrals of clients
Challenges
Additional follow up of businessplan implementation
Long-term accompaniment
Implementation of médium- and long-term goals of business plan

Lightning Rounds

Sustainability and
affordability in low-income
countries
Alexis Aimé Miharimanana
Social Franchise Channel Manager
MSI Madagascar
September 2017

Marie Stopes International134
Our ambitions
• We – the SF community - are very ambitious! We want SF to achieve:
• Health impact
• Quality
• Equity
• Cost-effectiveness
• Health market expansion
• Sustainability
• We have a proposed definition of sustainability: ‘continued high quality health
outcomes over time while achieving the social goals of social franchising’.
• We expect franchisors to reduce their dependence on institutional donors.
• We hope to secure public and private health financing of services and recover
costs from franchisees.

Marie Stopes International135
The reality of a low income country
• How do these expectations apply to a low income country like Madagascar?
• 77.1% live in extreme poverty
• 83% live in rural areas
• 64% of the population is <25 years old
• mCPR is 33.3%
• Absence of financial means with the treatment 68.6%
• Net ODA received is 53% of central gov’t expense (World Bank, 2014)
• All MoH activities depend on ODA.
• This context presents challenges for many SF goals, including sustainability.

Marie Stopes International136
Addressing affordability
• We can’t achieve health impact, equity and health market expansion without
addressing affordability.
• We’ve demonstrated this is possible with our voucher programmes:
• At least 70% of SF LARC clients are voucher clients.
• Vouchers can also incentivise and finance franchisees to deliver quality.
2013 2014 2015 2016 2017 Total
Unintended pregnancies
averted19,569 62,726 39,634 47,467 17,022 186,418
Maternal deaths averted52 157 95 109 37 450
Unsafe abortions averted5,809 18,621 11,765 14,091 5,053 55,339
Total DALYs averted 25,339 80,639 50,708 60,378 21,526 238,589
Direct healthcare costs
saved (2015 GBP)704,922 2,259,577 1,427,710 1,709,883 613,194 6,715,286

Marie Stopes International137
Who pays for the service if the client can’t?
• What options are available to a low-income country like Madagascar?
• Institutional donors: Invaluable USAID funding is ending; some other key
donors are yet to be convinced of the value of investing in voucher
programmes; DFID are beginning to show interest in.
• Public health financing: No prospect the government will purchase
services in the short-medium term.
• Private health financing: Few schemes exist; don’t enrol the poorest.
Marie Stopes International138
Matching the ambitions to reality
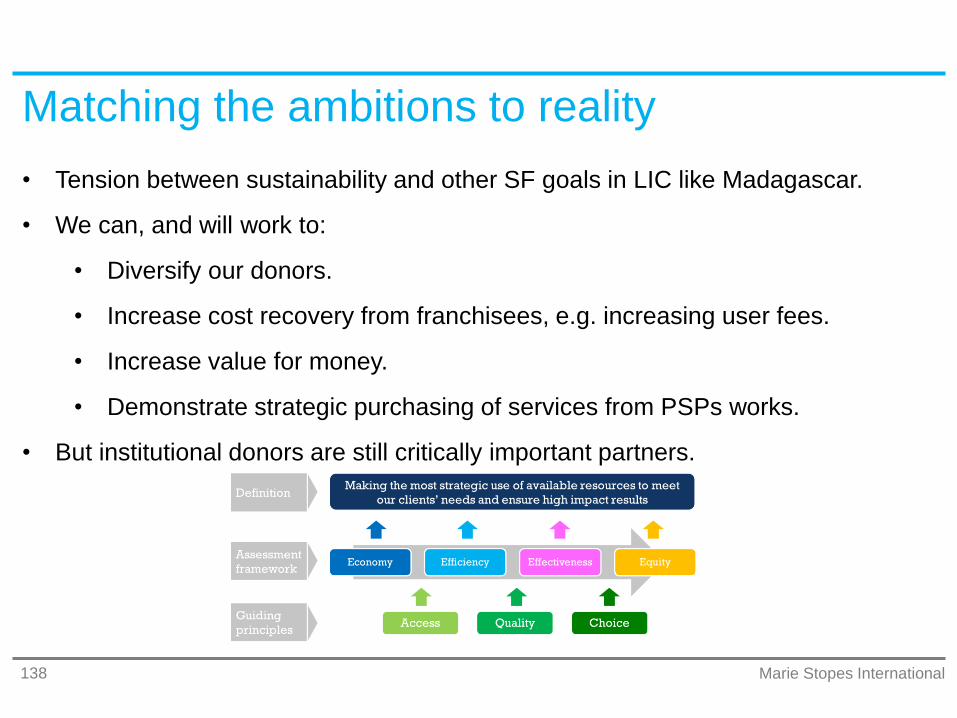
• Tension between sustainability and other SF goals in LIC like Madagascar.
• We can, and will work to:
• Diversify our donors.
• Increase cost recovery from franchisees, e.g. increasing user fees.
• Increase value for money.
• Demonstrate strategic purchasing of services from PSPs works.
• But institutional donors are still critically important partners.

Striving for Excellence in Sexual & Reproductive Health
Genet Mengistu
Executive Director
Family Guidance Association of Ethiopia
Enhancing Sustainability of Social Franchising
Supervision through Decentralization

Background Information
Established in 1966 as the first indigenous, non-
governmental, voluntary FP organization
IPPF affiliated member – since 1971
FGAE Operates in Eight Regions and Two City
Administrations
47 own facilities
1 Obst/Gynae Specialty, 8 Higher and 13 Medium Clinics
15 Youth Centres
10 Confidential Clinics
326 Social Franchised Clinics
226 Outreach sites in HLIs, Factories, Plantations,
Rural Health Posts and Public Youth Centres

Family Health Network Brand

Growth in size of Family Health Network
174 Primary FHNCs, 116 Medium FHNCs, 21 Higher FHNCs and 15
Plantation and Factories

Growth in impact
YearDALYs
Averted
CYPs
Provided
2014 119,431 181,897
2015 134,602 207,824
2016 196,330 325,443
Total 450,363 715,164
Social Franchise + Static Clinics

Shift in proportion of CYPs delivered by SF
clinics and static clinics
20%
42%62%
80%
58%38%
0%10%20%30%40%50%60%70%80%90%
100%
2014 2015 2016
SF Static

Reduced total cost of providing supportive
supervision to franchisees
-
100,000.00
200,000.00
300,000.00
400,000.00
500,000.00
600,000.00
2014 2015

FGAE’s Decentralization Approach

Decentralising management to enable
sustainable growth
8 Area Offices manage all franchisees in their area.
Model clinics have between 4-15 SF clinics anchored
to them
Quality assurance and monitoring decentralized and
costs associated with quality assurance and
supervision are reduced
Franchisees in an area are bought together for
learning and sharing

Thank You!

Sustaining Sun Quality Health Network
through linkage with health financing
schemesSocheat Chi, Executive Director, PSI Cambodia

150
Roadmap to move SQHN
toward sustainability
• Using improved business approaches as incentive
• Access to micro loan for business expansion
• From FP only to a wide range of services: including maternal child health,
malaria testing and treatment – integrated service delivery
• Quality assurance/improvement continuous medical education
• Data collection, reporting and link with national HMIS
• Accreditation
• Link to existing health financing scheme: National Social Security Fund, Health
Equity Fund etc - will require advocacy work
• Pay for service/support - membership fees

151
• Business training – financial/ HR
management and marketing
• Connect SF network to micro financial
institutions
• Expand services to fit with health
financing schemes
• Quality improvement to get accreditation
• Linkage with the NSSF for a specific
target group: garment factory workers
Areas of Focus
““
I want to put more
investment because
my clinic still has gaps
and not yet attractive,
that’s why I have few
clients, and I want to
serve more women…..

152
THANKYOU

The Philippines’ evolving
health financing landscapeOpportunities for a truly sustainable social
franchise
Miguel Antonio S. Lindo, Social Franchise Director
PSPI
September 2017
Marie Stopes International154
A conducive context
• Middle income country.
• Changing landscape but some stubborn statistics:
• 24.4% mCPR, 33.5% LAPM*.
• <40% of births are home deliveries.
• Gov’t have been supportive of contraception.
• Willing to procure services from private sector; PhilHealth is their vehicle for this.
• Supportive policy framework for this:
• Aquino Universal Healthcare Agenda 2010
• The Responsible Parenthood and Reproductive Health Act of 2012
• 2017 EO 12 attain and sustain “zero unmet need for modern FP”
AQUINO

Marie Stopes International155
The story so far• PSPI convinced gov’t to allow midwives to perform LARC in
maternity homes and pay for it:
• Gradual process, first PPIUD, then interval IUDs, then implants.
• Administrative Order licencing birthing homes to provide LARC.
• Circular accrediting midwives to receive LARC reimbursements.
• $ 40.00 for IUD, $ 60.00 for implants
• PSPI successfully franchised maternity homes, providing clinical
training, quality assurance, business training, etc.
• This expanded access and increased the franchisees’ sustainability.

Marie Stopes International156
It’s not all good news• Many challenges claiming reimbursements:
• National and regional government bureaucracy.
• Inconsistency in implementing the administrative orders.
• Low capacity to file reimbursement claims.
• ‘Buggy’ government IT and ERP Systems
• Increasingly competitive space
• Politics is still involved.
• This results in payment delays of <180 days.
• Creates cash flow problems.
• Impacts on midwives’ operations and personal lives.
• Midwives beginning to feel demoralised and exploring alternative careers.

Marie Stopes International157
The future - commercial franchise, social goals
1. Switching from franchisee fees to a commission based system
• Recently PSPI has started supporting midwives to set up maternity homes.
• Give: $25,000 no collateral loans, 5 years, 6% interest.
• Get: Higher franchise fees and 10% commission on LARC reimbursements.
2. Evolving our value proposition
• Mediation between PhilHealth and franchisees for claims management.
• Improved technical assistance to assure clinical and data compliance.
• Investment in brand visibility and marketing activities.
• A more robust entrepreneurial support and training program
3. Franchising standalone FP clinics
• Shape implementation guidelines; test in MSI centres; assess viability.

Marie Stopes International158
Further reflection and advocacy
Specialization vs Integration
Birthing + Family Planning Model
Polyclinic Model
Hospital Model
Expanding Services in
Lower Facilities
What other benefit packages can be performed in Birthing Homes, Stand Alone FP Clinics, Infirmaries
How can we expand government subsidies on Primary Care Benefit Packages
Influencing Government
on Family Planning
Where is FP in the Philippine Healthcare Agenda? Where is the FP Charter on the Philippine Health Insurance Corporation
What changes do we need to raise the value FP Services as a healthcare priority rather than a simple token or added service
How do we truly engage government
to pay for family planning?

Looking Towards the Future