presentation title (change in view slide master) date of presentation observations and...
TRANSCRIPT
Presentation title (change in view slide
master)
Date of presentation
Observations and Recommendations
on Draft HSRSU 2015-2025
Dr. Ihor Perehinets & Dr. Dirk HoremansWorld Health Organization
SAG Public Consultation MeetingKiev, Ukraine, 5 December 2014

Presentation title (change in view slide
master)
Date of presentation
General remarks on the Strategy
General Agreement on need and urgency for Health System Reform is omnipresent
The present document states “ …. Only a policy proposal to be submitted to the Council of Ministers” , not a detailed strategy but a setting of priorities to be addressed.
No need to wait for the perfect document to start Public Consultation; to this purpose it is a solid basis
Good Basis to develop a strong and comprehensive Health System Reform Strategy
Congratulations for strong consultation process (10 sessions over 2 months); stakeholder consultation and involvement is essential in any reform process => What is the process for selecting and consolidating of recommendations? Role of the MOH Coordination Committee, International and Bilateral Organizations, the Secretariat and the Experts?)
Different draft health system reform strategies are being developed in parallel; How to assure a comprehensive “STRATEGY” that considers the view of the different stakeholders?

Presentation title (change in view slide
master)
Date of presentation
General remarks on the Strategy
“Policy Direction Chapter” needs to define clearly Values, Vision, Goals, Principles and Objectives for the future Ukraine Health System and the Health System Reform.
–Quality and Safety–Accessibility through Universal Health Coverage–Equity, solidarity (progressive contributions)–Patient Centeredness–Good governance and accountability–Social Determinants–Investing in Health through the life course–Health for Wealth <= extreme high mortality rates for male working age population –Creation of a resilient Health System–Invest in Public Health (population based services)–Coordinated and Integrated Health Service Delivery with PHC as cornerstone–Participation and inter-sectorial collaboration approaches
Important to refer to WHO Health and Health System Values and principles Important to refer to EU association Agreement Health directives and recommendation

Presentation title (change in view slide
master)
Date of presentation
General remarks on the Strategy
All 6 Health Systems Components are mentioned but their present reform strategies need further development.
Many Health System Reform aspects are mentioned throughout the document but because of the present structure some important issues do not receive the necessary focus => Final document should have improved structure and clear statements
The chapter on main health status and health system issues should include HIV and TB aspects, MDR TB and the extreme low immunization rates, access to care in general and medicines in particular (OOP).

Presentation title (change in view slide
master)
Date of presentation
General remarks on the Strategy
The draft proposes Short-term, Medium-term and Long-term actions, each a mix of reform changes as well as preparatory work for next phases.
Many reform aspects/components would benefit from Policy Dialogue exercises, (WHO CO, Regional Office for Europe and HQ have a large pool of solid health experts in different fields to support such policy dialogues)
Support from International and Bilateral Organizations (WHO, WB), EU and others in the development of the Strategy. The strategy could also mention the envisaged role of those donors/stakeholders with regards to the implementation of the reform and their support towards the health sector. Related to need for improved Donor Coordination Mechanism.
Foster Cross Country learning and cooperation (relevant EU Member states and other neighboring countries)

Presentation title (change in view slide
master)
Date of presentation
General remarks on the Strategy Need for a “Health System Reform Communication Plan” addressing different stakeholders (Problems being addressed, expectations and timeframe, how changes affect them, how to use new systems, progress)
Monitoring of the reform (against set of reform indicators, measuring patient satisfaction)
Strategy document would be strengthened by source referencing for different statements and data.
Need to add a “Glossary of Terms” listing the terminology used in order to assure common understanding of terms.
How to assure that Key Reform Priorities and Approaches agreed through the HSRU will not be forgotten or reversed by a next legislature. To what extent can some be perpetuated by law (or constitution)? Depending its role WHO, as technical agency, could assure the institutional memory of the reform process and contribute to smoother continuation.
Presentation title (change in view slide
master)
Date of presentation
Primary Health Care
Appreciate the focus on PHC, but this section will also require further development•Service Delivery Logic: Coordinated and Integrated with PHC as its cornerstone•Rationale for PHC to be strengthened:
– Continuity, holistic– Ageing population & poly-morbidity– Efficiency, gatekeeping also a HCF issue
•Gatekeeper => Client navigator•Financial access to be covered in the Package of Services free of any charge (no co-payments)•Etc.
Presentation title (change in view slide
master)
Date of presentation
Health Financing• Important Values: Accessibility, Equity, Solidarity (progressive taxation/contribution), Quality, Efficiency• Health for Wealth >< Health sector already under financed budget cuts to be directed to other sectors • UHC “Free Health Care for All” not unachievable (achieved by countries such as Thailand and Brasil
(GDP>), defining service package, efficiency of systems. To the opposite Ukraine has very high OOP levels.• Too strong a focus on involvement of Private Sector and self-regulating markets.
– Health services market not governed by normal market principles– International trend towards compulsory public financing using either tax financing or compulsory
social health insurance contributions – (Private) Voluntary Health Insurances no added value
• If introduced a National Health Insurance Scheme should be Compulsory and Progressive (solidarity)• New HCF vision looks at its functions Collection, Pooling, Purchasing and Coverage Policy rather than on
the systems• Several efficiency measures are required (Hospital Sector, Pharmaceutical Sector, PPMs, Input-based
budget system)Necessity to improve Health Service Management: “Regulated” Management Autonomy with sound efficient management principles (cave user-fee proliferation => access )
• Cave! Complexity of multitude of systems (government budgets, co-payments, VHI, compulsory HI, different packages of activities, fragmented service provision systems, etc) will require strong regulations and monitoring. This will require a very heavy and COSTLY Administration and Monitoring System.
• Don’t forget the Public Health Services Budget

Presentation title (change in view slide
master)
Date of presentation
The insurance function in health
Old thinking: classifications or models
‘National health system’
‘Social health insurance’
‘Semashko’
New thinking:functions and policies
CollectionPoolingPurchasingCoverage policy
Are Germans more insured than the British, Swedes or Cypriots just because they call their system ‘insurance’?
Understand systems (and reform options) in terms of functions, not labels or models
Source: Joseph Kutzin, WHO
Presentation title (change in view slide
master)
Date of presentation
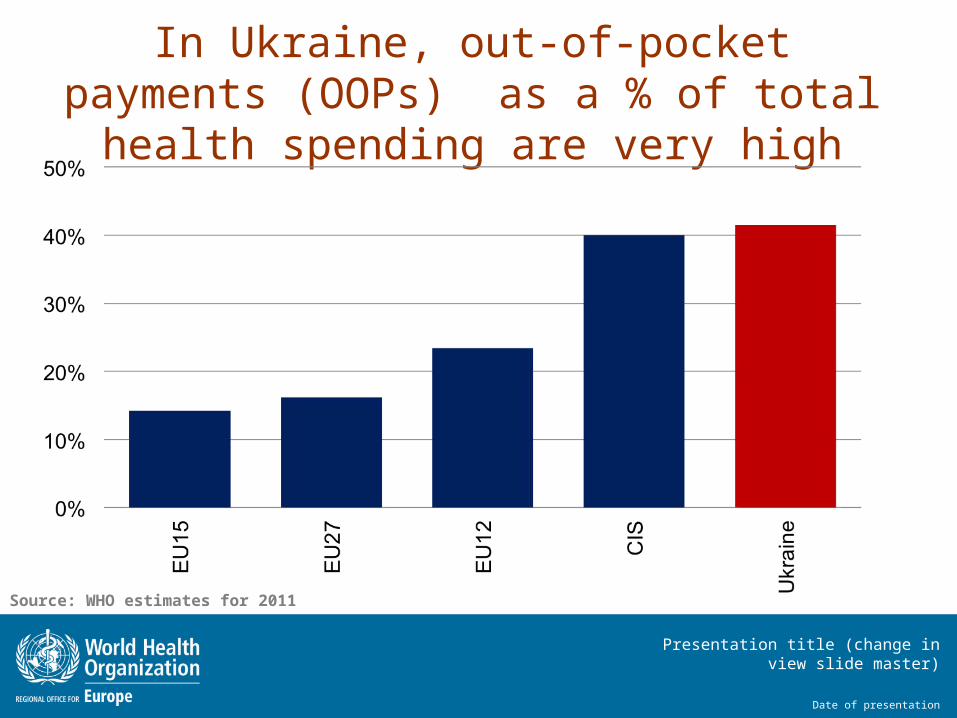
In Ukraine, out-of-pocket payments (OOPs) as a % of total health spending are very high
Source: WHO estimates for 2011

Presentation title (change in view slide
master)
Date of presentation
OOPs are high where governmentsspend less on health
Source: WHO estimates for 2012, selected countries with population > 600,000
Presentation title (change in view slide
master)
Date of presentation
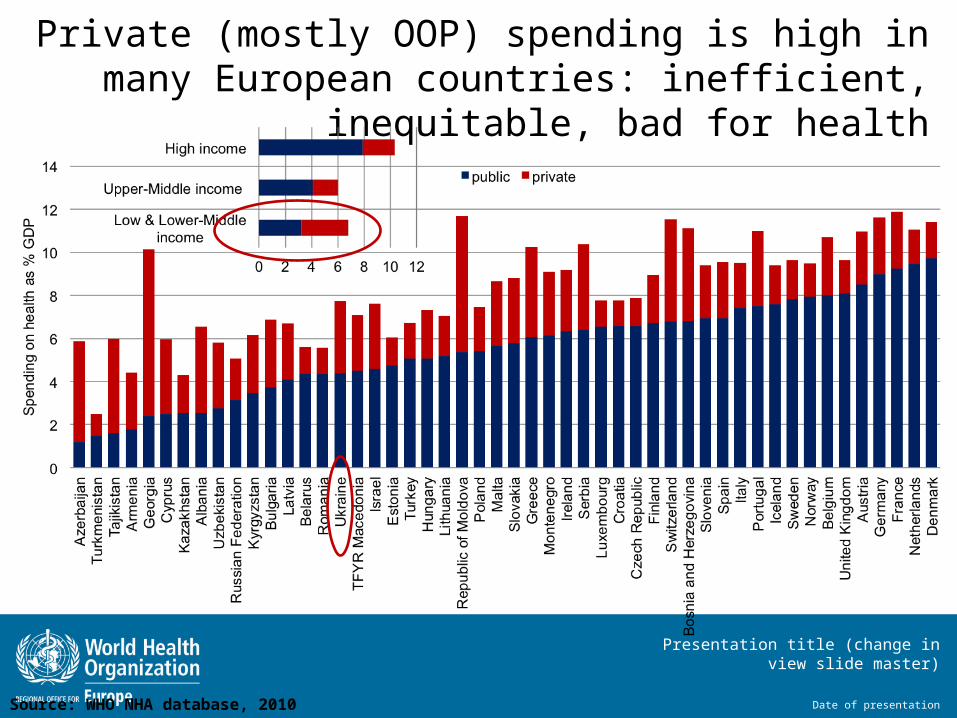
Private (mostly OOP) spending is high in many European countries: inefficient, inequitable, bad for
health
Source: WHO NHA database, 2010
Presentation title (change in view slide
master)
Date of presentation
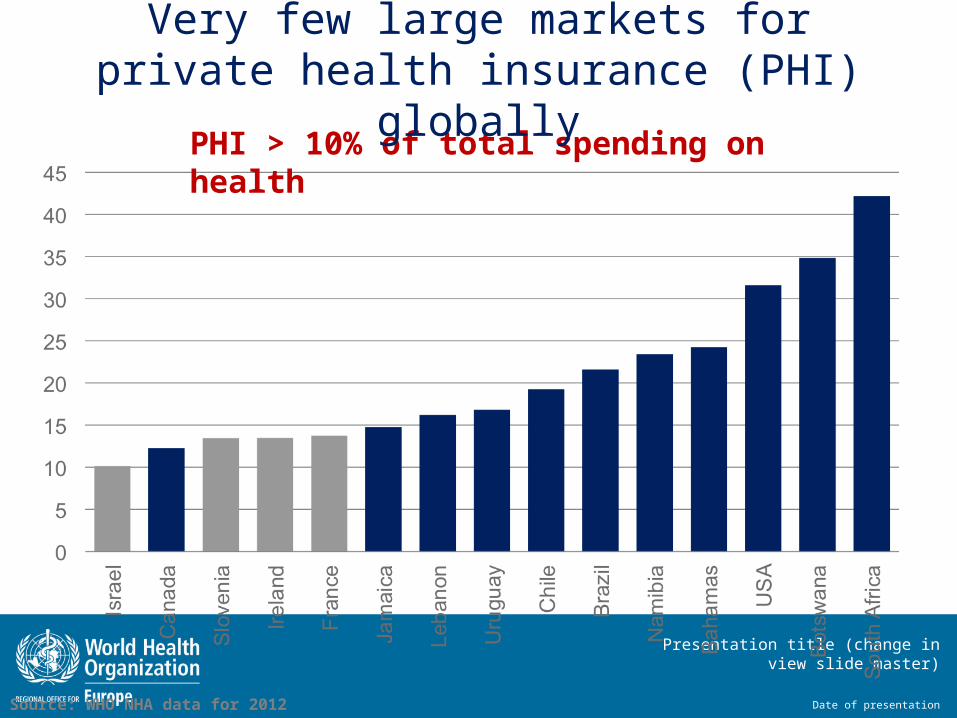
PHI > 10% of total spending on health
Very few large markets for private health insurance (PHI) globally
Source: WHO NHA data for 2012

Presentation title (change in view slide
master)
Date of presentation
PHI ranked by share (%) of private spending on health (from high to low) shows thatPHI does not do well in filling gaps in public coverage
Source: WHO data for 2011

Presentation title (change in view slide
master)
Date of presentation
Public Health
Promotion and prevention population level services should get special and increased attention.
Addressing social determinants through promotion and prevention (including taxation and other legislation) are mostly very effective and efficient actions.
– NCD crisis
– Immunization levels
PH functions need to be assessed and, after political and technical decisions, defined and organized into an efficient and effective PH system which receives adequate funding.
Presentation title (change in view slide
master)
Date of presentation
Human Resources for Health
Very important but underdeveloped component•Need for Health workforce development plan (present situation, projections and need assessment)•Revising professional education and compulsory continuous education (medical, nursing and other professionals), in line with EU standards•Training of Health Services Managers (hospitals, clinics, health administration)•Staff motivation: performance monitoring, incentives and changes in career path;
Remuneration revisions; How to get staff to rural remote areas (rural hardship allowances?)
•Close linked with other reform components; autonomous management of institutions, registration and licensing, CISHD and PHC, etc. •Need for strong Dual Practice regulations certainly in case of further privatization.

Presentation title (change in view slide
master)
Date of presentation
Others suggestions to the Strategy
Given the important and recognized “Corruption” problems it might be worthwhile to address this as a separate topic (not only under the Purchaser-Provider Split and Purchasing Agency; (Procurement problems, Informal payments, Under Table Payments (UTP), ghost staff and patients, etc.) with a description, analysis and recommendations.

Presentation title (change in view slide
master)
Date of presentation
Summary