presentatie dr. deborah falla
TRANSCRIPT

1
MUSCLE DYSFUNCTION IN CERVICAL PAIN AND THE IMPLICATIONS FOR TRAINING
Deborah Falla
CENTER FOR ANESTHESIOLOGY, EMERGENCY AND INTENSIVE CARE MEDICINE, UNIVERSITY HOSPITAL GÖTTINGEN, GERMANY
DEPARTMENT OF NEUROREHABILITATION ENGINEERINGBERNSTEIN CENTER FOR COMPUTATIONAL NEUROSCIENCEUNIVERSITY MEDICAL CENTER GÖTTINGEN, GERMANY
� Changes in sensorimotor control are an almost obligatory feature of musculoskeletal conditions
� Evidence for modification of motor and/or sensory functions has been reported for a broad array of conditions, and these changes have become common targets for rehabilitation
� It has been assumed that sensorimotor changes are relevant for the development, perpetuation or recurrence of pain and/or injury
� Reflect on these assumptions in relation to neck pain
Models of motor adaptation to pain
Musclepain
Group III & IVexcitation
Increasedmuscle activity
Muscleischemia
Vicious cycle theoryJohansson & Sojka. 1991
Musclepain
Group III & IV excitation
Decreased agonisticmuscle activity
Increased antagonisticmuscle activity
Inhibition ofα-motoneurons
Excitationα-motoneurons
This pathway is facilitated in case of agonistic muscle
activity
This pathway is facilitated in case of antagonistic
muscle activity
Pain adaptation theoryLund. Can J Physiol Pharmacol. 1991

2
Contemporary theory proposes that the motor adaptation:
(i) involves a diversity of changes from subtle changes in the distribution of activity within and between muscles
to complete/relative avoidance of movement;
(ii) is specific to the individual;
(iii) has a general aim (at least in the short term) to protect the painful/threatened body part from real or
anticipated further pain/injury;
(iv) may precede or follow the onset of pain/injury;
(v) has potential long term consequences if it is maintained, excessive or inappropriate
Hodges and Falla. GMMPT. 2015
Contemporary theory proposes that the motor adaptation:
(i) involves a diversity of changes from subtle changes in the distribution of activity within and between muscles
to complete/relative avoidance of movement;
(ii) is specific to the individual;
(iii) has a general aim (at least in the short term) to protect the painful/threatened body part from real or
anticipated further pain/injury;
(iv) may precede or follow the onset of pain/injury;
(v) has potential long term consequences if it is maintained, excessive or inappropriate
Hodges and Falla. GMMPT. 2015
Contemporary theory proposes that the motor adaptation:
(i) involves a diversity of changes from subtle changes in the distribution of activity within and between muscles
to complete/relative avoidance of movement;
(ii) is specific to the individual;
(iii) has a general aim (at least in the short term) to protect the painful/threatened body part from real or
anticipated further pain/injury;
(iv) may precede or follow the onset of pain/injury;
(v) has potential long term consequences if it is maintained, excessive or inappropriate
Hodges and Falla. GMMPT. 2015
3
100 200 300mV0
10
20
30
40
•
200
400
600
800
1000
1200
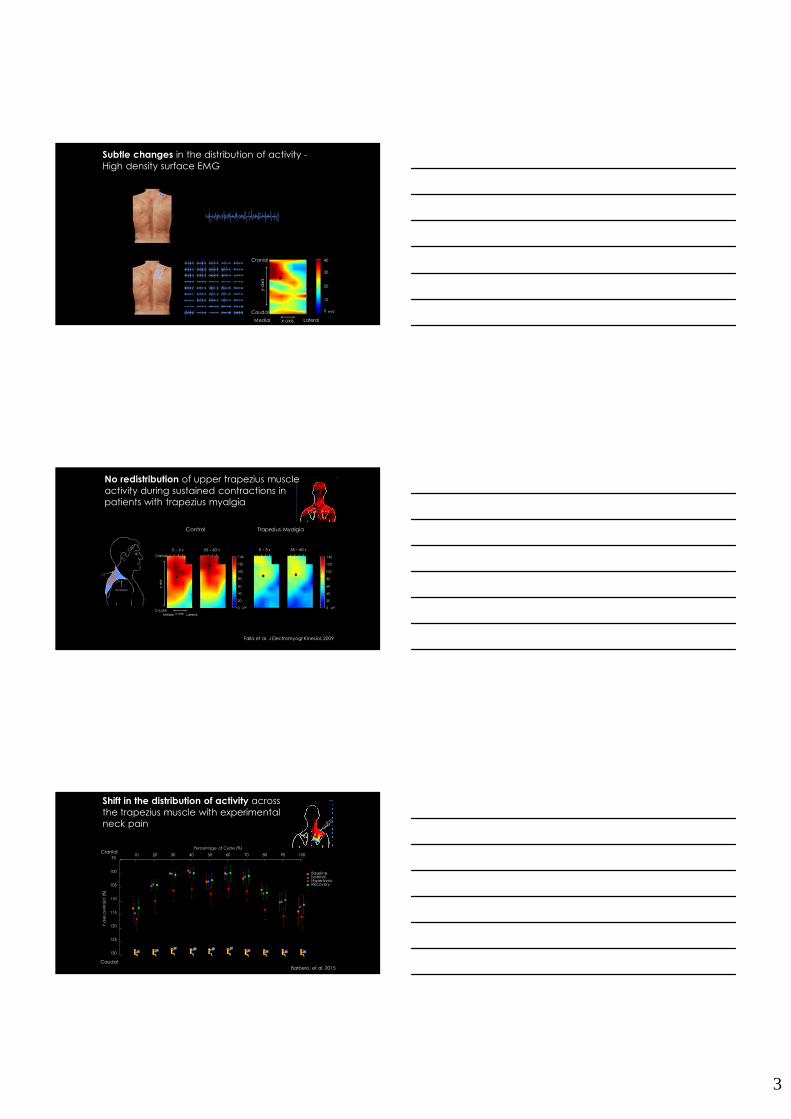
Subtle changes in the distribution of activity -High density surface EMG
LateralMedial
Cranial
Caudal
y-axis
x-axis
No redistribution of upper trapezius muscle activity during sustained contractions in patients with trapezius myalgia
Control
Cranial
Caudalx-axis
y-a
xis
Medial Lateral
0 – 5 s 55 – 60 s
140
120
100
80
60
40
20
0 µV
Trapezius Myalgia
0 – 5 s 55 – 60 s
Falla et al. J Electromyogr Kinesiol. 2009
140
120
100
80
60
40
20
0 µV
acromion
C7
Shift in the distribution of activity across the trapezius muscle with experimental neck pain
Barbero, et al. 2015
BaselineIsotonicHypertonicRecovery
10 20 30 40 50 60 70 80 90 10095
100
105
110
115
120
125
130
Percentage of Cycle (%)
Y-a
xis
ce
ntr
oid
(%
)
*
*
**
*
**
*
*
Caudal
Cranial
*
4
Contemporary theory proposes that the motor adaptation:
(i) involves a diversity of changes from subtle changes in the distribution of activity within and between muscles
to complete/relative avoidance of movement;
(ii) is specific to the individual;
(iii) has a general aim (at least in the short term) to protect the painful/threatened body part from real or
anticipated further pain/injury;
(iv) may precede or follow the onset of pain/injury;
(v) has potential long term consequences if it is maintained, excessive or inappropriate
Hodges and Falla. GMMPT. 2015
Persistence of the motor adaptation could also underpin reduced
“confidence” in the injured /painful region, thus promoting disuse or
modified use of the body part, that is, the adapted motor behaviour could
interact with psychosocial issues
Contemporary theory proposes that the motor adaptation:
(i) involves a diversity of changes from subtle changes in the distribution of activity within and between muscles
to complete/relative avoidance of movement;
(ii) is specific to the individual;
(iii) has a general aim (at least in the short term) to protect the painful/threatened body part from real or
anticipated further pain/injury;
(iv) may precede or follow the onset of pain/injury;
(v) has potential long term consequences if it is maintained, excessive or inappropriate
Hodges and Falla. GMMPT. 2015
5
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
EMG
am
plit
ud
e n
orm
alis
ed
to b
ase
line
S1 S2 S3 S4 S5 S6 S7 S8
RHYO
RSTER
RSCA
RUTR
RLTRLHYO
LSTER
LSCA
LSPLLUTR
LLTR
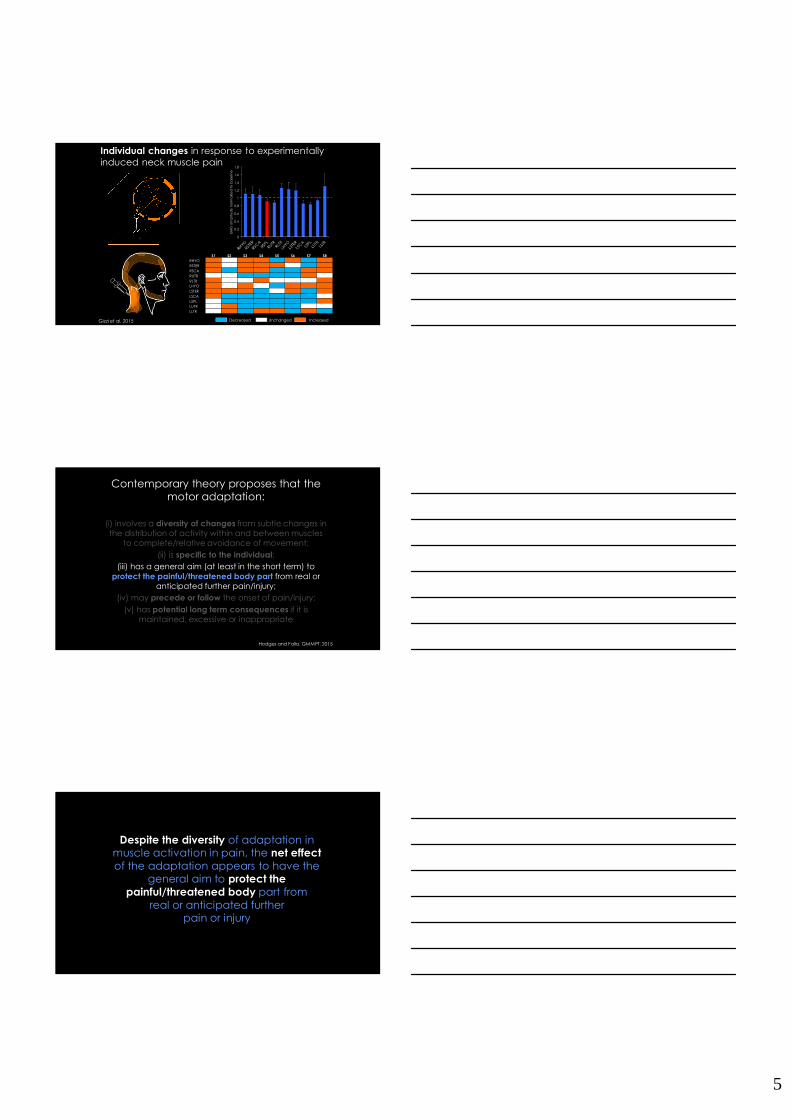
Gizzi et al. 2015
Individual changes in response to experimentally induced neck muscle pain
Decreased Unchanged Increased
Contemporary theory proposes that the motor adaptation:
(i) involves a diversity of changes from subtle changes in the distribution of activity within and between muscles
to complete/relative avoidance of movement;
(ii) is specific to the individual;
(iii) has a general aim (at least in the short term) to protect the painful/threatened body part from real or
anticipated further pain/injury;
(iv) may precede or follow the onset of pain/injury;
(v) has potential long term consequences if it is maintained, excessive or inappropriate
Hodges and Falla. GMMPT. 2015
Despite the diversity of adaptation in muscle activation in pain, the net effect
of the adaptation appears to have the general aim to protect the
painful/threatened body part from real or anticipated further
pain or injury
6
60
240
30
210
0
180
330
150
300
120
270 90
60
240
30
210
0
180
330
150
300
120
270 90
Left Sternocleidomastoid Right Sternocleidomastoid
Left Splenius Capitis Right Splenius Capitis
60
240
30
210
0
180
330
150
300
120
270 90
60
240
30
210
0
180
330
150
300
120
270 90
°
°
°
°
mean resultant vector (preferred direction)
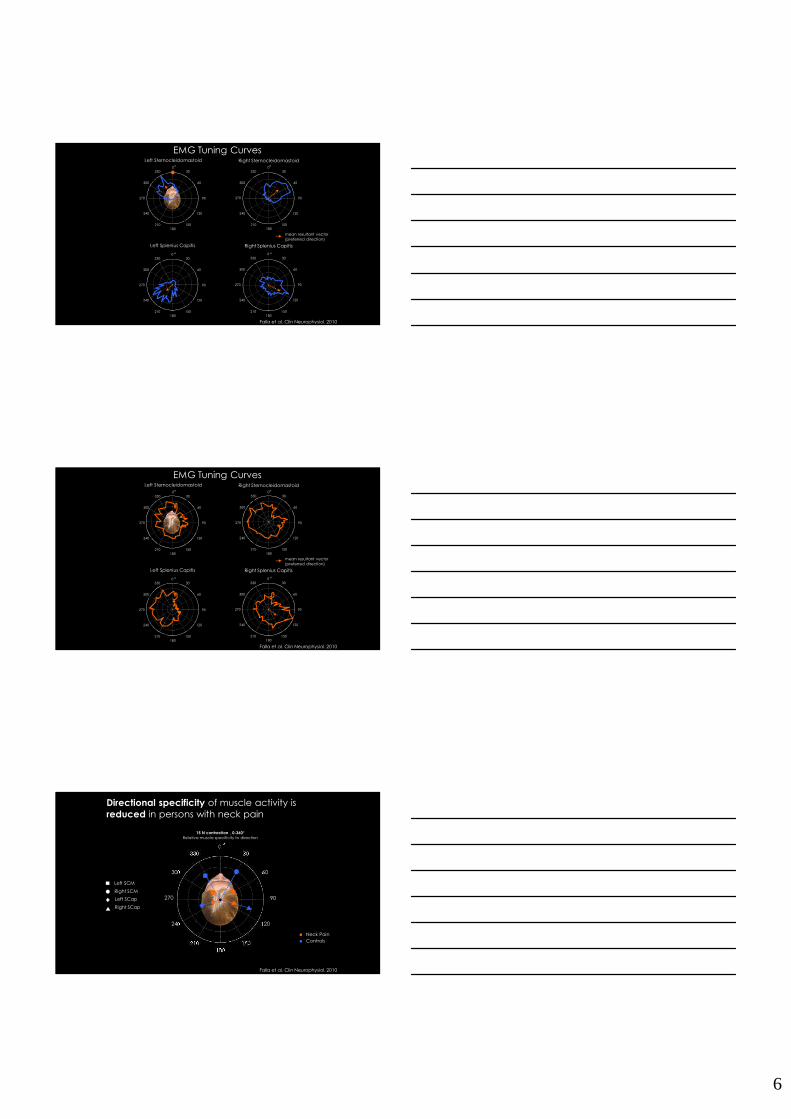
Falla et al. Clin Neurophysiol. 2010
EMG Tuning Curves
Left Sternocleidomastoid Right Sternocleidomastoid
Left Splenius Capitis Right Splenius Capitis
60
240
30
210180
330
150
300
120
270 90
60
240
30
210180
330
150
300
120
270 90
0 0° °
60
240
30
210180
330
150
300
120
270 90
60
240
30
210180
330
150
300
120
270 90
0 0° °
mean resultant vector (preferred direction)
Falla et al. Clin Neurophysiol. 2010
EMG Tuning Curves
60
240
30
210
0
180
330
150
300
120
270 90
°
Directional specificity of muscle activity is reduced in persons with neck pain
15 N contraction , 0-360°
Relative muscle specificity to direction
Neck PainControls
Left SCM
Right SCM
Left SCap
Right SCap
Falla et al. Clin Neurophysiol. 2010
7
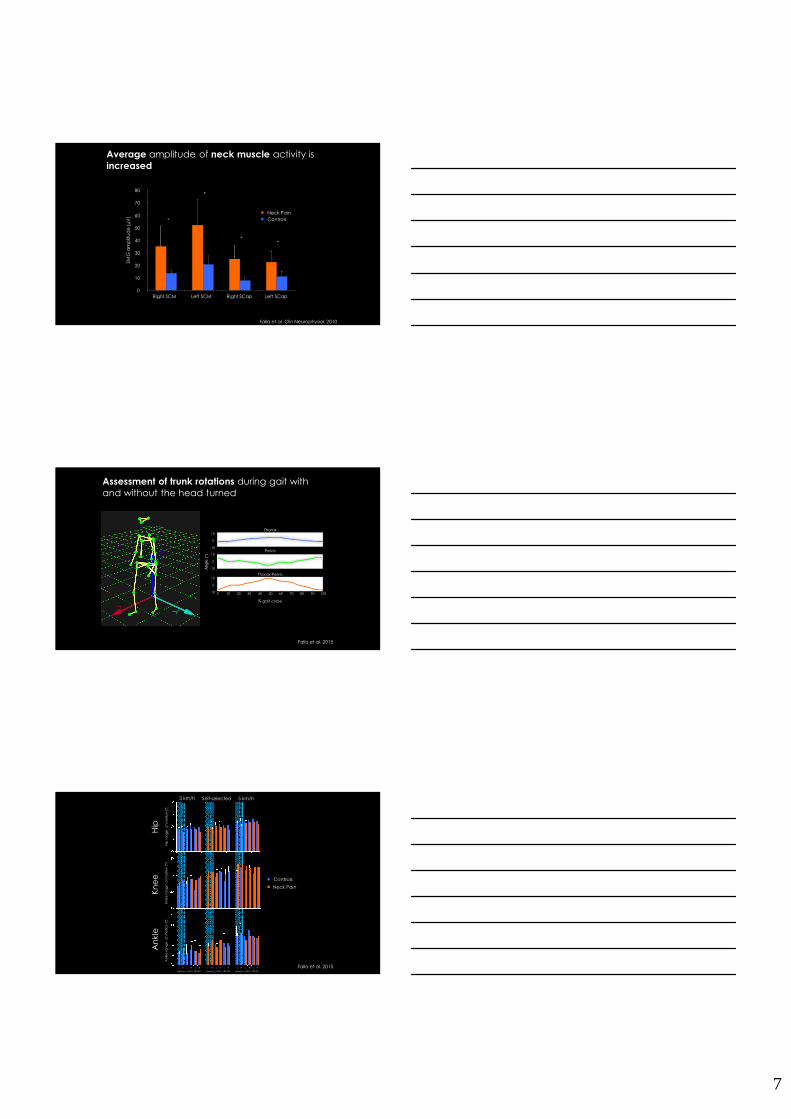
Average amplitude of neck muscle activity is increased
0
10
20
30
40
50
60
70
80
Right SCM Left SCM Right SCap Left SCap
Neck PainControls
EMG
am
plit
ud
e (
µV
)
Falla et al. Clin Neurophysiol. 2010
*
*
**
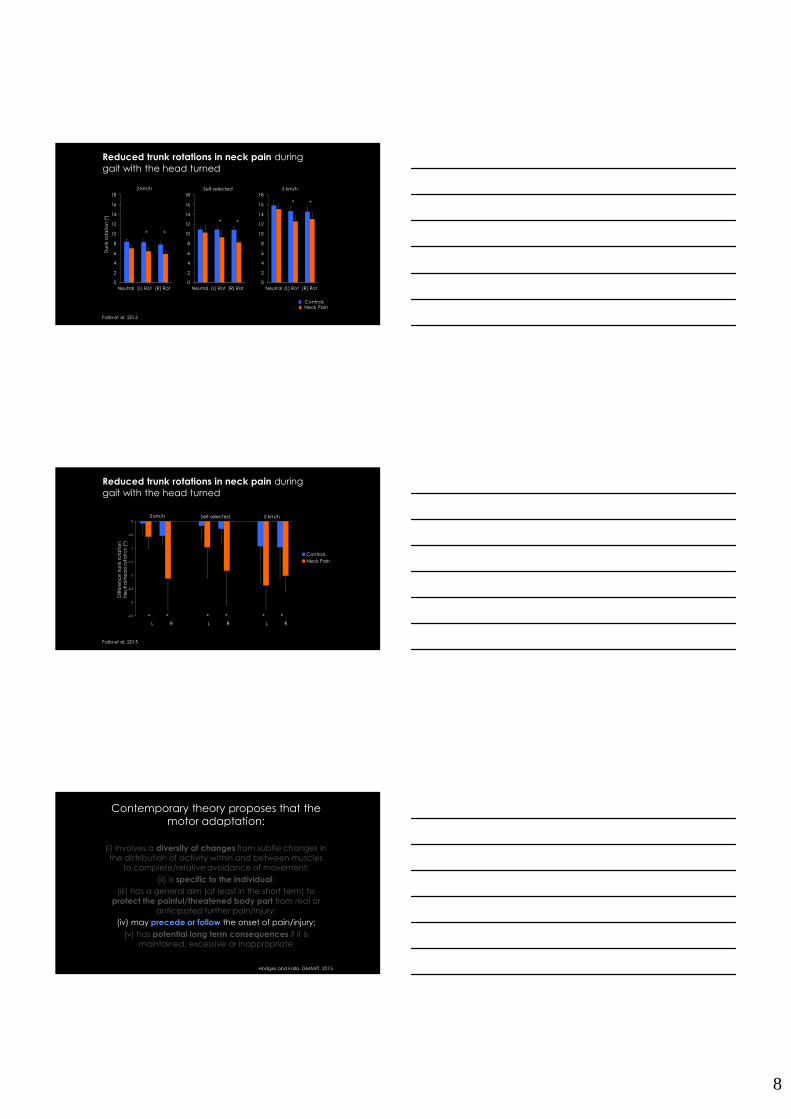
Assessment of trunk rotations during gait with and without the head turned
Falla et al. 2015
Pelvis
0 10 20 30 40 50 60 70 80 90 100-10
0
10
% gait cycle
Ang
le (
°)
Thorax-Pelvis
-10
0
10Thorax
-10
0
10
Neck Pain
Controls
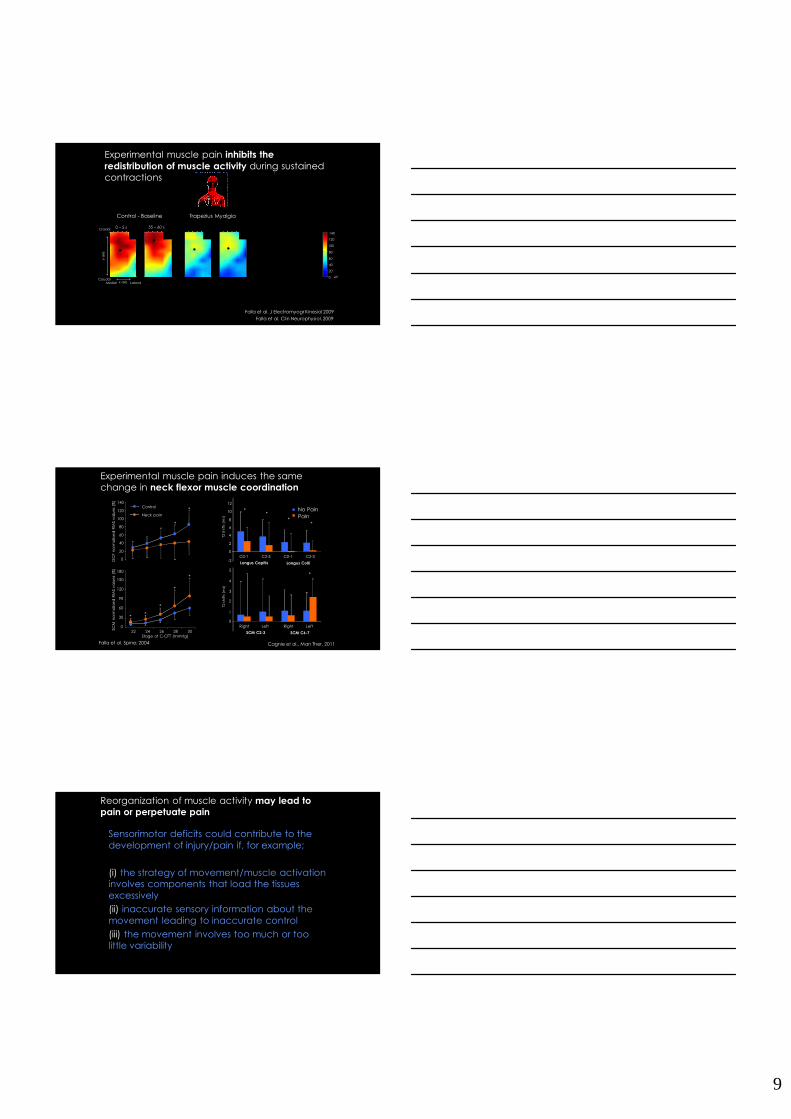
Hip
ra
ng
e
of
mo
tion
(°)
Kn
ee
ra
ng
e
of
mo
tion
(°)
An
kle
ran
ge
o
f m
otio
n (
°)
3 km/h Self-selected 5 km/h
Neutral (L) Rot (R) Rot Neutral (L) Rot (R) Rot Neutral (L) Rot (R) Rot
L R L R L R L R L R L R L R L R L R Falla et al. 2015
Hip
Kn
ee
An
kle
8
0
2
4
6
8
10
12
14
16
18
0
2
4
6
8
10
12
14
16
18
0
2
4
6
8
10
12
14
16
18
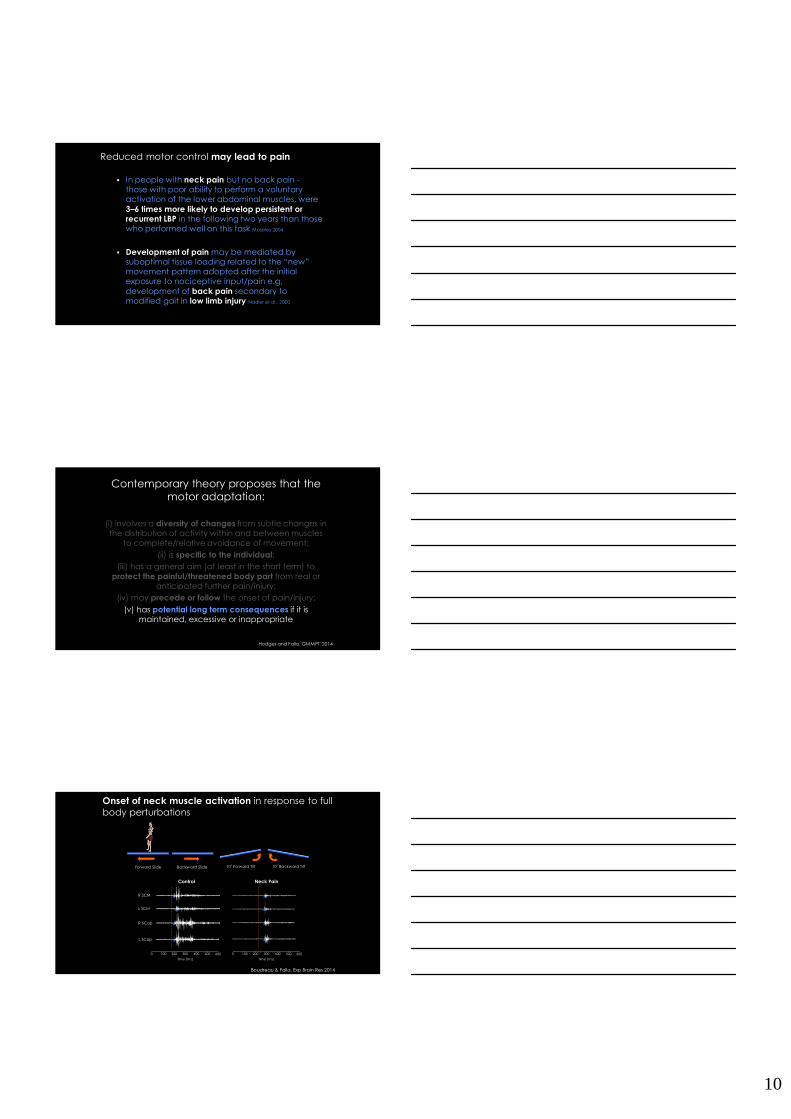
Tru
nk
rota
tio
n (
°)
Neutral (L) Rot (R) Rot Neutral (L) Rot (R) Rot Neutral (L) Rot (R) Rot
3 km/h Self-selected 5 km/h
Neck PainControls
Falla et al. 2015
Reduced trunk rotations in neck pain during gait with the head turned
* *
* *
* *
Reduced trunk rotations in neck pain during gait with the head turned
Diff
ere
nc
e t
run
k ro
tati
on
: N
eu
tra
l-he
ad
ro
tati
on
(°)
Neck Pain
Controls
3 km/h Self-selected 5 km/h
L R L R L R
-3.5
-3
-2.5
-2
-1.5
-1
-0.5
0
* * * * * *
Falla et al. 2015
Contemporary theory proposes that the motor adaptation:
(i) involves a diversity of changes from subtle changes in the distribution of activity within and between muscles
to complete/relative avoidance of movement;
(ii) is specific to the individual;
(iii) has a general aim (at least in the short term) to protect the painful/threatened body part from real or
anticipated further pain/injury;
(iv) may precede or follow the onset of pain/injury;
(v) has potential long term consequences if it is maintained, excessive or inappropriate
Hodges and Falla. GMMPT. 2015
9
Trapezius Myalgia
0 – 5 s 55 – 60 s
140
120
100
80
60
40
20
0 µV
Control - Baseline Acute Experimental Pain
Cranial
Caudalx-axis
y-a
xis
Medial Lateral
0 – 5 s 55 – 60 s 0 – 5 s 55 – 60 s
Experimental muscle pain inhibits the
redistribution of muscle activity during sustained contractions
Falla et al. J Electromyogr Kinesiol 2009
Falla et al. Clin Neurophysiol. 2009
No PainPain
0
2
4
6
8
10
12
T2 s
hif
ts (
ms)
-2C0-1
Longus Capitis
C2-3 C0-1
Longus Colli
C2-3
**
**
0
1
2
3
4
5
T2 s
hif
ts (
ms)
Right
SCM C2-3
Left Right
SCM C6-7
Left
*
Cagnie et al., Man Ther, 2011
Experimental muscle pain induces the same change in neck flexor muscle coordination
Control
Neck pain
0
20
40
60
80
100
120
140
Stage of C-CFT (mmHg)
DC
F n
orm
alis
ed
RM
S v
alu
es
(%)
0
30
60
90
120
150
180
22 24 26 28 30
SCM
no
rma
lise
d R
MS
va
lue
s (%
)
*
*
*
**
*
*
Falla et al. Spine; 2004
Sensorimotor deficits could contribute to the development of injury/pain if, for example;
(i) the strategy of movement/muscle activation involves components that load the tissues excessively
(ii) inaccurate sensory information about the movement leading to inaccurate control
(iii) the movement involves too much or too little variability
Reorganization of muscle activity may lead to
pain or perpetuate pain
10
� In people with neck pain but no back pain -those with poor ability to perform a voluntary activation of the lower abdominal muscles, were 3–6 times more likely to develop persistent or recurrent LBP in the following two years than those who performed well on this task Moseley 2004
� Development of pain may be mediated by suboptimal tissue loading related to the “new” movement pattern adopted after the initial exposure to nociceptive input/pain e.g. development of back pain secondary to modified gait in low limb injury Nadler et al., 2000
Reduced motor control may lead to pain
Contemporary theory proposes that the motor adaptation:
(i) involves a diversity of changes from subtle changes in the distribution of activity within and between muscles
to complete/relative avoidance of movement;
(ii) is specific to the individual;
(iii) has a general aim (at least in the short term) to protect the painful/threatened body part from real or
anticipated further pain/injury;
(iv) may precede or follow the onset of pain/injury;
(v) has potential long term consequences if it is maintained, excessive or inappropriate
Hodges and Falla. GMMPT. 2014
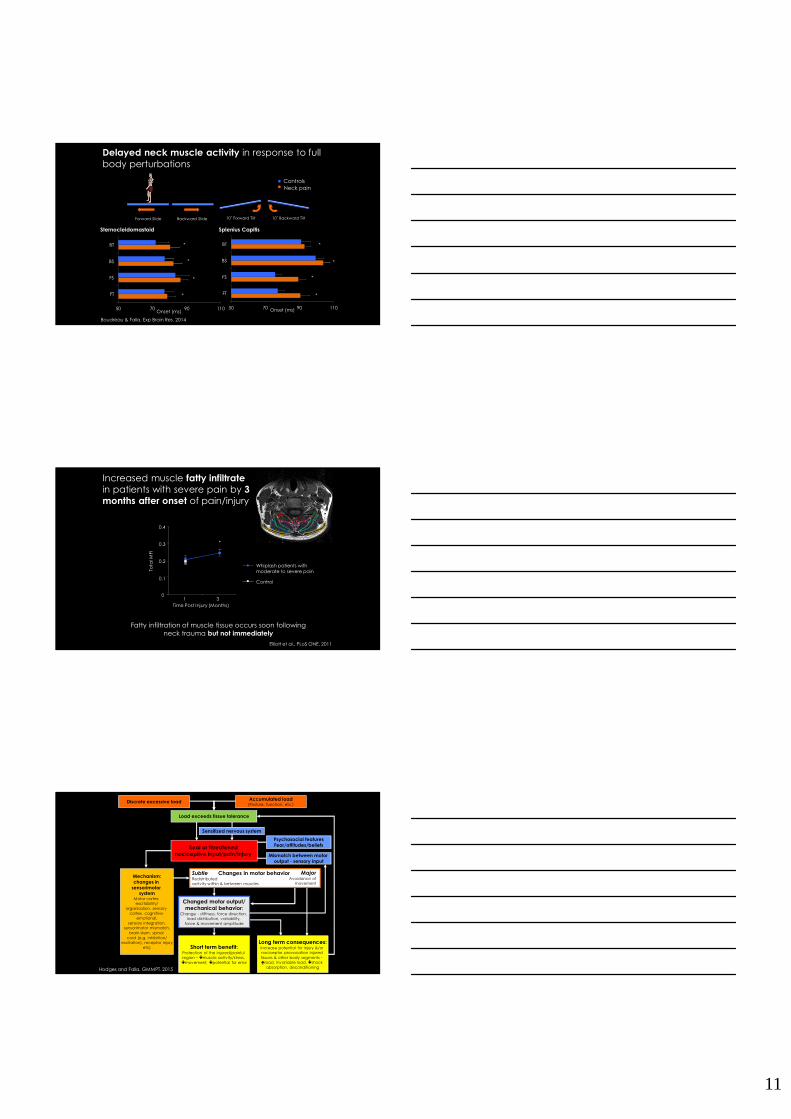
Boudreau & Falla, Exp Brain Res 2014
Onset of neck muscle activation in response to full body perturbations
0 100 200 300 400 500
Time (ms)
Control
R SCM
L SCM
R SCap
L SCap
600
Neck Pain
0 100 200 300 400 500
Time (ms)
600
Forward Slide 10˚ Backward Tilt10˚ Forward TiltBackward Slide
11
Forward Slide 10˚ Backward Tilt10˚ Forward TiltBackward Slide
Boudreau & Falla. Exp Brain Res. 2014
Onset (ms)
Delayed neck muscle activity in response to full body perturbations
ControlsNeck pain
50 70 90 110
FT
FS
BS
BT
50 70 90 110
FT
FS
BS
BT
Onset (ms)
Sternocleidomastoid Splenius Capitis
*
*
*
*
*
*
*
*
Elliott et al., PLoS ONE, 2011
Control
Whiplash patients with moderate to severe pain
Increased muscle fatty infiltrate
in patients with severe pain by 3
months after onset of pain/injury
0
0.1
0.2
0.3
0.4
1 3Time Post Injury (Months)
Tota
l MFI
Fatty infiltration of muscle tissue occurs soon following neck trauma but not immediately
*
Changed motor output/
mechanical behavior:Change - stiffness, force direction,
load distribution, variability, force & movement amplitude
Long term consequences:Increase potential for injury &/or nociceptor provocation injured tissues & other body segments -�load, invariable load, �shock
absorption, deconditioning
Load exceeds tissue tolerance
Discrete excessive loadAccumulated load
(Posture, function, etc.)
Short term benefit:Protection of the injured/painful region – �muscle activity/stress, �movement, �potential for error
Psychosocial features
Fear/attitudes/beliefs
Mismatch between motor
output - sensory input
Subtle Redistributed activity within & between muscles
Sensitized nervous system
Mechanism:
changes in
sensorimotor system
Motor cortex excitability/
organisation, sensory cortex, cognitive-
emotional,sensory integration,
sensorimotor mismatch,brain stem, spinal
cord (e.g. inhibition/excitation), receptor injury
etc)
MajorAvoidance of
movement
Changes in motor behavior
Real or threatened
nociceptive input/pain/injury
Hodges and Falla. GMMPT. 2015
12
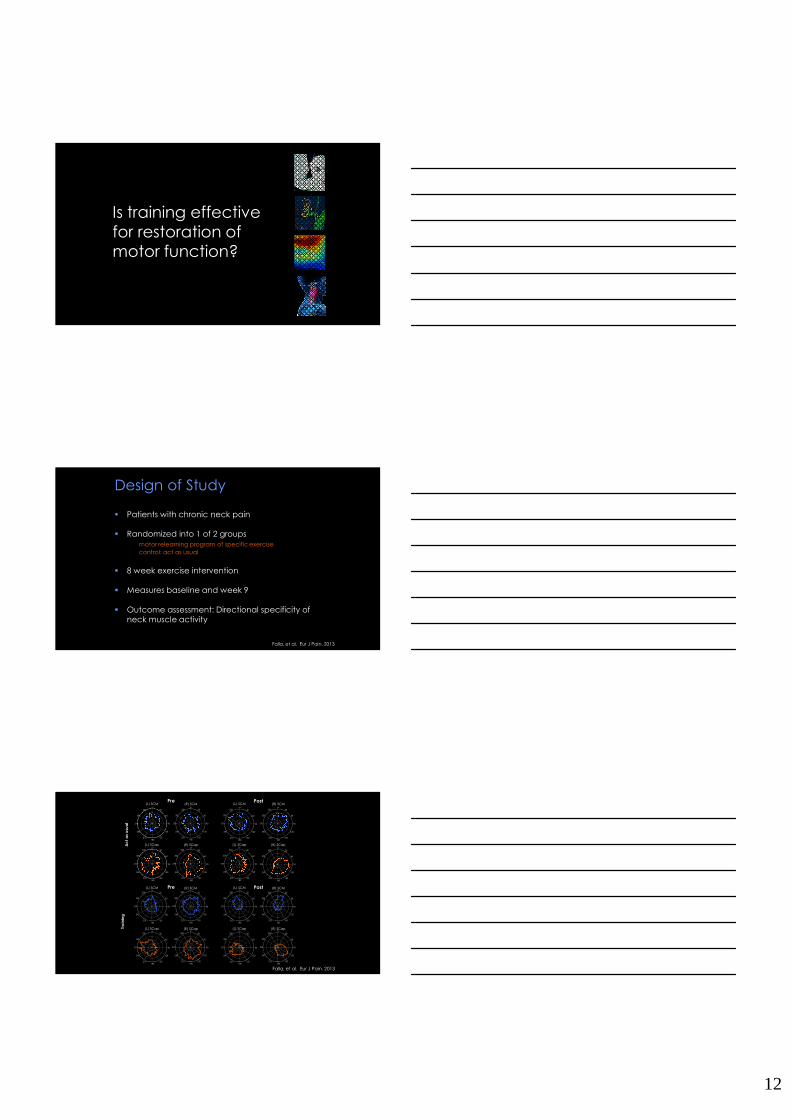
Is training effective for restoration of motor function?
Design of Study
� Patients with chronic neck pain
� Randomized into 1 of 2 groupsmotor relearning program of specific exercise control: act as usual
� 8 week exercise intervention
� Measures baseline and week 9
� Outcome assessment: Directional specificity of neck muscle activity
Falla, et al. Eur J Pain. 2013
60
240
30
210
0°
180
330
150
300
120
270 90
60
240
30
210
0°
180
330
150
300
120
270 90
60
240
30
210
0°
180
330
150
300
120
270 90
60
240
30
210
0°
180
330
150
300
120
270 90
60
240
30
210
0°
180
330
150
300
120
270 90
60
240
30
210
0°
180
330
150
300
120
270 90
60
240
30
210
0°
180
330
150
300
120
270 90
Pre Post
Pre Post
60
240
30
210
0°
180
330
150
300
120
270 90
60
240
30
210
0°
180
330
150
300
120
270 90
60
240
30
210
0°
180
330
150
300
120
270 90
60
240
30
210
0°
180
330
150
300
120
270 90
60
240
30
210
0°
180
330
150
300
120
270 90
60
240
30
210
0°
180
330
150
300
120
270 90
60
240
30
210
0°
180
330
150
300
120
270 90
60
240
30
210
0°
180
330
150
300
120
270 90
Tra
inin
g
Ac
t a
s u
sua
l
(R) SCM(L) SCM
(R) SCap(L) SCap
(R) SCM(L) SCM
(R) SCap(L) SCap
(R) SCM(L) SCM
(R) SCap(L) SCap
(R) SCM(L) SCM
(R) SCap(L) SCap
60
240
30
210
0°
180
330
150
300
120
270 90
Falla, et al. Eur J Pain. 2013
13
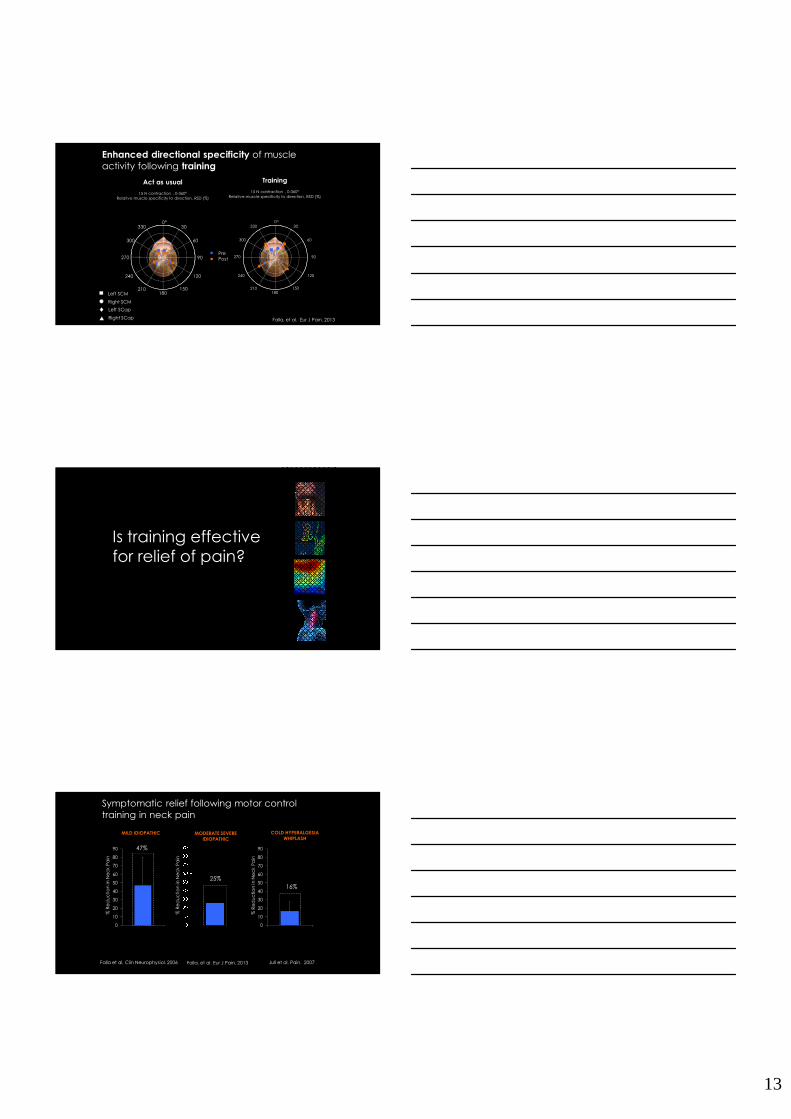
Training
15 N contraction , 0-360°Relative muscle specificity to direction, RSD (%)
Act as usual
15 N contraction , 0-360°Relative muscle specificity to direction, RSD (%)
60
240
30
210
0
180
330
150
300
120
270 90
°
60
240
30
210
0
180
330
150
300
120
270 90
°
PrePost
Left SCM
Right SCM
Left SCap
Right SCap Falla, et al. Eur J Pain. 2013
Enhanced directional specificity of muscle activity following training
Is training effective for relief of pain?
Symptomatic relief following motor control training in neck pain
Falla et al. Clin Neurophysiol. 2006
MILD IDIOPATHIC
Falla, et al. Eur J Pain. 2013 Jull et al. Pain. 2007
0
10
20
30
40
50
60
70
80
90
% R
ed
uc
tio
n in
Ne
ck
Pa
in
Resistance
47%
% R
ed
uc
tio
n in
Ne
ck
Pa
in
25%
MODERATE SEVERE
IDIOPATHIC
COLD HYPERALGESIA
WHIPLASH
16%
% R
ed
uc
tio
n in
Ne
ck
Pa
in
0
10
20
30
40
50
60
70
80
90

14
Numerous clinical trials have demonstrated the efficacy of interventions that target
rehabilitation of sensorimotor control for the management of neck pain
These interventions are more effective when targeted to findings of a detailed assessment
and that people with features consistent with nociceptive pain (e.g. features of pain that
imply a proportional and predictable relationship to mechanical loading) are
more likely to respond favorably
The relative involvement of sensorimotor, psychosocial, and other biological mechanisms
in a patient’s presentation will vary between
individuals and it is not possible to completely separate these mechanisms
A goal is to identify individuals who will benefit
most from rehabilitation targeted at restoration/rehabilitation of sensorimotor
changes and the best methods to address the
underlying mechanisms in those for whom it is relevant