presentasi kasus paru
TRANSCRIPT
Case ReportCase ReportPleural EffusionPleural Effusion
Atika Damayanti
Agustya Dwi Ariani
Hema Meliny J. P.
Raisa Mahmudah
Patient Identity• Full Name : Mrs. K• Sex : Female• Age : 60 years old• Nationality : Javanese• Marital status : Married• Religion : Islam• Occupation : Merchant• Educational background : Elementary School• Address : Pulau Seribu st.
Anamnesis• Taken from : autoanamnesis• Date : June 3rd, 2013• Time : 13.00 pm
• Chief complaint : Chest pain
• Additional complaint : Dry cough, constipation
History of The Present Illness
• Patient came to the hospital at May 31th, 2013 with chest pain on the right side since a week ago. Chest pain being felt suddenly without anything causes. The pain also getting worse when she was sleeping but getting better if she was sitting.
• Patient complained an intermitten dry cough since one month ago. She also complained constipation since 10 days ago.
• Decreased appetite was claimed by patient along with decreased weight. A week ago the patient had undergone pleural pungtion the right pulmo. After that, the patient felt better until came out the hospital.
• The history of taking 6 months drug package or family illness with the same symptom are denied.
The History of IllnessO Patient had experienced :
O Hemorrhoid O InfluenzaO Hypertension
History of Family• Her parent have already dead for unknown
reason at the 65 years old (father) and 55 years old (mother). She also had 2 child which is all are healthy.
Anamnese SystemO Skin : No complaint O Head : No complaintO Eye : No complaintO Ear : No complaintO Nose : No complaintO Mouth : No complaintO Throat : No complaintO Neck : No complaint
Anamnese SystemO Cor/Lung : Patient complained for chest
pain and coughO Abdomen : Patient complained for
constipationO Urogenital : No complaintO Katamenesis : No complaintO Haid : Post MenopauseO Muscles and neuron : No complaintO Extremities : No complaint
WeightO Average weight : unknownO Height : 157 cmO Present Weight : 41 kgO BMI : 16,4 astenicus
O Over all, patient experienced decreasing of her weight
Physical Examination• Skin
Colored olive, general sweating (-), localized sweat (-), hair growth normal, keloid (-), pigmentasi (-), edema (-), arteries : palpable, temperatur per palpable normal
• Lymphatic glandSubmandibula, supraklavikula, neck, armpit : no enlargement
• HeadFace expression normal, symetric, hair : black and grey, temporal artery : normal
• EarDeafnes (-), Foramen (-), Serumen (-), Bleeding (-), Liquid (-)
Physical Examination• Eyes
Exophtalmus (-), enopthalmus (-), palpebra : edema (-) /edema(-), lens : clear/clear, conjungtiva : anemis / anemis, visus : normal, sklera : anicteric
• MouthLips : cyanotic (-/-), tonsil : normal, palatal : normal, faring : normal, tongue : clean/normal
• NeckNo enlargement, JVP : normal
• ChestShape, arterial, and breast : normal
Lung• Inspection :
▫ Front : left : retraction (-), simetric ; right : retraction (-), simetric
▫ Back : left : simetric ; right : simetric• Palpation
▫ Front : left : pain (-), vocal fremitus decreased right : pain (-), vocal fremitus increased
▫ Back : left : pain (-), vocal fremitus decreased right : pain (-), vocal fremitus increased
• Percution▫ Front : left : sonor through ICS 6, right : sonor through ICS 4▫ Back : left : sonor through ICS 6, right : sonor through ICS 4
• Auscultation▫ Front : vesikular decreased in the right side, crackles (-),
wheezing (-)▫ Back : vesikuler normal, crackles (-), wheezing (-)
Cor• Inspection :
Ictus cordis not seen• Palpation :
Ictus cordis palpable at ICS 5 hemithorax sinistra
• Percution :Diffulcult to asses
• Auscultation :Heart sound 1 & 2 regular, murmur (-), gallop (-)
Physical ExaminationO Arteries : normal
O Abdomen :O Inspection : flatO PalpationO Stomach wall : undulation (-), pain (-)O Liver : hepatomegali (-)O Lymph : Splenomegali (-)O Kidney : ballotement (-)
O Percution : tymphaniO Auscultation : bowel sound (+)
Physical Examination• Movement Joint
▫ Arm Muscle : eutonia/eutonia Tones : normal/normal Mass : -/- Joint : normal/normal
▫ Movement : normal/normal▫ Strength : normal/normal
• Heel and legWound/injury : not found, Varices (-), Muscle normal,
Joint normal, Movement normal, Strength/power normal, Edema (-)
Laboratory• Routine Blood
▫ Hb : 8,6 gr/dl▫ WBC : 5400 /ul▫ Diff.count : 0/0/0/75/20/5▫ ESR : 140 mm/hour
• Effusion pleural analisis▫ Macroscopic : seroxantochrom▫ Microscopic : total sel 500 cell/ul, glucose 64 mg/dl,
protein 4,9 gr/dl, chloride (-), PMN 1%, MN 99%, rivalta test (-), LDH : 101 mg/dl, PH : 8
▫ cytologic analisis : no malignancy
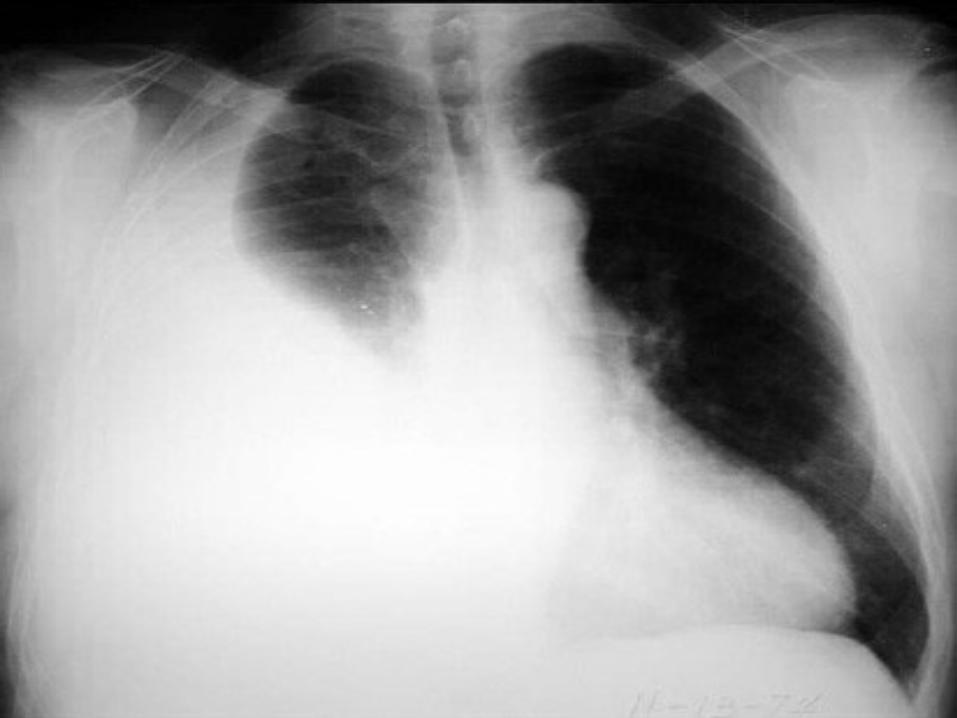
Chest X-ray
DiagnoseO Pleural effusion caused by
congestice heart failure
TreatmentO Pleural punction
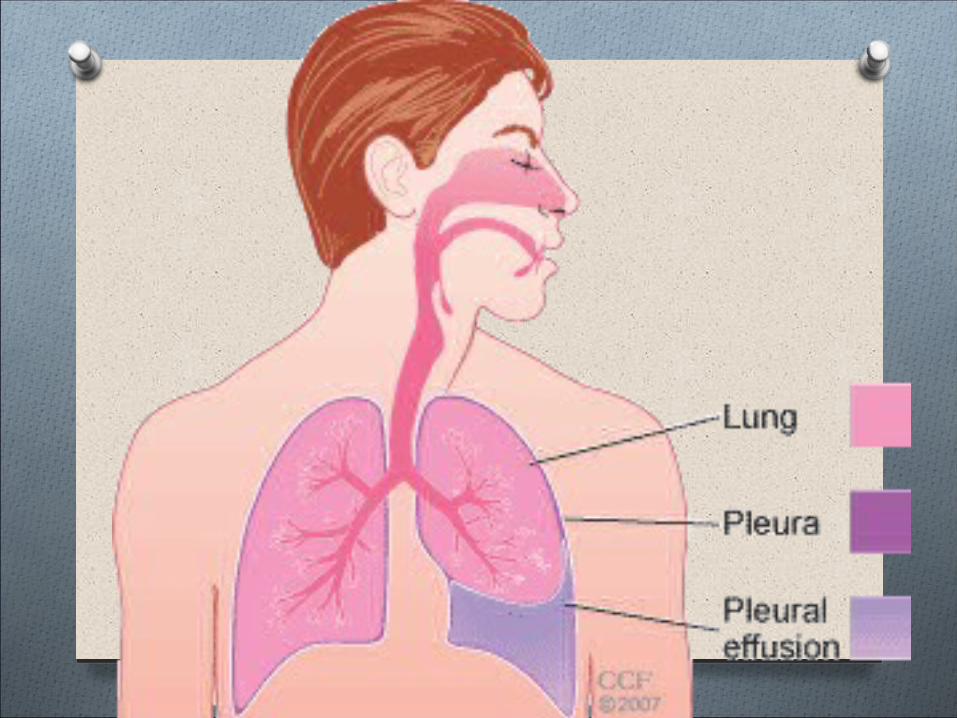
O Pleural effusion is an abnormal accumulation of fluid in the pleural space.
O Up to 25 ml of pleural fluid is normally present in the pleural space, an amount not detectable on conventional chest radiographs.
Pleural Effusion
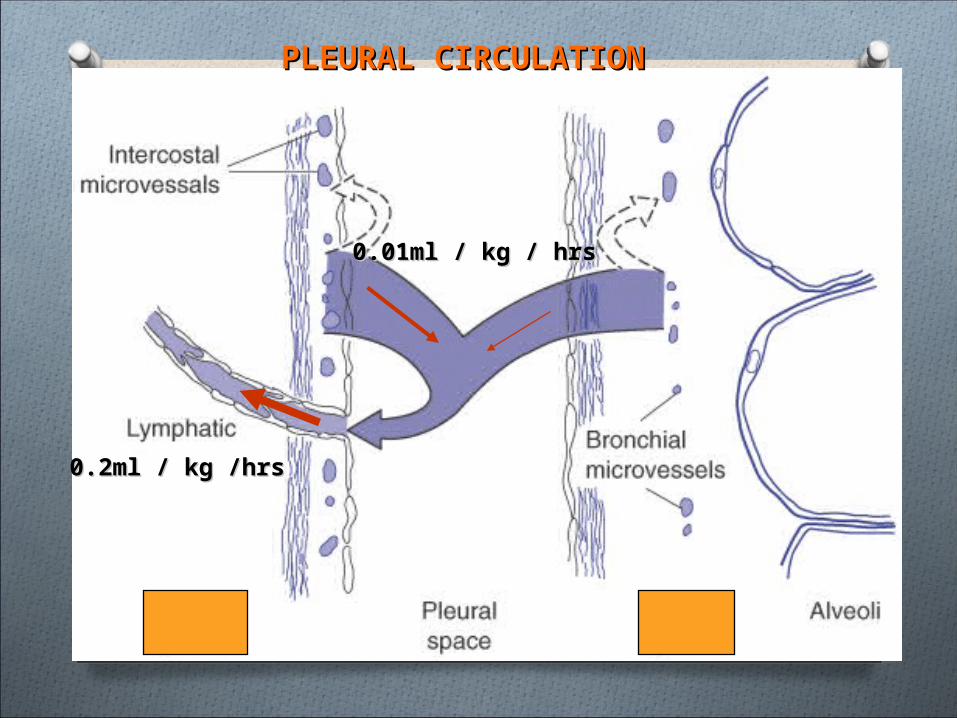
PLEURAL CIRCULATIONPLEURAL CIRCULATION
0.01ml / kg / hrs0.01ml / kg / hrs
0.2ml / kg /hrs0.2ml / kg /hrs
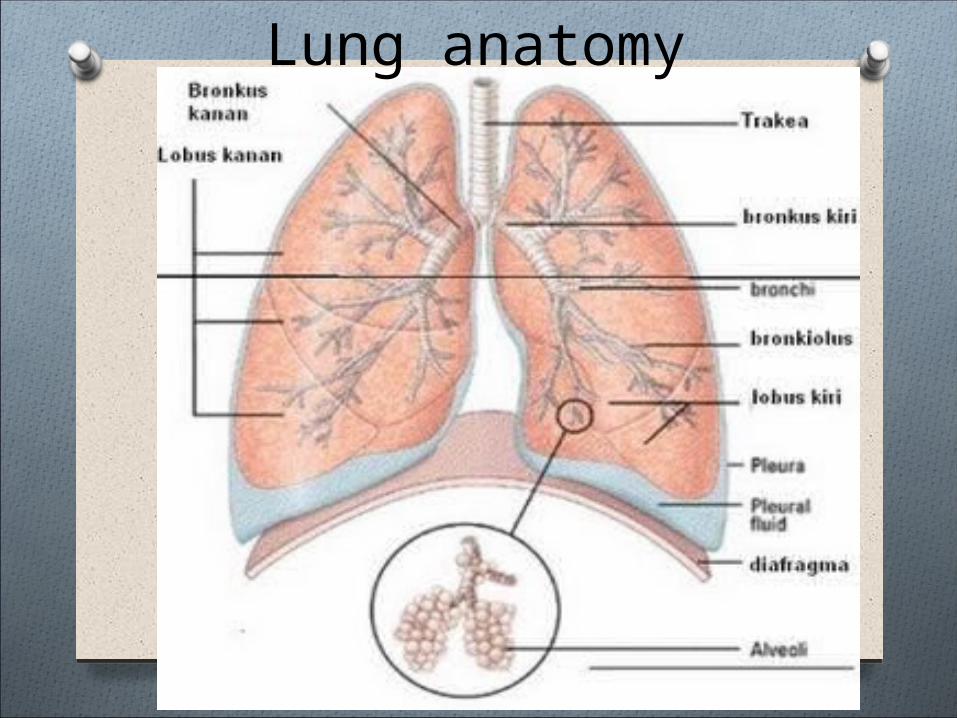
Lung anatomy
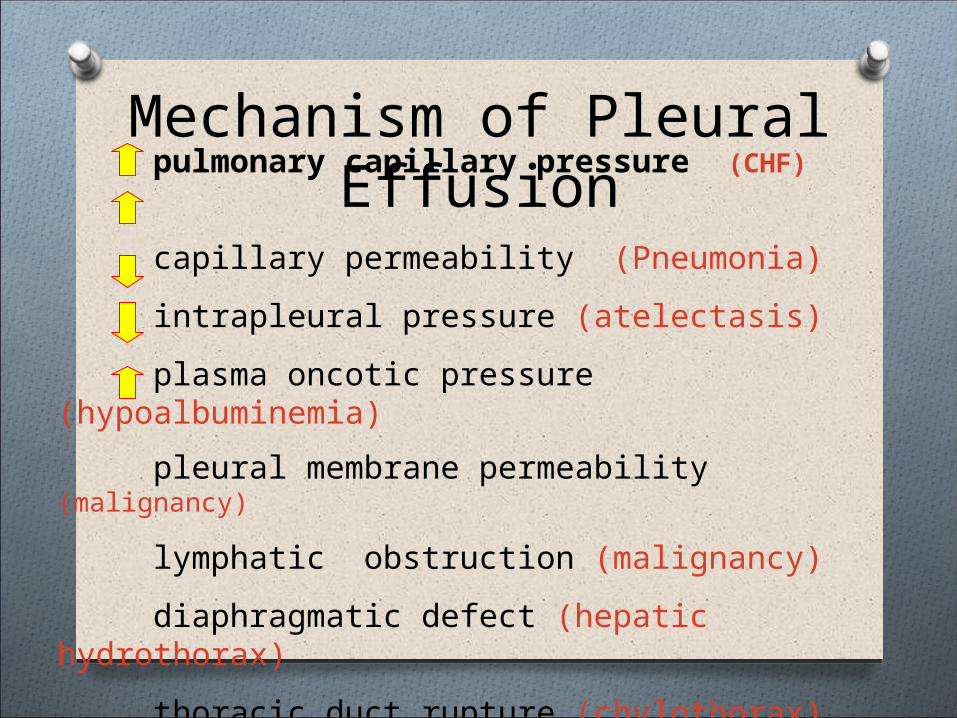
Mechanism of Pleural Effusion
pulmonary capillary pressure (CHF)
capillary permeability (Pneumonia)
intrapleural pressure (atelectasis)
plasma oncotic pressure (hypoalbuminemia)
pleural membrane permeability (malignancy)
lymphatic obstruction (malignancy)
diaphragmatic defect (hepatic hydrothorax)
thoracic duct rupture (chylothorax)
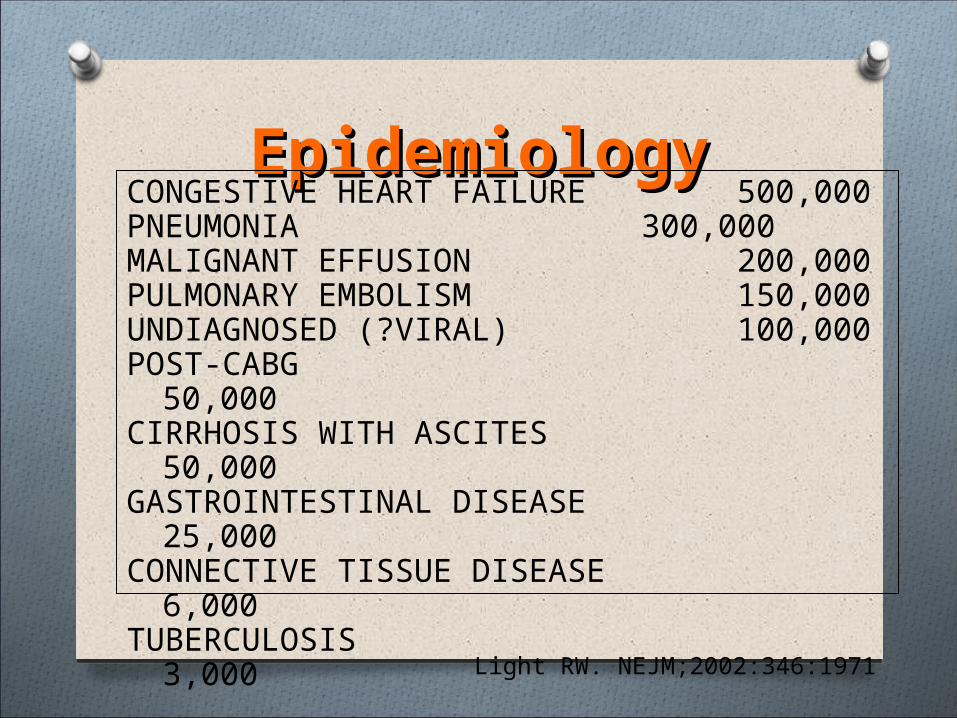
EpidemiologyEpidemiology
Light RW. NEJM;2002:346:1971
CONGESTIVE HEART FAILURE 500,000PNEUMONIA 300,000MALIGNANT EFFUSION 200,000PULMONARY EMBOLISM 150,000UNDIAGNOSED (?VIRAL) 100,000POST-CABG 50,000CIRRHOSIS WITH ASCITES 50,000GASTROINTESTINAL DISEASE 25,000CONNECTIVE TISSUE DISEASE 6,000TUBERCULOSIS 3,000
O The 5 major types of pleural effusion are: O Transudate, O Exudate, O Empyema, O Hemorrhagic pleural effusion or
hemothorax and O Chylous or chyliform effusion
Transudate
OClear, pale yellow, watery substanceO Influenced by systemic factors that alter
the formation or absorption of fluidO Increase in hydrostatic pressure ODecrease in plasma oncotic pressure OContains few protein cellsOCommon causes: CHF and liver or kidney
disease
Exudate
O Pale yellow and cloudy substanceO Influenced by local factors where fluid absorption
is altered (inflammation, infection, cancer) O Rich in protein (serum protein greater than 0.5)O Ratio of pleural fluid LDH and serum LDH is >0.6O Pleural fluid LDH is more the two-thirds normal
upper limit for serumO Rich in white blood cells and immune cellsO Always has a low pHO Common causes: pneumonia, cancer, and
trauma
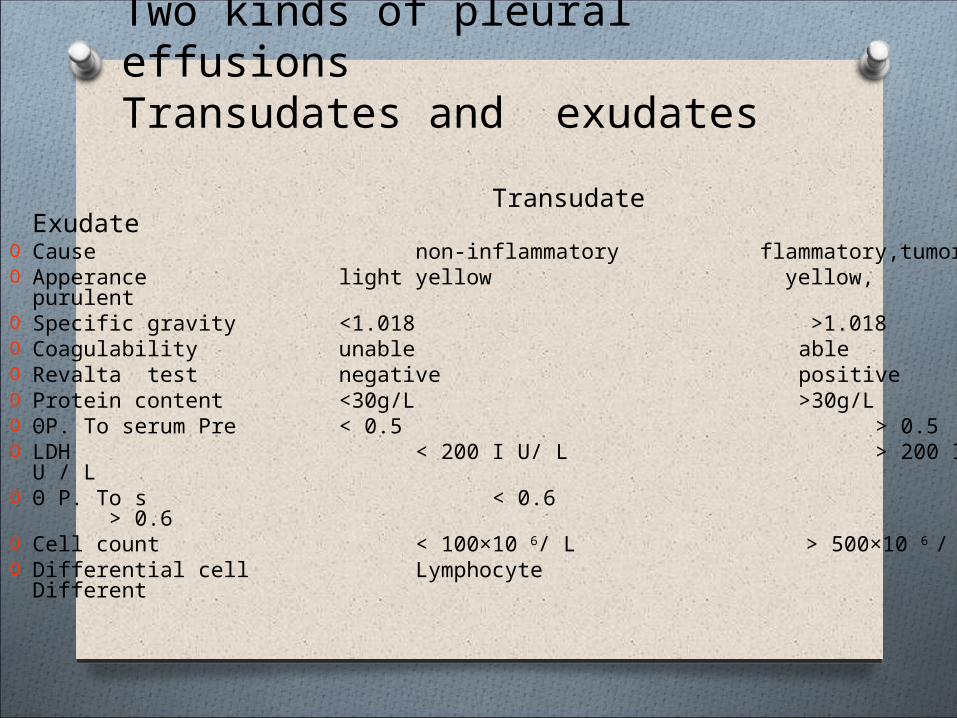
Transudate ExudateO Cause non-inflammatory flammatory,tumorO Apperance light yellow yellow, purulent O Specific gravity <1.018 >1.018O Coagulability unable ableO Revalta test negative positiveO Protein content <30g/L >30g/LO ΘP. To serum Pre < 0.5 > 0.5O LDH < 200 I U/ L > 200 I U / LO Θ P. To s < 0.6 > 0.6O Cell count < 100×10 6/ L > 500×10 6 / LO Differential cell Lymphocyte Different
Two kinds of pleural effusions
Transudates and exudates
O Pleural fluid protein divided by serum protein is greater than 0.5.
O Pleural fluid LDH divided by serum LDH is greater than 0.6.
O Pleural fluid LDH is greater than two-thirds the upper limit of normal for the serum LDH.
O If none of these criteria is met, the patient has a transudative pleural effusion
Light’s criteria
O fever, O pain or the feeling of heaviness in
the side, and O dyspnea (which develops due to
respiratory insufficiency caused by com pression of the lung).
O Cough is usually mild (or absent in some cases)
Clinical Manifestation
O Inspection of the patient reveals asymmetry of the chest due to enlargement of the side where the effusion accumulated; the affected side of the chest usually lags behind respiratory movements.
O Vocal fremitus is not transmitted at the area fluid accumulation
O Dullness percution at the side of effussion
Physical Examination
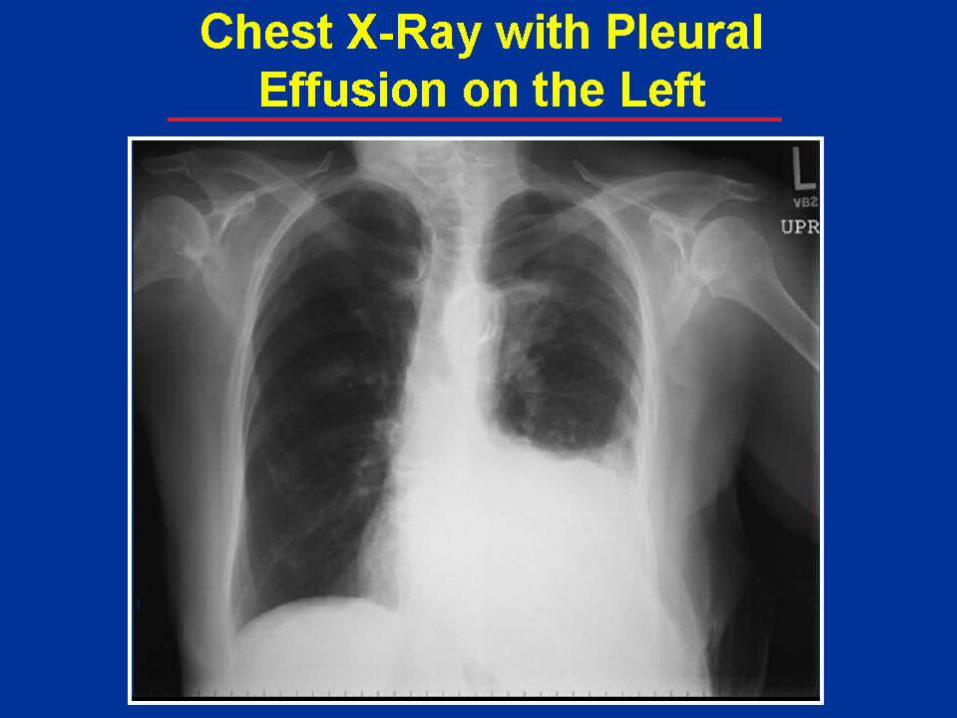
O Radioopaque on the side of effussion, O With lateral position, it can be found
where the effussion happened whether in front or back of the pleura
O Blunting of the normally sharp costophyrenic angle
O a concave shadow with its highest margin along the pleural surface
O shift of the mediastinum and the trachus toward the normal side
Radiology
O Thoracentesis – then treat underlying disease O Uncomplicated pneumonia –
antibioticsO Hemithorax involved/empyema –
tube thoracostomy O Malignant effusion- chest tube +/-
pleurodesis (sclerosants)
Treatment
Pleural Effusion et causa Congestive Heart Failure
O As the heart fails, pressure in the vein going through the lungs starts to rise.
O Due to the heart’s inability to move blood from the pulmonary circulation into the arterial side of systemic circulation, there is a decrease in cardiac output, an increase in left atrial and ventricular end-diastolic pressures, and congestion in the pulmonary circulation.
O As the pressure increases, fluid is pushed into the air spaces (alveoli)
O This fluid then leaks from the alveoli into the pleural space
O This fluid creates a pleural effusion and interrupts normal oxygen movement through the lungs, resulting in shortness of breath
Congestive Heart FailureCHF
O CHF is the most common cause of pleural effusion.
O Frequently the effusions are bilateral (approximately 75% of the time) but may occur alone on either side with the right side being more common.
O Fluid is usually straw colored, with low white blood cell counts (<500 cells/mm3) and a mononuclear cell predominance.
O With severe congestive heart failure, fluid may persist in spite of vigorous diuresis.
(National Lung Health Education Program, 2000)
CHF
Treatment O Thoracocentesis
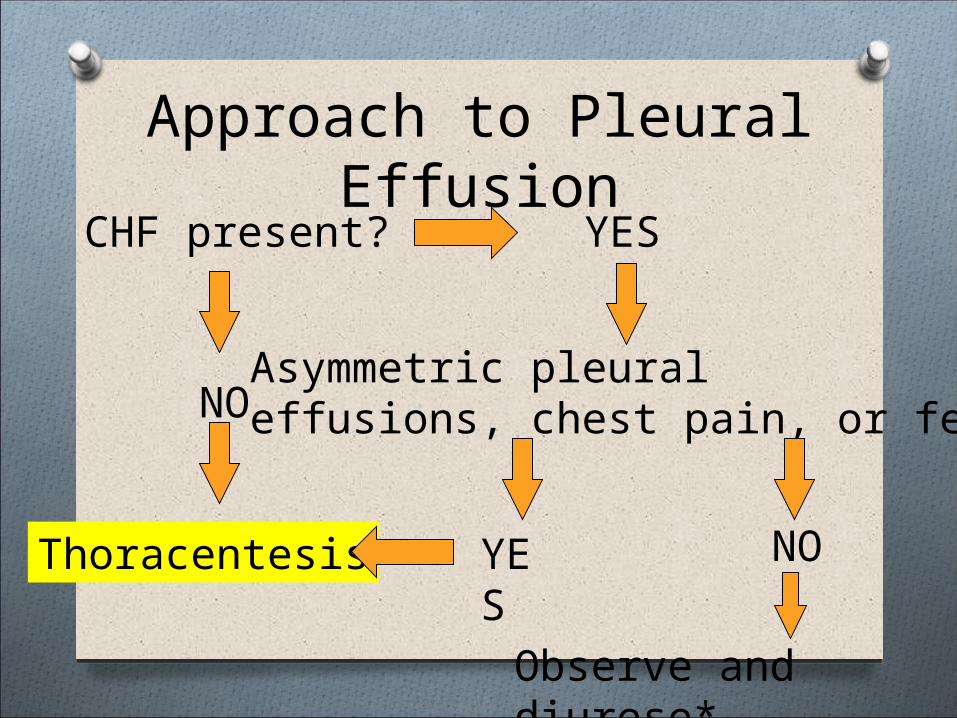
Approach to Pleural Effusion
CHF present?
NO
YES
Thoracentesis
Asymmetric pleuraleffusions, chest pain, or fever?
NO
Observe and diurese*
YES