presentación de powerpoint - forodebateoncologia.net · nuevas vías de señalización en cáncer...
TRANSCRIPT

Nuevas vías de señalización en cáncer de mama
Miquel Àngel Seguí Palmer

Nuevas vías de señalización en cáncer de mama
While the use of endocrine monotherapyremains an effective treatment option formany women, both in the first and secondline settings, the usefulness of endocrinetherapy over time becomes limited bychanges in tumor biology and consequentendocrine resistance.
Increasing understanding of thecomplexity of endocrine receptorsignaling and interactions with multiplesignaling pathways provide a frameworkfor the development and evaluation ofnew agents for use in combination withstandard endocrine therapy.
Emerging targeted agents against breast cancer under clinical development
Nuevas vías de señalización en cáncer de mama
• Selection of patients with advanced breast cancer asappropriate for endocrine manipulation according tohormone receptor status is a successful strategy.
• Unfortunately, the emergence of resistance is inevitableand subsequent treatment is not well defined.
• Numerous mechanisms have been implicated in thedevelopment of resistance; central among them is theactivation of compensatory signaling pathways.
Nuevas vías de señalización en cáncer de mama
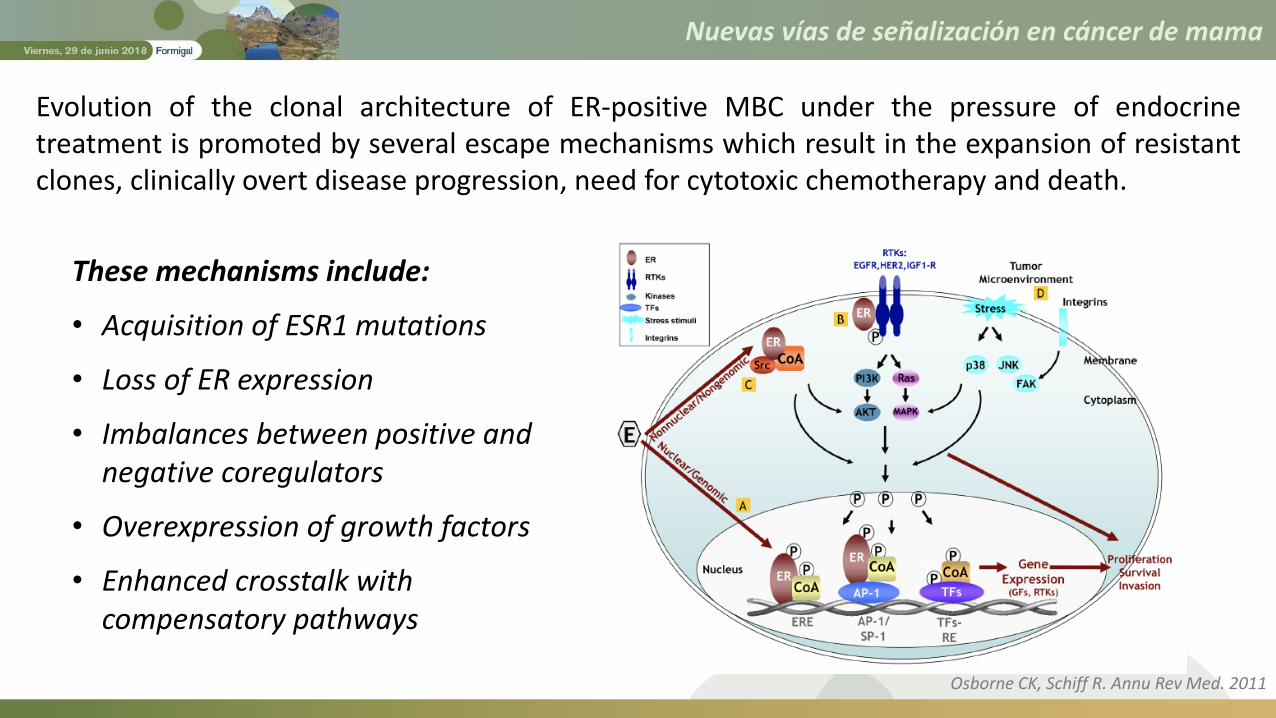
Evolution of the clonal architecture of ER-positive MBC under the pressure of endocrinetreatment is promoted by several escape mechanisms which result in the expansion of resistantclones, clinically overt disease progression, need for cytotoxic chemotherapy and death.
These mechanisms include:
• Acquisition of ESR1 mutations
• Loss of ER expression
• Imbalances between positive and negative coregulators
• Overexpression of growth factors
• Enhanced crosstalk withcompensatory pathways
Osborne CK, Schiff R. Annu Rev Med. 2011

Nuevas vías de señalización en cáncer de mama
Targetable genomic alterations under clinical investigation or withpotential clinical relevance in metastatic ER+HER2– breast cancers
Turner NC, et al. Lancet 2016

Nuevas vías de señalización en cáncer de mama
Key Pathways of Endocrine Resistance
ESR1 mutations
Nuevas vías de señalización en cáncer de mama
1. PI3K/Akt/mTOR Pathway
2. Inhibition of CDK4/6
3. PI3K/Akt/mTOR Pathway + Inhibition of CDK4/6
4. SERDs
5. HDAC Inhibitors
6. Immune Checkpoint Inhibition

Nuevas vías de señalización en cáncer de mama
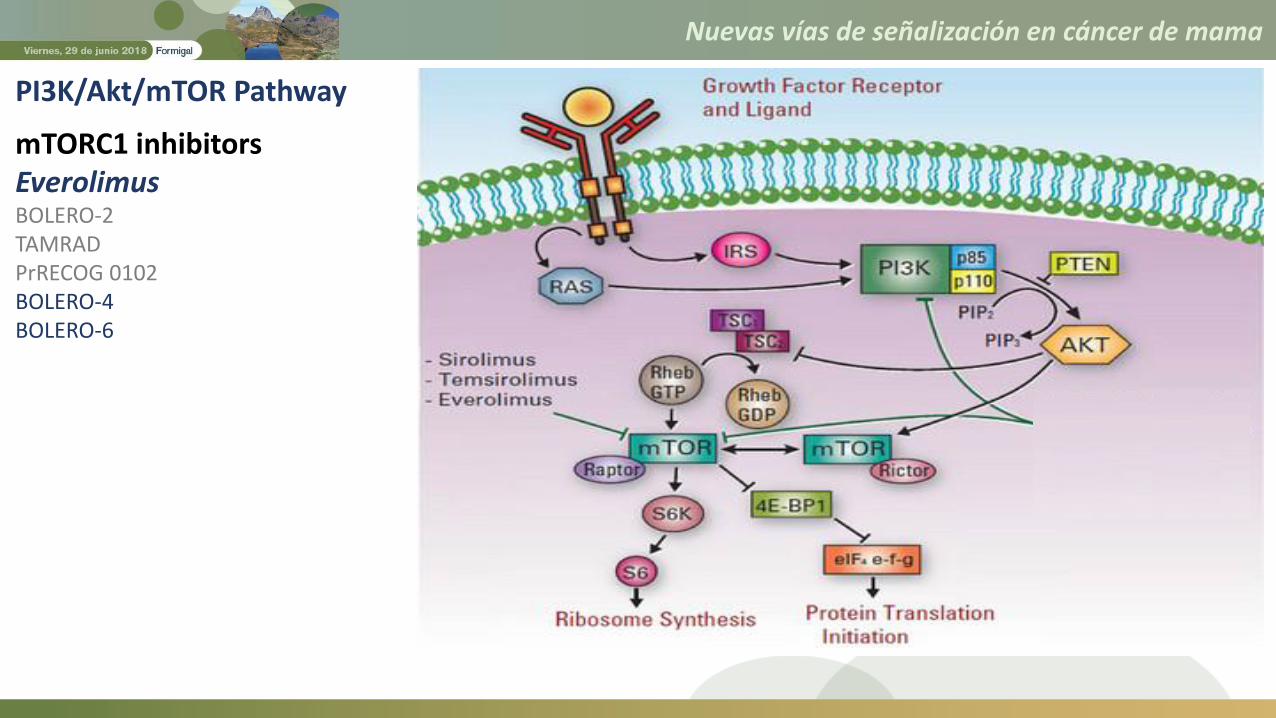
Most frequently mutated signalingpathway in breast carcinoma
PI3K activation is associated with bothde novo and also acquired endocrineresistance.
PI3K/Akt/mTOR Pathway
mTORC1 inhibitors Everolimus
Temsirolimus
Dual mTORC1/2 inhibitors AZD2014
TAK-228 (MLN0128)
Pan-PI3K inhibitors BKM120 (Buparlisib)
XL-147 (SAR245408)
PX-866
PKI-587 (Gedatolisib)
GDC-0941(Pictilisib)
PI3K inhibitors Wortmannin
LY294002
BYL719 (alpelisib)
GDC-0032 (Taselisib)
BAY 80-6946 (Copanlisib)
NK-1117
Dual PI3K/mTOR inhibitors BEZ235
BGT226
PF-4691502
GDC-0980
XL-765
AKT inhibitors MK2206
Nuevas vías de señalización en cáncer de mama
PI3K/Akt/mTOR Pathway
mTORC1 inhibitorsEverolimusBOLERO-2TAMRADPrRECOG 0102BOLERO-4BOLERO-6

Nuevas vías de señalización en cáncer de mama
PI3K/Akt/mTOR Pathway
mTORC1 inhibitorsEverolimusBOLERO-2TAMRADPrRECOG 0102BOLERO-4BOLERO-6
BOLERO-4: Phase 2 Trial of First-Line Everolimus Plus Letrozole in Estrogen
Receptor–Positive, Human Epidermal Growth Factor Receptor 2–Negative
Advanced Breast Cancer. (NCT01698918)
Royce M, et al. JAMA Oncol. 2018

Nuevas vías de señalización en cáncer de mama
PI3K/Akt/mTOR Pathway
mTORC1 inhibitorsEverolimusBOLERO-2TAMRADPrRECOG 0102BOLERO-4BOLERO-6
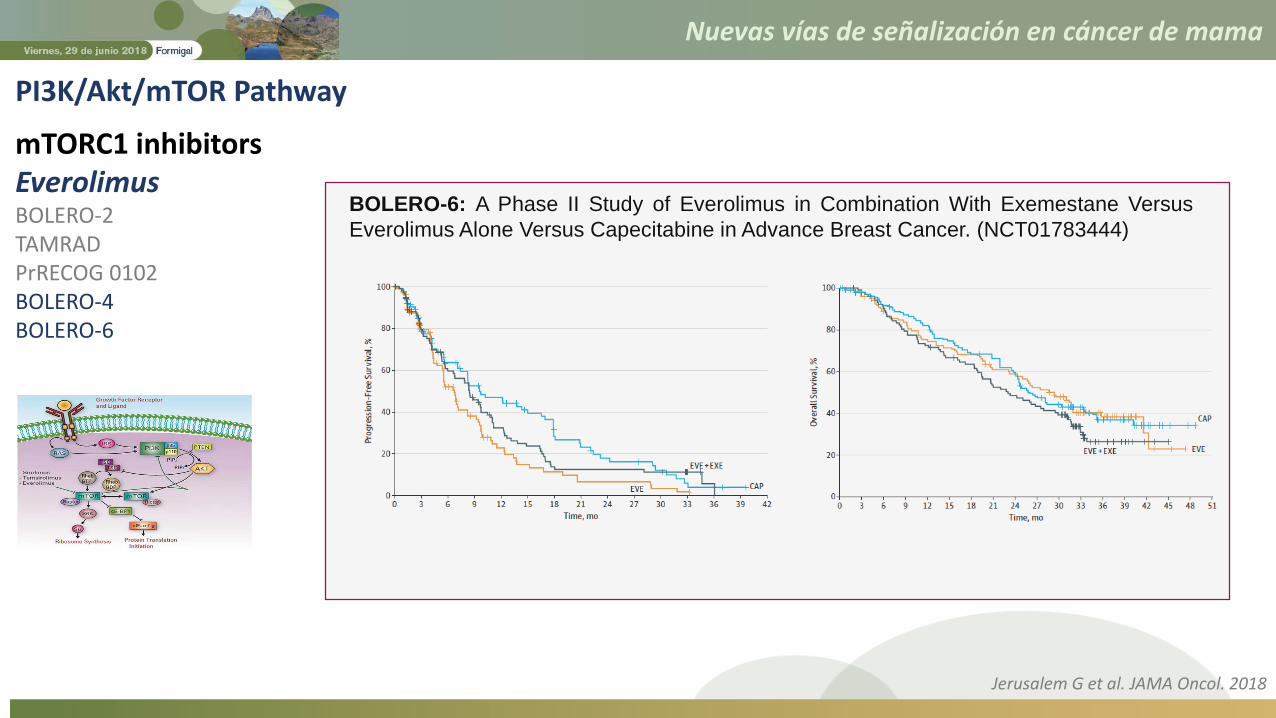
BOLERO-6: A Phase II Study of Everolimus in Combination With
Exemestane Versus Everolimus Alone Versus Capecitabine in Advance
Breast Cancer. (NCT01783444)
Nuevas vías de señalización en cáncer de mama
PI3K/Akt/mTOR Pathway
mTORC1 inhibitorsEverolimusBOLERO-2TAMRADPrRECOG 0102BOLERO-4BOLERO-6
BOLERO-6: A Phase II Study of Everolimus in Combination With Exemestane Versus
Everolimus Alone Versus Capecitabine in Advance Breast Cancer. (NCT01783444)
Jerusalem G et al. JAMA Oncol. 2018
Nuevas vías de señalización en cáncer de mama
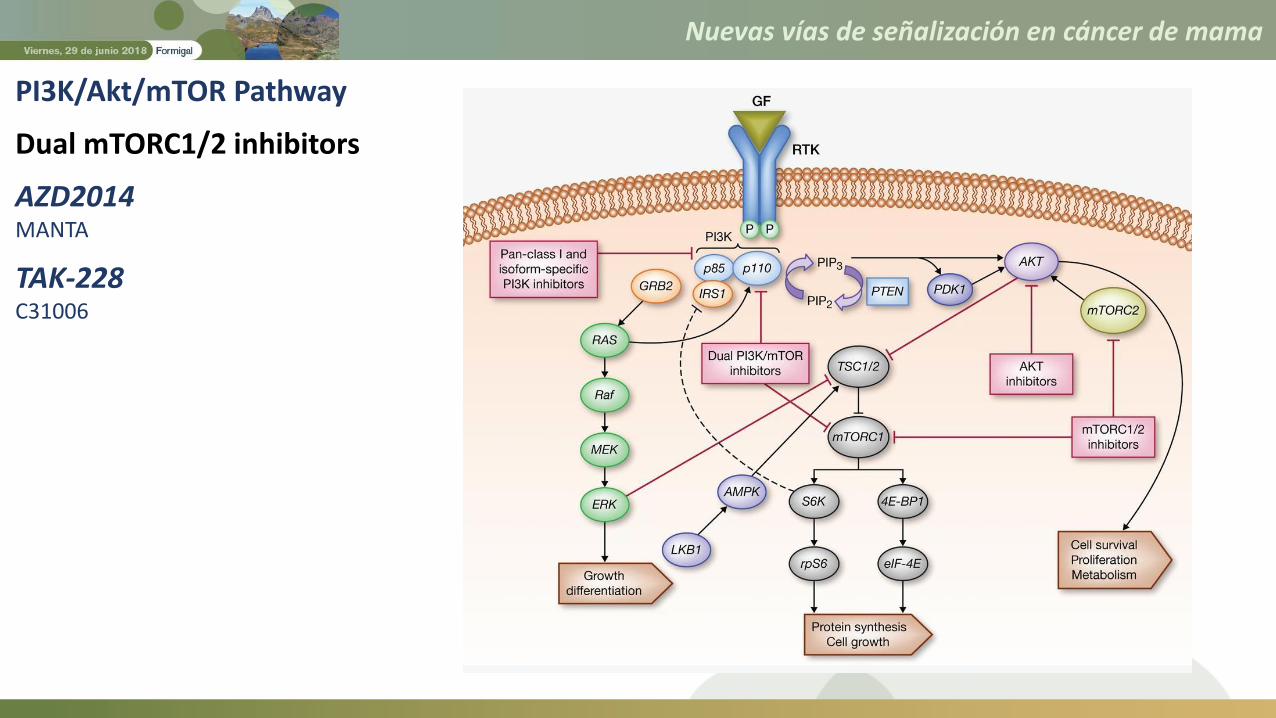
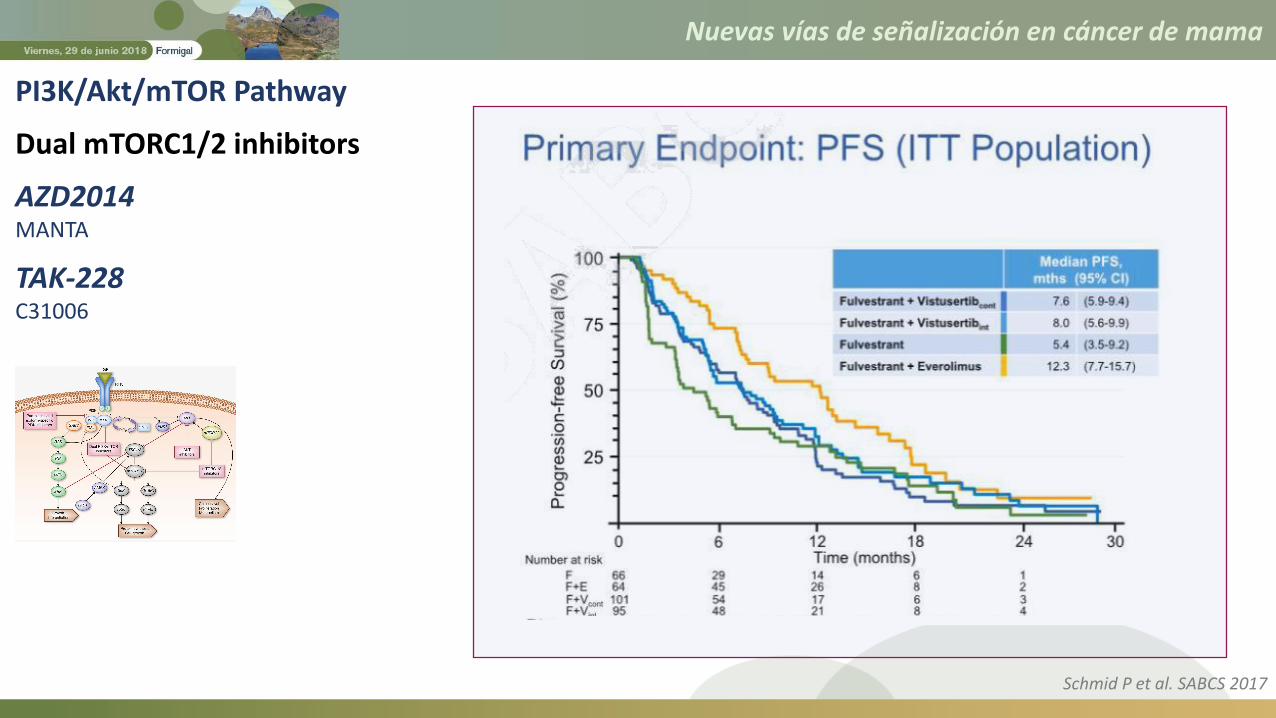
PI3K/Akt/mTOR Pathway
Dual mTORC1/2 inhibitors
AZD2014MANTA
TAK-228C31006

Nuevas vías de señalización en cáncer de mama
MANTA: A Randomized Study of AZD2014 in Combination With Fulvestrant in
Metastatic or Advanced Breast Cancer.
(NCT02216786)
Primary Outcome Measures:
• Progression free survival
PI3K/Akt/mTOR Pathway
Dual mTORC1/2 inhibitors
AZD2014MANTA
TAK-228C31006
Nuevas vías de señalización en cáncer de mama
PI3K/Akt/mTOR Pathway
Dual mTORC1/2 inhibitors
AZD2014MANTA
TAK-228C31006
Schmid P et al. SABCS 2017
Nuevas vías de señalización en cáncer de mama
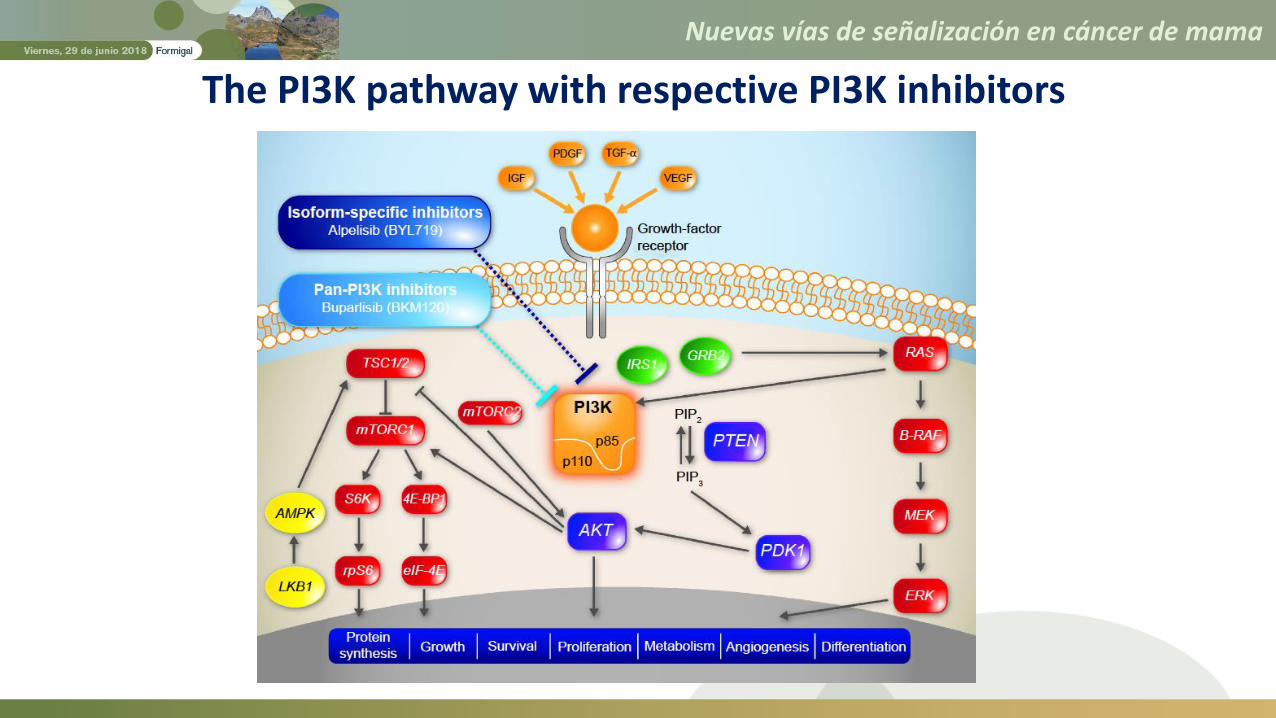
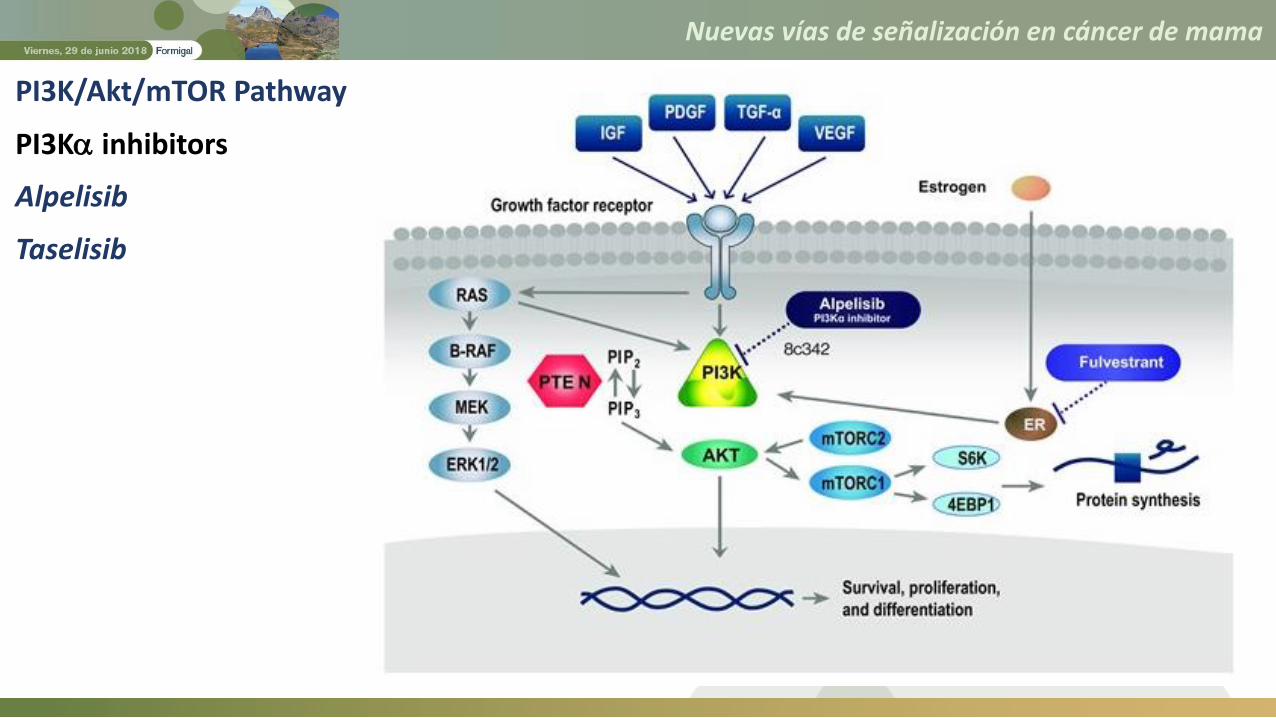
The PI3K pathway with respective PI3K inhibitors

Nuevas vías de señalización en cáncer de mama
Serious (grade 3 or higher) toxicity was reported in 77.3% receiving buparlisib and 61% of those receivingpictilisib in the BELLE-2 and FERGI trials, respectively.
The most commonly observed adverse events are elevated liver function enzymes, rash and hyperglycemia.Psychiatric disorders such as anxiety and depression have also been noted in patients receiving buparlisib.
PI3K/Akt/mTOR Pathway
Pan-PI3K inhibitors
BuparlisibBELLE 2BELLE 3
PictilisibFERGI
Baselga J, et al. Lancet Oncol. 2017; Di Leo A, et al. Lancet Oncol. 2018
Nuevas vías de señalización en cáncer de mama
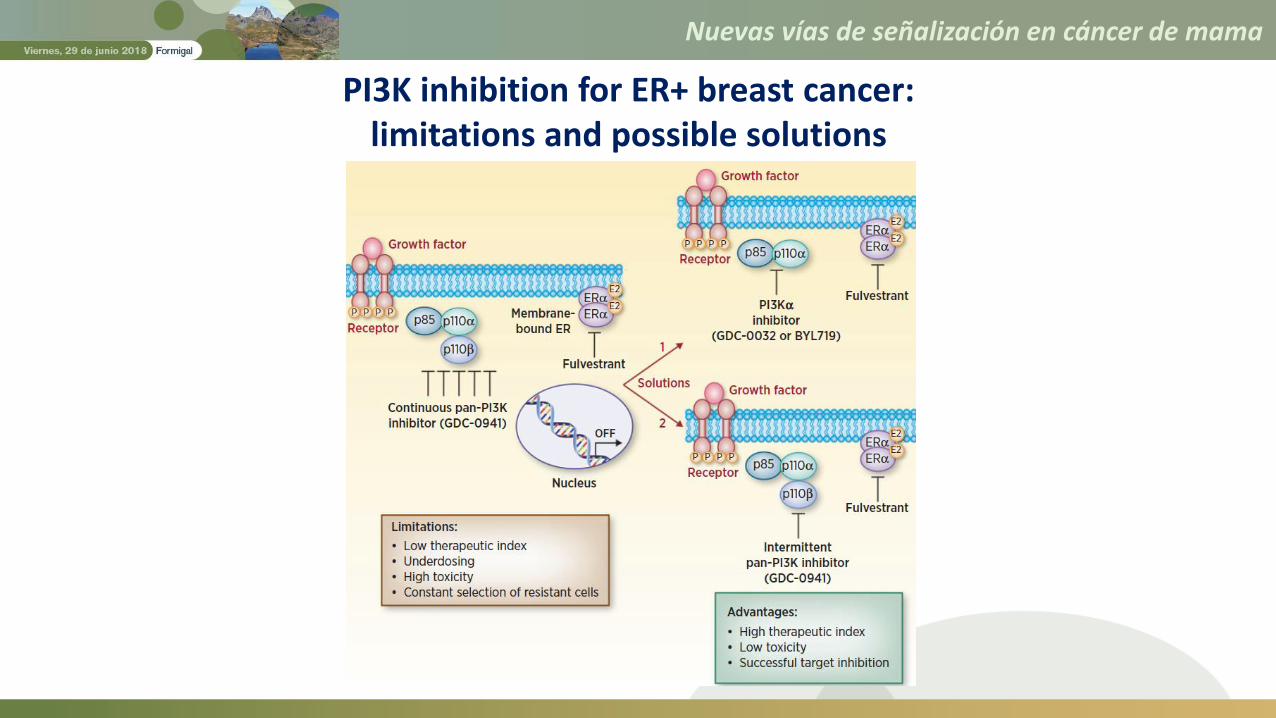
PI3K inhibition for ER+ breast cancer: limitations and possible solutions
Nuevas vías de señalización en cáncer de mama
PI3K/Akt/mTOR Pathway
PI3K inhibitors
Alpelisib
Taselisib

Nuevas vías de señalización en cáncer de mama
SOLAR-1: Study Assessing the Efficacy and Safety of Alpelisib Plus Fulvestrant
in Men and Postmenopausal Women With Advanced Breast Cancer Which
Progressed on or After Aromatase Inhibitor Treatment. (NCT02437318)
PI3K/Akt/mTOR Pathway
PI3K inhibitors
AlpelisibPIKNICSOLAR-1BYLieve
TaselisibLORELEIPOSEIDONSANDPIPER
Nuevas vías de señalización en cáncer de mama
PI3K/Akt/mTOR Pathway
PI3K inhibitors
AlpelisibPIKNICSOLAR-1BYLieve
TaselisibLORELEIPOSEIDONSANDPIPER
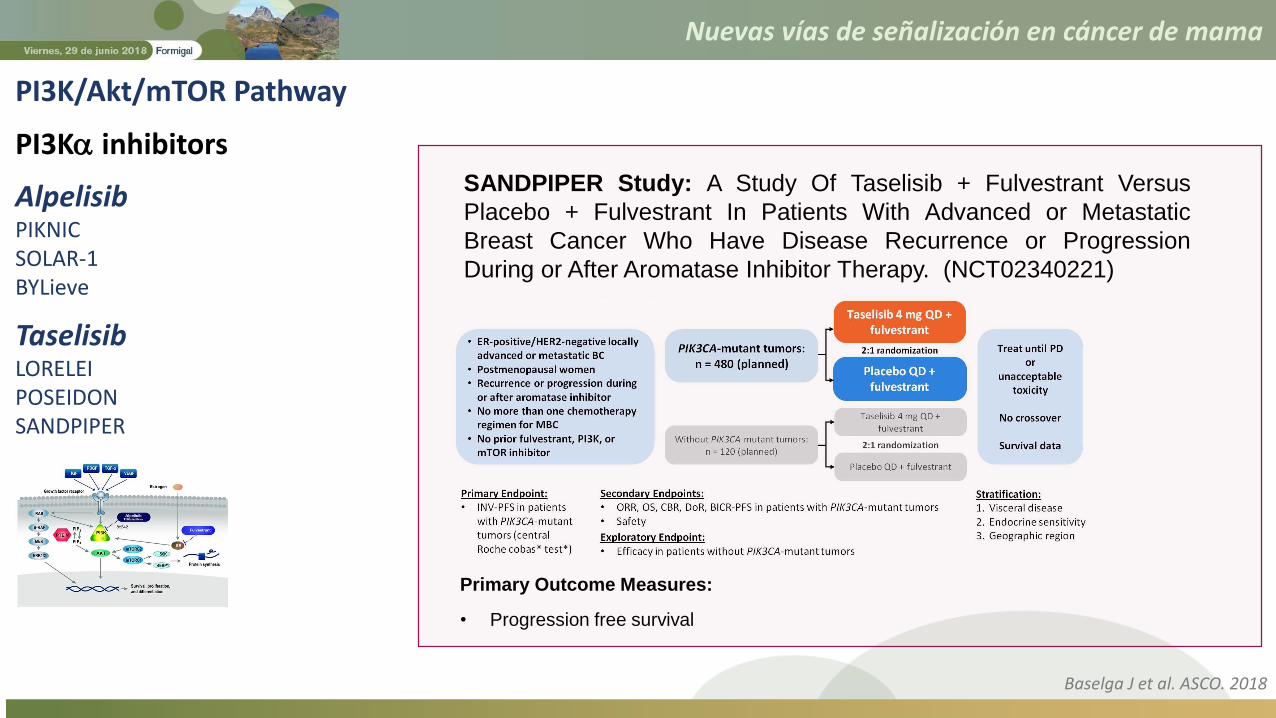
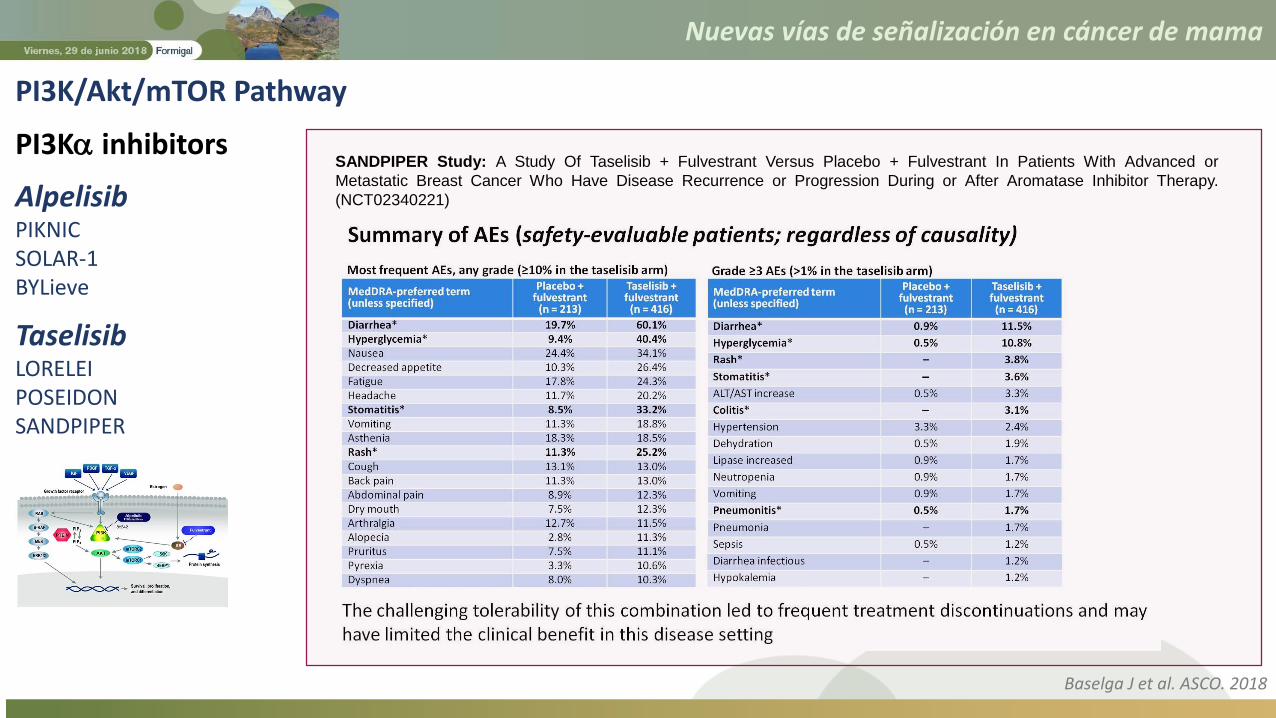
SANDPIPER Study: A Study Of Taselisib + Fulvestrant Versus
Placebo + Fulvestrant In Patients With Advanced or Metastatic
Breast Cancer Who Have Disease Recurrence or Progression
During or After Aromatase Inhibitor Therapy. (NCT02340221)
Primary Outcome Measures:
• Progression free survival
Baselga J et al. ASCO. 2018
Nuevas vías de señalización en cáncer de mama
PI3K/Akt/mTOR Pathway
PI3K inhibitors
AlpelisibPIKNICSOLAR-1BYLieve
TaselisibLORELEIPOSEIDONSANDPIPER
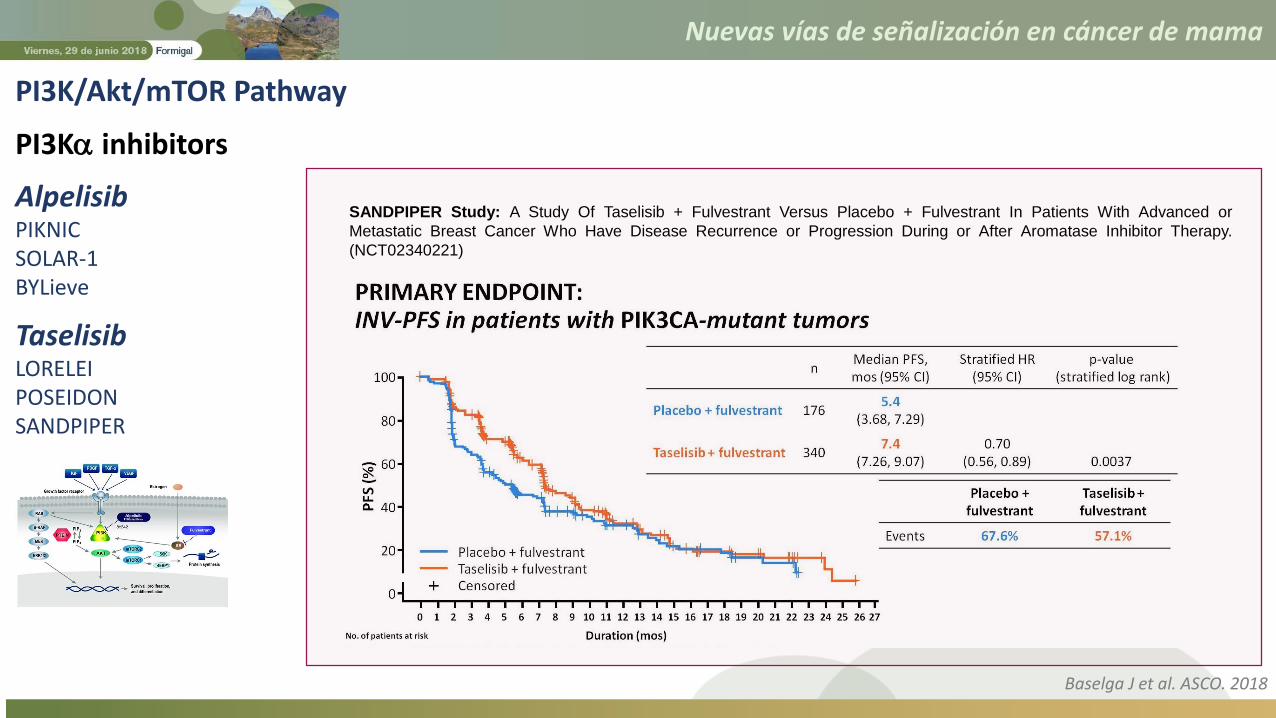
SANDPIPER Study: A Study Of Taselisib + Fulvestrant Versus Placebo + Fulvestrant In Patients With Advanced or
Metastatic Breast Cancer Who Have Disease Recurrence or Progression During or After Aromatase Inhibitor Therapy.
(NCT02340221)
Baselga J et al. ASCO. 2018
Nuevas vías de señalización en cáncer de mama
PI3K/Akt/mTOR Pathway
PI3K inhibitors
AlpelisibPIKNICSOLAR-1BYLieve
TaselisibLORELEIPOSEIDONSANDPIPER
SANDPIPER Study: A Study Of Taselisib + Fulvestrant Versus Placebo + Fulvestrant In Patients With Advanced or
Metastatic Breast Cancer Who Have Disease Recurrence or Progression During or After Aromatase Inhibitor Therapy.
(NCT02340221)
Baselga J et al. ASCO. 2018

Nuevas vías de señalización en cáncer de mama
Nuevas vías de señalización en cáncer de mama
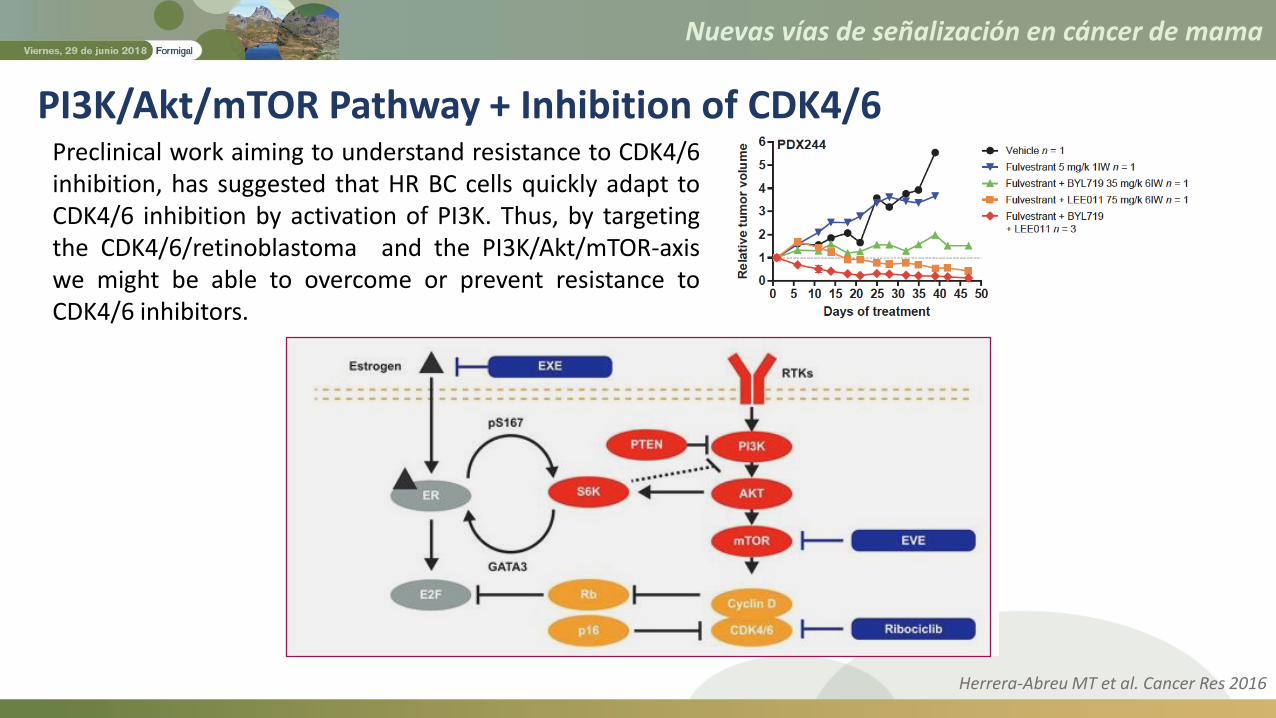
PI3K/Akt/mTOR Pathway + Inhibition of CDK4/6Preclinical work aiming to understand resistance to CDK4/6inhibition, has suggested that HR BC cells quickly adapt toCDK4/6 inhibition by activation of PI3K. Thus, by targetingthe CDK4/6/retinoblastoma and the PI3K/Akt/mTOR-axiswe might be able to overcome or prevent resistance toCDK4/6 inhibitors.
Herrera-Abreu MT et al. Cancer Res 2016

Nuevas vías de señalización en cáncer de mama
Available efficacy and safety data from triplet therapy clinical studies in patients with HR+, HER2 advanced breast cancer.
PI3K/Akt/mTOR Pathway + Inhibition of CDK4/6
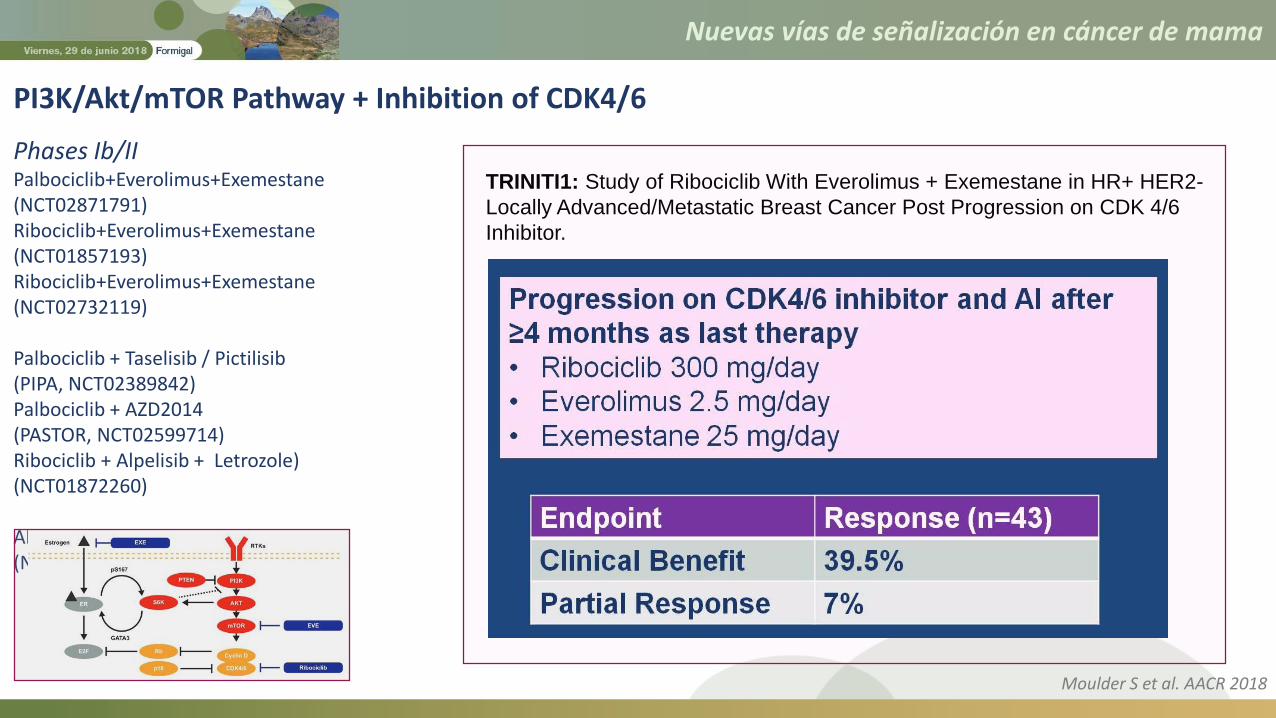
Phases Ib/II Palbociclib+Everolimus+Exemestane(NCT02871791)Ribociclib+Everolimus+Exemestane(NCT01857193)Ribociclib+Everolimus+Exemestane(NCT02732119)
Palbociclib + Taselisib / Pictilisib(PIPA, NCT02389842)Palbociclib + AZD2014(PASTOR, NCT02599714)Ribociclib + Alpelisib + Letrozole)(NCT01872260)
Abemaciclib+Everolimus+Exemestane(NCT02057133)
• Early trials combining CDK4/6 inhibitors, PI3K or mTOR inhibitors, andendocrine therapy have shown encouraging signs of clinical activity.
• However, further research is needed to help understand the extent oftreatment benefit from triplet therapy and where this strategy will fit inthe treatment sequence for patients with HR+ breast cancer.
Cortes J. et al. Cancer Treat Rev 2017

Nuevas vías de señalización en cáncer de mama
PI3K/Akt/mTOR Pathway + Inhibition of CDK4/6
Phases Ib/II Palbociclib+Everolimus+Exemestane(NCT02871791)Ribociclib+Everolimus+Exemestane(NCT01857193)Ribociclib+Everolimus+Exemestane(NCT02732119)
Palbociclib + Taselisib / Pictilisib(PIPA, NCT02389842)Palbociclib + AZD2014(PASTOR, NCT02599714)Ribociclib + Alpelisib + Letrozole)(NCT01872260)
Abemaciclib+Everolimus+Exemestane(NCT02057133)
TRINITI1: Study of Ribociclib With Everolimus + Exemestane in HR+ HER2-
Locally Advanced/Metastatic Breast Cancer Post Progression on CDK 4/6
Inhibitor.
Primary Outcome Measures:
• Phase I: Maximum Tolerated Dose (MTD) and/or the Recommended Phase II
Dose for the triplet combination.
• Phase II: Clinical Benefit Rate (CBR) among subjects receiving triplet therapy
Nuevas vías de señalización en cáncer de mama
PI3K/Akt/mTOR Pathway + Inhibition of CDK4/6
Phases Ib/II Palbociclib+Everolimus+Exemestane(NCT02871791)Ribociclib+Everolimus+Exemestane(NCT01857193)Ribociclib+Everolimus+Exemestane(NCT02732119)
Palbociclib + Taselisib / Pictilisib(PIPA, NCT02389842)Palbociclib + AZD2014(PASTOR, NCT02599714)Ribociclib + Alpelisib + Letrozole)(NCT01872260)
Abemaciclib+Everolimus+Exemestane(NCT02057133)
TRINITI1: Study of Ribociclib With Everolimus + Exemestane in HR+ HER2-
Locally Advanced/Metastatic Breast Cancer Post Progression on CDK 4/6
Inhibitor.
Moulder S et al. AACR 2018

Nuevas vías de señalización en cáncer de mama
Selective ER Downregulators (SERDs) are competitive ER⍺ antagonists that alsoinduce a conformational shift of the receptor that results in ubiquitination andsubsequent degradation of ER⍺, via the ubiquitin-proteasome system.
SERDs
• A mechanism of resistance that hasbeen recently suggested is thedevelopment of ESR1 mutations.
• Early BC samples showed a lowpresence of ESR1 mutations in 0.5%and of ESR1 amplification in 2.5% ofthe cases. In contrast, ESR1mutations have been reported in20-50% of recurrent or MBC after ETwith AIs.

Nuevas vías de señalización en cáncer de mama
Theoretically, a strategy of completely or nearly completelydestroying the ER, may lead to a more effective inhibition of highlyER-dependent tumors.
The recognition that ERα remains a viable target even in the settingof endocrine resistance and the limitations of fulvestrant led to thesearch for a new generation of orally bioavailable highly selectiveSERDs.
In particular, ER degraders may have a particular advantage in tumorswith ESR1 mutations, which may emerge after estrogen deprivationstrategies, but could potentially be less of a problem as a mechanismof resistance if ER is degraded.
SERDs

Nuevas vías de señalización en cáncer de mama
SERDs Antitumor activity of GDC-0810 in a tamoxifen-resistant breast cancer xenograft model.
Joseph JD et al. Elife 2016
Nuevas vías de señalización en cáncer de mama
SERDs
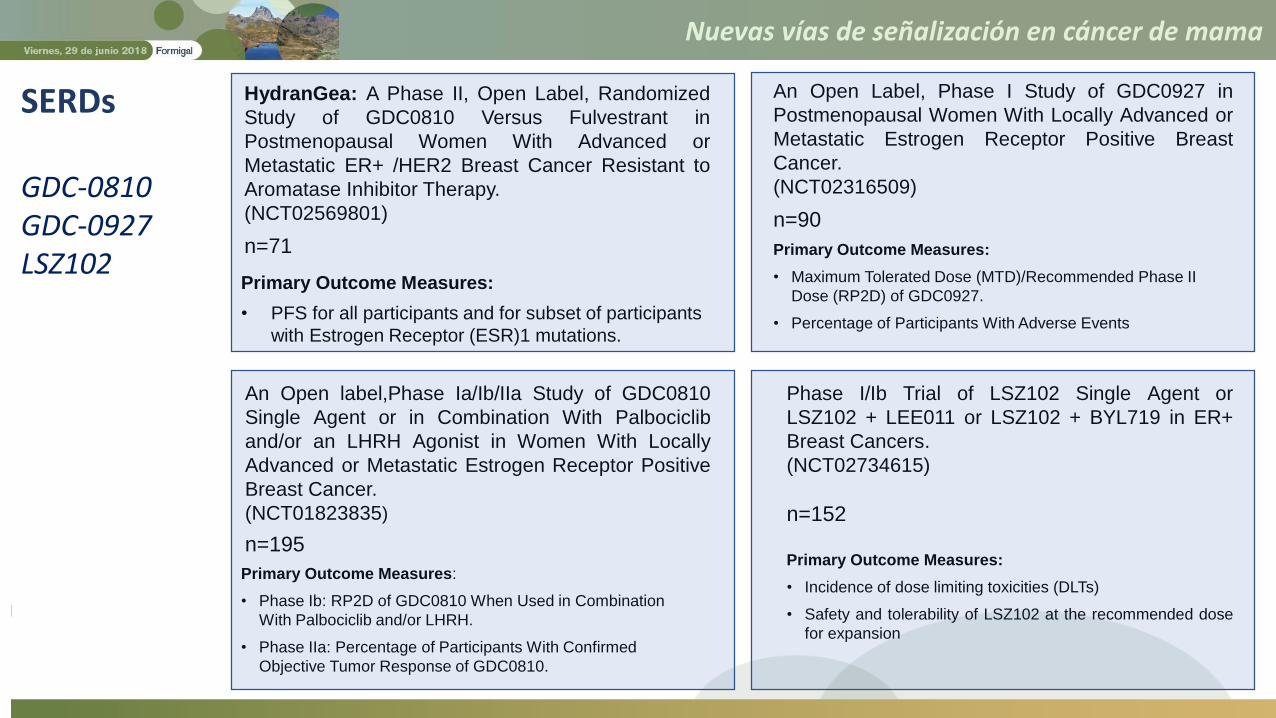
GDC-0810GDC-0927LSZ102
HydranGea: A Phase II, Open Label, Randomized
Study of GDC0810 Versus Fulvestrant in
Postmenopausal Women With Advanced or
Metastatic ER+ /HER2 Breast Cancer Resistant to
Aromatase Inhibitor Therapy.
(NCT02569801)
n=71
Primary Outcome Measures:
• PFS for all participants and for subset of participants
with Estrogen Receptor (ESR)1 mutations.
An Open label,Phase Ia/Ib/IIa Study of GDC0810
Single Agent or in Combination With Palbociclib
and/or an LHRH Agonist in Women With Locally
Advanced or Metastatic Estrogen Receptor Positive
Breast Cancer.
(NCT01823835)
n=195
Primary Outcome Measures:
• Phase Ib: RP2D of GDC0810 When Used in Combination
With Palbociclib and/or LHRH.
• Phase IIa: Percentage of Participants With Confirmed
Objective Tumor Response of GDC0810.
An Open Label, Phase I Study of GDC0927 in
Postmenopausal Women With Locally Advanced or
Metastatic Estrogen Receptor Positive Breast
Cancer.
(NCT02316509)
n=90
Primary Outcome Measures:
• Maximum Tolerated Dose (MTD)/Recommended Phase II
Dose (RP2D) of GDC0927.
• Percentage of Participants With Adverse Events
Phase I/Ib Trial of LSZ102 Single Agent or
LSZ102 + LEE011 or LSZ102 + BYL719 in ER+
Breast Cancers.
(NCT02734615)
n=152
Primary Outcome Measures:
• Incidence of dose limiting toxicities (DLTs)
• Safety and tolerability of LSZ102 at the recommended dose
for expansion
Nuevas vías de señalización en cáncer de mama
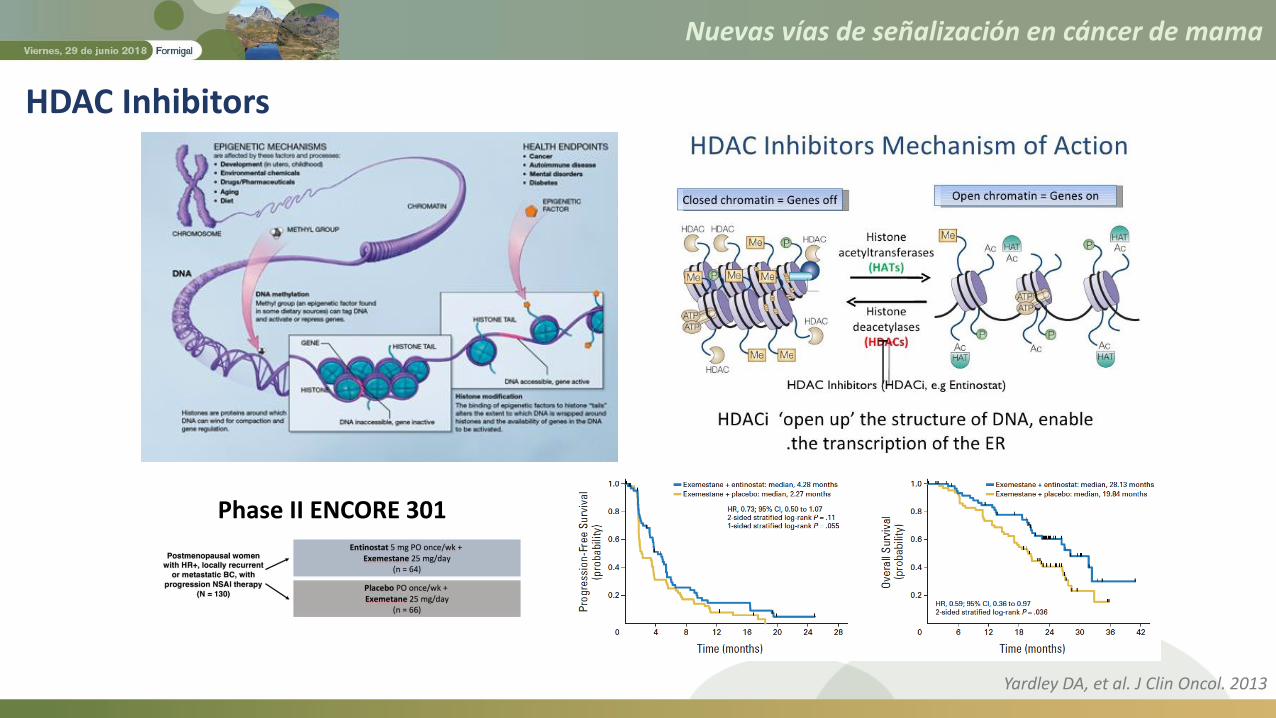
HDAC Inhibitors
Phase II ENCORE 301
Yardley DA, et al. J Clin Oncol. 2013
Nuevas vías de señalización en cáncer de mama
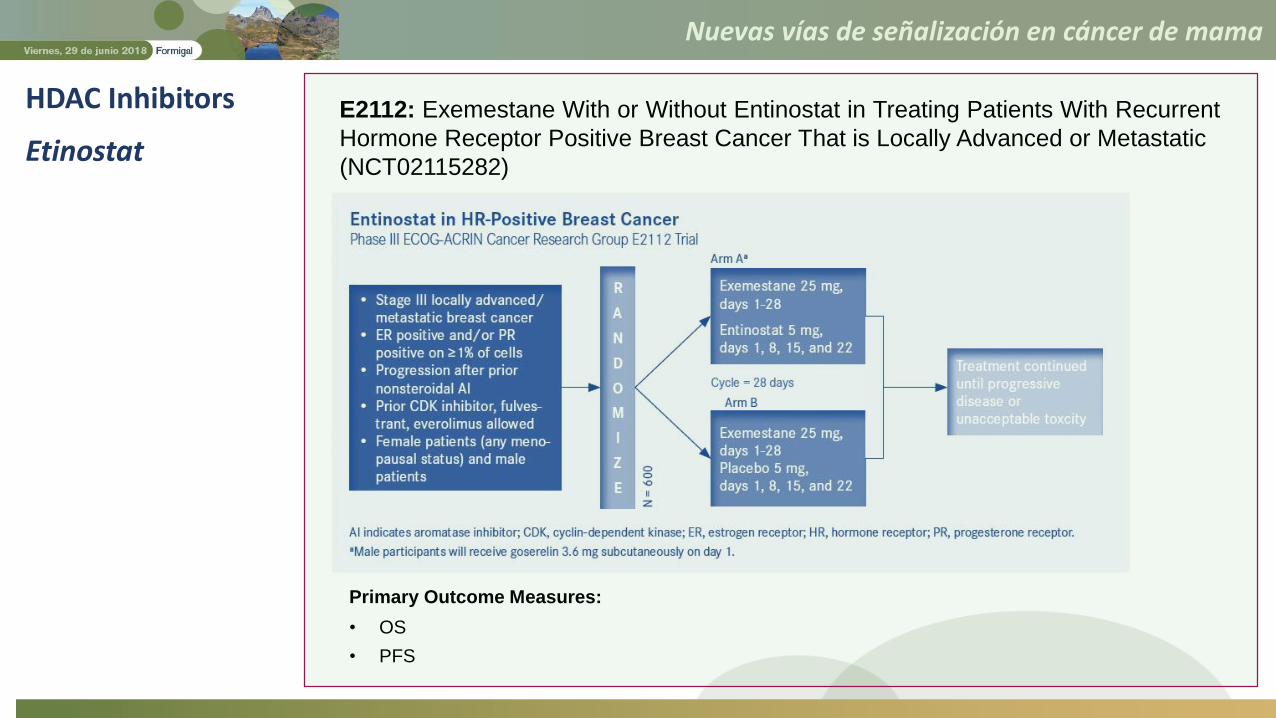
HDAC Inhibitors
Etinostat
E2112: Exemestane With or Without Entinostat in Treating Patients With Recurrent
Hormone Receptor Positive Breast Cancer That is Locally Advanced or Metastatic
(NCT02115282)
Primary Outcome Measures:
• OS
• PFS
Nuevas vías de señalización en cáncer de mama
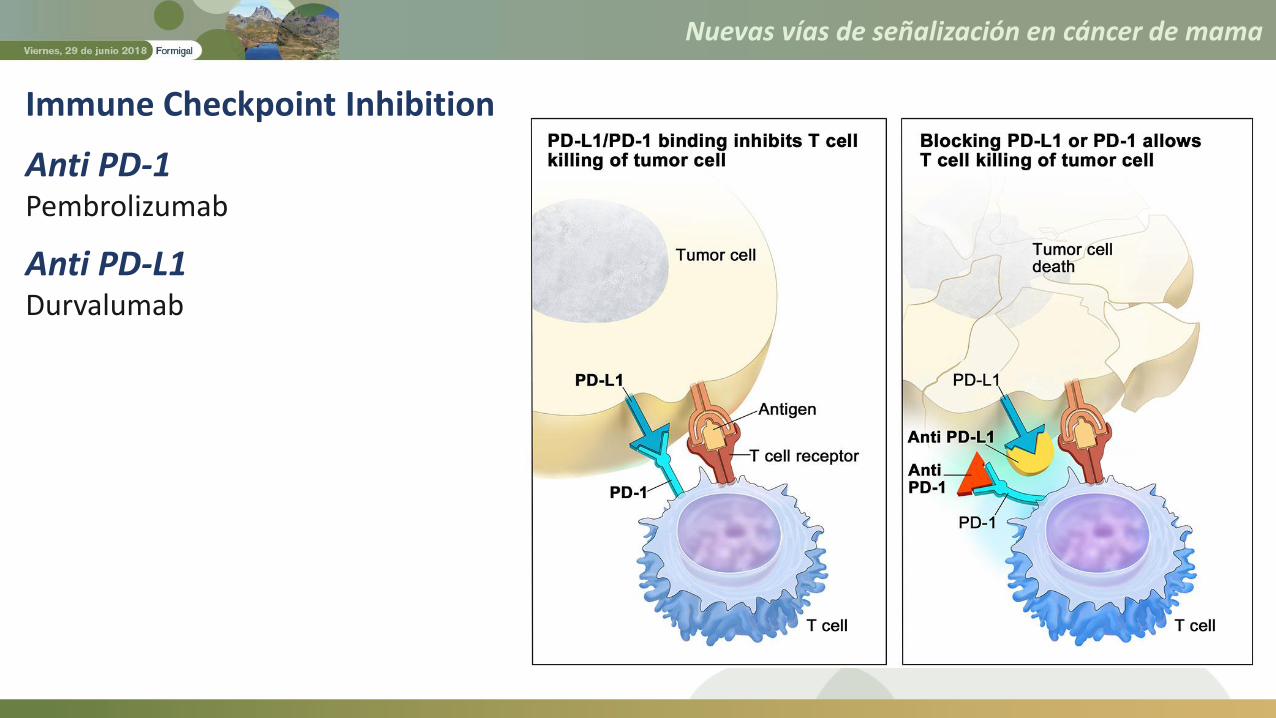
Immune Checkpoint Inhibition
Anti PD-1Pembrolizumab
Anti PD-L1Durvalumab

Nuevas vías de señalización en cáncer de mama
Goel X et al. Nature 2017; Deng X et al. Cancer Discovery 2017
Nuevas vías de señalización en cáncer de mama
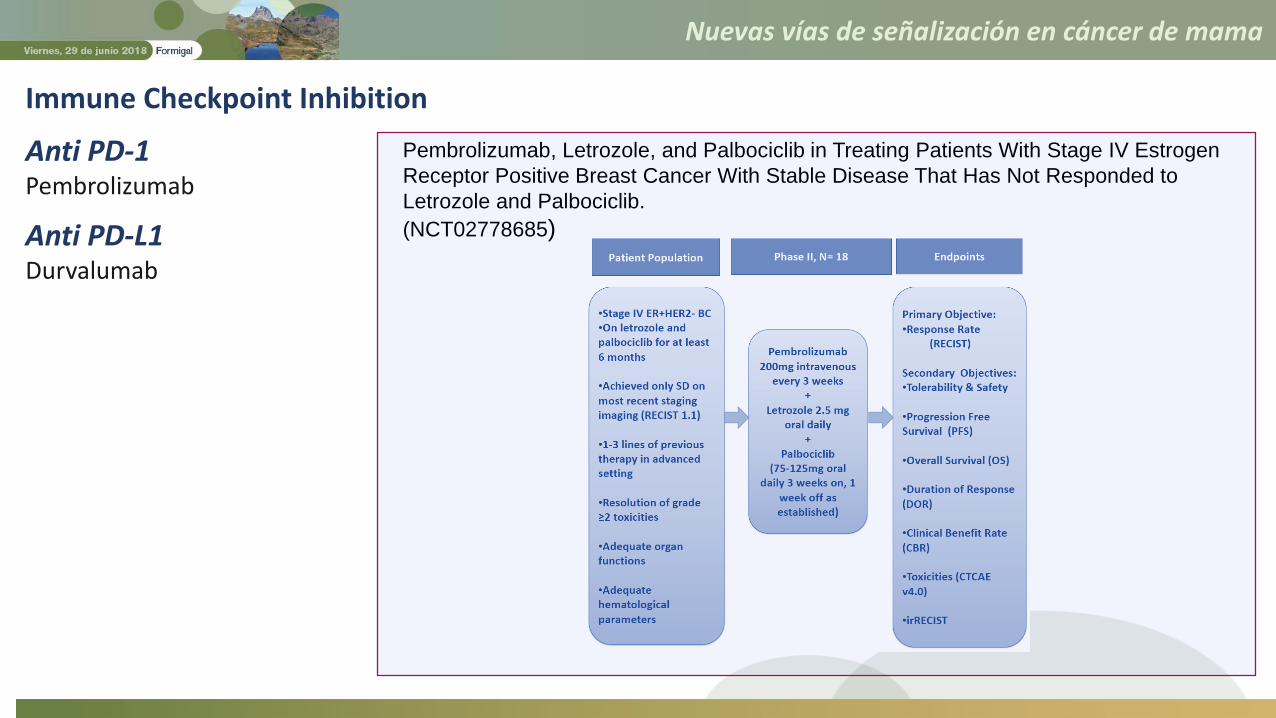
Pembrolizumab, Letrozole, and Palbociclib in Treating Patients With Stage IV Estrogen
Receptor Positive Breast Cancer With Stable Disease That Has Not Responded to
Letrozole and Palbociclib.
(NCT02778685)
Immune Checkpoint Inhibition
Anti PD-1Pembrolizumab
Anti PD-L1Durvalumab
Nuevas vías de señalización en cáncer de mama
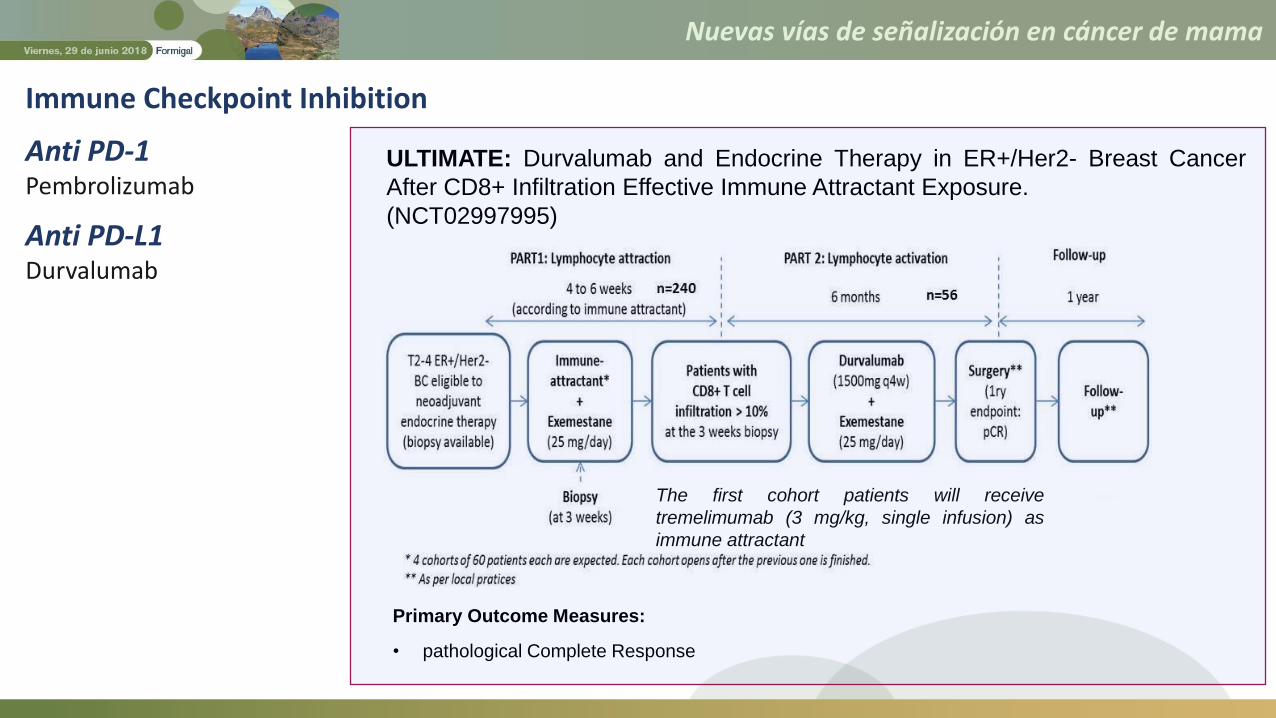
ULTIMATE: Durvalumab and Endocrine Therapy in ER+/Her2- Breast Cancer
After CD8+ Infiltration Effective Immune Attractant Exposure.
(NCT02997995)
Primary Outcome Measures:
• pathological Complete Response
The first cohort patients will receive
tremelimumab (3 mg/kg, single infusion) as
immune attractant
Immune Checkpoint Inhibition
Anti PD-1Pembrolizumab
Anti PD-L1Durvalumab

Nuevas vías de señalización en cáncer de mama
• Endocrine resistance in patients with HR-positive breast carcinoma continues to represent anoncological challenge.
• Efforts at elucidating the molecular mechanisms of endocrine resistance have revealed anumber of targets that act downstream or upstream the ER or that crosstalk with it.
• Alterations in the PI3K signaling pathway are among the most frequent somatic mutations inER-positive breast carcinomas, which are associated with endocrine resistance. NumerousPI3K inhibitors are currently undergoing preclinical and clinical development.
• Notable successes include agents targeting mTOR and CDK4/6 in combination with endocrinetherapy, whereas failures include the disappointing performance of pan-PI3K inhibition.PI3K⍺ inhibitors ??.
• Similarly, efforts to develop next-generation SERDs combining improved oral bioavaliabilitywith enhanced ER targeting, HDAC Inhibitors and Immune Checkpoint Inhibition, appearspromising.
Take home messages (1)
Nuevas vías de señalización en cáncer de mama
• We need to better identify which patients are most likely to derive themost benefit from combination therapy, and design efficient clinicaltrials that take into account ER-positive disease biology and timing ofadditional intervention to modulate endocrine response.
• Defining populations with a specific alteration in a given signallingpathway could improve the likelihood of benefit from a targeted agent,limit unnecessary exposure to toxicity and allow the sustainability ofthese newer treatments.
Take home messages (2)
Nuevas vías de señalización en cáncer de mama
Nuevas vías de señalización en cáncer de mama