preparation for transplantation dr ahmed kamal
TRANSCRIPT
PREPARATION FOR KIDNEY TRANSPLANTATION
Ahmed I. Kamal, MD, FISN
Mansoura Urology and Nephrology Center
Mansoura University
Rational for living donation
• Better out come
• Shorter waiting time
• Elective planning and optimization of the recipient health status
• Realistic chance for pre-emptive kidney transplantation
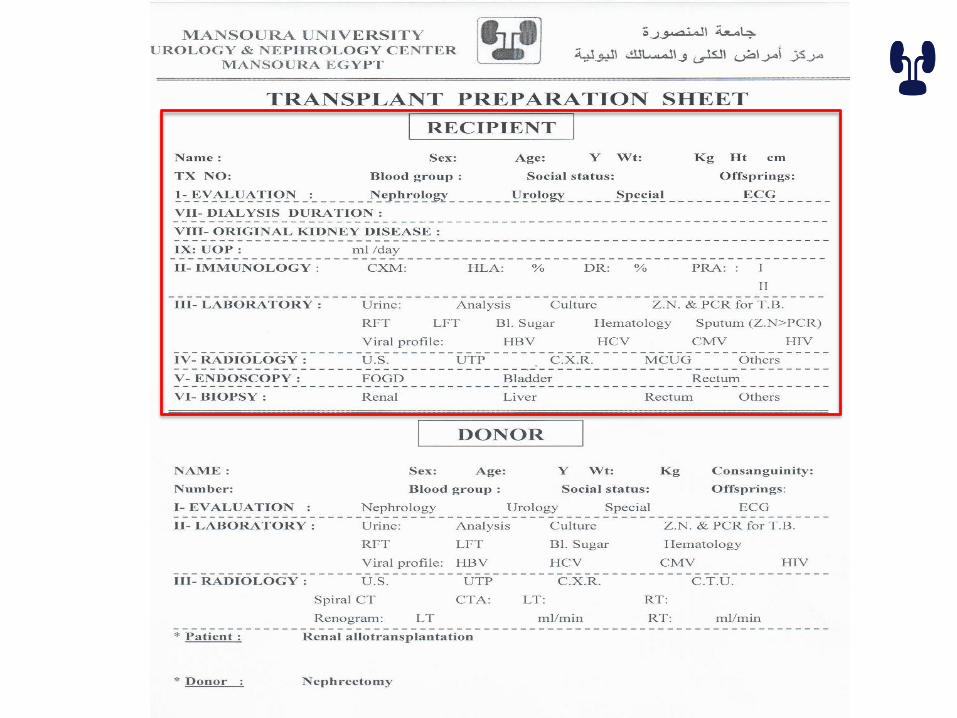
Preparation

Donor evaluation process
• Education, counseling and consenting
• Psychological evaluation
• Medical screening process
• Identification of transmissible infections
• Evaluation of renal anatomy

Education, counseling and consenting
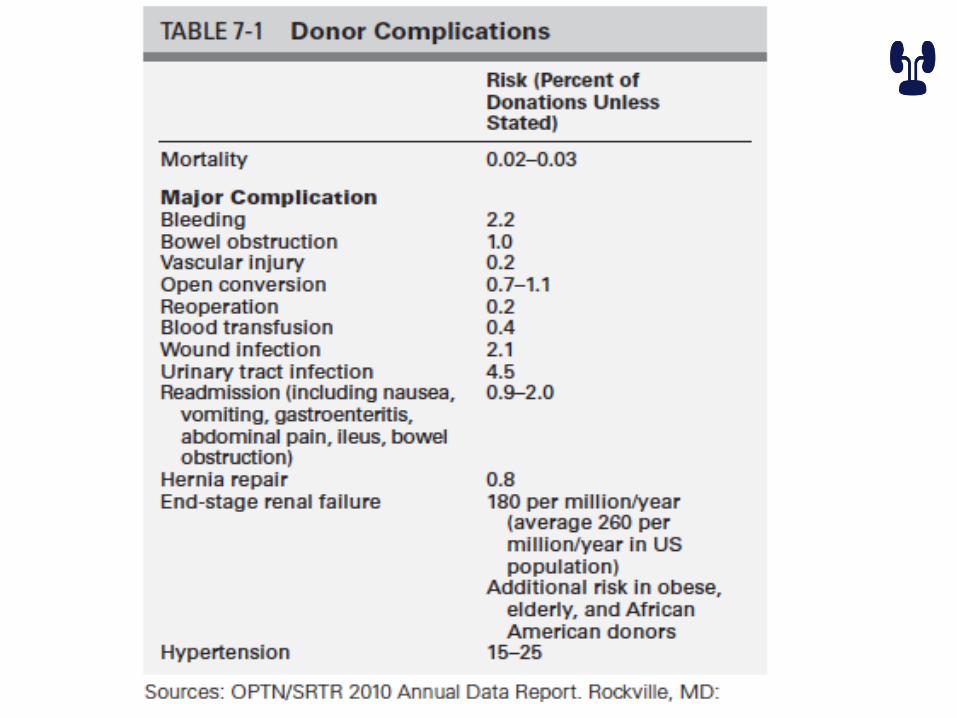
• Complications
• Blood grouping and HLA
• Medical evaluation steps
• Stress of the right to withdraw at any time
• Follow up
• Informed consent
Erratum in: Am J Transplant. 2015 May;15(5):1447

Psychological evaluation
• Psychiatrist, psychologist or social worker
• For :
– Psychological evaluation and identification of active mental health problems
– Social assessment including high risk behavior
– Assessment of consenting ability
Medical screening process
• History of physical examination
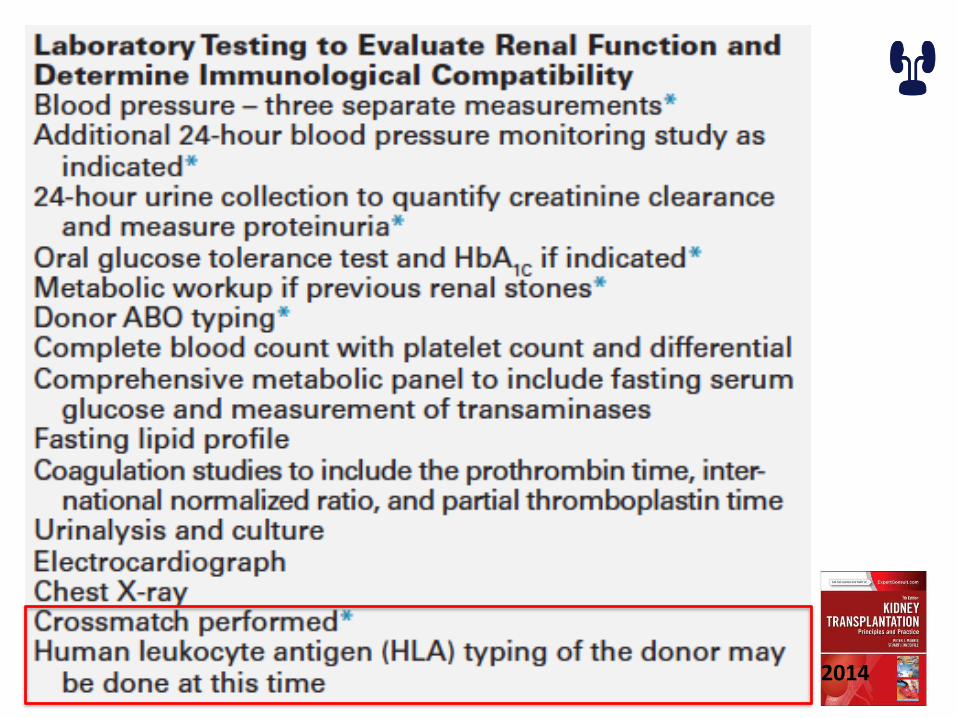
• Laboratory testing
• Identification of transmissible infection
• Evaluating renal anatomy and function
2014

COUPLE EVALUATION
• Education, counseling and consenting• Detailed history • Medical evaluation• Identification of active infections• Evaluation of urinary tract• Hematological and full chemistry • Virology screening • Microbiology
– Urine culture – TB ZN and PCR
2014
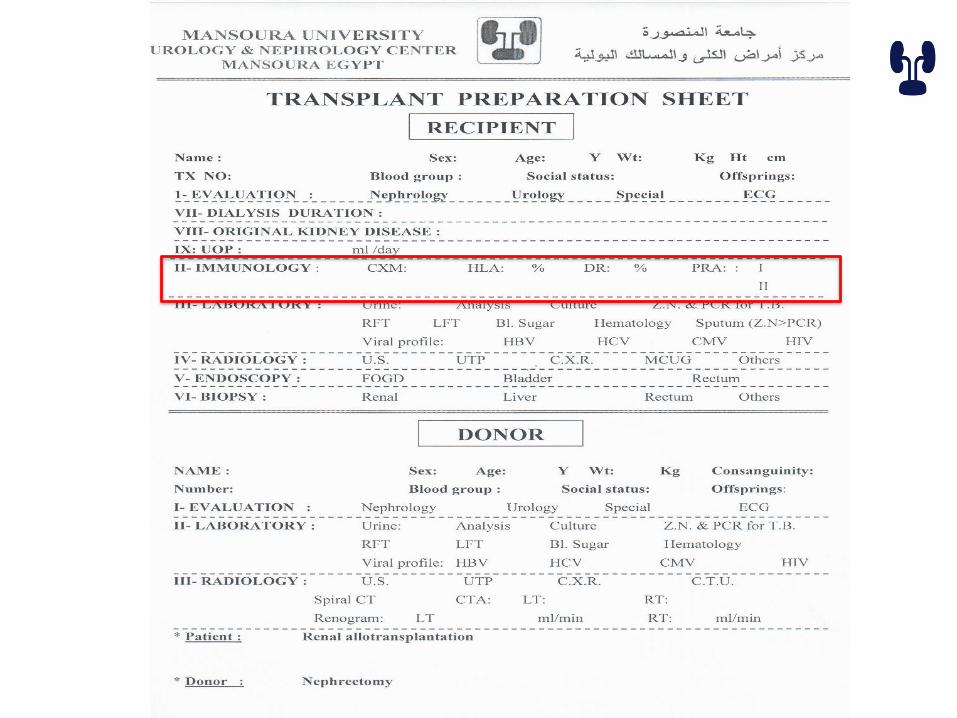
Immunological work up
• Cross Match
• HLA genotyping
• (PRA) panel reactive antibodies


Role of the NIH Standard Crossmatch in Kidney Transplant Outcomes
Graft SurvivalRecipients with Anti-HLA Antibodies Recipients
without Anti-HLA
AntibodiesPositive
CrossmatchNo
CrossmatchNegative
Crossmatch
ImmediateFailure
24 (80%) 6 (26%) 4 (15%) 4 (2.4%)
Failure < 3months
0 6 4 32
Failure > 3months
1 3 7 22
Survival < 3months
2 2 1 6
Survival > 3months
3 (10%) 6 (26%) 11 (41%) 104 (62%)
Total Patients 30 23 27 168
80
Patel and Terasaki, NEJM 280:735, 1969
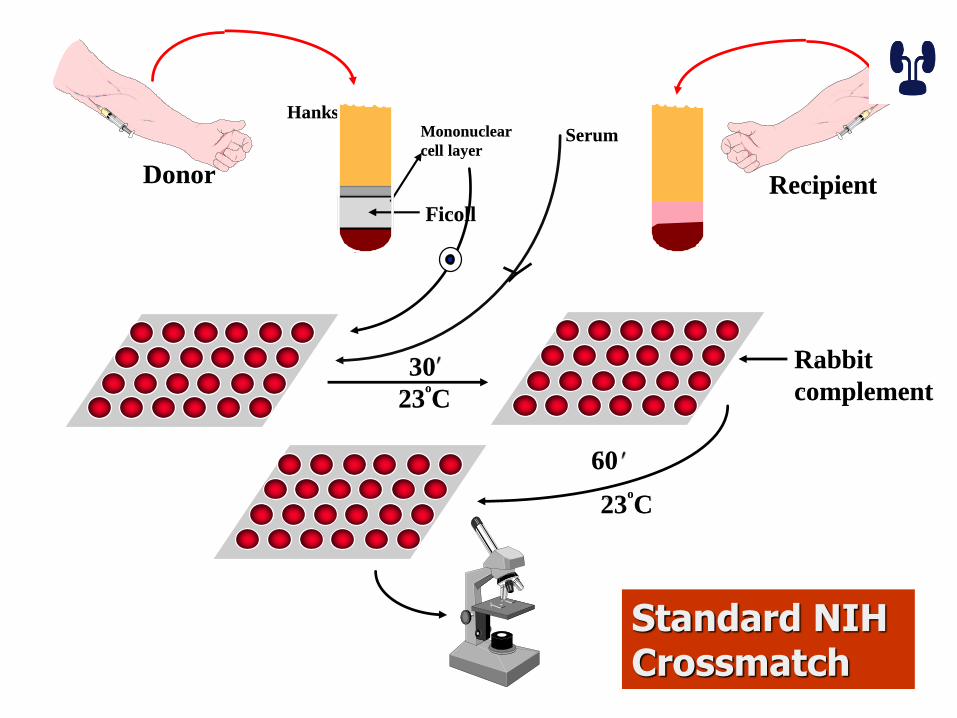
Donor
HanksMononuclear
cell layer
Ficoll
Recipient
Serum
23o
C
30
23o
C
60
Standard NIH Crossmatch
Rabbit
complement
Antiglobulin-Enhanced Technique
• More sensitive
• Can detect non-complement binding antibodies
• Can detect antibodies present in small amounts
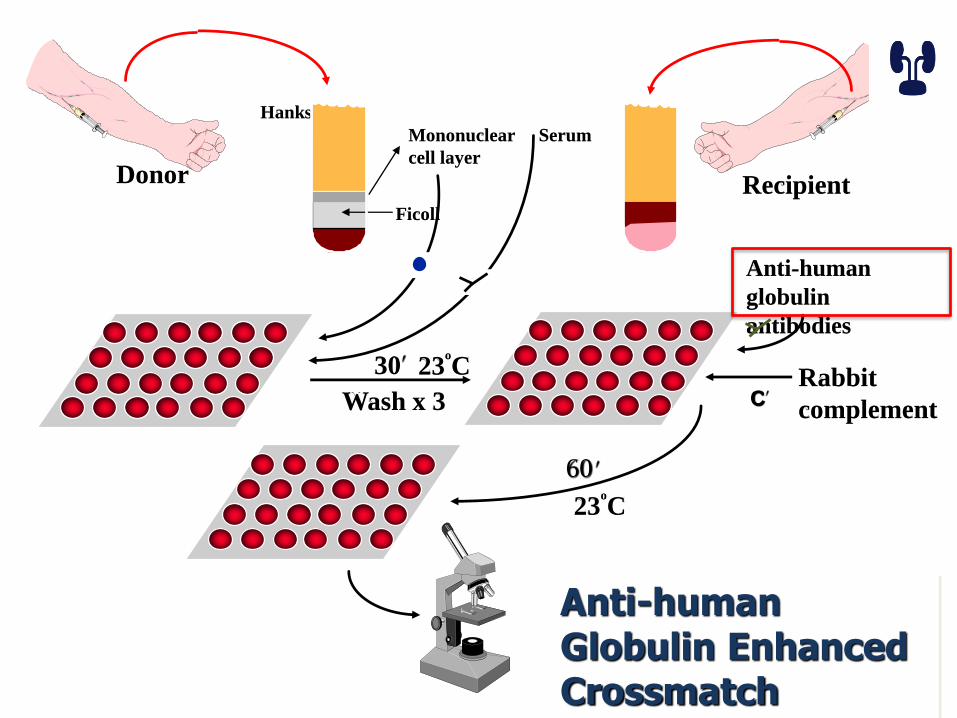
Donor
Hanks
Mononuclear
cell layer
Ficoll
Recipient
Serum
Anti-human
globulin
antibodies
23o
C30
23o
C
60
Anti-human Globulin Enhanced Crossmatch
Wash x 3Rabbit
complementC

Laser
Cells
Flow chamber
Laser activated fluorochromes
emit light in red or green spectrum
Flow Crossmatch
Donor cells are incubated with
recipient serum and then fluorochrome-coated antihuman
antibodies
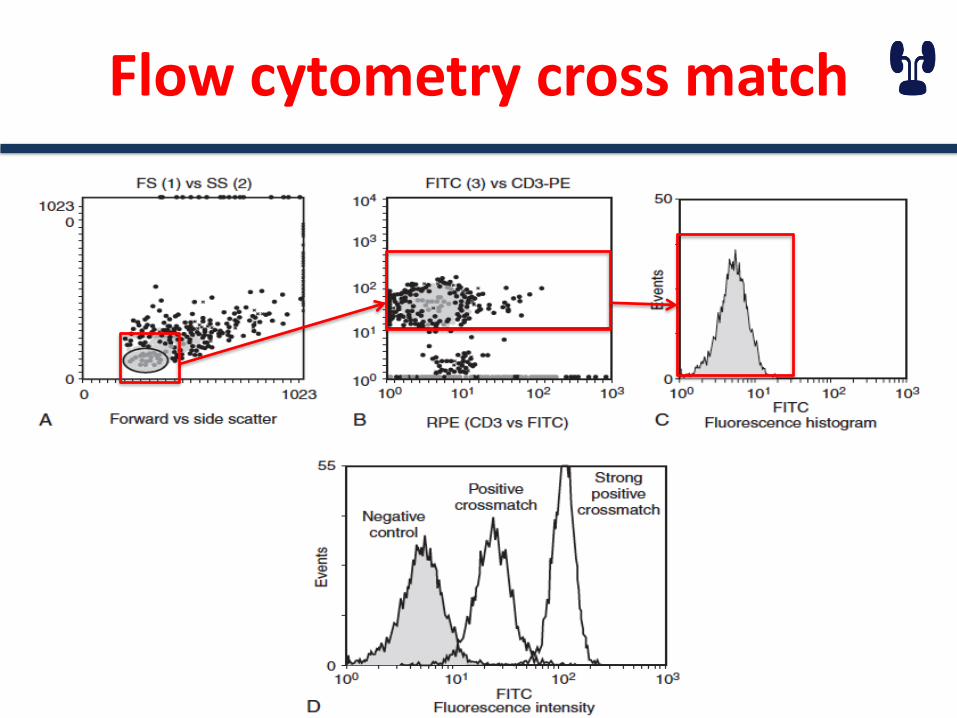
Flow cytometry cross match

HLA TYPING
•MHC class I molecules•HLA A, B, C•found on all nucleated cells
•MHC class II molecules•HLA DP, DQ, DR•Expressed on antigen presenting cells (and inducible)
•Nomenclature • according to the techniques “ serological or DNA sequencing “
Immunological work up
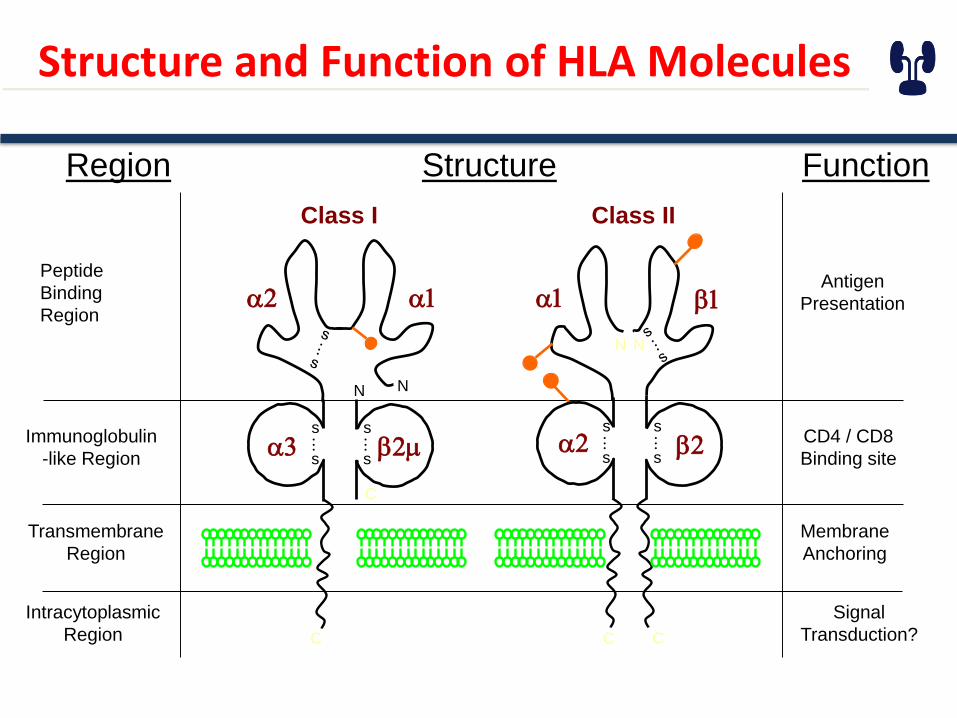
Structure and Function of HLA Molecules
StructureRegion
Peptide
Binding
Region
Immunoglobulin
-like Region
Transmembrane
Region
Intracytoplasmic
Region
Function
Antigen
Presentation
CD4 / CD8
Binding site
Membrane
Anchoring
Signal
Transduction?
C
C
Class I
a2 a1
NN
a3 b2ms
.
..s
s
.
..s
C C
Class II
NN
a1 b1
a2 b2s
.
..s
s
.
..s
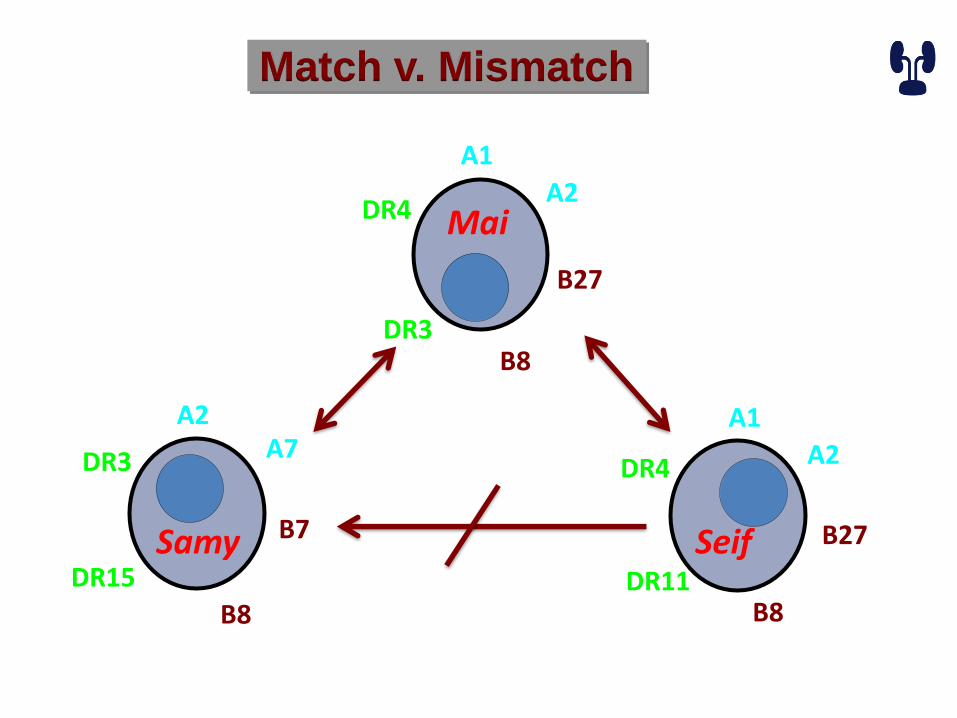
Match v. Mismatch
A2A7
B7
B8
DR15
DR3
Samy
A1
A2
B27
B8DR3
DR4 Mai
A1
A2
B27
B8DR11
DR4
Seif

PRA
• Panel Reactive Antibodies
• Donor non specific
• Donor specific
• Different limit across centers

Why Do Patients Make Anti-HLA Antibodies?
Antibodies occur due to exposure to:
-- blood product
-- pregnancies
-- transplants
-- idiopathic
Identification of transmissible infection
• Identification of transmissible infection
– HCV, HBV, HIV and CMV
– TB
– Rapid plasma reagin
– Strongleloids, Trypanosoma cruzi and West Nile virus
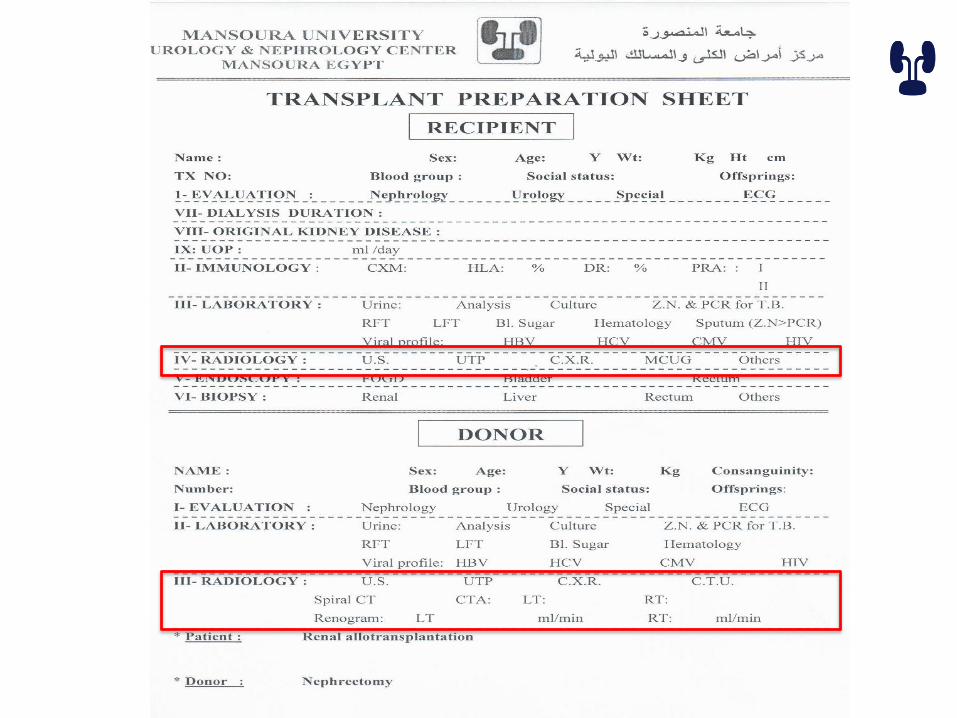

DONOR RADIOLOGICAL ASSESSMENT
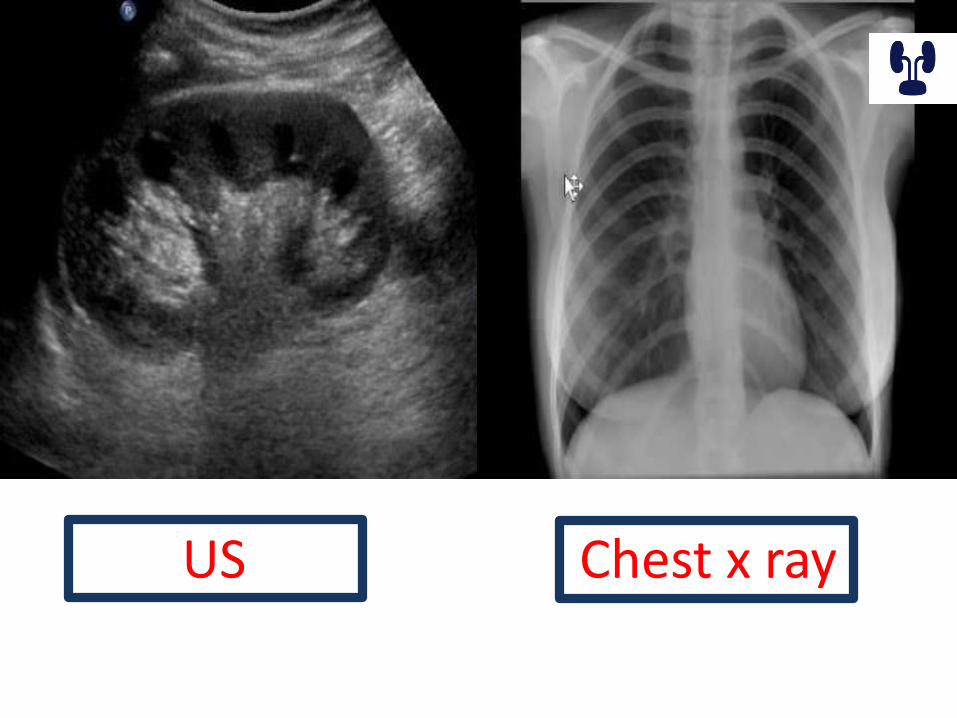
US Chest x ray
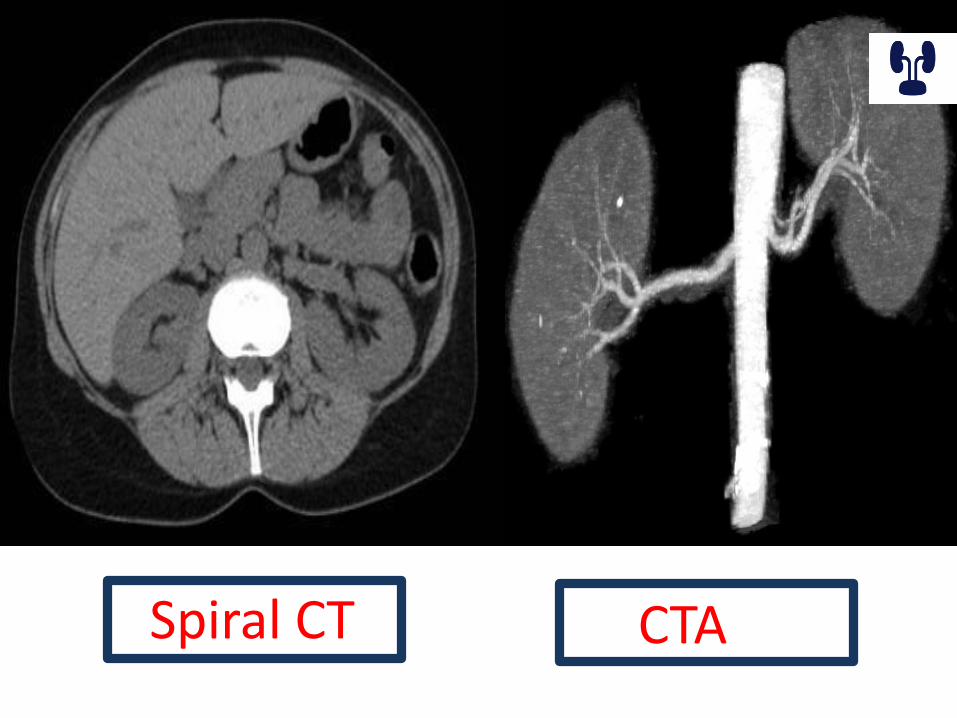
Spiral CT CTA
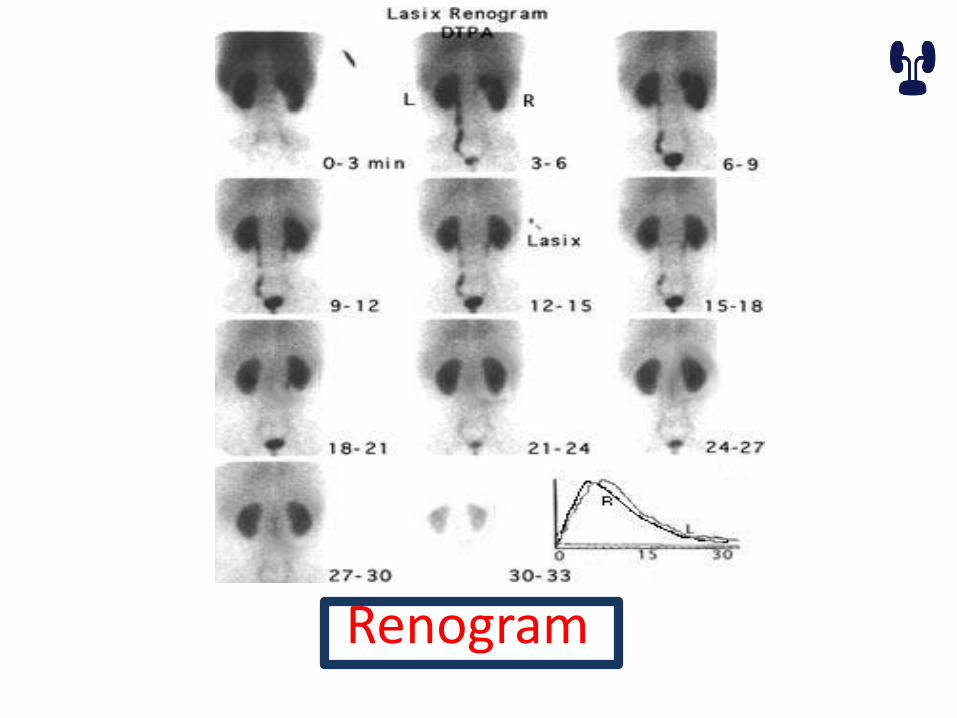
Renogram
RECIPIENT RADIOLOGICAL ASSESSMENT
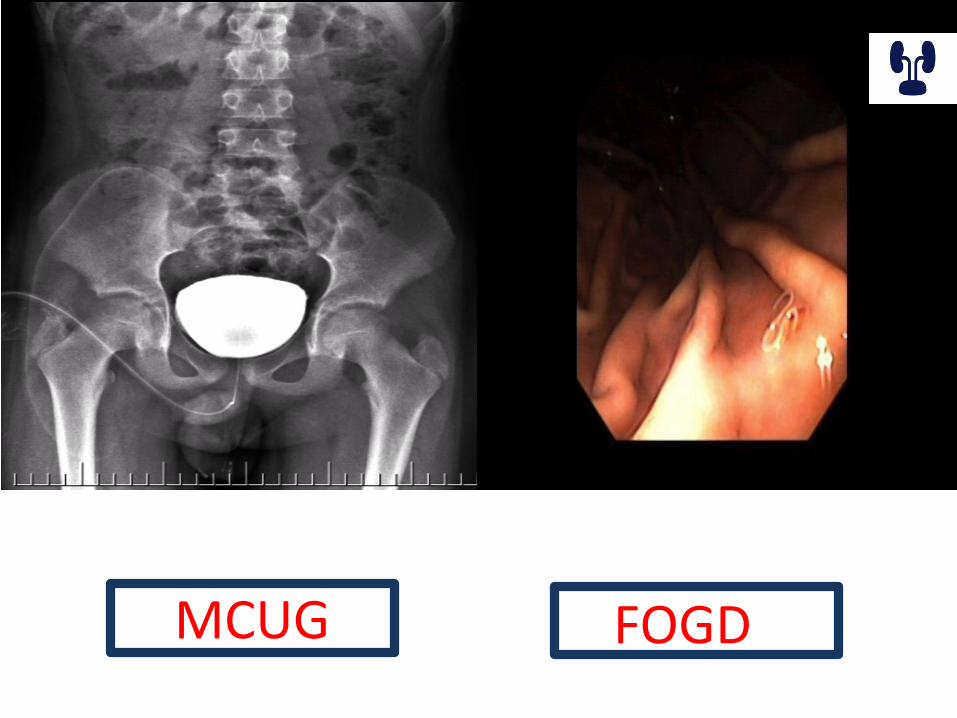
MCUG FOGD

ENDOSCOPY
• Cystoscopy
– Exclude any bladder lesion
–Any uretheral narrowing
–Assessment of bladder capacity
–Biopsy any suspicious lesions

SURPRISES
SURPRISES
• FINAL CROSS MATCH
• INEVITABLE BLOOD TRANSFUSIONS
• CATCHING INFECTIONS
• DONOR HESITATION
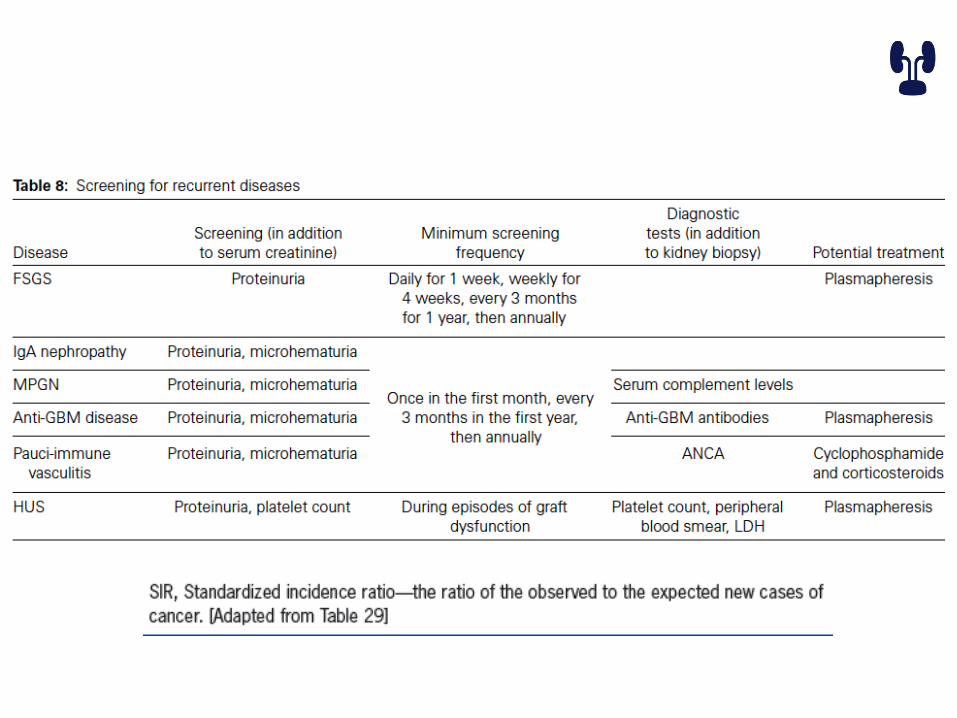
• RECURRENT DISEASES “MODIFIED PROTOCOL”
• MISSED DATA “HISTORY”
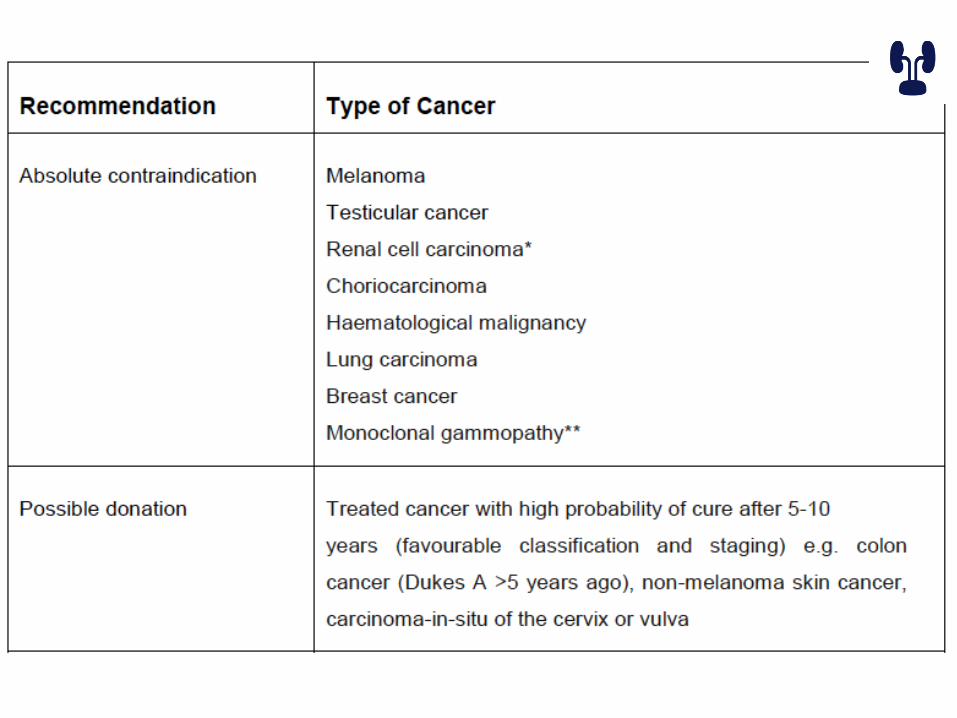
Contraindication for donation
• Absolute – <18 year-old – Active substance abuse– Impaired ability ta make a decision– Hypertension – DM– Morbid obesity– Renal disease– Renal stones – Inherited renal disease– Infections – Cancer – Cardiovascular disease – Significant size discrepancy

Contraindication for donation
• Relative
– Age > 65
– Controlled Hypertension
– Impaired glucose tolerance
– Obesity
– Borderline line renal function
– Microscopic hematuria
– Single renal stone
SPECIFIC SITUATIONS
• Re-transplant patient
– Cause of the first graft loss
– Duration of the first transplant
– Nephrectomy
– Malignancy, cardiovascular risk
SPECIFIC SITUATIONS
• pre-sensitized patient

How we detect it
• Serology
• DNA sequencing
– SSOP (sequence specific oligonucleotide probe)
– SSP (sequence specific primer)
– SBT (sequencing based typing)
Cells vs. Beads for PRA and antibody specificity determination
• Cells have multiple HLA antigens
• Use of donor cells determines if a patient has antibodies to donor antigens (OK for the crossmatch)
• But cells do not allow identification of specific antigens to which a patient has antibodies
• Beads have only HLA and their use can determine PRA and identify antibodies to specific antigens
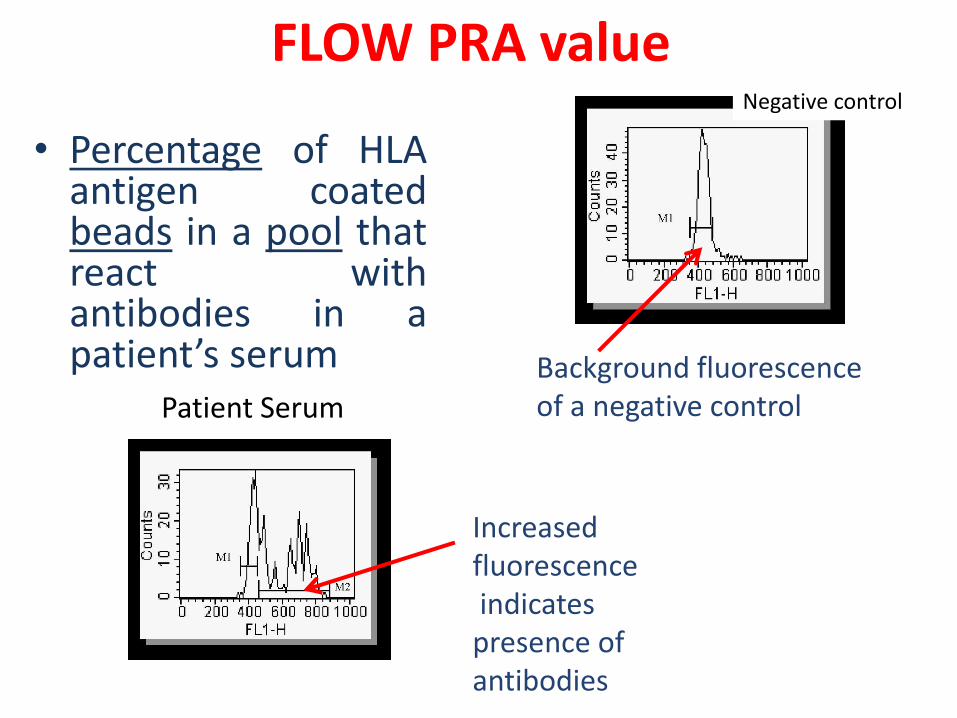
FLOW PRA value
• Percentage of HLAantigen coatedbeads in a pool thatreact withantibodies in apatient’s serum
Negative control
Patient Serum
Background fluorescenceof a negative control
Increased fluorescenceindicatespresence of antibodies
40
50
60
70
80
90
100
0 1 2 3 4
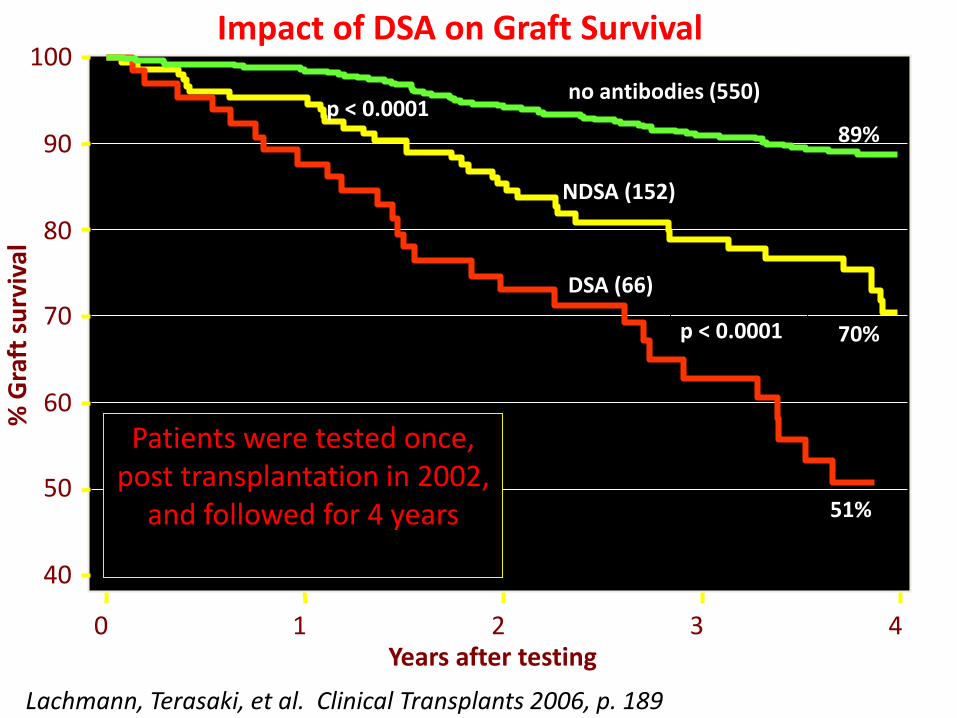
NDSA (152)
DSA (66)
no antibodies (550)
89%
Years after testing
% G
raft
su
rviv
al
p < 0.0001
p < 0.0001 70%
51%
Lachmann, Terasaki, et al. Clinical Transplants 2006, p. 189
Impact of DSA on Graft Survival
Patients were tested once, post transplantation in 2002,
and followed for 4 years
HLA Antibody Identification
•Using Luminex Single Antigen Beads
•Beads have HLA molecules of a single specificity
•Can identify unacceptable donor antigens
•Can identify acceptable donor antigens
