preoperative investigation of the surgical patient
TRANSCRIPT
PREOPERATIVE ASSESSMENT
Preoperative investigation ofthe surgical patientBrian McKinney
Elisabeth Harvey
AbstractPerioperative risk can be minimized through the identification, assess-
ment and optimization of co-morbidities. This article considers the role
of preoperative investigation, with reference to current anaesthetic and
surgical guidelines, in both the reduction of patient risk and improvement
of perioperative outcome.
Keywords Anaesthetic; guidelines; investigations; preoperative; routine;
surgical
Straight and Crooked Thinking
In an enlightening British Medical Journal article1 entitled
‘Straight and Crooked Thinking’ published in 1954, the physician
Richard Asher challenged doctors to consider five questions,
reproduced below, before requesting any medical investigations:
(1) Why do I order this test?
(2) What am I going to look for in the result?
(3) If I find it will it affect my diagnosis?
(4) How will this affect my management of the case?
(5) Will this ultimately benefit my patient?
Asher also suggested that every laboratory request form should
have a space in which the doctor stated the honest reason for
ordering the test. Whilst nearly 60 years have elapsed since this
article was published, the tongue-in-cheek answers he suggested
are still relevant today:
(1) I order this test because if it agrees with my opinion I will
believe it, and if it does not I shall disbelieve it.
(2) I do not understand this test and am uncertain of the normal
figure, but it is the fashion to order it.
(3) Whenmy chief asks if you have done this or that test I like to say
yes, so I order as many tests as I can to avoid being caught out.
(4) I have no clear idea what I am looking for, but in ordering this
test I feel in a vague way (like Mr Micawber) that something
might turn up.
(5) I order this test because I want to convince the patient there is
nothing wrong, and I don’t think he will believe me without
a test.
Brian McKinney MAMB BChir FANZCA is a Locum Consultant Anaesthetist at
Addenbrooke’s Hospital, Cambridge, UK. Conflicts of interest: none
declared.
Elisabeth Harvey BSc(Hons) MBChB (Hons) MRCS is a Speciality Registrar in
Anaesthetics at Addenbrooke’s Hospital, Cambridge, UK. Conflicts of
interest: none declared.
SURGERY 29:3 115
Clearly, if there is no genuine indication to order a test, and the
result will fail to alter management, there will be questionable
benefit for the patient. The simple process of reviewing medical
records, taking a thorough history and performing a clinical
examination is far more likely to highlight significant morbidity.
Preoperative investigations should merely supplement this impor-
tant process.
The Association of Anaesthetists of Great Britain and Ireland
(AAGBI) publication ‘Pre-Operative Assessment - The Role of the
Anaesthetist’2 features the pivotal observation that: ‘routine
preoperative investigations are expensive, labour intensive and
of questionable value, especially as they may contribute to
morbidity or cause additional delays due to spurious results’.
Types of preoperative investigation
Preoperative investigations can be subdivided into two
categories:
� Surgical investigations to assist in the diagnosis of disease or
planning of treatment.
� Anaesthetic investigations to:
� assess pre-existing co-morbidities
� identify potential anaesthetic problems
� assess the patient’s level of aerobic fitness and functional
reserve
� facilitate preoperative optimization
� enable proactive preparation for intraoperative events (e.g.
elective use of cell salvage for patients with atypical red cell
antibodies at risk of haemorrhage)
� recognize patients with a high risk of perioperative
complications
� enable risk stratification and informed consent
� establish the required level of postoperative care (ward,
high-dependency unit, intensive care unit)
� determine baseline measurements for postoperative
reference
� correct physiological abnormalities.
Routine investigations
Perioperative risk can be minimized through the identification,
assessment and optimization of co-morbidities. A traditional
strategy has been to order a set of ‘routine investigations’, and to
react to results outside the ‘normal range’.
The ‘normal range’ quoted for most laboratory results (e.g. hae-
moglobin, sodium, creatinine) is the mean � 1.96 standard devia-
tions. Therefore, 5% of ‘normal’ test results for ‘normal’ individuals
will lieoutside the reference range.As theprobability that the result of
a test will lie within the reference range is 0.95 (i.e. 95%), the likeli-
hood of obtaining 20 ‘normal’ results is only 36%(i.e. 0.9520¼ 0.36).
The greater the number of tests performed, the greater the chance of
finding an abnormal result in an otherwise healthy patient.3
Primum non nocere
Sensitivity is the measure of the ability of a test to correctly
identify a positive result where one exists. In contrast, specificity
is the measure of the ability of a test to correctly identify
a negative result where one exists. The ideal test would therefore
be both specific and sensitive, acceptable to the patient, cost
� 2010 Elsevier Ltd. All rights reserved.
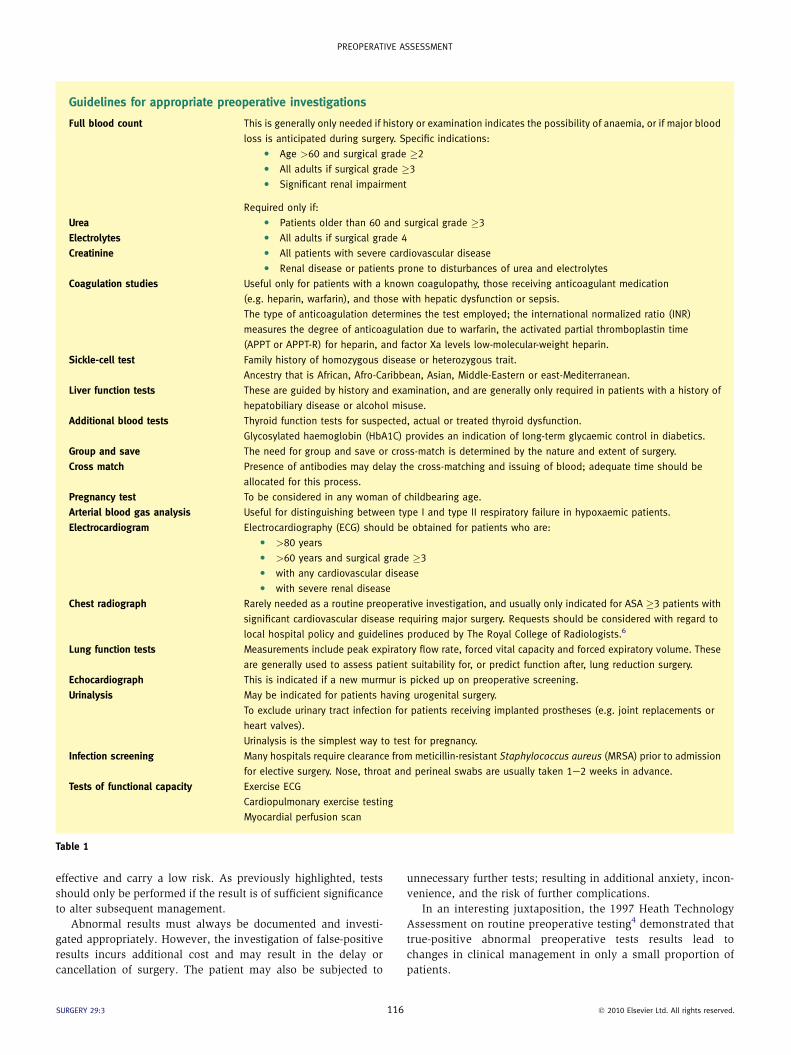
Guidelines for appropriate preoperative investigations
Full blood count This is generally only needed if history or examination indicates the possibility of anaemia, or if major blood
loss is anticipated during surgery. Specific indications:
C Age >60 and surgical grade �2
C All adults if surgical grade �3
C Significant renal impairment
Required only if:
Urea C Patients older than 60 and surgical grade �3
Electrolytes C All adults if surgical grade 4
Creatinine C All patients with severe cardiovascular disease
C Renal disease or patients prone to disturbances of urea and electrolytes
Coagulation studies Useful only for patients with a known coagulopathy, those receiving anticoagulant medication
(e.g. heparin, warfarin), and those with hepatic dysfunction or sepsis.
The type of anticoagulation determines the test employed; the international normalized ratio (INR)
measures the degree of anticoagulation due to warfarin, the activated partial thromboplastin time
(APPT or APPT-R) for heparin, and factor Xa levels low-molecular-weight heparin.
Sickle-cell test Family history of homozygous disease or heterozygous trait.
Ancestry that is African, Afro-Caribbean, Asian, Middle-Eastern or east-Mediterranean.
Liver function tests These are guided by history and examination, and are generally only required in patients with a history of
hepatobiliary disease or alcohol misuse.
Additional blood tests Thyroid function tests for suspected, actual or treated thyroid dysfunction.
Glycosylated haemoglobin (HbA1C) provides an indication of long-term glycaemic control in diabetics.
Group and save
Cross match
The need for group and save or cross-match is determined by the nature and extent of surgery.
Presence of antibodies may delay the cross-matching and issuing of blood; adequate time should be
allocated for this process.
Pregnancy test To be considered in any woman of childbearing age.
Arterial blood gas analysis Useful for distinguishing between type I and type II respiratory failure in hypoxaemic patients.
Electrocardiogram Electrocardiography (ECG) should be obtained for patients who are:
C >80 years
C >60 years and surgical grade �3
C with any cardiovascular disease
C with severe renal disease
Chest radiograph Rarely needed as a routine preoperative investigation, and usually only indicated for ASA �3 patients with
significant cardiovascular disease requiring major surgery. Requests should be considered with regard to
local hospital policy and guidelines produced by The Royal College of Radiologists.6
Lung function tests Measurements include peak expiratory flow rate, forced vital capacity and forced expiratory volume. These
are generally used to assess patient suitability for, or predict function after, lung reduction surgery.
Echocardiograph This is indicated if a new murmur is picked up on preoperative screening.
Urinalysis May be indicated for patients having urogenital surgery.
To exclude urinary tract infection for patients receiving implanted prostheses (e.g. joint replacements or
heart valves).
Urinalysis is the simplest way to test for pregnancy.
Infection screening Many hospitals require clearance from meticillin-resistant Staphylococcus aureus (MRSA) prior to admission
for elective surgery. Nose, throat and perineal swabs are usually taken 1e2 weeks in advance.
Tests of functional capacity Exercise ECG
Cardiopulmonary exercise testing
Myocardial perfusion scan
Table 1
PREOPERATIVE ASSESSMENT
effective and carry a low risk. As previously highlighted, tests
should only be performed if the result is of sufficient significance
to alter subsequent management.
Abnormal results must always be documented and investi-
gated appropriately. However, the investigation of false-positive
results incurs additional cost and may result in the delay or
cancellation of surgery. The patient may also be subjected to
SURGERY 29:3 116
unnecessary further tests; resulting in additional anxiety, incon-
venience, and the risk of further complications.
In an interesting juxtaposition, the 1997 Heath Technology
Assessment on routine preoperative testing4 demonstrated that
true-positive abnormal preoperative tests results lead to
changes in clinical management in only a small proportion of
patients.
� 2010 Elsevier Ltd. All rights reserved.

PREOPERATIVE ASSESSMENT
Guidelines for preoperative investigations
Preoperative investigations aid anaesthetic planning and
management. They are not designed, nor are they suitable, for
screening. Healthy patients undergoing minor surgery do not
require preoperative investigations. The AABGI guideline
emphasizes the importance of identifying patients who require:
� few or no preoperative investigations
� targeted investigations, the results of which must be available
when the anaesthetist sees the patient in the immediate
preoperative period
� further investigations or treatment before being referred for
anaesthetic assessment prior to admission for surgery
� further assessment or referral after specific investigations.In more complicated cases, a discussion with the anaesthetist, in
conjunction with reference to both local and National Institute for
Health and Clinical Excellence (NICE) guidelines,5 will influence
both the need and justification for subsequent investigations.
Important factors to consider include the following: the magnitude
or grade of surgery (see Table 3 on page 114 of this issue), the
physical status of patient (see Table 2 on page 113 of this issue),
specific patient groups (e.g. children, the elderly, the morbidly
obese) and specific procedures (e.g. the role of lung function tests in
thoracic surgery).
The context of an operation (elective versus emergency) will
also alter the necessity for preoperative investigations, as
emphasis shifts from non-essential tests to potentially life-saving
surgical intervention.
The preoperative tests
The standard preoperative tests, with reference to AAGBI
Guidelines, are discussed in Table 1.
Changes in clinical management
Successful investigations can reduce perioperative complications,
shorten the duration of admission, and avoid unnecessary delays or
cancellation of surgery. According to the consultant anaesthetists
and trainee surgeons who were interviewed by the National Insti-
tute for Clinical Excellence for the 2003 preoperative test guidelines,
the most common changes in a patient’s clinical management
following an abnormal preoperative test result include:
� referral to another specialist
� cancellation or postponement of surgery
� change in the surgical procedure
� change in the anaesthetic technique
� prescription of a new medication
� provision of physiotherapy
� change in existing medication
SURGERY 29:3 117
� proactive (rather than reactive) preparation for possible
events during surgery
� correction of physiological abnormalities
� administering a blood transfusion
� planning for higher levels of postoperative care
� planned overnight admission for patients previously sched-
uled as ‘day cases’.
These outcomes closely mirror the purpose of anaesthetic
preoperative investigations; the correct choice of test can therefore
alter patient management and result in an improved outcome.
Conclusion
The American Society of Anesthesiologists 2002 guideline on
preanesthesia evaluation concluded: ‘Routine pre-operative tests
(i.e. tests intended to discover a disease or disorder in an
asymptomatic patient) do not make an important contribution to
the process of perioperative assessment and management of the
patient by the anesthesiologist.’7
Clearly the process of successfully preparing a patient for
surgery requires good teamwork and effective communication
between surgical and anaesthetic teams. The pre-morbid state of
the patient, and both the nature and context of surgery, will
influence the necessity and speed with which investigations are
obtained. Tests should only be performed if the outcome will
change subsequent patient management. A
REFERENCES
1 Asher R. Straight and crooked thinking in medicine. Br Med J 1954; 2:
460e2.
2 Pre-operative assessment: the role of the anaesthetist. Association of
Anaesthetists of Great Britain and Ireland, http://www.aagbi.org/
publications/guidelines/docs/preop2010.pdf; 2010.
3 Klein AA, Arrowsmith JE. Should routine preoperative testing be
abandoned? Anaesthesia 2010; 65: 974e6.
4 Munro J, Booth A, Nicholl J. Routine preoperative testing:
a systematic review of the evidence. Health Technol Assess 1997;
1: ieiv.
5 Clinical guideline number 3. Preoperative tests: the use of routine
preoperative tests for elective surgery. National Institute for Clinical
Excellence, http://guidance.nice.org.uk/CG3; 2003.
6 Royal College of Radiologists. Making the best use of clinical
radiology services. 6th edn. London: Royal College of Radiologists,
2007.
7 American Society of Anesthesiologists Task Force on Preanesthesia
Evaluation. Practice advisory for preanesthesia evaluation.
Anesthesiol 2002; 96: 485e96.
� 2010 Elsevier Ltd. All rights reserved.