prenatal part 2 · preparing for c/s lots of people involved; anesthetist, obstetrician, residents,...
TRANSCRIPT

PRENATAL PART 2

PART 2 OUTLINE
Variations in Labour
Cesarean Sections
Hospital Routines/Inductions

VARIATIONS IN LABOUR

VARIATIONS IN LABOUR
Posterior position (OP)
Breech
Rapid/Short 1-4 hrs
Prolonged >24 hrs
Dysfunctional
Preterm
Cesarean Section

POSTERIOR POSITION
Baby face up instead of face down
A lot of back pain for mom
Coach …rubbing, back massage & hot/cold compresses

VARIATIONS IN LABOUR
Posterior position (OP)
Breech
Rapid/Short 1-4 hrs
Prolonged > 24 hrs
Dysfunctional
Preterm
Cesarean Section

BREECH
Frank, Complete, Incomplete (Footling)
Bum first presentation
Approx. 3 wks before due date, U/S will show babe’s position… usually stays in this position until delivery
May still deliver vaginally – Dr.’s recommendation


BREECH DELIVERY MAYBE…
Umbilical cord not in the way
Baby not too big/small (~5.5-8.5lbs)
Frank or Complete Breech Position
Maternal pelvis adequate diameter
Doctor’s skill/comfort level

VARIATIONS IN LABOUR
Posterior position (OP)
Breech
Rapid/Short 1-4 hrs
Prolonged >24 hrs
Dysfunctional
Preterm
Cesarean Section

RAPID LABOR
Occurs in 1-4 hrs
Difficult to get into a rhythm with contractions
Difficult to prepare self for contraction
DON’T drive self to hospital; call an ambulance

VARIATIONS IN LABOUR
Posterior position (OP)
Breech
Rapid/Short 1-4 hrs
Prolonged >24 hrs
Dysfunctional
Preterm
Cesarean Section

R/t:
Full Bladder
Small pelvis & large babe (CPD)
Bedrest
Dysfunctional labour
Note: Augmentation (getting labour going
with medical intervention) may be necessary.
PROLONGED LABOR (>24HRS)

VARIATIONS IN LABOUR
Posterior position (OP)
Breech
Rapid/Short 1-4 hrs
Prolonged >24 hrs
Dysfunctional
Preterm
Cesarean Section

DYSFUNCTIONAL LABOUR
Ineffective contractions, cervix not thinning or opening & babe not descending
May be related to position of babe
Medication/epidural given too soon
Note: Augmentation (getting labour going with medical intervention) may be necessary.

VARIATIONS IN LABOUR
Posterior position (OP)
Breech
Rapid/Short 1-4 hrs
Prolonged >24 hrs
Dysfunctional
Preterm
Cesarean Section
PRETERM DELIVERY
Delivery <37wks
7.8% of Cdn. deliveries (2012)
Cause is often uncertain
Some risk factors: smoking, overworked, alcohol/drug use, abuse, untreated infections, underweight, premature rupture of membranes.

VARIATIONS IN LABOUR
Posterior position (OP)
Breech
Rapid/Short 1-4 hrs
Prolonged >24 hrs
Dysfunctional
Preterm
Cesarean Section

CESAREAN SECTIONS

Maternal Medical
Conditions:
1. Gestational
Diabetes
2. Severe Toxemia
3. Ruptured
membranes
without labour
>24 hrs
4. Uterine
Dystocia
5. Arrested
Labour
6. Active Herpes

CESAREAN SECTIONS
Low Segment Incision Classical Incision
Only in emergency situations The common method

What to Expect…

PREPARING FOR C/S
Lots of people involved; anesthetist, obstetrician, residents, 2+ RNs, baby team
Don’t forget camera!!
Dad/Support Person changes into “greens” then waits outside OR, while mom goes in to be “prepped”
Mom to OR table, epidural inserted (if not already in place), monitors applied, urinary catheter inserted, abd. washed, draped with sterile green cloths

PREPARING FOR C/S CNT’D
Now Dad/SP called in to OR & sits by mom’s head
Surgery begins, takes approx. 1.5 hrs (start to finish)
Baby out in less than 10 mins
Note: Dad/SP not allowed in OR if mom getting general anesthesia (waits next door)

RECOVERY ROOM
Vital signs taken often
Vaginal flow & dressing monitored
Height of uterus (fundus) measured
Pain meds given
Epidural wears off & sensation returns
Most of the above also done after
vaginal birth

POST CESAREAN DIFFICULTIES
Discomfort d/t: pain at incision, abd. gas, lung congestion
Lack of mobility: IV, catheter, discomfort
Fatigue
Healing of incision
Bonding with Baby

PARTNER’S FEELINGS
Fear for loved one & baby during procedure
Not being needed
Overwhelmed & unsure of how to help loved one
Concerns related to baby
Neglected by family & friends who are concerned primarily about mom & baby

HELPFUL HINTS FOR HOME AFTER A C-SECTION
DON’T feel guilty about asking family for help (cooking, housekeeping, laundry, grocery shopping)
Postpone visitors for 1 week (for much needed rest) & keep visits short as you will find you tire easily
If friends or family offer to help, suggest a ready-made meal

HOSPITAL ROUTINES
INDUCTIONS

MONITORING
Purpose to monitor variations/changes in labour & detect complications
Vital signs; BP, pulse, temp
Vaginal/Pelvic exams
Cervical dilation
Station, presentation & position of baby
Amniotic fluid; odour, color
Fetal heart rate

EXTERNAL FETAL HEART MONITORING
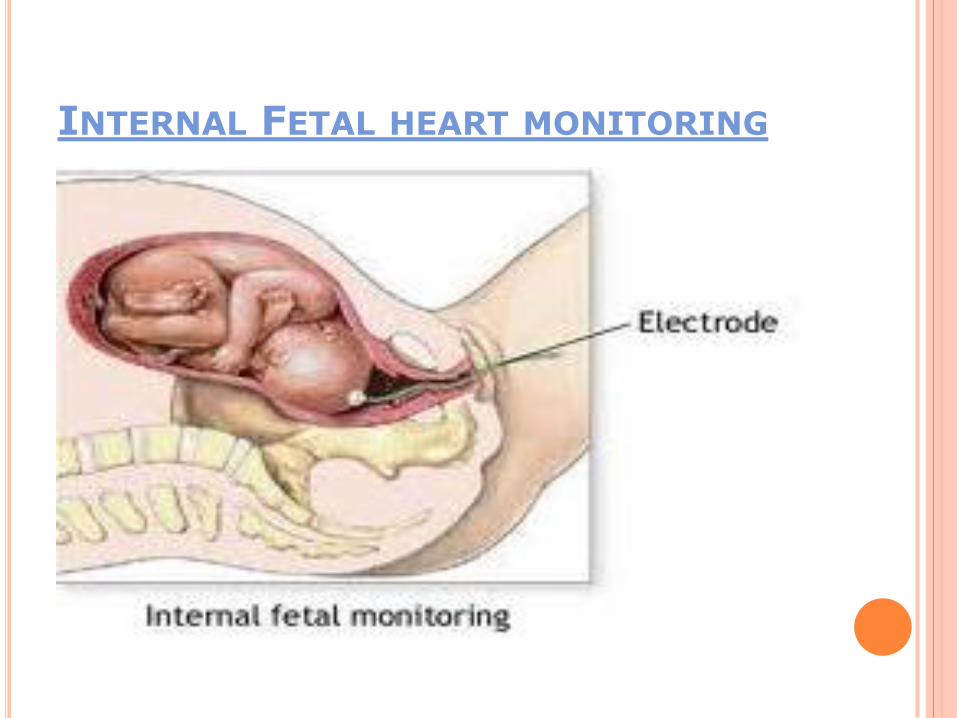
INTERNAL FETAL HEART MONITORING

INDUCTION OF LABOUR
The artificial initiation of labour
Considered when wellbeing of mother or baby makes delivery necessary
High blood pressure (PIH)
Diabetes
Overdue (close to 42 wks)
Decreased fetal movement or other fetal compromises
Rh Incompatibility (rare)

TYPES OF INDUCTIONS
Artificial rupture of membranes (ARM)
Prostaglandins (gel, suppository)
Prostin, Prepidil, Cervidil
Oxytocin/Syntocinon (Pitocin in USA)

ARTIFICIAL RUPTURE OF MEMBRANES
Amniotomy
Use an amnihook
Tear an opening in the amniotic sac

ARTIFICIAL RUPTURE OF MEMBRANES
Speeds up labour (pressure of babe’s head on cervix)
Examine amniotic fluid
Necessary for internal fetal heart monitoring
Doesn’t always work
No more ‘cushion’ of fluid around baby
Cord prolapse (if fetal head not well applied to cervix)
Benefits Risks

PROSTAGLANDINS
Ripens/softens the cervix
Gets labour started
More freedom for mom
May not work
Bring on labour ‘fast and furiously’
Benefits Risks

OXYTOCIN/SYNTOCINON
Increases frequency & intensity of contractions
Helps to dilate cervix & move baby down birth canal
Contractions more difficult to manage ( nature of labour)
Continuous fetal monitoring
Increased risk for more medical interventions
Benefits Risks

POSSIBLE ALTERNATIVES
Nipple stimulation – causes the release of oxytocin, increasing uterine contractions
Sexual intercourse – orgasm stimulates uterus to start contracting

EPISIOTOMY
Enlarge vaginal opening just before baby is born
Fetal distress
Protect pelvic floor
Forceps or vacuum
May tear spontaneously without one

ADVANTAGES OF EPISIOTOMY
Possibly shortens 2nd stage of labour
May prevent severe, uncontrolled tears

AVOIDING EPISIOTOMY/TEARING PRENATALLY
Kegel exercises
Practice the various positions used in labour
Perineal massage
Good nutrition to promote healthy tissues
Avoiding Episotomy/tearing during labour
Relaxing the perineum
Don’t rush ‘bearing down’
Use gravity – neutral positions (squatting, semi-sitting)
Perineal massage, support
Warm compresses

FORCEP & VACUUM EXTRACTION
Fetal distress
Babe not progressing down birth canal
Exhaustion
Anesthetic – mom too ‘frozen’ to push effectively
Vaginal canal too small & mom needs help delivering
FORCEP & VACUUM EXTRACTION DISADVANTAGES
May cause tears
May cause injury to babe
Temporary bruising or changes to shape
of baby’s head

REFERENCES
Slide10 http://www.umm.edu/graphics/images/en/19158.jpg
Slide24 bringbirthhome.com
Slide25 westechinc.com
Slide27 lifeinpain.org
Slide28 yoursurgery.com
Slide39 pregnancy.lovetoknow.com
Slide40 nlm.nih.gov
Slide43 babble.com