preliminary study of the situation of health care services for persons with depressive symptoms: the...
TRANSCRIPT

Preliminary study of the situation of health care services for persons with depressive symptoms:
the case study from Yasothorn province
Acharaporn Seeherunwong* DNS, RN, Assist. Prof.
Prapa Yuttatri* DNS, RN, Assist. Prof.
Atittaya Pornchaikate* PhD (Nursing), RN
Walailak Pumpuang* MA (Ed. Psy. and guidance)
Kedsaraporn Kenbubha** MSc (Epidemiology)
Chintana Polmesak*** BSc (Public Health)
Therapa Thanee** MEd (Guidance and Counseling)
* Faculty of Nursing, Mahidol University
** Prasrimahabhodi Psychiatric Hospital
*** Provincial Public Health Office

Acknowledgements
• Department of Mental Health, Ministry of Public Health
• Staff from Provincial Public Health Offices• Director and Staff from Prasrimahabhodi
Psychiatric Hospital• Consultants: Thoranin Kongsuk, Director of
Prasrimahabodhi Psychiatric Hospital : Siriorn Sindu, Assoc. Prof.,
Faculty of Nursing , Mahidol University

Background
• Depressive symptoms are a common health problem founded in all level of health services.
• Depressive disorders are the disorders that have the highest DALYs score among all psychiatric disorders (cause persons lose their years of healthy living)
(Bureau of Policy and strategy, MOPH, 1999) • Northeastern part of Thailand has the highest
prevalence of MDD (6.33%) and Dysthymia (2.48%)
(The 2003 National Epidemiology Survey on Mental Health in Thailand, Department of Mental Health, MOPH)

Purposes of the study
• To explore health care services for persons with depressive symptoms in three parts: access to care, resources, and competency of health care providers.

Health resources -Material -persons -Technology -budget
Health care provider
competency -village volunters
-nurses-Physicians
Access to health service-experience of persons
with depressive disorders

Methods
• Design:
Qualitative research design
• Data collection:
- In depth interview
- Focus group
• Data analysis
- Content analysis

Key informants
- From in depth interview
- Total 45 persons• 5 hospital directors & 1 physician• 2 staff from Provincial Public Heath Office• 20 nurses• 4 staff from District Health Office• 14 patients

Key informants (cont.)
- From focus groups
- Total 98 persons• 2 times of focus groups with general health
care providers (12 persons)• 1 time of focus group with nurses (4 persons)• 11 times of focus groups with villages
volunteers (82 persons)

Settings
• 1 general hospital
• 2 community hospitals (60 beds)
• 5 community hospitals (30 beds)
• 9 large primary care units (PCU)
• 5 small primary care units
From 8/9 districts in Yasothorn province


The province is subdivided into 9 districts (Amphoe). The districts are further subdivided into 78 communes (tambon) and 835 villages.
1.Mueang Yasothon 2.Sai Mun 3.Kut Chum 4.Kham Khuean Kaeo 5.Pa Tio
6.Maha Chana Chai 7.Kho Wang 8.Loeng Nok Tha 9.Thai Charoen
Map of Yasothorn province

Pathway of receiving mental health services
Formal service pathway to be covered by the universal health care coverage (30 Baht policy)
Prasrimahabhodi Psychiatric Hospital (PPH)
General hospital
Primary care unit
(PCU )
Community hospital
- Patients receive services at own convenience (pay for services by themselves)- 2 emergency visits covered by the 30 Baht policy)
Phrasrimahabodi (PPH)
General hospital
Primary care unit (PCU )
Community hospital
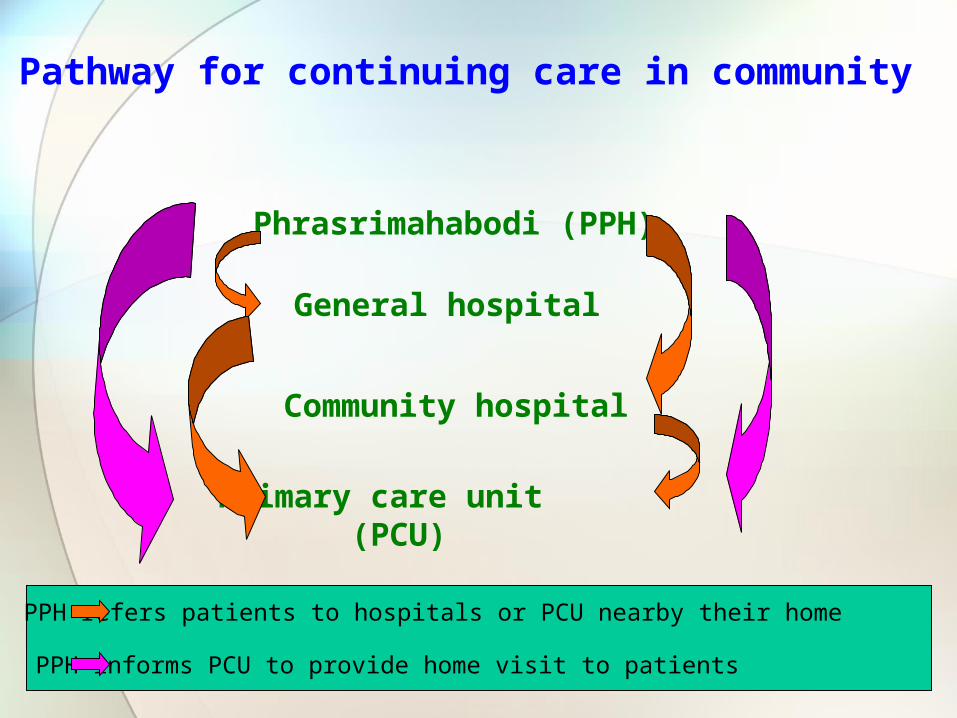
Pathway for continuing care in community
PPH refers patients to hospitals or PCU nearby their home
PPH informs PCU to provide home visit to patients

Results• 3 major aspects
- Health ResourcesPolicyBudgetMaterials Personnel
- Competency of ProvidersPhysiciansNursesPublic health officersVillage volunteers
- Access to Health CarePromotionPreventionCare and CureRehabilitation
Health resources
4 aspects were consideredPolicy
Budget
Materials
Personnel

Health resources: Policy
• There were top-down policies regarding mental health issues from MOPH to all local service centers.
• No specific policy about promotion and prevention of depression, though policy to decrease the rate of suicide was apparent.
• In addition to projects that served the central policy, many hospitals/PCU developed their own projects to serve the need of people in the community

Health resources: Budgets
• Budgets were received from MOPH and MOI: local administrative organization)
• No specific budgets for mental heath services (Budgets were shared among all other services within the hospitals/PCU).
• Allocation of budgets to mental health projects depended on abilities and interests of hospital directors and mental health teams.

Health resources: Materials
• Instruments for screening and case findings of depression were available at all service levels. Yet, no practice guideline as to when such instruments would be used.
• No standardized criteria for screening risk groups and also for treatment of depressive symptoms.
• Most of the treatment provided at hospitals/PCU follow guidelines from Prasrimahabhodi Psychiatric Hospital

Health resources: Materials
• There was only TCA group (e.g. amitriptyline) available for the treatment of depression
• No document about depressive symptoms/ disorders provided to lay persons

Health resources: Personnel
Physicians
• No psychiatrist, 1 psychologist• Normally one community hospital had 2-3
physicians • Each day one physician had to take care of
more than 100 patients; they thus did not have much time to assess patients with mental health problems.
• Most physicians who took care of psychiatric patients only went through short course training in mental health.

Health resources: Personnel
Nurses• In PCU: one professional nurse and one
public health officer • In community hospitals: 2-3 professional
nurses and 2-3 technical nurses working in the psychiatric sector (some hospitals had 1-2 advance practice nurses)
• In general hospital, 5 nurses working in psychiatric unit

Health resources: Personnel
Village volunteer
• Village volunteers received training and worked together with health care providers at the PCU in health promotion and prevention in their community.
• 1 village volunteer took care of 10 households.

Health care provider competency
• Physicians
• Professional nurses
• Public health officers
• Village volunteers

Competency: Physicians
• Physicians’ skills in detecting and giving treatment of depressive symptoms depended on their experience.
• Physicians working more than 10 years had more skills in detecting depressive disorders than the novice.
• Physicians normally referred patients with depressive symptoms to psychiatric hospital for diagnosis and treatment.

Competency: Registered nurses
• Had skills in mental health promotion and prevention and establish good relationship with people in the community.
• Had skills in providing psycho-education and counseling for persons with stress and anxiety.
• Limited skills in detecting depressive symptoms and provide psychosocial treatment for psychiatric patients.
Competency: Public health officers
• Worked together with the health care team in promoting mental health for people in the community, but no specific roles in assessing and providing care for people with mental health problems

Competency: Village volunteers
• Some Village volunteers had knowledge in taking care of persons with depressive symptoms but no skills in detecting such symptoms
• They visited and provided support for people at-risk for depressive disorders and persons after attempted suicide.
• They participated in health promotion projects.

Access to care
• Promotion
• Prevention
• Care & Cure
• Rehabilitation

Access to care: Promotion & Prevention
• Promotion & Prevention
- Had policies about mental health promotion and also projects to promote mental health developed by health care providers together with people in the community (increase community participation)
- Had elderly club
- Had health promotion project at school

Access to care: Promotion & Prevention
- Had friend-corner at school (student leaders helped screen friends who had problems and refer for help)
- Covered in certain areas and age groups depending on priority setting at the hospitals/health services centers and budgets allocated

Access to care: Care & Cure
• Had responsible personnel worked directly in mental health sector in community and general hospitals.• Screened mental health problems in
chronic illness patients• Developed psychosocial interventions for
chronic illness patients• Followed up treatment among psychiatric
patients
Access to care: Care & Cure
• Lack of awareness: village volunteers, patients, and their relatives did not aware of depressive symptoms (thought that such symptoms were normal) so they did not come for treatment.
• Under detection and misdiagnosis: some patients came to the health care center, but did not get detected (due to limitation of providers’ skills)
• Low priority setting: less severity than physical problems and took time to assess and detect

Access to care: Care & Cure
• In order for the treatment to be covered by the 30-bath policy, patients had to follow the formal pathway of treatment
• Limited choices of treatment • only had Amitriptyline • focus only on treating with medicines, no
other psychosocial treatment.• Limited choices of care
• no psychosocial intervention

Access to care: Care & Cure
• Financial difficulty• Many patients had little to no money for
drugs & transportation• Transportation difficulty
• not enough public transportation.

Access to care: Rehabilitation
• Had good referral and follow-up systems • For known cases, had good referral systems
by attempting to refer patients to receive treatment at nearby hospitals
• Some patients were afraid of stigma and willing to go to receive treatment at further psychiatric hospital (not in the community)
• Support systems were mainly from family

Access to care: Rehabilitation
• No formal community services such as self-help group, government and NGO for helping psychiatric patients.
• Having continuing care on drug adherence, but no resources for helping patients regarding social and occupational functioning

Discussion
• Mental health problems were set in low priority by many health care providers when compared to physical illness: • Less severity• Take time to assess and detect mental
illness• Less confidence to provide diagnosis and
treatment
Discussion
• Since Thai culture is a collective society which normally peoples take care of each other like their relatives, having village volunteers to take care of peoples in the community fit well with the life-style.
• Some other health promotion projects also helped promote mental health.

Suggestion
• Health care providers need more training to enhance their knowledge and skills in detecting and taking care of persons with depression.
• Mental health services should be available at the community level nearby patients' home.
Suggestion
• Raise awareness of people in the community about depressive symptoms and that depressive symptoms are treatable and manageable
• Promote mental health through out the life span (e.g. stress management skills).
• Promote community participation and provision of support to patients
Suggestion
• Improve providers’ skills in detecting depressive symptom, especially, at the screening section of the OPD
• Broaden antidepressant drug frame for the community hospitals to cover wider ranges of antidepressant drugs for patients
• Should have guideline for screening depression in high risk groups
• Should have occupational and social rehabilitation projects for patients with depressive disorders.

Conclusion
• Mental health care services at Yasothorn province are growing.
• Many health care providers put their efforts in improving and providing mental health services for people in their community.
• However, patients with depressive disorders remain under detected. Raising awareness and enhancing knowledge and skills of providers and people in the community about depressive symptoms and that depressive symptoms are treatable and manageable are important
