preliminary report - harvard university are several competing theories of justice that are regarded...
TRANSCRIPT

1
BENCHMARKS OF FAIRNESS FOR HEALTH CARE REFORM: EXPERIENCE AT AN
EUROPEAN UNION COUNTRY
Preliminary Report
Rui Nunes, Guilhermina Rego, Norman Daniels
1- INTRODUCTION
All countries face the issue of choice in healthcare. It is one of the main problems ofpluralistic societies. Allocation of healthcare resources is clearly associated with theconcept of distributive justice. Yet does justice, in this context, imply the existence of aright to healthcare? If it does exist is it a fundamental right? If it is accepted as such,there is still the question of whether this right should include all types of healthcareservices or if it should be limited to selected types. It follows that choices must be madeand priorities must be set1. Different ethical foundations do exist with regards claims ofjustice in healthcare. All of them try to fulfil the formal principle of justice that equalsmust be treated equally.
Despite this formal principal, attributed to Aristotle, Tom Beauchamp and JamesChildress2 state quite clearly that whatever the ethical theory endorsed, most healthcaresystems, in practice, accept different, even contradictory material principles of justice.In fact, these principles specifying relevant properties for distribution – like need, effort,contribution, or merit of the subject – or claiming for an equal share or a free-marketexchange, are usually put into practice in most developed countries. With regards healthcare policy, European tradition claims for universal access based primarily on personalneed but also on contribution (and therefore, although indirectly, on merit and effort)and fair procedures namely free market transactions.
There are several competing theories of justice that are regarded as the properfoundation of fairness in healthcare access and delivery3. Robert Nozick, a libertarian,claims that in a fair society, rights of property and liberty are paramount. Fairprocedures (procedural justice in acquisition, transfer and rectification) shouldguarantee these rights and state intrusion is only accepted to protect them.Redistribution of private property through taxation is regarded as unjust (usually viewedas an equivalent to forced labour). Healthcare is not considered as a right under thistheory4. On the other hand, John Rawls’ Difference Principle5 argues that not onlyliberty but also fair equality of opportunity should be considered. Nevertheless, somesocial and economical inequalities are permitted as long as the greatest benefit of theleast advantaged is pursued.
1 It is frequently claimed that health care needs are infinite and therefore allocation of resources andprioritising are inevitable in public services. See Mullen, P. and Spurgeon, P., “Priority Setting & thePublic”, Radcliffe Medical Press, Abingdon, (2000).2 Beauchamp, T., Childress, J., ”Principles of Biomedical Ethics”, Oxford University Press, New York,2001, fifth edition.3 See for instance Distributive Justice: Stanford Encyclopedia of Philosophy,http://setis.library.usyd.edu.au/ stanford/archives/win1997/entries/justice-distributive/; and Kilcullen, R:Robert Nozick: against distributive justice, http://www.humanities.mq.edu.au /politics/y64117.html.4 Nozick, R., “Anarchy, State and Utopia”, Basic Books, New York, 1974.5 Rawls, J., “A Theory of Justice”, Harvard University Press, New York, 1971.
2
This egalitarian theory of justice, in the healthcare context, would imply the existence ofa decent minimum of healthcare6 although, in principle, tiering is allowed as long as theaccess to the lower level is not undermined. Utilitarian views of justice are also thebasis of most welfare systems of healthcare delivery. As long as society as a whole isbetter off with a fair distribution of resources, because it may provide the citizens thesecurity they need and therefore promote social cohesion, utility is maximised. Itfollows that the distribution of basic healthcare to all citizens is usually accepted onutilitarian grounds.
In Europe distributive justice is more often related to the concepts of equity andsolidarity. As stated in the Report by the Government Committee on Choices in HealthCare, Ministry of Welfare, Health and Cultural Affairs, The Netherlands, 1992,“Solidarity is the awareness of unity and a willingness to bear the consequences of it.Unity indicates the presence of a group of people with a common history and commonconvictions and ideals. Solidarity can be voluntary, as when people behave out ofhumanistic motives, or compulsory as when the government taxes the population toprovide services to all”. Solidarity has different historical backgrounds. It can be found,although with different names, in catholic and protestant traditions, in Marxist, socialistand even libertarian thinking. Both as a doctrine and as a political choice it is deeplygrounded is most European health care systems7.
Equity means that the material principle of justice involved in distribution of wealth ismainly based on personal need8. The pursuit of equity usually implies a reduction ofunjust disparities between individual citizens or social groups9. Equity as a politicaloption has different social and economical implications: equity insofar as resources areallocated, equity in the way healthcare services are received, and equity in the way thoseservices are paid for.
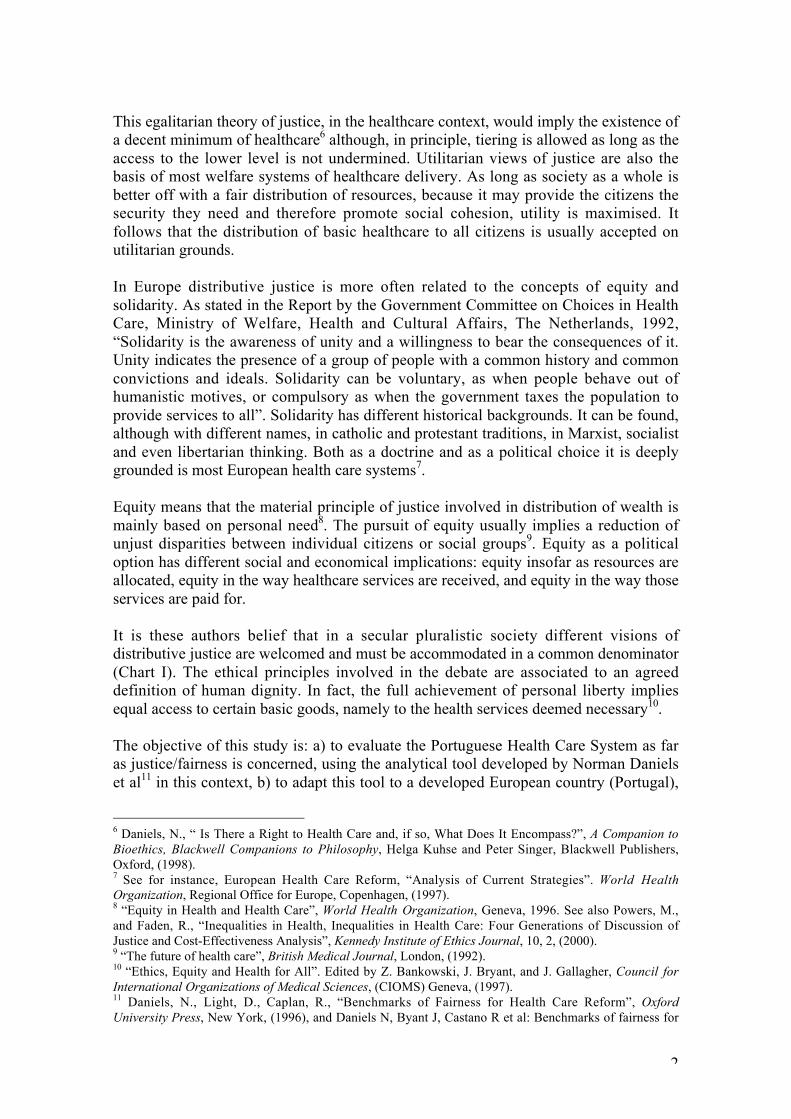
It is these authors belief that in a secular pluralistic society different visions ofdistributive justice are welcomed and must be accommodated in a common denominator(Chart I). The ethical principles involved in the debate are associated to an agreeddefinition of human dignity. In fact, the full achievement of personal liberty impliesequal access to certain basic goods, namely to the health services deemed necessary10.
The objective of this study is: a) to evaluate the Portuguese Health Care System as faras justice/fairness is concerned, using the analytical tool developed by Norman Danielset al11 in this context, b) to adapt this tool to a developed European country (Portugal),
6 Daniels, N., “ Is There a Right to Health Care and, if so, What Does It Encompass?”, A Companion toBioethics, Blackwell Companions to Philosophy, Helga Kuhse and Peter Singer, Blackwell Publishers,Oxford, (1998).7 See for instance, European Health Care Reform, “Analysis of Current Strategies”. World HealthOrganization, Regional Office for Europe, Copenhagen, (1997).8 “Equity in Health and Health Care”, World Health Organization, Geneva, 1996. See also Powers, M.,and Faden, R., “Inequalities in Health, Inequalities in Health Care: Four Generations of Discussion ofJustice and Cost-Effectiveness Analysis”, Kennedy Institute of Ethics Journal, 10, 2, (2000).9 “The future of health care”, British Medical Journal, London, (1992).10 “Ethics, Equity and Health for All”. Edited by Z. Bankowski, J. Bryant, and J. Gallagher, Council forInternational Organizations of Medical Sciences, (CIOMS) Geneva, (1997).11 Daniels, N., Light, D., Caplan, R., “Benchmarks of Fairness for Health Care Reform”, OxfordUniversity Press, New York, (1996), and Daniels N, Byant J, Castano R et al: Benchmarks of fairness for
3
and c) to acknowledge if cultural/linguistic bonds will help to introduce thismethodology of analysis in developing countries with a particular tradition (Portuguesespeaking countries).
CHART IHEALTH PROTECTION
PROCEDURAL JUSTICE
LIBERTARIANISM
UTILITARIANISM
IGUALITARIANISM
health care reform: a policy tool for developing countries. Bulletin of the World Health Organization 78(6); 740-750, 2000.
ACCOUNTABILITY
AUTO-DETERMINATION
COST CONTAINMENT
EQUAL OPPORTUNITIES
PRIORITIES

4
2- THE PORTUGUESE NATIONAL HEALTH SYSTEM
PORTUGUESE HEALTH SYSTEM (PHS) (it represents 8,6% of Gross Domestic Product -GDP) has two main components12:
• The NATIONAL HEALTH SERVICE (NHS), universally accessible, and publiclyfinanced through the social solidarity (taxes) of citizens (Table I). The publicexpenditure in healthcare (60% of the overall health budget) is processed directlyfrom the Global Budget.
• SUBSYSTEMS (SS) and PRIVATE PRACTICE (PP), (including commercial insuranceschemes and out-of-pocket payments), that accounts for 40% of the overall healthbudget.
Like in most European Countries13 the Portuguese government has a direct interventionin the structures rendering healthcare services. Moreover, it is instrumental in theplanning, regulation and evaluation of the system. Portuguese Health System pretendsto be a global model of rationalised care, centred on the General Practitioner (FamilyDoctor), as an attending physician, placing high emphasis on early intervention andguaranteeing the integration and continuity of care. A policy of incentives is in practice(but not yet fully implemented) that might stimulate practitioners’ productivity.
TABLE I
Resources (1997) Absolute Number Habitants perprofessional
Population 9.957.000Physicians 30.431 327Nurses 37.881 263Dentists 1.904 5.230Pharmacists 7.334 1.358General Hospitals 83Specialised Hospitals 12Pedia t r ic & MentalInstitutions
34
Private Hospitals 92Health Centres 386Pharmacies 2.539Consultations (1000) 32.777,9Emergencies (1000) 12.003,6
12 Ministry of Health: Saúde um Compromisso – “A Estratégia de Saúde para o Virar do Século (1998-2002)”.13 European health care reform, analysis of current strategies. World Health Organization, RegionalOffice for Europe, Copenhagen, 1997. See also, Report by the Government Committee on Choices inHealth Care, Ministry of Welfare, Health and Cultural Affairs, The Netherlands, 1992.
5
The country is divided in five different administrative areas. Each one of them haspartial independence with regards the central administration. Efficiency in themanagement of health resources implied, in the past, that conditions of transparency andaccountability were created that might encourage effective competition among publicand private institutions specially with regards secondary care in hospitals. Thegovernment is now implementing adequate alternatives – from a technical and humanepoint of view – for the caring of chronic patients namely elderly people.
The National Health Service has three different functions (Chart II): a) a strategy forinvestment in healthcare, b) the financing of healthcare services, and c) the delivery ofhealthcare14. All of them try to guarantee the tools for promoting efficiency inhealthcare. Also, the NHS recognises the fundamental role of social solidarityorganisations and also of the private sector. Future guidelines will try to promote a cleardistinction between the financing and the delivery components of the system stimulatingan accountability policy15. The NHS has also the task of regulating competition and ofpromoting the co-operation between different healthcare agents so that quality inhealthcare is obtained at the lowest possible cost16. Finally, it contributes to regulate themarket in healthcare both at the service and technology levels.
The State, trough government agencies, has also a fundamental role in controlling thepharmaceutical industry. The public policy on pharmaceuticals is a controversial issue.It is well known the fact that attitudes towards the pharmaceutical industry reflectpayer’s views on the benefits over pharmaceutical research and development. EuropeanUnion trademarks legislation regarding medicines, in particular brands and copyright,are usually seen as an extension of property as well as a patenting rights of innovativeproducts and inventions. However, the control of the expenses with pharmaceuticals iscrucial as Portugal has one of the highest per capita expenditures with these products inthe European Union.
14 Council for Reflection on Health: Recommendations for structural reform (Ministerial CabinetResolution no. 13/96, of January 24th – President: Daniel Serrão), Oporto, 1998.15 Tribunal de Contas: Auditoria ao Serviço Nacional de Saúde. Relatório Final. Lisboa, 1999.16 Wikler D, Marchand S: Macro-allocation: dividing the health care budget. A Companion to Bioethics,Blackwell Companions to Philosophy, Helga Kuhse and Peter Singer (Editors), Blackwell Publishers,Oxford, 1998.

6
CHART II
FINANCING MODEL – FINANCIAL FLOW CHART
CITIZENS______________________________________________________________________________
4 1 2 3 5
FUNDS
HEALTHCARE PUBLIC PRIVATEDELIVERY_________________________________________________________________________
Notes:1 and 2 – INCOME-BASED FLOW 1- IT REPRESENTS +/- 60% OF THE
OVERALL HEALTHCARE EXPENDITURES3 – RISK- BASED FLOW 2,3,4,5 - IT REPRESENTS +/- 40% OF THE OVERALL HEALTHCARE EXPENDITURES4 and 5 – UTILISATION-BASED FLOW
1 - COMPULSORY AND UNIVERSAL BASIS 2,3,4,5 - SELECTIVE BASIS
2 - IT BECOMES COMPULSORY 3 - VOLUNTARY BASIS
INSURANCE MECHANISMS
GLOBALBUDGET(IMPLICITINSURANCE)
SUB-SYSTEMS
COMERCIALINSURANCE
DIRECTPAYMENT
DIRECTPAYMENT
7
3- CONSIDERING THE REFORM PROPOSALS: THE NOVEMBER 2000 WORKSHOP
With the purpose of introducing the policy tool “Benchmarks of Fairness for HealthCare Reform”17 in our country a 3 day workshop was held at Oporto in November 2000.This workshop had 2 different objectives. First, to acknowledge its importance as anobjective tool for evaluating the Health Care System and the proposals of reform.Second to understand clearly its practicability. That is, how to apply the instrument.Different participants were present at the meeting. The authors of this study invitedinfluent people, namely a representative from the Ministry of Health, a hospital manager(from on of the largest – 600 bed – Portuguese hospitals), a past Treasure Secretary ofState, and the President of the Council for Reflection on Health, a Commission thatproposed the document “Recommendations for Structural Reform”.
At the workshop an historical perspective of Portuguese health care system was drawn.It was stated that prior to 1974 – the Portuguese revolution, and the transition todemocracy – Portugal had a laminated system, with rich people buying services out ofpocket, social security system for industrial workers and a large group of rural workersthat had no protection at all. There were two kinds of hospitals: government hospitals(included medical schools) with internships for specialities (the main problem wasgovernance because of conflict between professors in medical schools and the otherprofessionals), and old charitable hospitals (private). However, back in the 1940s thegovernment planned to build new hospitals in each district (now these hospitals aremore or less built all over country). So poor people had no security, rich people paid forprivate services, and salary workers went to social security (prior to the revolution). Inthe 1950s the Ministry of Health (MOH) began to get more power to control services tobeneficiaries. By 1974 poor had no real health service, and this changed after therevolution. All people got rights to go to hospital – affected some 60-70 percent ofpopulation.
The Portuguese Constitution of 1975 gives right to health protection through the NHS,and the Service must give general and free health care for all18. In 1978 the Parliamentpassed the Law on National Health Service (NHS): all Portuguese have right to go tothe NHS. But slight changes were introduced, namely that the principle that the NHSshould be general and universal. The service must have in consideration the economicsituation of citizens and must be free for those who need it. But, nevertheless, the Lawon National Health Service put some emphasis on the economic restrictions of thesystem and the limits on the right to health care access.
17 Daniels, N., Light, D., Caplan, R.: “Benchmarks of Fairness for Health Care Reform”. OxfordUniversity Press, New York, 1996.18 In Portugal, according to article 64 of the Constitution of the Portuguese republic everyone has the rightto have her or his health safeguarded and the duty to defend and foster it. This right shall be met, namely,by the creation of a National Health Service available to all people, and free of charge to the extent thatthe economic and social conditions of citizens require. In order to ensure the right to safeguarding ofhealth, the state has a primary duty, according to the referred article, to: a) guarantee the access of allcitizens, regardless of their economic circumstances, to both preventive and curative care; b) guarantee arational and efficient coverage of human resources and units through the whole country; c) provide thecosts of medical care and medicines from public funds; d) regulate and supervise privately fundedmedical practice co-ordinating it with the National Health Service to ensure that adequate standards ofefficiency and quality are achieved in public and private institutions.
8
Paradoxically, a period of economic recession – between 1974-1990 – was associated tohealth improvement. Probably, social determinants had more effect than the healthsystem did. Also, a million people returned from colonies (Angola, Mozambique,Guinea-Bissau), typically a younger population, and better off people than domesticpopulation. By 1980s Portugal had also a specific program on maternal and infant care,an intervention to improve hospital and health center treatment of women and children.Fifteen years led to great reduction in maternal mortality and infant mortality, soPortugal is now in the middle of European range. Are good results products of socialchange or intervention in the system? Better income of worse of parts of populationmeans they can seek and pay for services. Also a significant reduction of birth rateplayed a prominent role.
After 1979, a big debate was held among Portuguese society about co-payment and theamount paid by rich people. Social Democrats19 want rich people to pay services withinthe NHS, but socialists want services free for all. It is claimed that paying for services atthe NHS will lead to a shift of rich people to the private sector (managed care/insuranceor out of pocket). In the NHS, co-payments are a tool for rationalizing the System, notfor funding it. Plus tax system is itself fairly progressive. Poor and elderly pay no taxesand use services more, so co-payments do not work as expected to rationaliseutilization. Gross Domestic Product (GDP) since 1995 is over medium of Europe, butthe health care expenditure is now about 8,6% of the GDP (5,16% public and 3,44%private sector), over the medium of Europe (8,2%). So, reliance on private sector issignificant and a lot of trust in private practitioners and institutions is usual. Theconclusion is that, despite the efforts, Portugal still has a laminated system.
To achieve the goal of universality in coverage, the country is decentralized into fiveregions, but there is no decentralization of the rest of the government, so – in practice –it is not working. Also regional leaders are really appointed by the Ministry of Health.Further, as the Ministry of Health centralises financing and regulation, no real authorityfor contracting exists except as determined by central Ministry. Although health centershave 80% of the outpatient situation, devoted mainly to primary care delivery (althoughsome preventive care and community assistance is also a statutory obligation), hospitalshave larger budget and have political priority. The real issue is very high investmentlevels in hospitals but low investment in health centers.
It is nationality, not residence, that determines eligibility (unlike Britain). Nevertheless,there are in Portugal – for the time being – some 300.000 emigrants from Africa andcentral Europe (Ukraine, Croatia, Romania, etc.). Although not eligible, none of theseforeign citizens will be denied access to the public service. As most of them are notregistered, and are concentrated at the urban area of Lisbon, it represents a seriousproblem for the planning of services within the NHS.
The 1995 law entitles all citizens to health care services, but civil servants and manypeople working at particular areas of Portuguese economy, have specific entitlements(subsystems). These workers have access to different systems subsidised by a specifictax (1% for Civil Service workers) plus co-payments. Over a total of 10 million citizens,3 million have access to an extra health care subsystem. This policy implies the idea 19 In Portugal the two most important political forces are the Social Democrats and the Socialists. Theyhave been alternating in the government since the 1974 revolution.
9
that even the government doesn’t fully trust the NHS to give adequate treatment to CivilService workers. Many subsystems focus on special groups of workers, eg bankworkers, or military personnel. If these workers go to the NHS, they pay nothingthemselves, but the NHS bills special fund for the subsystems involved. It is claimedthat the Ministry of Health depends on this extra funding. Also, at least 1 million peoplehave a private insurance scheme (managed care).
In this social, economical and political background the Portuguese governmentinstituted in January 24th 1996, in its Ministerial Cabinet Resolution no. 13/96, theCouncil for Reflection on Health (President: Daniel Serrão). This council had sevenparticipants: two doctors, one lawyer, one economist, one hospital manager (Presidentof the Hospital Managers Association), one nurse (President of the Nurses Council). Itwas approved by the government and set up as an independent council. Results of thereport are public. No real public discussion of the document was achieved, thoughwidely distributed after a presentation with press conference at the end of 1998.
At a meeting with Parliamentary Commission on Health, including all parties, it wasacknowledged that only one deputy had actually read the document (from theCommunist Party) and another from the Social Democrat Party (who had been Ministerof Health). Most of the other members of this commission had not a deep understandingof the document. Communists said no threats are permitted to the NHS and SocialDemocrats said no threats to the doctors independent status (freedom of prescription,among others) are allowed. Afterwards, the meeting was adjourned but the second partnever happened.
The proposal was very clear in the acceptance of the principle that a structural reformon health is a common endeavour of all society and that agreement on all parties isneeded. A regime pact was therefore proposed between all political forces. Oppositionparties said they would agree, but the government party (socialist at that time) claimedthat they were elected to produce specific health reform goals. Therefore, no real publicdiscussion took place, perhaps because being an election year (1999), nothing would bedone till after elections. After the elections the socialist party had again the majority atthe parliament. The new Minister of Health (1999) – who was a financial specialist –was likely to address problems of budget. So the role of the Council for Reflection onHealth largely ended. Central proposal was a new organization model – and also tomake doctors available at a national level – but instead the new Minister of Healthclaimed that the key issues were waiting lists for surgery, probably due to its politicalimpact.
It must be emphasised that this was perhaps the only consistent reform proposal of thehealth care system in Portugal. Nevertheless, many individual and institutionaldocuments are available for study. They are also considered in this evaluation.
Key elements of this proposal were never really implemented: eg public discussion.Also, the tax reform, the National Health Council, the compulsory Public InsuranceProgram (clearly separated form other taxes) and the Public Institute for Financing(autonomous), etc. were not set up. About 20 specific recommendations were proposedin this document. The central idea was to get government to withdraw fromorganization and delivery of health care. Instead, its task should be to do planning,regulation and evaluation of Portuguese health system (both private and public). To

10
accomplish this purpose a proper information system (Health Intranet) is needed toconnect all parts of the system, public and private, general practitioners and specialists.Keeping the patient’s record across Intranet would help this interconnection.
One of the proposals is slowly taking place: that is the implementation of new models ofadministration of public hospitals so that value for money is increased. Unlike theBritish solution PFI (Private Finance Initiative20) were clinical services are “sacred”, asolution that took place in Portugal since 1996 (just in one hospital out of 95 publichospitals) is the offering of private management of all services including clinicalassistance. Not ownership or finance, only management. Payment is per capita whererisk is on management to produce a more efficient use of public funds (in effect thissolution is managed care services contracted by the NHS). The proposal is to run for atleast 20% less than public hospitals do. The objective is to look for efficiency.
Now this administration is running at 34-40% less in cost. Also, there has been anincrease in productivity, but on the other hand the hospital must pay more for higherproduction (incentives to doctors to work harder, use protocols and rules about whatmust be prescribed). Some critics contend that doctors will loose professional autonomyand that in the end it is a profit company were efficiency (value for money) scoreshigher than equity in access. However, despite critics, the hospital with this newmanagement (Amadora/Sintra) was the first Portuguese hospital to obtain accreditationthrough the Kings Fund Health Quality Service (late 2001). Physicians are fixed bysalary and then have some marginal funds to provide merit pay. Physicians shouldexercise autonomy in prior determination by a panel on what counts as proper treatment,not solely in the treatment process. Clinical guidelines obtained by Evidence BasedMedicine (EBM) are central in this process. Clinical protocols are incrementally added.Physicians get share in savings from increased productivity, so have good incentives tobe economical in the use of consumables, etc. To address the issue of productivityversus over-utilization, it is crucial to provide incentives through protocols, but also it ispreviously determined – on a contractual basis – the amount of clinical productionexpected. Other putative benefits of this kind of administration are: low administrativecosts, clear lines of command (versus public hospitals where lines of command areunclear) and shortening of hospital staying (outpatient diagnostic/therapeutic versusinpatient, etc.).
However, there are still some problems to resolve. First, many physicians and nursesbelong to NHS and by political pressure must remain so (Civil Service workers). But asthere is a shortage of professionals, many foreign nurses (Spanish) who do not belongto the NHS are working at the hospital. Also, with regards the Emergency Service,many people use it as first access to the system, and this a serious problem in theplanning of health care delivery. For the moment, academic studies by differentinstitutions are taking place – with clear benchmarking – to evaluate changes in deliveryof health care, in productivity and in access. Multiple experiments, in various regions,are important so that private management of public hospitals can be clearly evaluated.
20 In this perspective (PFI) the NHS is still responsible for the clinical services and a private financialgroup deals with every other aspect of the hospital organisation. Services are delivered on a contractualbasis with the NHS. Sussex, J.: “The economics of the private finance initiative in the NHS”. Office ofHealth Economics. London, 2001. Also, Smith, CA: “Making sense of the private finance initiative”.Radcliffe Medical Press, Oxford, 1999.
11
But it is not only the model hospital administration that is at stake. The organization ofthe system must also be addressed in the future. In the current system, people aresupposed to have unrestricted access to his/her general practitioner (GP). But, for manyhistorical and cultural reasons, GPs work at an institutional level – the health center. Itmeans not only that the individual nature of the patient/physician relation is lost but alsothat there is a bad articulation and co-ordination with specialists at an hospital level. Itmeant in the last decade a bad GP/specilist ratio with too few GPs in the country. Thefact that GPs are considered as civil servants has contributed to low level primary care.
That is no formal referral mechanisms to hospital care do exist: people can go to GPs orhospitals as they wish. Ideally citizens would go to family practice doctor who thenwould refer patient to health center, to hospital, to rehabilitation, or to hospice services(gatekeeper/signpost). Reform could allow some choice among groups of familypractitioners (GPs) as a compensation for losing option of going to hospital. This wouldnot only increase choice (patient and provider autonomy) but also efficiency.
The reform proposal is that private doctors (GPs) should work in small groups whocontract with the NHS, and should have a panel of patients under capitated arrangement.This model – as in the Danish system – with proper informatics is probably moreefficient and more quality is added to the system. A pitfall of the current system is thatsalaried health center based GPs chase away patients from the NHS but then do privatepractice, with regular patients mainly form the NHS. At a clinical level, again, EBMguidelines, as in Finland, should be developed with three levels of evidence – strongevidence, good reason to accept, and standardly done but not evidence – so that doctorscan choose the best available option to a particular patient.
With regards accountability, there is very little malpractice litigation; however, in thelast couple of years it has blown up in media. A proposal to circumvent this problem isto compensate injured patients (with or without guilt from the physician/institution) inproportion to the injury. This is the “compensation without fault” system that is in placein Nordic countries rather than the US litigation system. In Portugal, where fault maytake 3-4 years to demonstrate (without reasonable doubt), at the end, in general, judgescannot decide properly due to the absence of proof. Liability insurance does not work ifit is not possible to prove fault.
4- REVIEW OF THE REFORM
DISCUSSION OF BENCHMARK 1:
What to do about the fact that many elements of B1 are not in proposals but areaddressed by other reform efforts going on elsewhere? Suggestion was to give zeroscore but then note that these other programs exist and should be connected. Namely thereform proposal of the Ministry of Health itself 21. The point of the Benchmark 1 is tochange the way of thinking about separation of sectors. If reform is not scored down foromitting discussion, then there is no change of highlighting the importance ofintersectoral effort as part of reform. It turns out, however, that many of the items under
21 Ministry of Health: Saúde um Compromisso – “A Estratégia de Saúde para o Virar do Século (1998-2002)”.

12
the first subhead of B1 are addressed in the reforms. Nothing however on subheads 2and 3.
It must be emphasised that in the last couple of years the problem of intersectoral publichealth is acknowledged as an important part of the reform. Namely the connectionbetween the Ministries of Health, Environment, Transports, Communication, Educationand Science and Technology to deal with issues truly intersectoral. Particularly withregards B1 II and III.
DISCUSSION OF BENCHMARK 2:
In theory there are no financial barriers in the access to the basic package of health care.However, due to a deficient organization of the system there are, in fact, financialbarriers, that can be indirectly assessed by the percentage of private practice (40%versus 60% public). Supposing that tiering is fair if it does not compromise the basicpackage (politically or economically) the problem in Portugal is that tiering is a sub-product of the inefficacy of the system. To overcome financial barriers the problem ofefficacy/efficiency must be addressed.
Eventually the proposal to set up an Independent Entity to channel public funds withoutactually doing health care delivery (as now is the case in Ministry of Health), couldsolve the problem. This entity, that has public money, then would contract with bothpublic and private entities to deliver care. It allows tiering through insurance policies. Inthe meanwhile it is also expected that private insurance will grow, reducing direct out ofpocket payment to health care. It is expected that private insurance will only be 15–20%of the system. It might be more if reform does not take place. Much of the growth inprivate insurance will be group insurance through employers, but some will be on anindividual basis.
Within these restrictions, there is no problem of access to the public service by theinformal sector (300.000 citizens/emigrants).
DISCUSSION OF BENCHMARK 3:
Geographical maldistribution of human and technological resources is an importantproblem in Portugal (as well as in many other European Countries). From a distributivejustice approach we prefer the expression SPATIAL INEQUITY if the maldistribution isunfair. Important measures are proposed in the reform proposals namely thatgeographical financing of health care should be on a needs based budgeting (nothistorical) in accordance with the criteria “capitation adjusted to age, disease pattern,proximity form hospital or health center and level of economical development”.
Gender and cultural disparities are not important issues in Portugal. Discrimination onlyrarely occurs (specially to gypsies) in health care access although there is some mistrustwith regards gypsies and Africans.
13
DISCUSSION OF BENCHMARK 4:
For the time being “all effective and needed services deemed affordable, by all neededproviders” are only theoretically accessible. Long queues mean in effect that manyimportant services are unavailable. Combining access to some private facilities withinbudget accessible to NHS users will reduce tiering. Increasing insurance sector willsomewhat increase it prior to any reform. As previously stated tiering is mainly due tothe inefficacy of the NHS in fulfilling its obligations. It is claimed by some sectors ofsociety (more liberal) that, within certain limits, tiering can indirectly increase theefficiency of the NHS because of the shifting of many patients to private insurers. Thiswould lead to some decompression of the public system and increase value for money.
DISCUSSION OF BENCHMARK 5:
The NHS is largely financed by progressive taxation. Although there is room to make itmore progressive, for the time being – and bearing in mind that the level of earning ofPortuguese people is much lower than the average European (1/2) – it is unrealistic toassume that progressivity can increase further. Pulling many private payers intoinsurance will increase equity in financing. But, again, it needs to be carefully assessedbecause if many patients go out of the NHS to the private sector this could mean someloss of solidarity in financing the global system. As the NHS is tax funded, a commonfeeling is that justice in health care means also justice in the fiscal system. Tax evasionis observed as one of the most important social problems in Portugal. Important reformsare also in course in this area.
DISCUSSION OF BENCHMARK 6:
Some emphasis in the reform proposal is put on the GP as the gatekeeper. For the timebeing there is no true choice of GP and there is also no real training for communitybased delivery. The adequacy of incentives is not clear, but this is one of the mostimportant issues of any future proposal. Little emphasis also on communityparticipation. There is a clear attention to referral mechanisms in all proposals, but notnecessarily related to the principle of respect for autonomy.
Evidence-based practice and quality are emerging problems is Portugal. There isgrowing awareness that this concepts are not only management tools but also importantethical imperatives. Accreditation of hospitals and certification (ISO, SA 8000) of otherhealth care facilities is in course. Although there is little emphasis on the regularassessment of quality in reform proposals it is now a major topic of public discussion.
Quality in healthcare has different levels of intervention: a) general practice (primarycare), b) laboratories, and c) quality control of pharmaceuticals. Also, to assure qualityand efficiency the entire Portuguese Health System is to be processed into computerdata bases and made into a national network – Intranet – which interconnect all theagents involved.
Evidence-Based Medicine is now an accepted practice in our country. For several yearsnow Schools of Medicine have implemented in the pre and post-graduation courses this
14
concept both with regards the evaluation of the effectiveness of drugs and theintroduction of new technologies. As an example, specific disciplines of quality inhealthcare and Evidence-Based Medicine have been implemented. It is regarded as anacademic movement following the accepted standard of scientific methodology namelythe need to share information.
DISCUSSION OF BENCHMARK 7:
There are many problems about technology acquisition, and to its fair distribution allover the country. There is no mention of this issue in reform proposals. Marketing costsmay grow with private sector growth. Problems of multiple oversupply of sometechnologies do exist and it is not foreseeable in the future a true interest in rationalizeits use and distribution.
Cost shifting reductions are built into proposal to regulate referral and limit directaccess to hospitals. There are some abuse and fraud issues, but not obviously addressedby reforms. Nevertheless, there is the common feeling that a new organization model ofthe NHS – increasing responsibility and accountability, and also emphasising incentives– will help dealing with this situation. Increasing the efficacy and efficiency of thesystem is linked, inevitably, to decreased benefits of the Civil Service. Probably thecontractual basis of health care professionals will evolve from collective (Civil Service)to individual – based on productivity with careful assessment of the performance.
Drug purchasing is negotiated between the Ministry of health and the industry. The rateof public subsidy – a form of large purchasing, but not really price regulation – iscurrently under debate. Also, generics are increasingly accepted by the medicalprofession and by the public22. The acceptance of generic medicines by the medicalprofession and by the general population seems to be crucial for the control of theoverall healthcare expenditure.
DISCUSSION OF BENCHMARK 8:
Performance reports are not regularly used, and there is no mention of its necessity inproposals. Also, no provision for accountability for reasonableness in difficultdecisions. Some reasons, and some public discussion, was put forward with regardssetting up funding that would contract with private sector as well. There is someimprovement in the global budget accountability namely with regards the discussion atthe Parliament of the reasons for a specific health care budget.
Physicians, as well as other health professionals, are very well organized into unions,and professional orders (medical council). Unions have mainly economic and careerpurposes. As far as accountability is concerned there is some public mistrust withregards conflict of interest in pharmaceuticals’ prescription. The EU Directive
22 These authors have stated that as long as freedom of prescription is generally accepted as the standardfor clinical practice, medical ethics should acknowledge the fact that resources are scarce and the use ofgenetic drugs might increase efficiency (value for money) and therefore can be considered as an ethicalimperative, as long as the best interest of the patient is not at stake. Rego, G., Nunes, R., Brandão, C.: “Omercado dos medicamentos: Concorrência e intervenção”. X Jornadas Luso-Espanholas de GestãoCientífica, Actas, Vilamoura, 2000.

15
92/28CEE is very clear with regards these issues. In particular, issues like theacceptance of gifts, loans, or hospitality are usually considered as unethical due to themoral risk involved23. Legal procedures are increasingly dealing with this issue. Just afew days ago four doctors were criminally held accountable (passive corruption) foraccepting illegal and unethical gifts from the industry.
Non-legal grievance procedures are not discussed in proposals. But, privacy protectionis widely discussed in Portugal (both in the reform proposal as in the media) andpatients frequently complain about lack of professional confidentiality. Althoughregarded as a right, access to medical records is not unlimited. Patients have no clearright to see the chart, although EU directives guarantees the right to access to personaldata. Portuguese lawyers do not interpret this as right to see the chart, rather as a right towrite and get the information contained.
Some development of advocacy groups intervention in public policy, eg disabled, HIVpatients, prisoners, has occurred. There is not a strong women’s health movementprobably because reproductive health has been usually one of the most important healthissues. Cancer advocacy groups have been a partner for a long time now. Stimulatingpublic debate is not high on current political agenda.
DISCUSSION OF BENCHMARK 9:
The reform proposals usually agree that there should be no assignment of people toPrimary Care providers (GPs) but rather people should have the right to choose. It isalso a common complaint of most citizens the fact that the family doctor isadministratively assigned. In the NHS now there is little or no autonomy in choice.Patient is assigned to doctor both at the hospital as at primary care. On coming to aparticular NHS facility for treatment, the physician is assigned permanently. If a secondopinion is needed, recent proposals, and its implementation, guarantee this right. Thereis a governmental chart of patient’s rights that acknowledges this possibility24. Referralby the GP to a speciality is to a specific hospital, but not to a specific doctor.Administratively the person is assigned to particular specialist. Proposals do not solvethis problem. There is some limits put on the degree of choice. Probably, in the future, itwill be possible also to choose the specialist but always after referral by primary caredoctor. Alternative providers are not in system, so there is no current choice.
In private practice, patients get full choice of specialist only in a few subsystems and inout of pocket payments. More and more Managed Care limits the choice of specialist.Current NHS loses out on content of deepening the relationship between patient andphysician because assigned patients are not the ones to whom doctors feel as close or asmuch responsibility.
23 Only in specific circumstances might it be proper for doctors to accept “a grant which enables him totravel to an international conference or to acceptance, by a group of doctors who attend sponsoredpostgraduate meeting or conference, of hospitality at an appropriate level, which the recipients mightnormally adopt paying for themselves”. See (British Medical Association, 1993). British MedicalAssociation Medical Ethics Today: Its Practice and Philosophy. BMJ Publishing Group, London, 1993.24 Carta de Direitos e Deveres do Doente, Direcção-Geral da Saúde, Lisboa, 1998.

16
As stated previously, physician autonomy is wide. Medical Council wants fullindependence of physicians to write prescriptions, exams, access to diagnostics. Moreand more in the NHS and in private insurance, there is some compromise of autonomy.In practice, when a hospital has a true management policy it will inevitably lead todiminished professional autonomy. Public sector contracting with these hospitals willencounter restrictions on autonomy.
So reform proposals might lead to negative scores on physicians autonomy. But it mustbe emphasised that in Portugal physicians have almost unrestricted autonomy, and eveninformed consent policies are only recently been accepted as a fundamental issues inmedical ethics. Gradually more doctors inform patients about options and give themsome opportunity to choose between medical options. Some doctors are less oriented toinformed consent, especially surgeons in private practice. Reports push for good ethicalstandards on informed consent, but do not specifically say how this will be achieved.Best practical way is to get a second opinion right.
5- SCORING (ANNEX)
In this study it will be used the original methodology for scoring the benchmarks(USA). The scoring system takes the status quo as a “0”, assigns a maximal positiveoutcome a “5” and a maximal regression from the status quo as a “-5”. As Danielspoints out “it remains clear that these (numbers) reflect the ordinal rankings on complexdimensions, not cardinal measures of some quantity. The purpose of actually assigningscores for each criterion is to force deliberation about the specific, interacting effects ofthe reforms being compared”. In this vein the rationale that explains the score in aparticular benchmark is probably more important than the score itself.
6- CONCLUSION
It is commonly accepted that a right to health care protection, or at least to health careaccess, is a social right in most pluralistic societies25. At an European level guidelinesregarding healthcare delivery do exist, namely the Convention for the Protection ofHuman Rights and Dignity of the Human Being with Regard to the Application ofBiology and Medicine26 claiming for a universal right to healthcare delivery – taking inconsideration the financial restrictions of the system – promotes this point of view.However, some authorities, such as H. Tristram Engelhardt Jr., claim that natural andsocial lotteries are “the result of natural forces, not the actions of persons” and also thatit may “very well be unfeeling or unsympathetic not to provide such help but it isanother thing to show that one owes others such help in a way that would morallyauthorise state force to redistribute resources“. This author also states that “a basichuman right to the delivery of healthcare even to the delivery of a decent minimum ofhealthcare does not exist”27.
25 Daniels, N., “Just Health Care. Studies in Philosophy and Health Policy”, Cambridge University Press,New York, (1985)26 Convention of the Protection of Human Rights and Dignity of the Human Being with Regard to theApplication of Biology and Medicine. Council of Europe, Strasbourg, November, 1996.27 Engelhardt, H., “The Foundations of Bioethics”, Oxford University Press, New York, (1986).

17
In this context the assessment of fairness in health care must take into considerationdifferent perspectives of distributive justice, namely equality of opportunity, autonomyand freedom of choice as well as utilitarian values. Specially when all countries face theissue of shortage of resources. In fact, the increasing costs to health care – mainly due toscientific/technologic development, increasing age of the population and consumerism –make it an ethical imperative as well as an economic one, to establish priorities inhealthcare delivery and access.
These authors believe that the “Benchmarks of Fairness for Health Care Reform” is auseful tool not only to assess the fairness of reform proposals in developing countriesbut also in developed countries with a long standing experience of health care delivery.Namely in European Union countries where for many different reasons there are unjustcircumstances in the financing, access and degree of choice of consumers.
With regards Portuguese reform proposals, it must be noted that although the per capitaGNP of this European Union country is 1/3 of the American one, many health indicesscore higher in Portugal than at the USA. Probably due to the fact that a public service(NHS) does exist, that protects the health of all citizens, and also due to a decrease ofeconomic and social disparities between well and worse off segments of the population.Nevertheless, some important aspects of fairness are still at stake, namely waiting timesto surgery and access to GPs and hospital care within reasonable period of time. Alsoeconomical efficiency (value for money) must be increased so that scarce resources canbe used to increase access to a reasonable level of health care. The next step willprobably be the implementation of a true democratic accountability process and alsosome degree of empowerment of citizens and groups of citizens (like the disabled).
Also it will be possible to expand this evaluation to developing countries where (the)special cultural and linguistic connections will make it easier to evaluate proposals aswell as implement the reform. As could be the case with the (as a possible) expansion ofthis study to Angola, Mozambique, Guinea-Bissau, and even Brazil.