preliminary experimentation with specific immunotherapy of neoplastic disease in man. i. immediate...
TRANSCRIPT

PRELIMINARY EXPERIMENTATION WITH SPECIFIC IhlMUNOTHERA4PY OF NEOPLASTIC DISEASE IN MAN
I . Immediate Eflects of Hyperimmune Equine Gamma Globulins SERCIO DE CARVALIIO, M.D.
ROlEIN ANTIGENS FROM HUMAN TISSUES, P both normal and neoplastic, were extracted by the fluorocarbon method described earlier.* With the proteins from normal tissues im- mune antinormal gamma globulins were pro- duced in horses. These antinormal gamma globulin antibodies were used to absorb nor- mal components from the fluorocarbon ex- tracts of neoplastic tissues.* Antibodies and antiserums against malignant cells have here- tofore been obtained by absorption of anti- body mixtures with antigens from normal org;ins or plasma.3 Absorption of antigen mix- tures by antinormal antibodies used here first and the dissociation of proteins, undenatured, from nucleic acids by fluorocarbonR, 9 represent the developments that made these proteins available for serological analysis and specific iniinuni za t ion. Tumor-speci fie antigens left after this absorption were used to imniunize other horses. Hyperimmune gamma globulins from these animals were used as experimental therapeutic agents in leukemia and other cancers. Some of the in vitro and early in vivo properties of these preparations, includ- ing immediate, short-term, clinical effects are described here.
This methodology was applied by us0 and o t h c r s ~ ~ ~ 24 on some animal cancer models. The results obtained helped to form the basis for a preliminary clinical trial. Much more can and must be done with animal models. For example, fluorocarbon extraction of X
From the Department of Hematology, Doctors Hos- pital, Cleveland, Ohio, and the Cancer Research Lab- oratory, Rand Development Corporation, 13600 Deise Ave., Clevclanrl 10, Ohio.
Normal and neoplastic tissi~c.~ were obtained through the courtesy of Dr. Richard Rtnner, Doctors Hospital, Cleveland, Ohio; Dr. George Crile, Jr., Cleveland Clinic, Cleveland, Ohio; Dr. E. von Haam, Ohio Statc Uni- versity School of Medicine, Columbus, Ohio; and Dr. Harold Carlson, Detroit, Mi&.
It is impossible to make complete mention of all colleagues in this country and abroad who so under- standingly contributed clinical material for these studies and the specialists who helped with their skills toward the evaluation of different I-linical aspccts of each patient.
Rereivcd for publication May 2, 1962.
antigens in the mouse followed by precipita- tion of H2 antigens by anti-HZ isologous or heterologous antibodies. Given the widespread finding of X antigens in murine leukemias and lymphomas of varied etiology and age,15 this situation may present features in parallel with human leukemia. Induction of immunity and tolerance12 with the clean leukcinic anti- gens will be most desirable.
This is not the place for a formal discussion of the rationale of immunotherapy of cancer. Several recent reviews203 21 deal with the sub- ject. In one of these,20 ihe reviewer, quite foreseeingly, calls for the following requisites. “Passive immunization calls for the production of antibody to cancer antigcns in a recipient (the serum donor) other than the cancer pa- tient, with subsequent administration to the patient o f the antiserum so produced. T h e production problems in such an approach are many. In theory, the best approach would be the production of a tailor-made antiserum for earh patient. The alternative is a multivalent antiserum produced against mixed antigens from many different tumors. By either method, the serum would contain antibodies to normal tissues as well as the desired anticancei anti- bodies, unless i t were possible to isolate the cancer antigen before immunization of the serum donor or to selectively remove the antinormal antibodies before administration of the antiserum to the patient. The tremen- dous mass of cancer tissue which an adniinis- tered antibody would have to affect in the patient with advanced cancer is also a point of great discouragement, but this objection would not be pertinent if serum treatment could be used in an early stage of cancer, as would be logical if an effective agent were available. T h e serum donor would presum- ably be an animal, such as horse, sheep, or rabbit, and thus the patient’s treatment would be limited by sensitization to the heterologous serum protein.” These requisiles were all met here and even beyond. Instead of whole ani- mal serum, purified gamma globulin fractions were used, thus greatly minimizing or elimi-
306
No. 3 IMMLJNOTHERAPY OF NEOPLASTIC DISEASE I N MAN. I. - de Cal-valho 307
nating the risk of serum reactions borne by the serum fractions not related to precipitat- ing antibody.1
It must be emphasized that the results here given do not represent, nor are intended to represent, a definite evaluation of the clinical value of the preparation. Such evaluation may require highly organized study plans, includ- ing standardization of the preparations, homo- geneous cancer patient groups, double-blind and double-check studies by several study groups and time. The clinical methodology of evaluation used in experimental chemo- therapy ought to be applied to immunother- aPY.
The immediate results of this preliminary study are here presented as a first probe of the method to open the way to a first-stage evaluation by other investigators.
The following concluding remarks regard- ing the future of cancer chemotherapy16 apply here with great propriety: “. . . preliminary experience of drug therapy in patients with advanced disease and a minimal number of surgical patients with noncurable lesions con- stitutes a sufficient trial for use of the drug in curable patients.” Regardless of the length of remission “. , . compounds which produce marked but temporary remissions may be very effective when used as adjuvants but may be valueless for palliative therapy.”
MATERIALS AND METHODS
The following human tissues obtained at operation or autopsy with histological control were used in this study.
Normal Tissues. The normal tissues con- sisted of liver, kidney, thyroid, striated mus- cle, pancreas, ileum, spleen, leukocytes, uterus, bone marrow, stomach, and brain.
Tumors. The tumor tissues used in the study were from melanoma, spindle cell sar- coma, mediastinal sarcoma, thymoma, fibrosar- coma, carcinosarcoma, dysembryoma, and as- trocytoma (brain), and from carcinomas of bladder, lung, rectum, neck, colon, breast, cardia, stomach, Fallopian tubes, kidneys, cer- vix, prostate, ileum, cecum, ovary, thyroid, pancreas, uterus, and salivary glands. Also included were leukemic spleens from children and adults with a variety of acute leukemias and lymph nodes from patients with lympho- blastic lymphosarcoma. No material from pa- tients with chronic lymphatic or myeloid leukemia was included.
NORMAL “COCKTAIL”
i 1
FLUOROCARBON EXTRACTION
NORMAL ANTIGENS
1 TUMOR OR LEUKEMIC “COCKTAIL‘ IMMUNIZATION OF A NORSE
I I 4
HORSE ANTI-NORMAL GAMMA GLOBULIN
1HNGGl
I
1 FLUOROCARBON
EXTRACTION
I L A0 SORPTION t
”MALIGNANT’ ANTIGENS * MIXTURE OF NORMAL AND
I 1 SUPERNATANT PRECIPITATE (DISCARDEOI (”MALIGNANT” ANTIGENS 1
I IMMUNIZATION OF
ANOTHER HORSE
1 HORSE ANTI-TUMOR (HTUGG) OR ANTI-LEUKEMIA (HLKGG)
GAMMA GLOBULIN
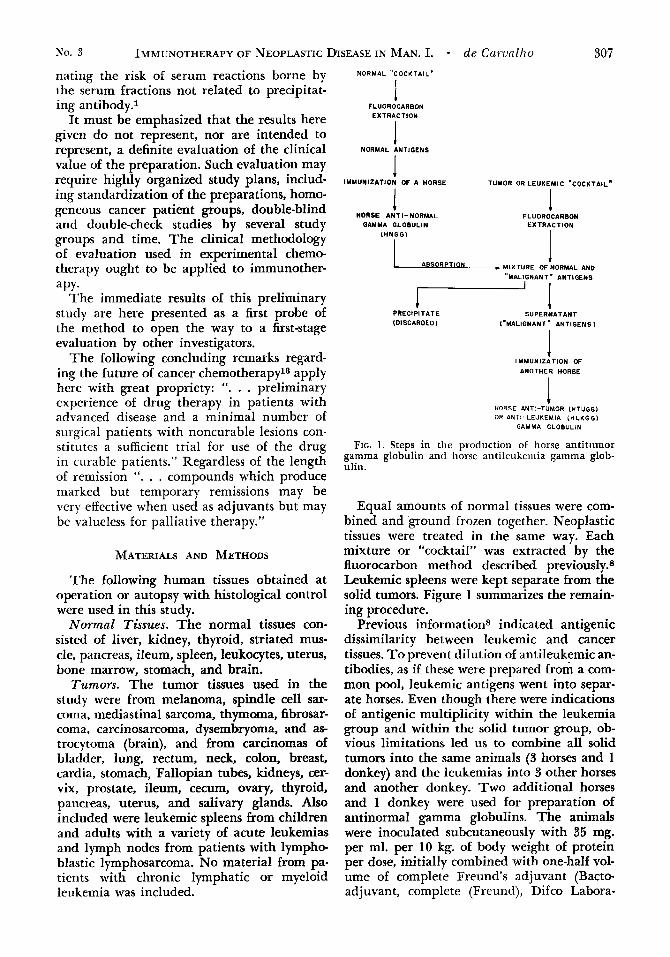
FIG. 1. Steps in the production of horse antitumor gamma globulin and horse antileukemia gamma glob- ulin.
Equal amounts of normal tissues were com- bined and ground frozen together. Neoplastic tissues were treated in the same way. Each mixture or “cocktail” was extracted by the fluorocarbon method described previously.8 Leukemic spleens were kept separate from the solid tumors. Figure 1 summarizes the remain- ing procedure.
Previous informations indicated antigenic dissimilarity between leukemic and cancer tissues. To prevent dilution of antileukemic an- tibodies, as if these were prepared from a com- mon pool, leukemic antigens went into separ- ate horses. Even though there were indications of antigenic multiplicity within the leukemia group and within the solid tumor group, ob- vious limitations led us to combine all solid tumors into the same animals (3 horses and 1 donkey) and the leukemias into 3 other horses and another donkey. Two additional horses and 1 donkey were used for preparation of antinormal gamma globulins. The animals were inoculated subcutaneously with 35 mg. per ml. per 10 kg. of body weight of protein per dose, initially combined with one-half vol- ume of complete Freund’s adjuvant (Bacto- adjuvant, complete (Freund), Difco Labora-

308 Vol. 16
PREl MMUNE
A
A
CANCER iMarch 1963
HYPERIMMUNE
A /1
5
HYPER1 MM UNE 6ALyYA GLOBULI
(16% SOLUTION)
C FIG. 2. Paper electrophoresis of horse serums. A, l'rcimmune serums; B, Hyperimmune scrums; C. Sixteen
per cent gainma globulin solution extracted hv cold ethanol as Cohn's Fraction I1 from the hyperimniune se- rums in Fig. 2B.
tories, Detroit, Mich.). Small samples of serum are tested weekly for antibody titration by a quantitative modification of the single gel- diffusion method11 and large samples har- vested when, with the aid of booster injections, an antibody ceiling is reached (titers up to
Electrophoresis of the hyperimmune serums showed that the globulins may become prac- tically all gamma globulin (Fig. 2B). Gamma globulin preparations of 95 to 100% purity (Fig. 2C) were separated from the hyperim- mune sera as Cohn's Fraction I1 by the Pentex Corporation of Kankakee, Ill. Solutions of 15 to 19% concentration of gamma globulins were placed in sterile vials and kept at -20" C.
These preparations were injected deep in- tramuscularly, avoiding entering the blood stream at 1- to 2-cc. doses daily initially, for as long as 45 days, and then spaced 1, 2, 3, 5 , 7, 15, or more days apart.
Leukemic patients have had at times, or continuously, concomitant corticosteroid ther- apy ranging from 4 to 64 mg. of methylpred- nisolone orally or parenterally daily. Few of the cancer patients received adjuvant therapy during the administration of immune gamma globulin.
Since the number of tumors included in the antigenic cocktails is limited, the efficacy of a given lot of immune gamma globulin was
2-6).
anticipated, to an extent, by in vitro testing the preparation against a sample of the tumor tissue or the leukemic cells. Two tests were used in this connection.
Immunocytolysis Tests. Washed nucleated cells from peripheral blood or bone marrow from leukemia patients and, occasionally, from fluids containing tumor cells were suspended at 100 cells per ml. in buffered saline, pH 7.2, at 37" C. Two-tenths of a aiilliliter of the cell suspension was mixed with 0.2 ml. serial logz dilutions of immune gamma globulins and with 0.4 ml. of a reconstituted lyophilized guinea pig complement preparation (Cappel Laboratories, Inc., West Chester, Pa.). After 4 minutes of incubation at room temperature, the unagglutinated cells were counted. The agglutinated and lysed cells have been studied in phase contrast.10
Gel-Diffusion Methods. The gel-diffusion methods used were the modification o f the Ouchterlony methodls by Korngoldlx (Fig. 3B) and our modification of the Oudin method13 (Fig. 3 4 . A fluorocarbon-extracted protein of the tumor sample was tested against dilutions of the immune gamma globulin. The end p i n t or titer is the last dilution that still shows precipitation in thc gel. When tumor material was not available for these tests, the immune gamma globulin was tried ex iuvantibus when a similar t.umor from another

No. 3 IMMUNOTHERAPY OF NEOPLASTIC DISEASE IN MAN. I. - de Carvalho 309
patient had been included in 1 of the tumor cocktails.
RESULTS
Immediate General Eflects of the Hyperim- mune Gamma Globulins on Leukemia and Tu- mor Patients. General effects common to both leukemia and tumor patients receiving either antileukemic or antitumor gamma globulins included local inflammatory reaction with erythema, moderate, occasionally severe pain, and localized urticariform rash. It is now known that procaine hydrochloride (Novocain) can be added to the gamma globulin. These ef- fects were quite variable from patient to pa- tient, were not constant, and were less fre- quent in tumor patients. They occurred 3 to 6 hours after the injection and subsided com- pletely in 24 hours. No generalized allergic, hypersensitivity, or anaphylactic phenomena were observed in our groups of patients. Ho,w- ever, 2 other workers6 using our immune gamma globulins have communicated that in 2 cases a generalized serum-sickness type of reaction occurred, one in a leukemia patient, another in a tumor patient. Localized, short- lived, urticariform rash may be explained by the accumulation of a relatively large amount of unabsorbed gamma globulin. As this is absorbed into the system it becomes fixed by serological specificity onto tumor tissue. On the other hand, this residual activity could be due to occasional contaminating traces of al- bumins in the preparation.
Some tumor patients had no local reactions
at all after 45 consecutive daily injections. Local inflammatory reactions have been re- lated to the degree of subcutaneoas infiltra- tion and seepage. Subcutaneous injections in- variably produced erythema followed by induration. Pain was associated with the locale of injection. It was practically absent in the gluteal region if the injections were given above a line connecting the anterosuperior and the posterosuperior iliac processes.
Elevation of temperature to 38 to 39.5' C. 12 hours after the injection was found but not constantly. In 3 leukemia patients, increased hemolysis was seen during the administration of gamma globulin. In 2, the treatment could be continued under cover of corticosteroids, and in 1, it had to be discontinued. The last had a high leukemic cell count.
The reason for this hemolysis could be two- fold. One is the possibility of antinormal ac- tivity of the immune gamma globulin due to incomplete absorption of the leukemic ex- tract by antinormal gamma globulin. Such ac- tivity is easily detected and can be corrected. The other possibility, which was demonstrated in the third patient, is the following: a saline eluate from the patient's erythrocytes precipi- tated strongly the immune gamma globulin while the washed erythrocytes were no longer agglutinated by the gamma globulin. The possibility arises that antigens liberated from large numbers of disintegrated leukemic cells become absorbed onto the erythrocytes. This would be in agreement with the observations of Calaresu et al.5 and Zilber.25
The pharmacodynamics of this agent are
FIG. 3. A, Modified Oudin technique. The gamma globulin (Fig. 2C) and its dilutions (Z0, a to Z-5, f ) are incorporated in agar in the lower half of the Wintrobe tube. Tumor antigens are also incorporated in agar on the upper part of the tube. After centrifuging for 1 hour at 1,5OOxg, the lines of precipitation appear at or near the interface. B, In this figure, the same system in Ouchterlony double diffusion show the correspondence of the dilutions (2O, a to
f ) . The titer was 2-5.B as determined in extrapolating tubes.

310 CANCER March 1963 Vol. 16
far from being explorecl. The dosage, form, and schedule, length, and routes of administra- tion, limits of tolerance, and adjuvants of the therapy have not been determined precisely. Quite recently, we found that this material can be placed safely in the peritoneal and in the pleural cavities. Lysis of tumor implants by direct contact may be expected.
In leukemia patients, combination with cor- ticosteroids seems to be synergistic. In the ad- vanced cancer patients, transfusions of fresh plasma have been added to the therapy in view of the in vitro neeld of complement for immunocytolysis and indicatioas that thesc patients might be depleied of complement.17
lmmediate Effects of Immune Gamrnaglo- biilinotherafiy on Symptcims and Signs of hTeo- plnslic Disease. Pain. Pain due to the neoplasia, whether localized or radiating, was one of the f ir s i symptom5 to be relieved. Occasionally there WPS an initial exacerbation following the first 2 or 3 injections. This was probably due t o necrosis, inflammation, and edema in a n d around the tumor. It was followed by gradual decrease and complete abolishment. This effect was measured by the amount ol narcoiics and setlativec; required before anti during treat- ment. It was noticed in !ionic patients on sev- el a1 occasions that when the gamma globulin was replaced by a placebo, the pain always re- curred (Fig. d).
General Condition. Improvement ol general condition was measured by the increase in hemoglobin in tumor patients,4 weight gain, improvement of appetite, and a sense of well- being.
Regression of signs and symptoms in tumor patients was detected by clinical, radiologiral, endoscopic, histological, laboratory, and pho- tographic methods with their inherent limita- tions, before, during, and after a course of treatment.
In leukemia patients, daily peripheral blood counts and bone marrow studies when leuke- ink cells disappeared from the blood, consti- tuted the main basis for evaluation. A trend towards the restoration of normal hematopoie- sis and the suppression of leukemic elements represented a trend towards remission. A par- tial remission is considered a situation in which hematopoiesis is sufficient and stable despite the presence of leukemic cells in the blood, hence in the marrow, usually in small num- bers. An incipient relapse is a stage when liernatopoiesis shows slow progressive decline, usually with an increase in the number of leu-
7
I
+ + + t t.?411/6I DATE 1120/61 t t t
GG PI GG GG GG GG GG PI
FIG. 4. Case 27. Patient M.O. Relationship of the number of codeine tahlets required for pain in 24 hours and the injection of immune gamma globulin (GG) and placebo (Pl).
kemic cells. In full relapse, there is failure of hematopoiesis. A complete remission is a stage of normal hematopoiesis without circu- lating leukcmic cells and with a number of leukemic cells in the bone marrow that would not or barely per se enable the diagnosis of leukemia in a patient who is otherwise asymp- tomatic.
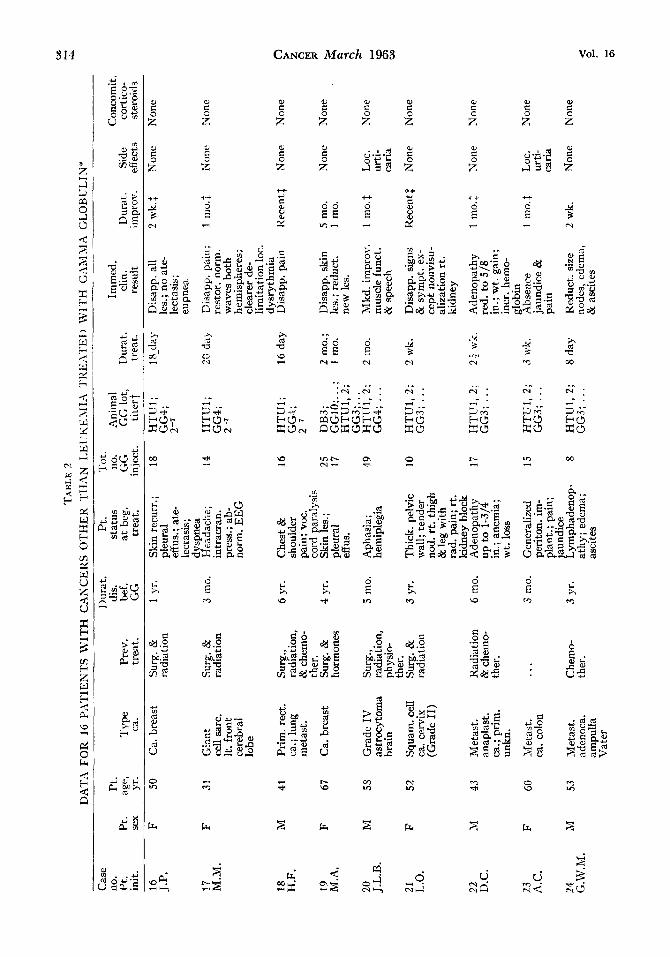
Immediate Therapeutic Eflects of Equine Antileukemic Gamma Globulin on I5 Leu- kemia and 16 Cancer Patients. Tables 1 and 2 summarize the data for the patients, the therapy given, and the immediate results. Each case is abstracted and described separately in text.
As can be seen from Table 1, this group of 15 leukemia cases is quite heterogeneous. Five of the patients were children. Of these, 2 had acute lymphatic leukemia and 2 had acute stem cell leukemia. Of the latter, 1 had a con- genital form of the disease. This case was in- cluded because specific passive immunotherapy was used even though iso- rather than hetero- antibodies were the therapeutic agent and be- cause of the unusually long remission period. Of the 10 adults, 3 had acute rnyeloblastic, 1 acute stem cell, 1 acute monocytic, and 1 chronic lymphatic leukemia; 1 patient had acute erythromyelosis (DiGuglielmo’s clisease), and in 3 cases, the disease represented transi- tion forms between lymphosarcoma and acute lymphatic leukemia. Lack of decrease of leu- kemic cells in the case of chronic lymphatic leukemia was anticipated. Previous in vitro re- sultss, 26 showed lack oE cross reaction between antibodies against forms of acute leukemia and antigens from the lymphoid elements of chronic lymphatic leukemia. On the other hand, the last, as mentioned before, had not been included in the leukemic cocktails.

IMMUNOTHERAPY OF NEOPLASTIC DISEASE IN MAN. 1. * de CnrvUlho 31 1 No. 3
CASE REPORTS
In the case reports that follow, the letters “LK” accompanied by numerals indicate the order in which the leukemia patients and/or leukemic materials (samples of blood, bone marrow, spleen) became available. They do not necessarily mean the series of treated pa- tients. Numbers omitted do not mean patients omitted.
Case 1. (LK17). E.M. was a 7-year-old white girl. The diagnosis of acute leukemia was made on Feb. 13, 1958. The child received blood transfusions, corticosteroids, and 6- mercaptopurine between this date and June, 1958. A partial remission started Apnl 15, 1958, and lasted to June 3, 1958, when signs of relapse appeared. On this date, the hemo- globin was 9 gm. per 100 cc. There were 1,000 white blood cells per cu. mm., with 80% of them lymphocytes, and there were 55,000 plate- lets per cu. mm. The only treatment given for this relapse was 20 injections of donkey gamma globulin 5 at 3-day intervals. By mid-August, the hemoglobin was 13 gm. er 100 cc. There
which 87% were neutrophils, and there were 250,000 platelets per cu. mm. This was taken as a sign of remission, and the treatment was discontinued. I n May, 1959, the hemoglobin was 8 gm. per 1OQ cc. There were 4,000 white blood cells per cu. mm., 22y0 of which were blast cells, and there were 50,001) platelets per cu. mm. A second series of 14 injections was given as the only treatment during April and May, 1959, after which the hemoglobin was 12 gm. per 100 cc. There were 4,900 white blood cells per cu. mm., 64% of them neutrophils. There were 230,000 platelets per cu. mm. Treatment was discontinued. This remission lasted until June, 1961, when the patient died from an acute illness without receiving a third course of gamma globulin.
Case 2. (LK38). J.S. was a mongoloid baby boy born to a healthy young mother on Sept. 21, 1959. The child weighed 8 lb,. and was slightly jaundiced at birth. A moderate ABO incompatibility existed. Examination of the peripheral blood 2 hours after birth revealed a white blood cell count of 50,000 per cu. mm., of which 90% were highly anaplastic stem cells; 5y0, normoblasts; and 5%, normal leu- kocytes. The hemoglobin was 9 gm. per 100 cc., and there were 50,000 platelets per cu. mm. A bone marrow sample was poor In cells but revealed the same anaplastic elements seen in the blood. A blood transfusion succeeded in raising the hemoglobin but did not change ap- preciably the nucleated cell count and the
were 10,000 white blood cel P s per cu. mm., of
over-all picture. 6-Mercaptopurine was insti- tuted at 8.5 mg. per day but had to be dis- continued after 6 days because of severe toxic signs, such as profuse diarrhea, severe dehydra- tion, and weight loss, and because there was no change in the number and quality of the leukemic cells. Hematological studies on the mother showed her blood to be completely normal.
A fluorocarbon protein preparation was made from the child’s blood cells and tested in gel-diffusion plates against the mother’s se- rum and against other isoagglutinating and compatible control serums. The mother’s se- rum was also tested against protein of leu- kocytes from different individuals. These tests disclosed a marked precipitation reaction be- tween the mother’s serum and the leukemic protein from the child.
For this reason, AB substances were added to the mother’s serum to neutralize isoagglu- tinins and then given intramuscularly to the child. Eighteen doses of 2 ml. each on consecu- tive days were injected. On the third day after the serum therapy, the number and percent- age of leukemic cells started declining as those of the neutrophils and lymphocytes rose. After the eighteenth day the child was in complete remission with a residual basophilia (3 to 5%), which persisted for a month. No other treat- ment was instituted, and no signs of recurrence have appeared to the date of writing (March 14, 1962).
This case raises some questions. In the litera- ture, 4 children with congenital leukemia, diag- nosed in the first few days or weeks of life, are reported to have a survival time od no longer than 6 months. The unusual course in this in- stance raised doubts as to the true leukemic nature of the case, even when the early blood smears were examined. However, independent examinations of the smears by hematologists not knowing of their source have been con- firmatory of leukemia. Berman2 concluded his report, “Your sealed note did not help me. On a purely objective morphologic basis I would have to call this leukemia. However, it is not the usual picture of acute leukemia quanti- tatively. One would expect that the atypical stem cells would have been almost the only kind of cells in the blood, at the b,eginning (Slide 0). On the other hand, the picture is certainly not that of hemolytic disease of the newborn-the stem cells are far too abnormal.” Association with mongolism makes it 4 times more probable of being leukemia. With 1 single exception,’ leukemic babies have been born of nonleukemic mothers.
The association of leukemia and ABO iso- immunization might have facilitated exposure of the mother to leukemic antigens of the fe-

w
N
L-
TA
BL
E
1 D
AT
A F
OR
15
PA
TIE
NT
S W
ITH
VA
RIO
US
LE
I:K
EM
IAS
'I'R
E,\T
EP)
W
ITH
GA
Mh1
-I G
LO
BU
LIN
AN
D C
HE
MO
TH
ER
APY
*
Cas
e N
o.
Dur
at.
Pt.
T
ot.
Len
gth
Con
- G
G r
emis
s.
no.
Pt.
Prev
. ch
emo-
di
s.
stat
us
Ani
mal
, no
. tr
eat.
/ co
mit.
Le
uk.
Pt.
age,
T
ype
chem
o-
ther
. be
f. at
beg.
G
G lo
t, G
G
no.
cort
ices-
Pt
l.,
Com
pl.,
Tot
. Si
de
no.
sex
yr.
leuk
. th
er.
rem
iss.
G
G
trea
t.
tite
rt
inje
ct.
inje
ct.
tero
ids
no.
no.
no.
Dur
at.
effe
cts
1 LK
17
2 LK
38
3 iK39
4 LK
45
5 LK
46
6 LK
47
7 LK
48
8 LK
66
9 LK
69
10
LK
70
11
LK
71
12
LK
73
13
LK
74
14
LK
76
15
LK
79
F
M
M
M
M
M
M
M
M
M
M
M
F M
M
7 A
cute
Y
es
lym
phat
ic
New
- A
cute
stem
Y
es
born
51
12
48
22 ...
52
40
48 4 38
67
50
14
56
cell
Acu
te s
tem
Y
es
ceii
Acu
te
Yes
ly
mph
atic
A
cute
mye
- N
one
lobl
astic
A
cute
Y
es+
lym
pho-
X
-ray
bl
astic
Lyr
npho
sarc
. Y
es
8r a
leuk
. ac
ute
lym
- ph
atic
leuk
. A
cute
mye
- Y
es
lobl
astic
Acu
te
Yes
er
ythr
emic
m
yelo
sis
Acu
te s
tem
Y
es
cell
Acu
te m
ye-
Yes
lo
blas
tic
Chr
. N
one
lym
phat
ic
Lym
pho-
Y
es
sarc
omat
osis
A
cute
mye
- Y
es
lo-m
ono-
cy
tic
Acu
te
Non
e m
onoc
ytic
1 com
pl.
0 0 1 com
pl.
0 1 pt
l.
1 pt
l.
0 1 pt
l.
0 1 pt
l.
1 pt
l.
4 m
o.
8 da
y
8 da
y
5 m
o.
1 d
ay
6 m
o.
15 r
no.
8 m
o.
9 m
o.
6 m
o.
6 m
o.
12 m
o.
14 m
o.
7 m
o.
4 da
y
Full
D
B1;
GG
5;
rela
pse
199
Full
M
othe
r's
rela
pse
seru
m;
1:2,
500
Full
D
B3;
GG
6;
reia
pse
1:2*
B
eg.
DB
3; G
G6
rela
pse
& 7
; 1 :24
In
cip.
D
B3;
GG
8;
dis.
1 :
20,0
00
Full
D
B3;
GG
8 re
laps
e &
9; . . .
Re-
H
LK
2,3;
la
pse
GG
4; 1
:26
Full
H
LK
2,3;
bl
own
GG
4; 1
:26
DB
3; G
G4;
1 :
26
DB
3; G
G4;
1 :
28
Full
H
LK
2,3;
bl
own
GG
4; 1
:26
Full
H
LK
2;
blow
n l:2
5
Exa
cer-
H
LK
lJ;
bati
on
GG
3; . .
. B
eg.
HL
K1,
2;
rela
pse
GG
1; 1
:22
Beg
. D
B3;
re
laps
e G
G12
;
Full
D
B3;
GG
12;
blow
n l:
24
1 :24
34
18
17
42 8 38
55
30
20
15 7 15
15 7 18
10 w
k.
Non
e 0
2
18 d
ay
Non
e 0
1
26da
y/S
Yes
3
2 da
y/2
18 m
o.
Inte
r-
0 1
m
itt.
60
day
Non
e 1
0
28 d
ay
Inte
r-
0 1
mit
t.
36 d
ny/l
2 In
ter-
0
1 30
0 da
y/43
m
itt.
3 w
k./1
2 C
ontin
. 0
1 7
wk.
/4
2 w
k./1
4
6 w
k.
Con
tin.
0
1
2 7
wk.
N
one
1 29
mo.:
N
one
3 3,
6, 2
N
one
1 20
mo.
N
one
1 2
mo.
N
one
wk.
1 3
mo.
LO
C. in
- fl
amm
. re
act.
aft.
$?
mod
. 1s
t inj
ect.;
pa
in
z 2 1
1 yr
.$
Non
e A
%
7 1
90da
yS
Non
e 3
r)
Y
20 d
ay
Con
tin.
1 0
3 w
k.
Con
tin.
0
0
4 m
o.
Con
tin.
O$
0
4 w
k.
Con
tin.
0
1
7 da
y C
ontin
. T
rend
0
anti
met
ab.
& tr
ansf
us. to
war
d re
mis
s.
18 d
ay
Non
e 1
0
1 22
day
H
emol
y-
sis(
?)
Cyt
o-
peni
a( ?)
ot
Non
e
1 8
wk.
$ H
emol
y-
sis(?)
O$
10 d
ay
Non
e
0 01
1
1: 18
day
Non
e .c: 2
> *T
he re
sults
giv
en i
n th
e ta
ble
are
as o
f M
arch
14,
196
2.
tIn
this
col
umn,
DB
ref
ers
to d
onke
y ga
mm
a gl
obul
in, a
nd H
LK
ref
ers
to h
orse
ant
ileuk
emia
gam
ma
glob
ulin
. SA
live a
t ti
me
of w
ritin
g (M
arch
14,
196
2); t
reat
men
t co
ntin
ues.
$M
arke
d pl
atel
et i
ncre
ase.
]]
Die
d of
infe
ctio
us h
epat
itis
whi
le i
n re
mis
sion
. Q
)

No. 3 IMMUNOTHERAPY OF NEOPLASTIC DISEASE IN MAN. I. . de Cnwalho 313
tus. Hence the antileukemic properties of the mother's serum. In vitro these properties could be demonstrated by the cytotoxicity tests de- scribed previously.
Case 3. (LK39). H.M. was a 51-year-old man. The diagnosis of acute leukemia was made on Dec. 17, 1959. On admission to the hospital his hemoglobin was 9.8 gm. per 100 cc. There were 6,900 white blood cells per cu. mm., 15% of them leukemic cells, and 170,000 platelets per cu. mm. The bone marrow was hypoplas- tic and paucicellular, with 45% Mast cells. The temperature was 38.5"C. Blood transfu- sions, methylprednisolone, and 6-mercaptopu- rine were given from Dec. 31, 1959, to Feb. 26, 1960. Cytotoxicity tests with donkey B3 gamma globulin 6 titered only to 1 to 1. Five injec- tions of 1 cc. and 0.5 cc. were given during this period. On Feb. 26, 1960, the hemoglobin was 10 grn. per 100 cc. There were 5,200 white blood cells per cu. mm., with 6% leukemic cells, and there were 266,000 platelets per cu. mm.
He was in partial remission and asympto- matic but relapsed 3 weeks later (March 14, 1960). The hemoglobin was 6.55 gm. per 100 cc. There were 41,000 white blood cells per cu. mm., with 8.5% leukemic cells, and there were 60,000 platelets per cu. mm. The mar- row was 90% blast cells, and there was pro- fuse hemorrhage. The treatment given earlier was resumed, and he received 10 injections of donkey B3 gamma globulin 6. He was dis- charged from the hospital on April 12, 1960, in partial remission. At that time the hemo- globin was 12.35 gm. per 100 cc. There were 6,100 white blood cells per cu. mm., with 19% leukemic cells, and there were 288,000 platelets per cu. mm. The marrow showed 25% blast cells, and he was asymptomatic.
He relapsed in 6 weeks (June 1, 1960). The hemoglobin was 8.35 gm. per 100 cc. There were 20,000 white blood cells per cu. mm., with 80% leukemic cells, and there were 70,000 platelets per cu. mm. The marrow was com- pletely blastic, the submaxillary lymph nodes and the spleen were enlarged, and there were fever and bleeding. Two injections of donkey B3 gamma globulin 6 were given, and by June 13, 1960, the nodes had regressed. The hemo- globin was 9.2 gm. per 100 cc. The white blood cell count was 5,100 per cu. mm., with 50% leukemic cells, and there were 164,000 plate- lets per cu. nun. He was asymptomatic except for weakness. Two weeks later (June 27, 1960), he had severe hematuria and a cerebral hemor- rhage. The hemoglobin was 6.8 gm. per 100 cc. The white blood cell count was 150,000 per cu. mm., with 100% leukemic cells, and there were 20,000 platelets per cu. mm. The patient died, and the autopsy revealed massive leu-
kemic infiltration, hemorrhages of the organs, and a large cerebral hemorrhage.
Case 4. (LK45). H.S. was a 12-year-old white boy. In November, 1959, he had a complete physical examination that was negative. In March, 1960, he became pale, bruised easily, and on 3 occasions had cramplike pains in the abdomen not followed by diarrhea or dark stools. On April 18, he was admitted to the hospital with discrete splenomegaly, fever, ane- mia, petechiae, generalized large ecchymoses, and an ulceration in the mucosa of the lower lip that had been present for a month. Bone marrow study by 2 hematologists led to the diagnosis of acute lymphatic leukemia. He re- ceived 3 blood transfusions, cortisone, and 6- mercaptopurine. On May 3, 1960, he was dis- charged, greatly improved, with edema of the face, a weight gain, and in remission. He was maintained on 3 tablets of cortisone per day for gradual withdrawal. By July 27, 1960, he was receiving 1 tablet per day. There had been no fever, bleeding, or other symptoms since he had been discharged from the hospital.
The history revealed that there had been Rh incompatibility in the mother's second and third preceding pregnancies, which had required exchange transfusions. The child's growth curve had been normal, and he was breast fed until the eighth month. At 1, 2, and 3 weeks of age he had had X-ray treatments for an enlarged thymus. During early child- hood he had had measles, rubella, and vari- cella. In December, 1959, he had complete antirabic immunization after being bitten by a dog. There had been no immediate side ef- fects. When first seen by us on Aug. 31, 1960, there was residual obesity from the corticoster- oid therapy. There was no adenopathy; the spleen and liver were not palpable. There was slight hypochromia, with 0.5% lymphoblasts, leukopenia, and a severe thrombopenia. The bone marrow contained 90% leukemic cells. The cortisone was discontinued gradually until 2 weeks before Sept. 10, 1960, at which time active leukemic immunization was started. One milliliter of a leukemic antigen was in- jected intramuscularly. Three days later there was a maculopapular petechial rash over the lower part of the trunk, and there was mod- erate eosinophilia. A tourniquet test was slightly positive; however, a skin test with the leukemic antigen was negative. Vitamins C and P were given for the capillary fragility, and the leukemic antigen was continued for 4 more injections over the next 3 weeks. During this period, the hemoglobin increased from 12 to 15 gm. per 100 cc. and the number of platelets in- creased from 100,000 to 150,000 per cu. mm. No leukemic cells were seen in the peripheral blood. A bone marrow study on Jan. 27, 1961,
‘r.\B
LE
2
DA
T-1
FOR
16
1’A
TIEN
TS \
VI’l
‘H
CA
XC
EK
S O
TH
ER
1‘H
AN
I.E
I K
IilI
l-\
IKE
.\TE
I) b
’l TH G.11111:\
GL
OB
UL
IN”
^_
__
_
__ -
_.
-
Cas
e D
urat
. Pt
. T
ot.
no.
Pt.
dis.
st
atus
no
. :’h
ima1
Im
med
. C
onco
mit.
P
t.
Pt.
age,
T
ype
Prev
. be
f . at
beg
. G
G
GG
lot
, D
urat
. cl
in.
Dur
at.
Side
co
rtic
o-
init.
se
x yr
. ca.
trea
t. G
G
trea
t. in
lcct
. ti
ter t
tr
eat.
resu
lt im
prov
. el
fect
s st
eroi
ds
16
J.P
.
17
M.M
.
18
H.F
.
19
M.A
.
20
J.L.B
.
21
L.O
.
22
D.C
.
23
‘4.C
.
24
G.W
.M.
F I; M
F M
F M
F M
50
21
“I
41
67
58
52
43
60
53
Ca.
bre
ast
Giz
nt
cell
sarc
. It.
fro
nt
cere
bral
lo
be
Prim
. rec
t. ca. ; lu
ng
met
ast.
Ca.
bre
ast
Gra
de I
V
astr
ocyt
oma
brai
n
Squa
m. c
ell
ca. c
ervi
x (G
rade
11)
Met
ast.
anap
last
. ca
.; pr
im.
unkn
.
Met
ast.
ca. c
olon
Vet
ast.
ad
enoc
a.
ampu
lla
Vat
er
Surg
. &
radi
atio
n
Siirg
. 2
radi
atio
n
Surg
., ra
diat
ion,
&
che
mo-
th
er.
Surg
. &
horm
ones
Surg
., ra
diat
ion,
ph
ysio
- th
er.
Surg
. &
radi
atio
n
Rad
iatio
n &
che
mo-
th
er.
...
Che
mo-
th
er.
1 yr
.
3 ili
o.
6 yr
.
4 yr
.
5 in
o.
3 yr
.
6 m
o.
3 m
o.
3 yr
.
~
Skin
rec
urr.;
pl
eura
l ef
fus.
; ate
- le
ctas
is;
dysp
nea
u”
-A
..L
a.
Llc~
uat.,
I1c,
in
trac
ran.
pr
ess.
; ab
- no
rm.
EE
G
Che
st &
sh
ould
er
pain
; voc
. co
rd p
aral
ysis
Sk
in le
s.;
pleu
ral
eff u
s.
Aph
asia
; he
mip
legi
a
Thi
ck.
pelv
ic
wal
l; te
nder
no
d. r
t. th
igh
& le
g w
ith
rad.
pai
n; r
t. ki
dney
blo
ck
Ade
nopa
thy
in.;
anem
ia;
Wt.
loss
Gen
eral
ized
pe
rito
n. i
m-
plan
t.; p
ain;
ja
undi
ce
Lym
phad
enop
- at
hy; e
dem
a;
asci
tes
up to
1-3!4
18
4“
L*
16
25
17
49
10
17
15 8
HTI
Tl ;
GG
4;
2 -7
I yyT
G 1 ;
G
G4 ;
2-
7 HT
Iyl;
G
G4 ;
DB
3;
GG
10;.
. . ;
HT
U1,
2;
GG
3;. .
. H
TU
l, 2
; G
G4;
...
HT
U1,
2;
GG
3; . .
.
2-7 HT
U1,
2;
GG
3; . .
.
HT
UI,
2;
GG
3; . .
.
HT
U1,
2;
GG
3; . .
.
18-d
ay
20 d
dj.
16 d
ay
2 m
o.;
1 m
o.
2 tn
o.
2 wk.
2: wk.
3 Wk.
8 da
y
Dis
app.
all
les.
; no
ate
- le
ctas
is;
eupn
ea
uisa
pp,.
pdiii
; re
stor
. no
rm.
wav
es b
oth
hem
isph
eres
; cl
eare
r de
- lim
itatio
n lo
c.
d ysr
ythm
ia
Dis
app.
pai
n
r\.
Dis
app.
ski
n le
s.;
redu
ct.
new
les
.
Mkd
. im
prov
. m
uscl
e fu
nct.
& s
peec
h
Dis
app.
sig
ns
& s
ympt
. ex-
ce
pt n
onvi
su-
aliz
atio
n rt
. ki
dney
Ade
nopa
thy
red.
in
.; w
t. to 5
/8
gain
;
incr
. he
rno-
gl
obin
A
bsen
ce
jaun
dice
&
pain
Red
uct.
size
no
des,
ede
ma,
&
asc
ites
2 wk.$
1 m
0.i
Rec
ent $
5 m
o.
1 m
o.
1 mo
.$
Rec
ent $
I in
o.1
1 m
o.1
2 w
k.
Non
e
7.7 no
ne
Non
e
Non
e
LOC.
ur
tj-
cari
a
Non
e
Non
e
LO
C.
urti-
ca
ria
Non
e
Non
e
F i4 !!
Non
e
,-
%
Non
e
f
Non
e
Non
e
Non
e
Non
e
3 CI
Q,

TA
BL
E
2 (C
oncl
uded
) D
AT
A F
OR
16
PA
TIE
NT
S W
ITH
CA
NC
ER
S O
TH
ER
TH
AN
LE
UK
EM
IA T
RE
AT
ED
WIT
H G
AM
MA
GL
OB
UL
IN*
Cas
e D
urat
. P
t. T
ot.
no.
Pt.
dis.
st
atus
no
. A
nim
al,
Imm
ed.
Con
com
it.
init.
se
x vr
. ca
. tr
eat.
GG
Pr
ev.
bef.
at b
eg.
GG
G
G lo
t, D
urat
. cl
in.
Dur
at.
Side
co
rtico
- tr
eat.
inje
ct.
tite
r?
trea
t. re
sult
impr
ov.
effe
cts
ster
oids
P
t. P
t. ag
e,
Typ
e
25
F M
.C.K
.
26
J.Y
.
27
M.O
.
28
M.C
.
29
R.O
.
30
M.R
.
31
H.C
.
M
F
F
M
M
F
55
75
29
44
54
70
70
Ade
noca
. si
gmoi
d co
lon
Ade
noca
. pa
ncre
as
with
me-
ta
st.
Ret
rope
ri-
ton.
fib
ro-
sarc
omat
osis
M
etas
t. ad
enoc
a.
brea
st
Ca.
jeju
num
w
ith r
etro
- pe
riton
. m
etas
t.
Met
ast.
rena
l ce
ll ca.
Met
ast.
adv.
sc
hirr
ous
tum
or b
reas
t
Ptl.
rese
ct.
Non
e
Surg
., 2d
op.
Surg
., ho
rmon
es,
radi
atio
n
Surg
. &
radi
atio
n
Surg
. &
radi
atio
n
Non
e
8 m
o.
6 m
o.
14 m
o.
6 m
o.
1 yr
.
9 m
o.
3 yr
.
Con
stip
atio
n ;
pain
; con
- st
rict
. les
.; ex
trem
e an
orex
ia
ho
p. w
iden
ed
duod
ena!
loop
; pa
in; e
pi-
gast
r. p
rom
i- ne
nce;
enl
gd.
liver
Se
v. p
ain;
pe
lvic
mas
s
Mul
t. pa
th.
frac
t.; p
ain
Pain
; em
acia
- tio
n ; a
nore
xia ;
X-r
ay e
vid.
tu
mor
Met
ast.
skin
, lu
ng, &
bon
e;
pain
; cou
gh;
hem
opty
sis ;
an
orex
ia ;
emac
iatio
n Lg
e. i
nfla
mm
. m
ass;
cer
vi-
cal,
supr
a-
clav
ic.,
&
axill
. nod
es;
oste
olyt
ic
met
ast.;
sev
. pa
in
23
28
45
20
31
32 +
10
oral
do
ses
8
HT
U1,
2;
GG
3; . .
.
HT
U1,
2;
GG
3; ..
.
DB
3;
GG
5 &
6;
...
HT
U1,
2;
GG
1; . .
.
HT
U1,
2;
GG
1; . .
.
HT
U1,
2;
GG
1; . .
.;
GG
3; . .
.;
GG
4; . .
.
HT
U1,
2;
GG
4: . .
.
21
mo.
30 d
ay
14 m
o.
2 m
o.
9 da
y
3 m
o.
3 m
o.
6 da
y
Rec
ov. n
orm
. bo
wel
mov
e-
men
t; di
sapp
. pa
in;
wid
en-
ing
lum
en
cons
tric
t. le
s.; i
mpr
ov.
appe
tite
Red
uct.
duo-
de
val l
oop
&
pain
; no
epi-
gast
r. m
ass;
liv
er n
ot p
alp.
Dis
app.
pai
n &
pel
vic
mas
s
Hea
ling
frac
t.;
sl. r
egre
ss.
les:;
redu
ct.
pain
T
epp.
red
uct.
pain
; pos
s. m
inim
al r
e-
duct
. tum
or;
in g
enl.,
neg
. re
sults
R
egre
ss. s
kin
met
ast.;
re-
du
ct. l
ung
met
ast.;
fre
e-
dom
pai
n
Dis
app.
in-
fla
mm
. rea
c-
tion
; sof
t. tu
mor
; dis
app.
su
prac
lavi
c.
node
; red
uct.
0th.
nod
es;
free
dom
pai
n
3 m
o.3
1 m
o.$
11 m
o.$
2 m
o.$
1 m
o.
. . .$
3 m
o.$
Rec
ent t
Non
e
Non
e
Non
e
Non
e
Non
e
Non
e
Non
e
Non
e
Inte
rmit
t.
1 m
o.
Non
e
Non
e
Non
e
Non
e
*The
resu
lts g
iven
in t
he ta
ble
are
as o
f M
arch
14,
196
2.
?In
this
col
umn,
DB
refe
rs to
don
key
gam
ma
glob
ulin
, and
HT
U re
fers
to
hors
e an
titu
mor
gam
ma
glob
ulin
. $A
live a
t tim
e of
wri
ting
(Mar
ch 1
4, 1
962)
; tre
atm
ent
cont
inue
s un
less
oth
erw
ise
indi
cate
d.

Vol. 16 316 CANCER March 1963
revealed 10%. leukemic cells. During this pe- riod, antibodies against the injected leukemic antigen (isoantigens included) had raised to 1 to 200 the titer in the first 2 weeks; i t declined to 1 to 30 in the last week of the antigen ad- ministration. The improvement in the general condition of the peripheral blood and the rise and then fall in the antibody titer were inter- preted as signs of initial antibody stimulation followed by antibody inhibition due to antigen saturation, an effect oft en observed (luring active tumor immunization.D For this reason, passive immunization with immune gamma globulin from a donkey immunized repeatedly with the same leukemic antigen was started (B3 pmma globulin 9). 'The precipitin titer of this gamma globulin was 1 to 2;. One milliliter of 16% gamma globulin was given intramuscularly every 5 days for 3 months. Ten day5 after the initiation of passive therapy, 4 mg. of methylprednisolone was given for 14 days and then discontinued gradually to dis- courage formation of antibody against the donkey gamma globulin Except €or a trans- ient febrile reaction after the first 3 injeciions, no side effects resulted from the administration of more than 132 gm. of immune gamma glob- ulin. During this period of passive immuno- therapy, the hemoglobin fluctuated between 12 and 15 gm. per 100 CIC. An increase in the number of neutrophils to 75% of the count of 6,500 leukocytes per cu. mm. was noted also. No leukemic cells were seen in the periph- eral blood during this period. The platelet count had ranged €rom 68,000 to 150,000 per cu. mm., and the bone marrow was free of leukemic cells on 2 occasions. The patient had been asymptomatic, with steady weight, activ- ity, and appetite, and had been leading a nor- mal school life. Eighteen months after the initiation of the therapy, antibodies against the gamma globulin could not be demonstrated. In December, 1961, while in remission, the patient became severely jaundiced and died 1 week later with signs of acute hepatic failure. Autopsy revealed acute infectious hepatitis with no leukemic infiltration of the organs.
Case 5. (LK46). W.B. was a 48-year-old man. Fatigability and dizziness were noticed 3 months prior to a hematological diagnosis of acute myeloblastic leukemia on Sept. 7, 1960. The hemoglobin was 9,2 gm. per 100 cc. The white blood cell count was 24,300 per cu. mm., with SOYo niyeloblasts, a d there were 38,000 platelets per cu. mm. The marrow contained 90% myeloblasts, and the submandibular lymph nodes were enlarged. The temperature was 40" C. Between Sept. 7, 1960, and Oct. 16, 1960, he received 6 blood transfusions, 8 in- jections of donkey gamina globulin 8, and antibiotics, but no cori.icosteroids or anti-
metabolites. On Oct. 23, 1960, the cervical nodes were not palpable. The patient was afeb- rile and comfortable. The hemoglobin was 10 gm. per 100 cc., and the white blood cell count was 4,000 per cu. mm., with 10% mye- loblasts and 57% neutrophils. There were 160,000 platelets per cu. mm. On Nov. 11, 1960, there was severe hemorrhage and death. The autopsy showed no leukemic infiltrations in the organs, but there were multiple large hemorrhagic splotches.
Case 6. (LK47). W.S. was a 22-year-old man, Acute lymphatic leukemia with lymphosar- coma was diagnosed in June, 1960, b y hemato- logical studies and lymph node biopsy. From June to July, 1960, he received 2,350 r of radi- ation for mediastinal lymphadenopathy, with reduction of the shadow seen by roentgeno- gram and some amelioration of symptoms. From August to December, 1960, he received blood transfusions, corticosteroids, and 6-mer- captopurine, and during that time the white blood cell count decreased from 78,000 to 300 per cu. mm. Before starting immunotherapy with B3 gamma globulin 9, on Dec. 19, 1960, the blood count was: hemoglobin 10 gm. per 100 cc.; white blood cells, 77,500 per cu. mm., with 97yo lymphoblasts; and platelets, 20,000 per cu. mm. The temperature was 40" C., and there were enlarged cervical and axillary lymph nodes as well as enlargement of the spleen. The 6-mercaptopurine was discon- tinued but he continued to receive corticos- teroids. During this period, the patient re- ceived 3 transfusions.
On Jan. 27, 1961, after the injection oE gamma globulin, the hemoglobin was 14.2 gm. per 100 cc., and the white blood cell count was 8,000 per cu. mm., with 1% lymphoblasts. There were 140,000 platelets per cu. mm. The bone marrow contained 77:) lymphoblasts. The lymph nodes were not palpable, the spleen was smaller, and the patient was afebrile. He was maintained on the injections weekly and then biweekly. The blood picture remained stationary until April 20, 1961, when the white blood cell count rose to 66,000 per cu. mm., with 90% lymphoblasts, and the number of platelets decreased to 30,000 per cu. mm. Staphylococcal septicemia developed, and the patient died on April 22, 1961. The autopsy confirmed the diagnosis of septicemia and showed leukemic infiltratcs and hemorrhages.
Case 7. (LK48). S.S. was a 52-year-old man. Acute lymphatic leukemia with lymphosar- coma was diagnosed by hematological study and biopsy on Dec. 19, 1960. There was marked cervical and axillary lymphadenopathy with compressive dysphagia and dyspnea and fa- tigue. He received 400 mg. of chlorambucil

No. 3 IMMUNOTHERAPY OF NEOPLASTIC DISEASE IN MAN. I. * de Caruallio 317
over a 45-day period. This led to reduction but not to disappearance of the lymph nodes. Following therapy, the blood count was: hemoglobin, 10 gm. per 100 cc.; white blood cells, 2,000 per cu. mm.; and platelets, 100,000 per cu. mm. On March 22, 1961, the lymph nodes had enlarged to the previous dimensions, and the bone marrow showed 80% lympho- blasts. He was started on immunotherapy. After 3 injections of gamma globulin at 3-day intervals, all lymph nodes had disappeared. He has been maintained on weekly and later biweekly injections oE gamma globulin, with corticosteroids given intermittently. The remis- sion has lasted to the present time (March 14, 1962). The blood is normal (hemoglobin, 15 gm. per 100 cc.; white blood cells, 6,000 per cu. mm., with a normal differential; and platelets, 400,000 per cu. mm.) as is the bone marrow.
Case 8. (LK66). H.C. was a 40-year-old man. The referring doctor wrote that he had first seen the patient on April 14, 1960, because of bleeding gums of 4 week's duration. The pa- tient had been on long-term anticoagulants following a myocardial infarction in 1960, The therapy was stopped with the onset of the pres- ent illness. Because of persistent bleeding, he was referred to a hematologist. Physical ex- amination at that time showed a well-devel- oped, well-nourished white man. Vital signs were within normal limits. Multiple areas of purpura were noted oveT the extremities and mucous membranes. The gums were actively bleeding. There was no significant peripheral lymphadenopathy or hepatosplenomegaly. The remainder of the physical examination was within normal limits. Laboratory data were as follows: hemoglobin, 9.6 gm. per 100 cc.; white blood cells, 15,250 per cu. mm., with 69% myeloblasts, 1 % metamyelocytes, 1 myelocytes, 17% lymphocytes, 3% eosinophiz and 9% plymorphonuclear leukocytes; and 10,000 platelets per cu. mm. The sternal mar- row examination confirmed the diagnosis of acute myeloblastic leukemia. The patient was started on 6-mercaptopurine, 300 mg. per day. With this therapy, there was a significant de- crease in the white cell count, an increase in the platelets, and a decrease in the bleeding. On June 28, 1961, the white cell count was 2,500 per cu. mm., with 4% myeloblasts. The platelet count was 120,000 per cu. mm. A sternal marrow examination showed a hypocel- lular specimen with approximately 10% mye- loblasts.
At this time, the patient was on a mainte- nance dose of 100 mg. of 6-mercaptopurine per day. The patient did fairly well until August, 1961, when the white blood cell count began to rise, with an absolute increase in the
number of myeloblasts. The platelet count decreased, and bleeding again became a prob- lem.
On Sept. 14, 1961, the patient was read- mitted to the hospital. There were multiple skin hemorrhages. The gingivae were hyper- trophied and hemorrhagic. No lymphaden- opathy or hepatosplenomegaly was noted. The hemaglobin was 9.5 gm. per 100 cc.; white blood cells, 15,650 per cu. mm., with 90% myeloblasts; and there were 34,000 platelets per cu. mm. ?"he sternal marrow was hypercellular, and 85% of the cells were myeloblasts. The 6- mercaptopurine was increased to 300 mg. per day.
After 10 days of therapy, there was no sig- nificant change in the peripheral blood count, and the patient was started on 7.5 mg. of 4-amino-W0-methyl pteroylglutamic acid (Methotrexate) per day. After 10 days of ther- apy, the patient developed the classic toxic reactions encountered with this drug. He was also noted to have a pericardial friction rub, which was felt to be secondary to a small peri- cardial hemorrhage. This cleared in approxi- mately 10 days. The white cell count had dropped to 1,550 per cu. mm., with 2% blast cells. The bone marrow examination revealed 55% myeloblasts; the remainder of the cells were erythroid. During this time, the patient was given several transfusions with fresh whole blood in an attempt to decrease the gum bleeding and the skin hemorrhages. After stopping the Methotrexate, the white cell count increased to 16,000 per cu. mm., with 79% blast cells. The hemoglobin remained in the range of 9 to 10 gm. pm 100 cc., and the platelet count was approximately 80,000 per cu. mm. On Nov. 8, 1961, it was elected to start the patient on methyl glyoxal bis guanyl- hydrazone dihydrochloride in an attempt to induce a remission. The dose suggested by the National Cancer Institute was used, and the patient received 270 mg. intravenously per day. He remained on this dose until Nov. 29, 1961.
On Nov. 24, 1961, the white cell count was 5,100 per cu. mm., with approximately 10% blast cells. The hemoglobin was 8.3 gm. per 100 cc., and there were 34,000 platelets per cu. mm. A sternal marrow aspiration showed sheets of myeloblasts comprising approxi- mately 90% of the cellular elements. Remis- sions have been reported with this drug in the fourth to seventh week of therapy. His course was complicated by multiple axillary ab- scesses and continuous fever. There was some improvement in the sites of infection; how- ever, the patient remained febrile despite mul- tiple antibiotics. On Nov. 29, 1961, the white cell count decreased to 2,400 per cu. mm. The

318 CANCER March 1963 Vol. 16
methyl glyoxal bis guanylhydrazone dihydro- chloride was discontinued. Prednisone, 60 mg. per day, was started. There was a dramatic drop in the temperature to normal levels. On Dec. 6, 1961, the hemoglobin was 10 gm. per 100 cc.: there were 3,350 white cells per cu. mni., 5% of which were blast cells, and there were 28,000 platelets per cu. mm. The sternal bone marrow was hypocellular. The cellular elements present were myeloblasts, plasma cells, and some megaloblastoid normoblasts. The patient was given 2 units of packed cells on Dec. 7, 1961, and discharged from the hos- pital on Dec. 8, 1961, on 10 mg. of prednisone 3 times a clay.
The patient was started on horse immune gamma globulin with adjuvant corticosteroids on Dec. 19, 1961. On Dec. 28, the hemoglobin was 11 gm. per 100 cc. The white cell count WIS 4,500 per cu. mm., with 2y0 myeloblasts and 677; neutrophils. ‘There were 290,000 platelets per cu. mm. The marrow contained fjo,l, myeloblasts. On Jan. 10, 1962, the patient had ii posterior myocardial infarction (the third in 2 years) during which immunotherapy rv‘is continued. Despite the daily administra- tion of heparin, there were no bleeding epi- sodes. During this period, the hemoglobin fluctuated between 12 and 14 gm. per 100 cc.; the white cells, betwecn 6,000 and 7,000 per ru. mm., with 0 to 2% myeloblasts; and there wcre between 300,000 and 500,000 platelets per cu. mm. His recovery was uneventful. He h a s received injections of gamma globulin at 1- to %day intervals until the present time (March 1-1, 1962). His blood count as of this date shows 12.5 gm. of hemoglobin per 100 cc.; 5000 white blood cells per cu. mm., with 0.5% myeloblasts; and 400,000 platelets per cu. mm.
Case 9. (LK69). T.H. was a 48-year-old man. Acute erythromyelosis (Di Guglielmo’s disease) was diagnosed in February, 1961. He received 52 blood transfusions, corticosteroids, and 6- mercaptopurine until January, 1962, during which period the hemoglobin remained at about 9 grn. per 100 cc., and the white cells fluctuated between 1,000 and 3,000 per cu. mm., with between 50 .and 90% abnormal erythroblasts. The platelet count was always less than 90,000 per CLI. mm. Injections of horse immune gamma globlin were started on Jan. 17, 1962. On this date the hemoglobin was 9.8 gm. per 100 cc. There were 2,050 white cells per cu. mm., with 2501, abnormal eryth- roblasts, and there were 90,000 platelets per cu. mm. The bone manow contained 85y0 paraerythroblasts. The patient had petechiae, fever, splenomegaly, ulceration of the hard palate, weakness, and dizziness. On March 1, 1962, after 20 injections of immune gamma globulin, the hernoglobin was 11.5 gm. per
100 cc., and there were 5,300 white cells per cu. mm., with 30% neutrophils, 60% lympho- cytes, 9% monocytes, and about 2% eosino- phils. The bone marrow showed normoblastic erythropoiesis, 5% myeloblasts, and normo- blastic leuko- and thrombopoiesis. The patient was afebrile, there were no petechiae, and the ulceration of the hard palate had healed.
Case 10. (LK70). K.C. was a 4-year-old boy. Acute stem cell leukemia was diagnosed in June, 1961. He had had 1 partial remission of 4 months’ duration on 6-mercaptopurine and a second partial remission, lasting for 1 month, on Methotrexate. Before starling horse im- mune gamma globulin injections, he was on corticosteroid maintenance therapy. This was continued. On Jan. 9, 1962, the hemoglobin was 10 gm. per 100 cc. The white cell count was 5,050 per cu. mm., with 50y0 blast cells, and there were 150,000 platelets per cu. mm. Two weeks after daily injections (Jan. 20, 1962), the hemoglobin was 10.1 gm. per 100 cc. There were 20,000 white cells per cu. mm., with 60% blast cells in clumps, and 304,000 platelets per cu. mm. On Jan. 30, 1962, the hemoglobin dropped to 3.8 gm. per 100 cc. There were 1,350 white cells, with 95p0 leu- kemic cells, and there were 50,000 platelets per CLI. mm. Coombs’s tests, both direct and indirect, became positive, and thcrc was se- vere autoagglutination ol the erythrocytcs. Following transfusions of erythrocytcs, the patient became severely jaundiced, wi ih bil- irubinemia of 12.20 gm. per 100 cc. by direct test and 5.70 mg. by indirect test. Despite massive corticosteroid therapy, the patient be- came acutely ill and died 2 days later. At the time of death, the hemoglobin was 9.8 gm. per 100 cc., there were !JOO white cellu, all blast cells, and 38,000 platelets per cu. mm. Autopsy revealed massive leukemic- infiltration of the organs and hemorrhages.
Case 11. (LK71). K.H. was a 38-year-old man. Acute myeloblastic leukemia was diag- nosed at the time the first symptoms appeared (Aug. 5, 1961) by peripheral blood and bone marrow studies. Hc received blood trans- fusions, antimetabolites, and corticosteroids. No remission was obtained. Immediately bc- fore the start of gamma globulin (Dee. 28, 1961), the hemoglobin was 9 gm. per 100 cc. There were 4,000 white cells, with 201, myelo- blasts, and 45,000 platelets per cu. mm. Con- ventional treatment was continued during the period in which he received gamma globulin. On Jan. 20, 1962, after 7 injections of gamma globulin, the hemoglobin was 10 gm. per 100 cc., and there were 12,000 white cells per cu. mm., with 63% myeloblasts, and there were 18,000 platelets per cu. mm. The patient’s

No. 3 IMMUNOTHERAPY OF NEOPLASTIC DISEASE IN MAN. I. . de Cnrvalho 319
course was progressively downhill and he died on Feb. 6,1962.
Case 12. (LK73). J.F. was a 67-year-old man. Chronic lymphatic leukemia had been diagnosed on Feb. 14, 1961. At the time of diagnosis there was generalized lymphadeno- pathy and hepatosplenomegaly, with full lymphoblastic bone marrow, although the pe- ripheral white blood cell count was not more than 3,000 per cu. mm., with 83% lyyphoid elements. He received no treatment until Dec. 8, 1961, when epigastric distress, severe anemia, hemorrhage, and fever started. At this date the hemoglobin was 8.3 gm. per 100 cc., and the white b'lood cell count was 50,000 per cu. mm., with 99% lymphocytes and lymphoblasts. There were 50,000 platelets per cu. mm. He received several transfusions, corticosteroids, antibiotics, and, in addition, 14 injections of horse gamma globulin between Dec. 8, 1961, and March 1, 1962. On the last date the blood count showed 10 gm. of hemoglobin per 100 cc. and 20,000 white blood cells per cu. mm., with 85y0 lymphocytes. There were 300,000 platelets per cu. mm. There was no reduction in the size of the liver and spleen. Otherwise, the patient was asymptomatic.
Case 13. (LK74). M.H. was a 50-year-old woman. On Dec. 30, 1960, she was found to have an abdominal mass. Routine laboratory studies showed the urine to be normal and the hemoglobin to be 11 gm. per 100 cc., with 5,400 white cells per cu. mm., and a normal differential. The erythrocyte sedimentation rate was 54. Gastrointestinal roentgenograms and rectoscopy were negative. The chest roent- genogram was negative, as were studies of the kidneys, ureters, and bladder, and an intra- venous pyelogram. On Jan. 19, 1961, an ex- ploratory laparotomy was performed. A large retroperitoneal tumor was found, which, on biopsy, proved to be a giant follicular cell lymphoma. The patient received a course of nitrogen mustard in the postoperative period. On Feb. 28, 1961, she received X-ray therapy to the area of the previously described mass. On March 1, 1961, a marked left pleural ef- fusion was noted, and 1,300 cc. of fluid was removed. On April 14, she developed a neuritic type of pain in her jaw and received X-ray therapy to this area with good response. On July 3, the patient was readmitted to the hos- pital, complaining of pain, especially in the dorsal spine area. The erythrocyte sedimenta- tion rate at this time was 113 and the hemo- globin was 11 gm. per 100 cc. She received X-ray therapy to the dorsal spine area with the relief of svmDtoms. She was next admitted to the hospital Gn Aug; 28, 1961, because of wide- spread rheumatic-type symptoms and rather " , _ I
severe headache. At this time, the sedimenta- tion rate was 95, and the hemoglobin was 10 gm. per 100 cc., with a white cell count of 5,000 per cu. mm. and a normal differential. During this admission, she received 20 mg. of nitrogen mustard in 2 doses. On Sept. 22, at which time she was much improved sympto- matically, the hemoglobin was 9.5 gm. per 100 cc., with a white cell count of 3,500 per cu. mm. and a normal differential. The patient was again admitted to the hospital on Sept. 28, 1961, with widespread rheumatic complaints, a hemoglobin of 10 gm. per 100 cc., and a sedi- mentation rate of 95. She received 20 mg. of nitrogen mustard in 2 doses and 1 blood trans- fusion during this period of hospitalization. She was then followed as an out patient until Nov. 10, at which time the blood count was essentially normal; however, the sedimenta- tion rate was in the 80's. At this time, she was first given cyclophosphamide (Cytoxan) 50 mg. twice daily. She was next seen on Nov. 24, 1961, when the hemoglobin was 10.5 gm. per 100 cc. and the white cell count was 4,000 per cu. mm. The dose of Cytoxan was de- creased to 25 mg. per day; however, she took 25 mg. every other day. She was seen again on Dec. 5, 1961, at which time the hemoglobin was 11.9 gm. per 100 cc., and the white cell count was 4,900 per cu. mm.
Immediately before the beginning of gamma globulin therapy (Jan. 22, 1962) the hemo- globin was 9.8 gm. per 100 cc. The white cell count was 2,050 per cu. mm., with 27% atypi- cal lymphocytes classified as lymphosarcoma cells, and there were 40,000 platelets per cu. mm. The marrow showed the same type of cells. She was febrile, had extensive herpes simplex on the right side of the face and en- larged cervical nodes on both sides, but no splenomegaly or abdominal masses. Between Jan. 22, 1962, and Feb. 17, 1962, she received 15 injections of gamma globulin, during which time 2 blood transfusions were re uired and
date, the hemoglobin was 11 gm. per 100 cc., and the white cell count was 7,000 per cu. mm., with normal differential. There were 370,000 platelets per cu. mm. The marrow did not show any lymphoblasts, and the patient was asymptomatic.
Case 14. (LK76). R.P. was a 14-year-old white boy. Acute myelomonocytic leukemia was diagnosed in August, 1961. With the aid of corticosteroids, transfusions, and antimetabe lites, he was maintained in a stage of partial remission. In January, 1962, there was some lymphadenopathy, with a palpable spleen, in- creased blast cells in the blood, and a platelet count of 65,000 per cu. mm. On March 5, 1962, before starting on dailv iniections of B3
corticosteroids were continued. As o P the latter

CANCER March 1963 Vol. 16 320
gamma globulin 12, the hemoglobin was 7 gm. per 100 cc,, with ar white cell count of 1,300 per cu. mm., with 84% lyofhocytes, 6% blast cells, and 10% neutrophi s, and there were 60,000 platelets per cu. mm. The marrow was completely blastic. After 7 injections of immune gamma globulin, the hemoglobin was 8.4 gm. per 100 cc. There were 2,500 white cells per CU. mm., with 50% lymphocytes, 46% neutrophils, and no blast cells, and there were 98,000 platelets per c11. mm.
Case 15. (LKT9). K.T. was a 56-year-old man. Acute monocytic leukemia was diagnosed Feb. 27, 1962. A t that time the hemoglobin was 8.9 gm. per 100 cc., and the white cell count was 84,000 per cu. mm., with 60% leukemic cells, and there were 130,000 plate- lets per cu. mm. The marrow was completely blastic. There were markedly enlarged cervi- cal lymph nodes and aphonic hoarseness that had started 2 days ear11 er. Pharyngolaryngo- logical examination did not reveal inflamma- tion or other lesions. The temperature was 40" C. No therapy other than antibiotics had been given. Horse immune gamma globulin (2 cc. intramuscularly, Idaily) was given first on Feb. 27, 1962. After 3 injections (March 2, 1962), the lymph nodes were not palpable, he had regained his voice, and he was afebrile. On March 5, 1962, the hemoglobin was 11.7 gm. per 100 cc., and the white cell count was 50,000 per cu. mm., witb 7% monocytes and 6807, neutrophils. There were 250,000 platelets per cu. mm.
Table 2 lists a heterogeneous group of tumors (breast, brain, colon, kidney, cervix, ampulla, jejunum, fibrosarcomatosis, and met- astatic cancer from an unknown primary) in patients ranging in age from 29 to 73 years with the history of disease dating from 3 months to 3 years. Of these, only 1 was un- treated, all others having received several courses of different form of therapy before experimental treatment. Significant improve- ments, when existent, took place within 3 to 30 days. Reduction of pain was probably the first and a constant feature. Recurrence of signs and symptoms after initial improvement happened as early as 2 weeks.
The mechanisms of the therapeutic effects are not known. Recurrence may be due to ac- quired selective resistance of the tumor cells, such as the one known irt chemotherapy, or to antibody response of the organism to the horse gamma globulin. 'The last could be pre- vented by concomitant steroids, desensitization techniques, radiation or chemotherapeutic suppression of antibody formation, or other
means of obtaining immunological unrespon- siveness. The possibility 01 mounting radio- isotopes or antimetabolites14 onto the immune gamma globulins is also worth exploring. A great deal of investigation is indeed required to uncover the unknowns and the potentials of iminunotherapy of neoplastic disease.
Case 16. J.P., a 50-year-old white woman, had had a left mastectomy €or carcinoma of the breast in 1960. On Feb. 1, 1962, before be- ginning therapy, she complained of pulmonary symptoms, dyspnea, and a gating feeling when she breathed. There was atelectasis of the left lower lobe due to mediastinal metastases. She also had an inflammatory type of intracutan- eous cancer, which was biopsied and showed cancer cells in the skin. I t was one of those flat lesions that could not be ielt as a raised tumor but manifested itself by erythema. After 9 days of treatment (daily injections of hy- perimmune gamma globulin), the erythema of the skin was much more marked than it was before, and some new areas had appeared on the back as raised inflammatory-appearing islets of tumor that were large enough to be palpable. After 9 more days of therapy, the erythema had nearly disappeared from over the upper half of the lesion and was much less apparent throughout except for 1 spot in the medial border. The raised nodules in the back disappeared completely, and the over-all ap- pearance of the lesion was greatly improved. At that time the patient stated that when she got up in the morning the lesion looked en- tirely white and that it was only after walking around with her breast prosthesis on that there was any redness remaining in the area. In addition to this, a roentgenogram of the chest at that time showed clearing of the atelectasis at the left lung base, and, although it was difficult to bc certain, there appeared to be some shrinkage of the size of the mediastinal shadow (Fig. 5A and B). Two weeks later, the skin resumed the inflammatory aspect it had had before treatment, although a roentgeno- gram of the chest showed it to be unchanged. No biopsy was done at this time, and treat- ment is being continued.
Case 17. M.M., a 31-year-old white woman, was admitted to another hospital as an "emer- gency" on Nov. 16, 1961. Because of aphasia, she was not able to give a very accurate his- tory. However, information was obtained from her husband, who stated that this had been a rather rapidly progressing story of headache, confusion, aphasia, and weakness of the right upper and lower extremities. There was no evidence of papilledema; there was definite right hemiparesis. There was no evidence of

No. 3 IMMUNOTHERAPY OF NEOPLASTIC DISEASE IN MAN. I . * de CU7‘7JU~hO 321
FIG. 5. Case 16. Patient J.P. This woman had carcinoma of the breast. A, Before treatment, showing atelec- tasis at the left base. B, After 18 injections of immune gamma globulin, there is clearing of the atelectasis at the left base, and, although it is difficult to be certain, there appears to be some shrinkage of the size of the mediastinal shadow.
a field defect. The electroencephalogram re- vealed a grade I1 delta localization in the frontosylvian area, and roentgenograms of the skull showed a shift of the pineal gland to the right of the mid-line, and the pineal gland was pushed backward and downward by a frontally placed lesion. Carotid angiography was advised and carried out on Nov. 17; it re- vealed a shift of the anterior cerebral complex toward the right and the displacement down- ward of the middle cerebral complex. At op- eration the same day, a giant cell sarcoma of the posteroinferior part of the left frontal lobe was encountered and removed as totally as possible, though complete removal could not be carried out. The tumor was partially cystic, and the cyst evacuated. Bleeding was con- trolled, and the operation was terminated.
After the o eration, the patient had severe headache in $oth temporal regions with a sensation of pressure (“outward pulling”) and occasional vomiting. She was admitted to the hospital for immunotherapy on Feb. 3, 1962. At that time, she required sedation every 2 hours, day and night. The hemoglobin was 9.2 gm. per 100 cc. There was no papilledema. Her appetite was poor, and there was nausea. An electroencephalogram revealed slow wave patterns aver bath hemispheres, with dysrhyth- mia localized over the left frontocentroparietal
area (Fig. 6A and 33). The first 3 injections of gamma globulin were given at 2- to 3-day in- tervals. Eight hours after the third injection, she slept for 10 hours uninterru tedly and
on daily injections. Five hours after the fifth injection, she had very severe headache, an increased sensation of pressure, and vomiting. This disappeared in 3 hours, after which she slept for 8 hours. From the eighth injection on, she was completely asymptomatic and ate well. The hemoglobin was 12 gm. per 100 cc. The encephalogram on Feb. 28, 1962 (20 days later), showed restoration of normal waves over both hemispheres, with the extent of the focal dysrhythmia clearly demarcated (Fig. 6C and D). She was discharged from the hospital, ambulatory, to continue treatment. After she went home she was reported to have had headache and nausea during a menstrual pe- riod that occurred at the same time as a viral infection of the upper respiratory tract and to improve afterward.
Case 18. H.F. was a 41-year-old white man. In 1956, he had had an adenocarcinoma of the rectum removed surgically via the ab- dominal route with end-to-end anastomosis. There was no evidence of recurrence until 1960, when apparently a nodule developed in
woke without headache. She was t K en started

(For caption see page 324.)
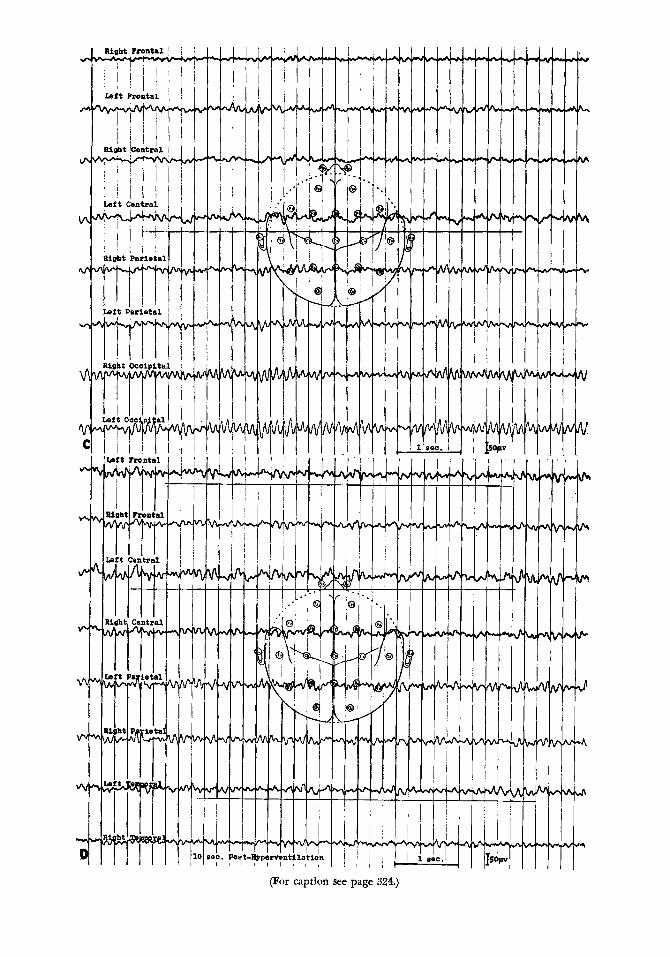
(For caption see page 324.)

3 24 CANCER March 1963 Vol. 16
the right lung, and a pneumonectomy was done. There was tumor left riding over the 2 main bronchi, carina, and lower part of the trachea. In 1961, the patient began to lose weight and received radioactive cobalt (CosO) therapy aimed at the right lung area and the mediastinurn. T h e patient had lost 15 lb. be- fore therapy, and he lost 25 lb. during therapy. He was treated 5 days a week for 8 weeks. Dur- ing and after radiotherapy he became hoarse and later aphonic. Progressive difficulty in breathing and swallowing ensued. In January, 1962, the patient received 6 treatments with 5- fhorouracil. There was improved swallowing. Breathing was noisy, but there was better air exchange. On admission to the hospital, he had considerable right chest pain necessitating narcotics (8 times a day) in spite of a negative chest roentgenogram. The trachea and larynx were nonmovable. Paralysis of the vocal cords prevented complete occlidon of the glottis and was responsible for the aspiration of lood and liquids. He was started on antitumor gamma globulin 4 011 Feb. 20, 1962. After the sccond injection, there was mai~ked decrease of chest pain. On March 5, 1962, there was no pain, the appetile was improved, and the patient felt better. The hoarseness persisted, and his speech still had a whispering quality. His weight was stationary at 115 Ib. On March 10, 1962, there was increasing difficulty in breathing, and a bronchoscopy was performed that showed tu- mor over the carina and invading the left main bronchus.
Case 19. M.A. was a 617-year-old woman. In November, 1957, she had had a left radical mastectomy for carcinoma of the breast with node involvement. No radiation was given. In January, 1931, there was pleural effusion and a recurrence to the lymph nodes on the left axilla, which was biopsied. She was treated by estrogens. On April 16, 1961, there were num- erous papulonodular erythematous lesions over the entire area of the skin of the chest on the left side. Riopsy showed carcinomatous infil- tration. There were circulating tumor cells. The patient received 25 injections of donkey B3 gamma globulin 10, after which all lesions in the skin cleared, and the pleural effusion,
which had been evacuated, did not recur. She was asymptomatic from May, 1961, until Oc- tober, 1961, when numerous erythematous skin nodules appeared again over the same region accompanied by dyspnea clue to pleural ef- fusion. After 17 injections ol: antitumor gamma globulin 3, the skin lesions were greatly reduced although the fluid continued to accumulate. In February, 1962, she de- veloped cerebral thrombosis and died. The cerebral thrombosis was confirmed at autopsy, but the examination showed no carcinomatous lesions on the pleura, which was otherwise markedly fibroplastic. There were 2 metas- tases in the liver. These showed marked signs of regression. They were necrotic and umbili- cated, with wrinkled edges.
Case 20. J.L.B., a 58-year-old man, had had a craniotomy and partial excision of an astro- cytoma, Grade IV, from the left posterior, frontal, and parietal regions close to the falx on Nov. 20, 1961. After the operation there were nominal aphasia and hemiplegia. Fifteen treatments with CoGO were given, followed by physiotherapy. On Jan. 1, 1962, there was slight improvement of speech but not in the function of the limbs. From Jan. 6 to March 5, 1962, he received 49 injections of 1 ml. each of horse immune gamma globulin and con- tinued physiotherapy. At this date (March 14, 19G2), he has regained partial use of his limbs, takes a few steps unsupported, has ac- quired voluntary control of bowel and bladder, and made further progress in speaking. The treatment continues.
Case 21. L.O., a 52-year-old white woman was admitted to the hospital on Feb. 13, 1962, for swelling of the lower extremities. This was most prominent on the right, with pain and tender nodules on the posterior aspect of the right thigh. Symptoms which included low back pain, had been increasing steadily for 3 to 4 months previously. They were first no- ticed in August, 1961. The patient had had 3 previous admissions to the hospital. She had been admilted the first time on May 8, 1959, for irregular and heavy vaginal bleeding. Phys- iral examination had revealed a marked e r e
FIG. 6. Case 17. Patient M..M. Electroencephalograms taken before administration of immune gamma globulin (A and B, page 322) and after (C and D, page 323). A and B show irregular slow 5 to 7 per second bursts that arc essentially manifested bilaterally but occasionally appear alternatingly over homologous areas, namely, the frontal-central-parietal regions. During the period following cessation of hyperventilation there also appears 1 sim- ilar burst over both hemispheres that is more accentuated on the right. The over-all pattern was amsidered ab- normal with minimal bilateral dysrhythmia with slight accentuation over the left central region. C, and D show normal occipital alpha rhythms remaining intact. The slow wave formation bursts noted earlier over both hemispheres are no longer evidenced. The extent of focus narrowed down to areas, namely, the left central- frontal-temporal lobe areas. Choppy and slow activity, apparent more as an irregular base line pattern, charac- terize the noted regions, especially over the left central area. In contrast to previous tracings, these changes point toward more definite localization. The diminishing of the slow activity essentially over both hemispheres is of sig- nificance.

No. 3 IMMUNOTHERAPY OF NEOPLASTIC DISEASE IN MAN. 1. - de Cnrvalho 325
sion of the cervix that appeared to be carcinoma. On May 9, 1959, a biopsy was per- formed, and radium was inserted. The patho- logical diagnosis was Grade I1 squamous cell carcinoma of the cervix. On May 13, the pa- tient had another radium treatment, Outside of hypertro hic osteoarthritis, there was no
tient was readmitted to the hospital on Aug. 13, 1959, for panhysterectomy and bilateral salpingeoophorectomy. The pathologist found residual squamous cell carcinoma of the cervix in the pericervical area. No roentgenographic studies were made at the time. The patient entered the hospital again on Jan. 25, 1960, for colporrhaphy and ventral herniorrhaphy. There were no symptoms at this time, and there was no evidence of recurrence of the carcinoma. When she was admitted on Feb. 13, 1962, there were tender nodules that were most marked on the right thigh and leg and a smooth enlargement of the right elvic wall. An intravenous pyelogram on Fel!. 16, 1962, disclosed soft tissue density in the elvis ad-
deviation of the bladder to the left. The right upper urinary tract was not visualized. There were no evident metastases to the lumbar spine. The peripheral blood was positive for tumor cells on Feb. 22, 1962. Irregular fever persisted in spite of antibiotics. The hemo- globin dropped to 8.6 gm. per 100 cc. by Feb. 27, 1962. Antitumor gamma globulin 3, 2 ml. intramuscularly daily, was begun on Feb. 21, 1962, and by Feb. 26, 1962, the patient was free from pain, and the tender nodules on the right and left thighs had disappeared. The anemia was corrected with 1 unit of blood on Feb. 27, 1962. As of March 3, 1962, the hemo- globin was 12.3 gm. per 100 cc. Pelvic exami- nation on March 5, 1962, showed no mass of the pelvic wall and no induration or masses of the vaginal fornices or rectum. The treat- ment continues.
Case 22. D. C., a 43-year-old man, in early 1961 had complained of swelling and tightness in his left thigh of several months’ duration. Many tests were done and consultations were held with no diagnosis being derived. How- ever, in October, 1961, he developed bilateral inguinal adenopathy. One of the nodes was biopsied, and the pathological diagnosis was “anaplastic carcinoma, probably metastatic, primary source not identified.” After that, he had 2 courses of X-ray therapy and 2 courses of cyclophosphamide (Cytoxan). His condition became somewhat stable, although he had low back pain. Roentgenograms showed no chest lesion nor any bone involvement. The total proteins and the albumin to globulin ratio were within normal limits. The hemoglobin
evidence of B one lesions at this time. The pa-
jacent to erosion of the right iliac ! one and
was 12 gm. per 100 cc. The white cell count was 4,000 per cu. mm., with 50% lymphocytes and 50% segmented neutrophils. His nutri- tional status remained relatively good, even though he had lost about 23 lb. since the on- set of illness. He had occasional fever up to 101” F. On Feb. 8, 1962, bilateral axillary lymphadenopathy was apparent. He had been receiving radiotherapy to the left axilla but therapy to the right one was purposely avoided. This, the patient felt, might have undergone shrinkage and apparently it had reduced in diameter from 18/4 to approxi- mately 1 ?A2 inches or less. Another criterion of improvement was his weight. After the insti- tution of gamma globulin therapy, he showed a weight gain from 128 lb. to 135y2 lb. On the other side of the ledger, however, he de- veloped an enlarged cervical lymph node that appeared 5 days after the beginning of gamma globulin therapy. This was treated by X-ray therapy. I t must be borne in mind that he had an incision and drainage of an abscess in the lower abdomen that was apparently necrotic tumor tissue resulting from the earlier X-ray therapy. This material was cultured, and a gas-producing bacillus was recovered. It would, of course, be a possibility that this procedure gave him some stability and may have resulted in the weight gain. After 17 injections of gamma globulin, his weight consistently shows elevation. As of Feb. 24, 1962, his weight was 142 lb.; he felt well, the metastatic lesion in the right axilla had shrunk in size to five- eighths of an inch. On Jan. 17, 1962, i t had been three-quarters of an inch. He had been anemic and had been given blood transfusions a number of times. His last blood count showed a hemoglobin of 14 gm. per 100 cc. He feels well enough to return to work on a half-day schedule.
Case 23. A.C., a 60-year-old white woman, in January, 1962, had a laparotomy that re- vealed peritoneal carcinomatosis with primary tumor in the colon. There were jaundice, as- cites, low grade fever, anemia, anorexia, nau- sea, weakness, and abdominal pain. After 15 injections of horse immune gamma globulin, she feels better, the jaundice has not recurred, and the pain has disappeared. Local urticaria of 12 hours’ duration at the site of injection appeared on 1 occasion during treatment.
Case 24. G.W.M., a 53-year-old man, had adenocarcinoma of the ampulla of Vater dis- covered at operation in July, 1959. From that date up to February, 1962, he developed num- erous lymph node metastases; chemotherapy was of no avail. On Feb. 4, 1962, he started receiving antitumor gamma globulin. After 8 daily injections, his general sense of well-being

326 CANCER March 1963 Vol. 16
was better although he complained of weak- ness. T h e lymph nodes in the right axilla and the left supraclavicular area were definitely smaller than they had been 1 month earlier but they had not disappeared. The ascites was not to the early se~erely distended stage but was present in a soft, flaccid abdomen. The edema of the left thigh, which had been present, remained about the same. There was also some edema of the right thigh and lower back area. T h e patient received 5 more injec- tions at %day intervals and died suddenly with increased edema and ascites.
Case 25. M.C.K., a 55-year-old female nurse, had carcinoma of the rectum. The symptoms of rectal bleeding and watery diarrhea ap- peared in May, 1961. In July, 1961, a roent- genogram showed a constricting lesion at the rectosipoid junction. ‘This measured 4 to 5 cni. in length and had he typical appearance of annular carcinoma. Resection of the sig- m o d colon revealed adenocdrcinoma. From die date of operation to December, 1961, she waa constipated and recpired enemas to evac- uate the bowels; stools were ribbon-like and blood-streaked. There was loss of weight and complete anorexia, nausca, and pain in the lowei abdomen that required constant seda- tion. On Dcc. 30, 1961, she started receiving horse immune gamma globulin. After 8 injer- tions (1 week), there was elimination 01 necro- tic, hemorrhagic, foul material rectally. After 14 injections (2 weeks), she had no pain, and there were 2 spontaneous bowel movements a tlav of formed stools. The injection5 were then spaced at 3-day intervals. T o date (March 14, 1962), she has received 23 injections. She has gained 10 lb., her appetite has improved, though she feels very weak, arid shc maintains good bowel function. A roentgenogram shows that the lumen or the constricting lesion of the sigmoid colon has widened to 1 cm.
Case Z(i. J.Y., a 75-yenr-old man, had had symptoms dating back to June, 1961. On Oct. 18, 1961, at laparotoniy, a large tumor mass, measuring about the sin: of a man’s fist, was found in the body of the pancreas, and meta- static nodules up to 6 tm. in diameter were found in the liver. There was no resection. From the date of the operation to Ilec. 14, 1961, there was loss of weight and anorexia, nausca, and epigastric pain that required con- stant sedation. On this date there was epigas- tric prominence with tenderness on palpation. T h e liver was palpable (2 fingerbreadths), but no nodes could be felt. Roentgenograms showed an enlarged duodenal loop (Fig. 7A). Between Dec. 18, 1961, and Jan. 16, 1962, he received 28 injections of immune gamma glob- ulin. T h e roentgenograms showed that the
duodenal loop was reduced in size (Fig. 7B); the abdomen was flaccid and nontender, and no masses could be felt. The pain had de- creased but was not abolished; he required about one-quarter of the amount of sedation given previously. His appetite was improved, and the liver was not palpable. Injections were spaced from 3 to 5 days apart. He returned home and it is reported that the pain has re- sumed, with weaknesb, but there is no other evidence of recurrence. Treatment continues.
Case 27. M.O., a 29-year-old woman, had had a capsulated, well-differentiated, pelvic retroperitoneal fibrosarcoma partially removed in October, 1959. Pain, with sciatic radiation, persisted. In April, 1960, a second resection was needed to relieve the pain. This, too, did not bring palliation. Heavy sedation was re- quired; there was impairment of movement of the right lower limb, and, owing to the pain, sitting was impossible. In January, 1961, the pain increased, requiring constant seda- tion. There was anorexia, and the patient be- came emaciated. T h e mass could bc felt by vaginal examination. She was started on B3 gamma globulin 6 on Jan. 23, 1961, at 5-day intervals. After the first injection, her temper- ature rose to 101O I;. and remained thus for 4 days. On the following day, there was less pain. T h e pain declined progressively, as shown by the number of codeine tablets re- quired for sedation (Fig. 4). After 10 injections, pelvic examination revealed niarkcd reduction of the tumor mass. T h e patient could sit, walk, and move the right leg freely. She was asymp- tomatic, with increased appetite and a gain in weight until December, 1961, when a hys- terectomy was performed because of a clinical diagnosis of uterine fibromatosis. This did not reveal microscopic evidence of tumor. Injec- tions of gamma globulin have been given at 15- to 20-day intervals. She is free of pain and other symptoms as of March 14, 1962. Treat- ment continues.
T h e relationship of the administration of the gamma globulin with the decrease and clisappearance of pain is probably more sig- nificant than is the evolution of the tumor itself. An authority on these neoplasias22 gives the following views. “A growth that is so well differentiated that it resembles scar tissue may exhibit a stubborn, aggressive, infiltrative growth, procgressively invading surrounding tissues in such a fashion as to cause the loss of an extremity or even of the victim’s life if un- checked. Such growths can occur in both chil- dren and adults. They are quite unpredictable. Growth may be continuously progressive as described or may cease for periods up to 30

No. 3 IMMUNOTHERAPY OF NEOPLASTIC DTSEASE IN MAN. I. 9 de C a l m l h o 327
FIG. 7. Case 26. Patient J.Y. This patient had carcinoma of the pancreas. A, Roentgenogram of the upper gastrointestinal tract before treatment. B, After 4 weeks of treatment (reduction in size of duodenal loop).
years, only then to resume activity. After such periods of inactivity, the tumor usually main- tains the differentiation it had in the begin- ning. Such growths, if they remain well-differ- entiated, can metastasize by embolism but do so only with extreme infrequency, probably in not more than 0.5% of cancers. One must consider the possibility of metastasis if the tumor shows mitoses. These tumors are classi- fied as fibromatoses.”
Case 28. M.C., a 44-year-old woman, had had adenocarcinoma of the breast (Grade 11) diagnosed on Dec. I , 1959. On this date, there were metastases to the dorsal spine and ribs. Excision of the tumor and bilateral oophorec- tomy were performed. She was given androgens in a dose of 100 mg. for 25 doses. Radiation therapy was given on June 14, 1960. There were progressive weight loss, anorexia, anemia, and severe pain that required constant seda- tion. There was no change in the previous bone lesions and in addition there were new ones in the pelvic bones. The patient was in a wheel chair because of severe kyphosis and
back pain. On June 20, 1961, she was started on horse immune gamma globulin with the injections spaced at 3-day intervals. On Aug. 15, 1961, the radiologist reported: “The ap- pearance of the chest has not changed ap- preciably since the last examination dated June, 1960. There has been no further ad- vancement of lesions that I can see, and in fact, there may have been slight regression.” Pain was reduced to the need for 1 dose of a mild sedative per day; the patient could walk. She did not receive treatment until November, 1961, when new bone lesions appeared in the ribs and pelvis, with pathological fractures and increased pain. Nine more injections of gamma globulin were given, after which the radiologist reported “some slight filling in near the fracture (rib). No remarkable change is seen, however. There is evidence of callus and new bone formation. There is more callus and new bone formation around the pathological fracture of the pubis on the right. There may be also some filling in on the ischium. The pelvis is otherwise unchanged.” Again, the pain was greatly reduced. The treatment was unintentionally discontinued, and 1 month

CANCER March. 1963 Vol. 16 3 28
later, all of the bone lesions showed signs of progression. The pain and the associated symp- toms had resumed. The patient was not avail- able for further treatment.
Case 29. R.O., a 54-year-old white man, had had increasing epigastric pain, vomiting, and loss of weight for 3 or 4 months. On Feb. 16, 1960, a segmental jejunal resection, duodenal jejunostomy, cholecystec tomy, appendectomy, and gastrostomy were performed. Pathological study revealed adenocircinoina of the jeju- num within 4 cm. of the ligament of Treitz. Symptoms that were typical of upper small bowel obstruction recurred. On Sept. 19, 1960, segmental jejunostomy with resection of part of the tail of the pancreas in continuity and end-to-end anastomosis of the duodenum and jejunum were performed. The pathology re- port was “recurrent jejunal adenocarcinoma and duodenal ulcer.” On Oct. 5, 1960, there W;IS adhesion lysis, and masses in the small in- testinal mesentery and the gastrojejunostomy were biopsied. The biopsy specimen was re- ported to show fat necrosis. On Feb. 31, 1961, a laparotomy disclosed metastases to the mesentery of thc small bowel with involvement of the superior mesenteric artery and vein. No resection was performed. X-ray therapy was given (4,000 r with a Co@O unit with pendu- lum-type distribution). Cytoxan, 50 mg. twice daily, was also given. Pain continued, and on Feb. 27, 1961, a bilateral splanchnic block, us- ing eucupine oil, was performed. Re-evaluation on Feb. 22, 1961, showed him to be in good condition and with ncl evidence of diseasc. Roentgenograms of the bowel revealed no de- formity of the duodenal loop. On Aug. 2, 1961, because of recurrent pain and a ques- tionable retroperitoneal mass shown on roent- genogram, 3,000 r of radiation was given. On Oct. 6, 1961, roentgenograms showed a mid- line mass, 7 ~ 7 . 3 cm., opposite the second lum- bar vertebra. The beginning of bone destruc- tion of the vertebra was noted. On Oct. 10, 1961, the first of 10 treatments with cobalt therapy to the spine was given. On Jan. 12, 1962, he had constant pain radiating to the back, tenderness of the upper abdomen, in- ability to sleep at night, and loss of weight (15 lb. in the previous 2 months), and anorexia. Physical exatnination revealed marked tender- ness in the epigastrium but no masses. There was definite tenderness over the tenth dorsal vertebra. There was roentgenographic evi- dence of degenerative changes in D9 and DIO (thought by the radiologist to be metastatic disease). Beginning on Feb. I , 1962, he re- ceived 2,500 r daily for 5 days to his back through a 10~15-cm. port. The patient felt better after the therapy but still had slight tenderness. On Jan. 12, 1962, he was started
on 2 ml. daily of antitumor 1,2 gamma globu- lin 2. At the beginning of therapy, the hemo- globin was 10.1 gm. per 100 cc., and the serum glutamo transaminase was 33 units. One unit of whole blood was given on Jan. 16, 1962, raising the hemoglobin to 11.7 p. per 100 cc., but i t continued to fall, and there was a per- sistently high erythrocyte sedimentation rate of 50 to 62. The blood was positive for tumor cells on Jan. 16, 1962. The serum glutamo transaminase value rose to 53 units on Jan. 20, 1962, and, on Jan. 26, 1962, the stool was positive for blood, with a drop in the hemo- globin to 9.8 gm. per 100 cc. Another unit of whole blood was given. Coombs’s tests, direct and indirect, were negative on Feb. 8, 1962, but the hemoglobin dropped to 10 gm. per 100 cc., and 1 unit of packed cells was given. The erythrocyte sedimentation rate continued to be high. There was some diminishment of the pain but this varied from day to day. Anti- tumor 1 gamma globulin 2 (1 ml. a.m. and 2 ml. p.m.) was begun on Jan. 20, 1962, with no marked objective improvement. On Feb. 2, 1962, antitumor gamma globulin 1 (2 ml. every 2 days) was begun. The abdominal and back pain were considerably less, requiring less sedation. On Feb. 26, 1962, there were in- creased abdominal pain, loss of weight, and vomiting. The hemoglobin was 9.5 p i . per 100 cc., and the pain was most severe 2 hours after eating. The patient was started on anti- tumor gamma globulin 4 , 2 ml. twice daily. On the fifth day of therapy, the patient started passing streaks of blood in the stool. The pain had increased in intensity in the cpigastrium. On the seventh day of therapy (March 5, 1962), the abdominal pain had decreased, and roentgenographic studies of the upper gastro- intestinal tract on March 6, 1962, were sug- gestive of a decrease in the tumor mass. Epi- gastric fullness and tenderness had also decreased. The stool was positive for occult blood on March 7, 1962. Beginning on Feb. 28, 1962, the patient had received 1 unit of albumin daily, or 7 units up to March 7, 1962. His appetite improved and activity in- creased. Complaints, particularly of pain, varied from day to day. In general, no definite clinical improvement has been shown, al- though the treatment has been prolonged far beyond the average time by which most of the other patients had registered benefits of some kind. The negative results in this case may il- lustrate the lack of immunological cross re- action between this rare tumor not included in the antigen cocktail and other tumors of the gaftrointestinal tract that were included.
Case 30. M.R., a 70-year-old man, had had a left nephrectomy in March, 1961, for renal cell carcinoma. There had been progressive

No. 3 IMMUNOTHERAPY OF NEOPLASTIC DISEASE IN MAN. I. * de Carvalho 329 deterioration and a weight loss of 80 lb. since the operation. In November, 1961, he noticed reddish, fleshy skin lesions of the right occiput, face, chest, and back. In December, 1961, there was increased erythema of the left upper arm, with tenderness and pain and increased in- ability to use the limb. There was progressive edema of the arm. He had had intermittent hemoptyses and dyspnea for the preceding 8 to 10 months. Roentgenograms on Jan. 21, 1962, revealed emphysema and numerous sharply delineated densities of both lung fields with bilateral pleuritis. On Feb. 13, 1962, these same lesions were noted to be increasing in size. The left humerus showed extensive de- struction of the entire distal half of the shaft with complete destruction of the bony cortex. From Jan. 27, 1961, until March 7, 1962, he received 32 injections of antitumor 1 gamma globulin. The pain in the right shoulder dis- appeared on the fifth day of thera y. After the
gram of the left arm showed “melting” of the tumor. Oxygen therapy was discontinued after 10 days of treatment because of improvement in breathing. The skin lesions became sharply demarcated and progressively darker in color. They became necrotic and hemorrhagic and 2 of them sloughed off completely without ul- ceration of the skin. Hemoptysis continued but was less intense. Because of the patient’s bel- ligerence and refusal to accept any more injec- tions, the last 10 doses of gamma globulin were incorporated into 20 ml. of milk and given orally.19 A roentgenogram of the chest now shows reduction in the lung lesions, particu- larly on the right side. Medication for pain has been reduced from injections of dihydro- morphinone hydrochloride (Dilaudid Hydro- chloride) every 4 hours to codeine, 2 gr. twice daily as demanded by the patient. He has re- fused to continue treatment.
Case 31. H.C., a 70-year-old woman, noticed a mass in her left breast in 1959. She received no treatment until March, 1962, when the mass became a large scirrhous inflammatory tumor. At ihis time, there were enlarged cervi- cal, axillary, and supraclavicular lymph nodes, the latter the size of a Ping-pong ball. There were also osteolytic lesions on the dorsal verte- brae. She had considerable pain. On March 3, 1962, she started receiving antitumor 1,2 gamma globulin 4 in a dose of 2 ml. intra- muscularly daily. On March 6, 1962, she was free of pain. On March 8, the supraclavicular lymph node was barely palpable, the inflam-
sixth day of treatment a rechec kp roentgeno-
matory reaction had “blanched out.” The breast was softer, and there was some retluc- tion of the size of the cervical and axillary lymph nodes.
SUMMARY
Hyperimmune gamma globulins were pre- pared from the serums of animals receiving purified antigens from a variety of cancer and leukemic tissues. These antigens were sepa- rated from normal antigens by precipitation of the latter by antibodies against normal tis- sues. Several batches of these horse and donkey gamma globulins with titers ranging from 2-2 to 24 were administered to 15 leukemia and 16 cancer patients.
Of 15 leukemia patients, 11 had previous hormone and chemotherapy that had resulted in remissions of different degrees and duration in 7. Thirteen of these patients had remissions on immune gamma globulin lasting from 4 weeks to 29 months. Among these were some with no previous treatment and some who had had no remission on chemotherapy.
In the group of 16 cancer patients, a nearly constant feature was the alleviation of pain, partial or complete recovery of functions im- paired by the neoplastic growth, and partial or complete clearance of objective tumor le- sions. These benefits have lasted from 2 weeks to 11 months and were observed in 15 patients. Side effects included mild inflammatory reac- tions at the place 01 injection and a slight ele- vation of temperature.
ADDENDUM
Inevitably in a preliminary report such as this, advances and changes from the time of acceptance to the time of publication have made the results here presented outdated. Wide exploration of dosage, schemes of admin- istration, intravenous, oral, intracavitary, and intraluminal routes and of means of sup- pression of hypersensitivity reactions now encountered, have led to new results both in leukemia and in solid tumors. These will be the subject of a paper under preparation.
As of Jan. 12, 19663, there have been no signs of recurrence in case 2 (LK38); in case 7 (LK48) there is still remission.
(For references see following page.)

330 Vol. 16
1. ALADJFM, F.; MAcLARF.~., W. R., antl CAMPBELL, 1). H.: Skin-scnsitizing activity of gloliulin fi-actions from rabbit immune scrnnis. Scieiace 125: GX2-634, 19557.
2. BLRMAN, L.: Personal ci~mmrn~ication, 1959. 3. BJ~KKLUND, R.: Antigenicity of malignant and nor-
nial human tissues by gel cliffusion techniques. Intrrnaf. Arch. Allrrgy 8: 179-192, 1!356. 1. BRADA, Z.: Study of tumour-host relationship; part
I, 011 interrelation between haeinoglobin concentration and tumour growth. hTeog lmm 6: 132-137, 1959.
5. CALARESU, F.; SrumIER, W., and SmwArcrz, S. 0.: Studies in leukcmia; V, aiiitigenic differences between leukemic and non-leukemic red blood cells. J . Lab. C- C l h . N e d . . iX: 102-107, 1956.
6. COLLARORATION GROI!P FOR EVALL'A~~ON OF EQUINE I M ~ I I I N E G A ~ ~ I I A CI.OHCU,IK: Yrorcrtlings of first meet- ing. Unpublished.
S.: T..eukemia in infant born of mother with lenkemia. Se719 England .7. Med. 259 727-729, 1!68.
8. DLCARVALHO, S.: Segregation of antigcns from hu- man lenkemic and tumoral cells hv fluorocarbon ex-
7. CRAX1III.F1"I., H. G.; FRIFIl\.(AN, J. L., ;Ind N A J J A R .
iraction; I, detection by gcl diffusion mcthod. J. L n D . 2 Clin . Xd. 56: 333-341, 1960.
9. D~CARVALHO, S., and RAND, H. J.: Effects of iso- and hetcro-antibodies against specific antigens of trans- plant ablc Novikoff hepatoma of rat (solid form). hJa- t ior , London 195: 950-952, 1!362.
10. DFCARVALHO, S.; RANI), H. J., antl UHRICK, J. R.: IXfferences in information ton tent of ribonucleic adds from malignant tissues and homologou3 organs as ex- pressed by their biological activities. Exper. & Molec.
11. DFCARVALHO, S.; T T ~ ~ ~ ~ ~ , J., and RaND, H. J.: Diffusion of antigen into antibody-charged agar in \\'introhe hematocrit tubcs accelerated by centrifuga- tion. A'nturc. Z.ondon 194: 1275-12i6. 1962.
I?. HAYS, E. F.: Effect of acqu~icd immunologic tol- erance on development of leukemia. Blood 19: 454- 459. l'JYj2.
IS. K~RIWOLD. I..: Distribution and imrnunochemi-
Z ' c ~ t h . I : 96-103, 1962.
cal properties of human tissuc and tumor antigens. Ann. New York Acad. Sc. 69: 681-697, 1957.
14. MATHB, G.; TRAN BA Loc, and BERNARD, J.: Effet sur la leucCmie 1210 de la S80itris d'une conibinaison par diazotation d'A-methopterine et de y-globulines de hamsters porteurs de cette lenckmie par hPtkrogreffe. Cornlh rend. Acad. Sc. 246: 1626-1628, 1958.
15. MILLER, J. F. A. P.: Etioiogv and pathogenesis o f mouse leukemia. Advances Canker Res. 6: 291-368, 1961 .
16. MOORE, G. E.: Future of cancer chemotherapy. Zn Cancer Chemotherapy Reports, No. 16. Rethesda, Md. Cancer Cheniothcrapy National Service Center.
17. OSLFX, A. G.: Functions o f complement system. Advances Zrnmzmol. I : 131-210, 1961.
18. OUCFITF.KI.OKY, 0.: ilnt.igen-antibody reactions in gels. Ark. kenzi mineral. o. g d . 26-B (14): 1-9, 1948- 1949.
19. SABIN. A. R.. and FIEI.nSTEEL, A. H.: .Intipolio- inyelitic activity of human and bovine colostrum and milk. Pediatrics 29: 105-115, 1962. 20. SOUTHAM, C. M.: Relationships of immunology
to cancer: review. Cancer Res. 20: 271-291, 1960. 21. SOUTIIAM, C. M.: Applications of immunology t o
clinical cancer; past attempts and future possibilities. Cancer Res. 21: 1302-1916, 1%1.
22. SToirr, A. P.: Sarcomas of soft tissues. Cn 11:
23. 'I'RIJFELLI, T.: Pcrsonal communication. 1961. 24. WOOD, S.: Personal communication, 1962. 25. ZILRER, L. A.: Specific tumor antigens. Advanre.\
1962; pp. 589-591.
210-231, 1961.
Cancer Res. 5 : 291-329, 1958.
ADD I '110N A L KI-F F.RI:N C 1;.
26. I)L:CARVAI.HO, S.; RAND, H. J., and ASIII)\-, $1.: In vitro properties of a specific heterologous anti- leukemic and anti-tunlor cytotoxic antibody and thcii- bearing nn its application in vivo. Exper. 2 ilfoler-. Path. In press.