pregnancy physiology
DESCRIPTION
By Dr Steve HallworthTRANSCRIPT
Physiology of Pregnancy
Dr Stephen Hallworth, Consultant Anaesthetist
Royal London Hospital
Physiological Changes of Pregnancy
Airway
Breathing
Circulation
Gastrointestinal
Haematological
Endocrine
Pregnancy
Most physiological adaptations have a purpose
Most adaptations occur in advance of the need for them
Respiratory System- Airway
Capillary engorgement of upper airway
Exacerbated by: URTI
Fluid Overload
PET / Eclampsia
Occasionally severe UAO
Large tongue + breasts
Significance for the Anaesthetist 1
Extreme care with : manipulation of airway
suctioning
use of airways
laryngoscopy
Anticipate difficult intubation
Use smaller COTT due to glottic oedema
UAO may occur early after induction
2000
4000
Vol[ml]
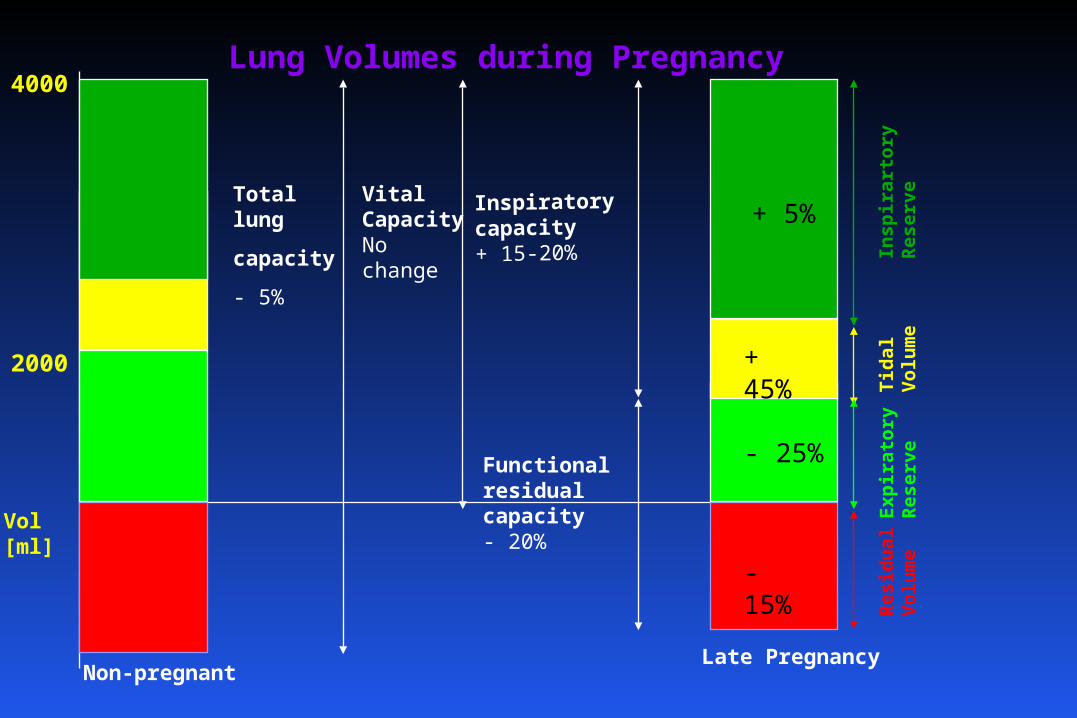
VitalCapacityNochange
Non-pregnantLate Pregnancy
Insp
ira
rto
ry
Res
erve
Tid
al
Vo
lum
eE
xpir
ato
ry
Res
erve
Res
idu
al
Vo
lum
e
Inspiratorycapacity+ 15-20%
Lung Volumes during Pregnancy
Total lung
capacity
- 5%
+ 45%
- 25%
- 15%
+ 5%
Functional residual capacity- 20%
Respiratory System- BreathingOther Variables
Respiratory rate / / Airways resistance - 50%
Physiological dead space ??
FEV1 and FEV1 / FVC unchanged
Chest wall compliance - 45%
Lung compliance unchanged
Total compliance - 30%
Respiratory System- BreathingMinute Volume
45% increase in MV
Progesterone oestrogen effect
Direct effect on respiratory centre
Increased sensitivity to respiratory centre to CO2
Increased level of carbonic anhydrase B in RBCs
Also due to increased CO2 production
Respiratory System- BreathingMinute Volume
Non-pregnant state: Increased ventilation by 1.5 L/min for each
1mmHg PaCO2 rise
Pregnant state: Increased ventilation by 6 L/min for each
1mmHg PaCO2 rise
Oxygen consumption Oxygen consumption + 15 - 20%
40 ml / min increase
Due to BMR
work of breathing
fetus
uterus
placenta
cardiac work
Respiratory System - BreathingOxygen tensions
In 1/3 to 1/2 of women at term airway closure occurs
during normal tidal breathing when supine
PAO2 : PaO2 gradient 2 kPa sitting
3 kPa supine
PaO2 due to PaCO2 + AVO2 difference
Respiratory System - BreathingCarbon dioxide tensions
Mixed venous PCO2 1 kPa less than non-pregnant level
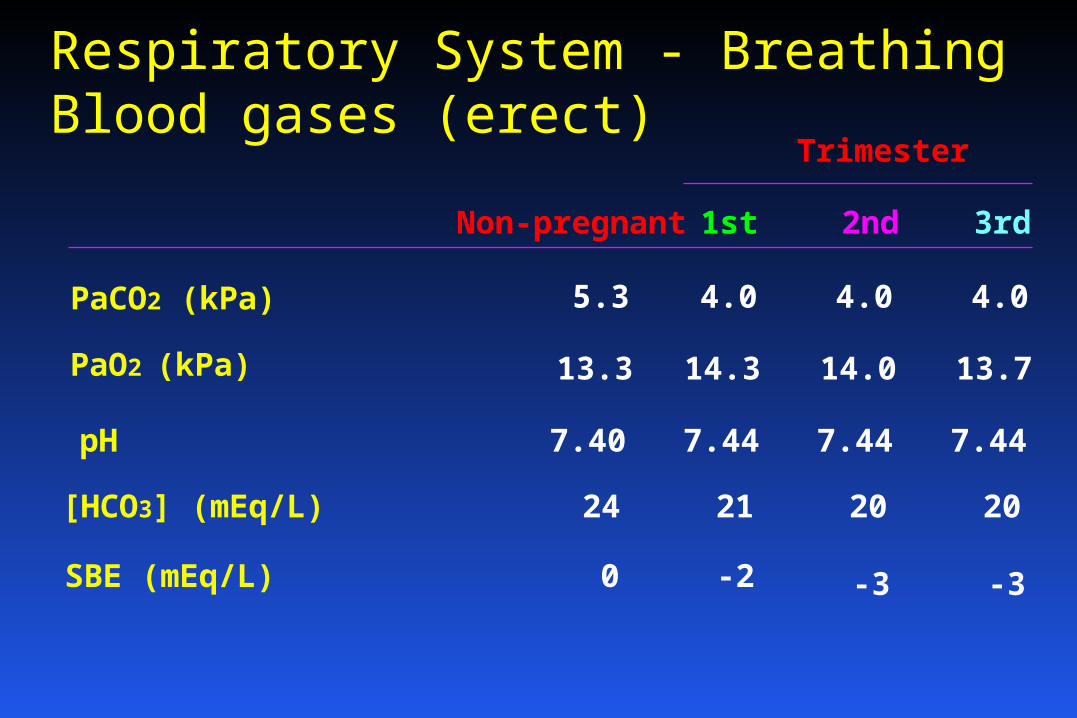
Respiratory System - BreathingBlood gases (erect)
Trimester
1st 2nd 3rdNon-pregnant
PaCO2 (kPa) 5.3 4.0 4.0 4.0
PaO2 (kPa) 13.3 14.3 14.0 13.7
pH 7.40 7.44 7.44 7.44
[HCO3] (mEq/L) 24 21 20 20
SBE (mEq/L) 0 -2 -3 -3
Respiratory System - BreathingHaemoglobin dissociation curve
Shifted to the right
P50 increases from 3.6 kPa to 4.0
U
T
E
R
O
P
L
A
C
E
N
T
A
L
C
I
R
C
U
L
A
T
I
O
N
Um
bilica
l arte
ry Um
bili
cal v
ein
Ute
rine a
rtery
Ute
rine v
ein
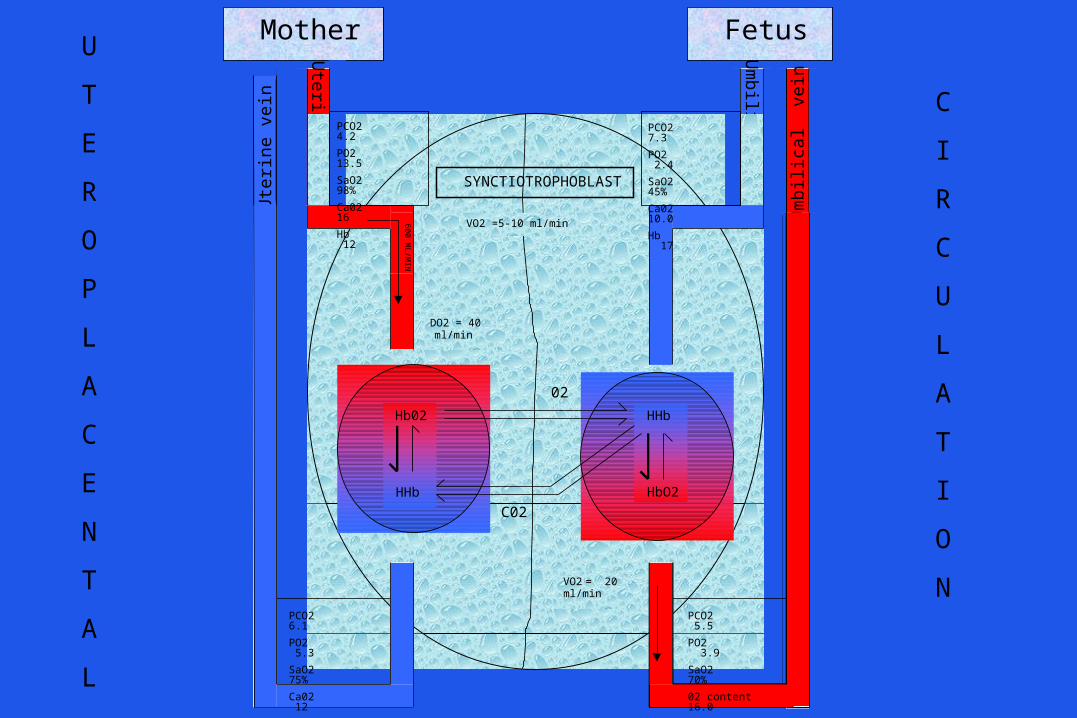
Mother Fetus
Hb02
HHb
HHb
HbO2
SYNCTIOTROPHOBLAST
60
0 M
L/MIN
02
VO2 =5-10 ml/min
DO2 = 40 ml/min
VO2 = 20ml/min
PCO2 7.3
PO2 2.4
SaO2 45%
Ca02 10.0
Hb 17
PCO2 4.2
PO2 13.5
SaO2 98%
Ca02 16
Hb 12
PCO2 6.1
PO2 5.3
SaO2 75%
Ca02 12
PCO2 5.5
PO2 3.9
SaO2 70%
02 content 16.0
C02
Significance for the Anaesthetist 2
Rapid maternal desaturation following induction for GA (10 kPa / min faster than non-pregnant)
Pre- O2 for 5 mins recommended
Avoid aortocaval compression at all times
Epidurals may prevent fetal hypoxaemia during labour
Cardiovascular SystemHeart position
Pushed upwards and forwards
AB 4th intercostal space
Gives impression of cardiac enlargement on CXR
But - it is enlarged by ~ 12% (70 - 80 ml)
Cardiovascular System / Heart sounds
1st: Louder & exaggerated splitting
2nd: Not affected
3rd: Heard loudly in majority
4th: Detected by phonocardiography in ~16%
Early- to mid-systolic ejection in most at LS
Diastolic murmurs also fairly common due to tricuspid flow murmur
Cardiovascular SystemECG
LAD (15%)
Flat Ts / inverted in III
Atrial / ventricular ectopics
Cardiovascular SystemCardiac output
25% by 13/40
50% by 20/40 to term ~ 2 L / min (e.g 4.5 - 6.5)
20% in heart rate ~ 15 bpm (e.g 70 - 85)
13/40 until term
20% in stroke volume ~ 12 ml (e.g 64 - 76)
Cardiovascular systemRegional blood flow
Uterus 500-600 ml (+ 400%)
Kidney 400-500 ml (+40%)
Skin 500-600 ml (+150%)
Other 300-600 ml
Cardiovascular systemBlood pressure
No change in SBP
20-25% in DBP at 20/40 (normal at term)
Cardiovascular systemTotal peripheral resistance
~ Must
~ 1000 dyne / sec / cm-5 at 20/40 (35% )
~ 1300 dyne / sec / cm-5 towards term (20% )
Cardiovascular systemVenous pressures
No change in CVP / RA / arm veins
2.5 in femoral / IVC / leg veins at term
Causes: weight of uterus on iliacs / IVC
pressure of fetal head on iliacs
hydrodynamic obstruction
Cardiovascular systemSupine hypotensive syndrome
From 20/40
Majority of women placed in supine position at term get a 30-50% in CO but don’t become hypotensive due to TPR
10% get a 30% in SBP
A / w RAP / CO / MAP
Cardiovascular systemOedema
Pedal oedema in 40% of normotensives
Colloid osmotic pressure 22 mmHg at onset of labour and 16 mmHg 6 hr post delivery
Non-cardiogenic pulmonary oedema can occur at 13-16 mmHg
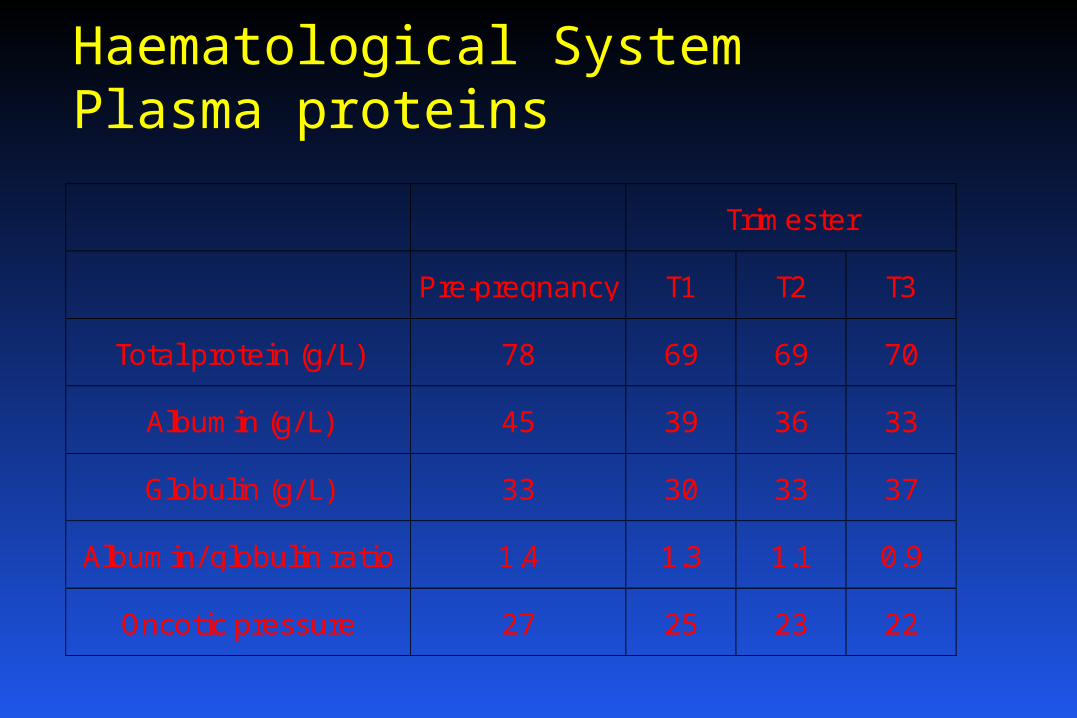
Haematological SystemPlasma proteins
Trimester
Pre-pregnancy T1 T2 T3
Total protein (g/ L) 78 69 69 70
Albumin (g/ L) 45 39 36 33
Globulin (g/ L) 33 30 33 37
Albumin/ globulin ratio 1.4 1.3 1.1 0.9
Oncotic pressure 27 25 23 22
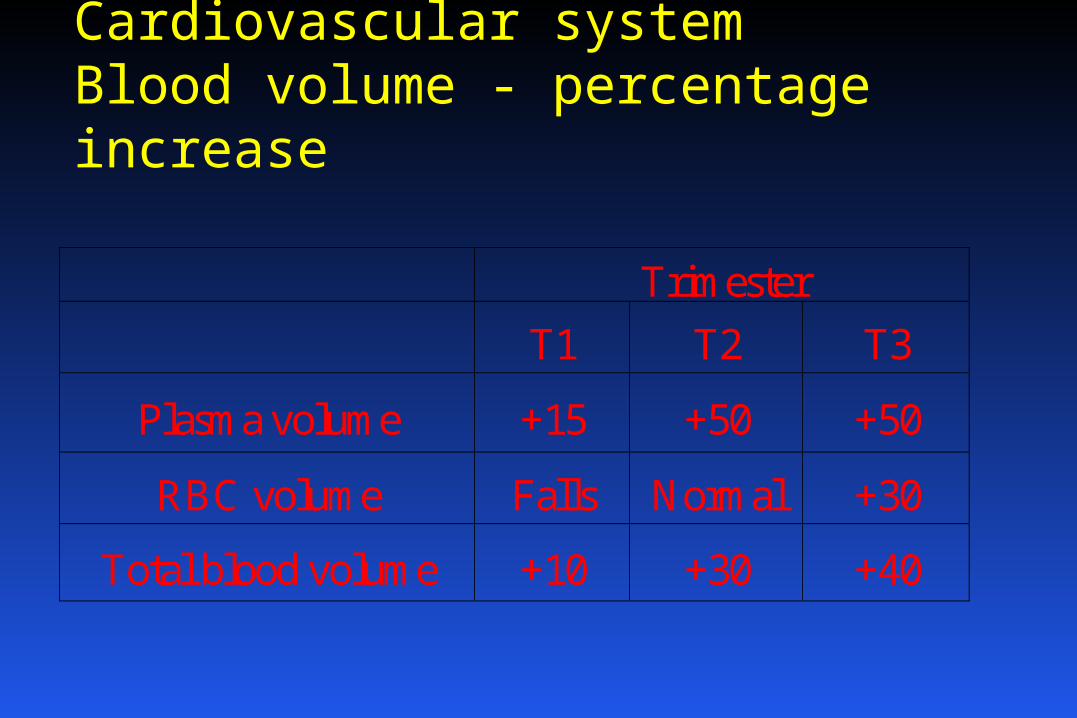
Cardiovascular systemBlood volume - percentage increase
Trimester
T1 T2 T3
Plasma volume +15 +50 +50
RBC volume Falls Normal +30
Total blood volume +10 +30 +40
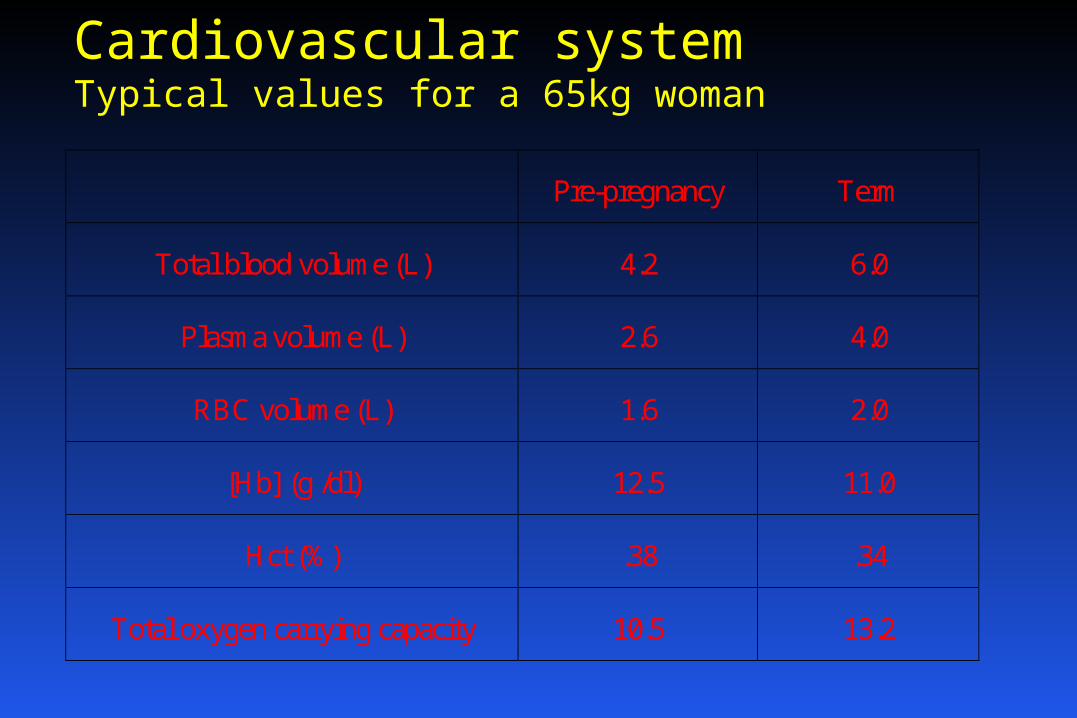
Cardiovascular systemTypical values for a 65kg woman
Pre-pregnancy Term
Total blood volume (L) 4.2 6.0
Plasma volume (L) 2.6 4.0
RBC volume (L) 1.6 2.0
[Hb] (g /dl) 12.5 11.0
Hct (%) .38 .34
Total oxygen carrying capacity 10.5 13.2
Significance for the Anaesthetist 3
Hypervolaemia allows for moderate blood
loss at delivery
Avoid aortocaval compression
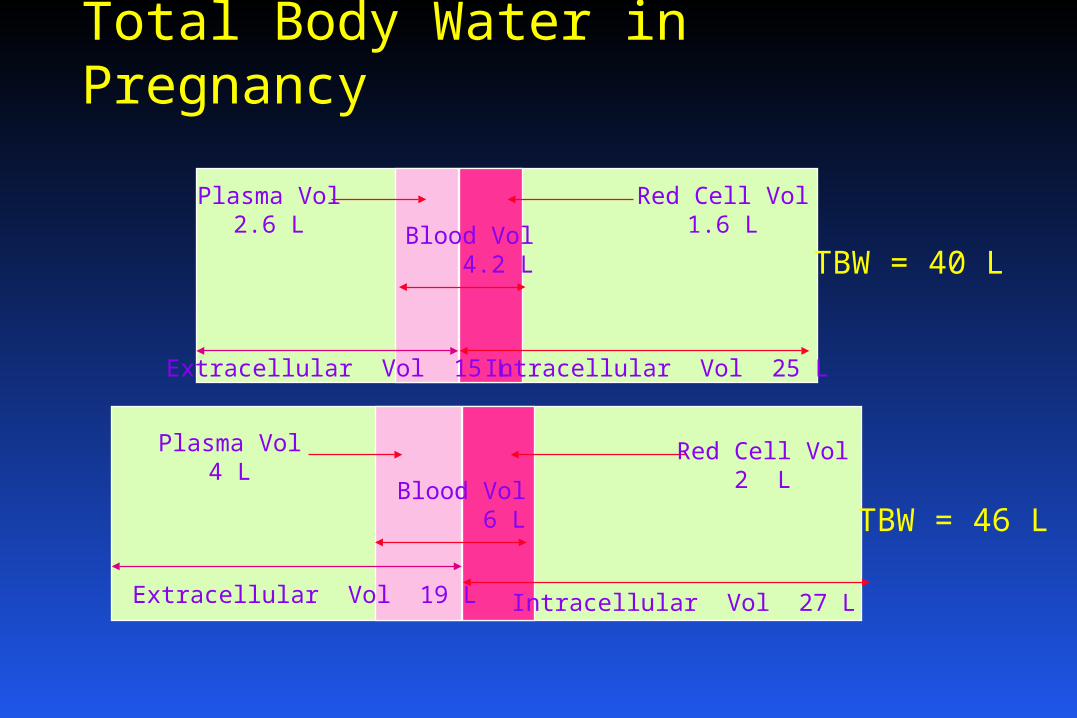
Total Body Water in Pregnancy
Red Cell Vol1.6 L
Plasma Vol2.6 L
Intracellular Vol 25 LExtracellular Vol 15 L
Blood Vol 4.2 L
Red Cell Vol2 L
Plasma Vol4 L
Intracellular Vol 27 LExtracellular Vol 19 L
Blood Vol 6 L
TBW = 40 L
TBW = 46 L
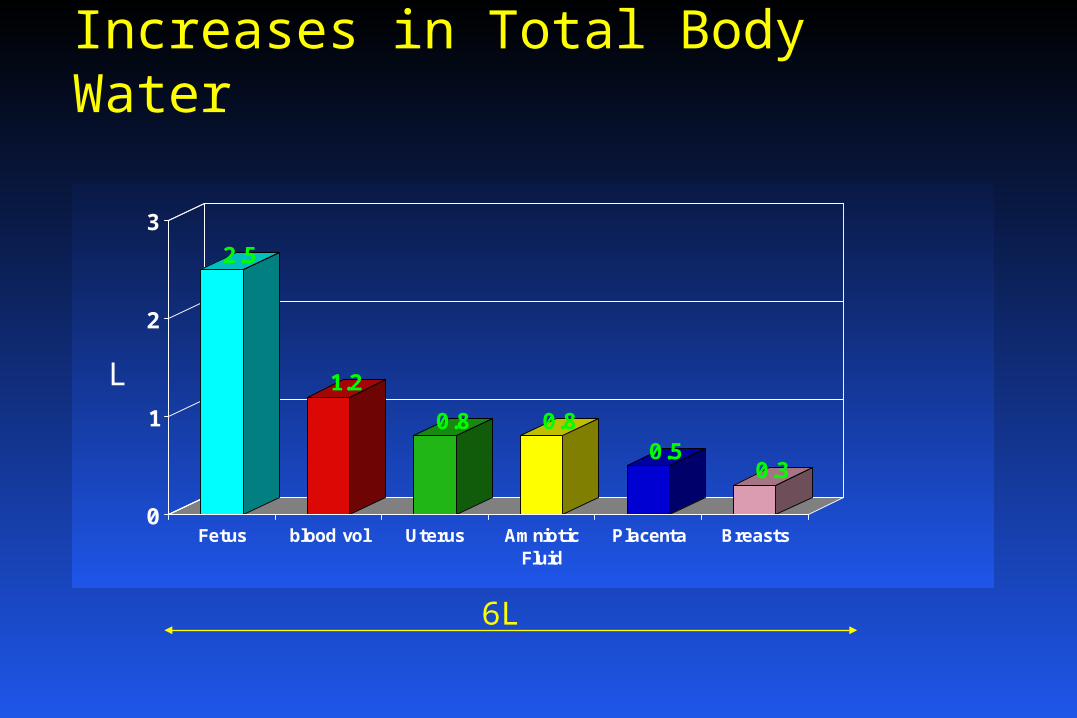
Increases in Total Body Water
2.5
1.2
0.8 0.80.5
0.3
0
1
2
3
Fetus blood vol Uterus AmnioticFluid
Placenta Breasts
L
6L
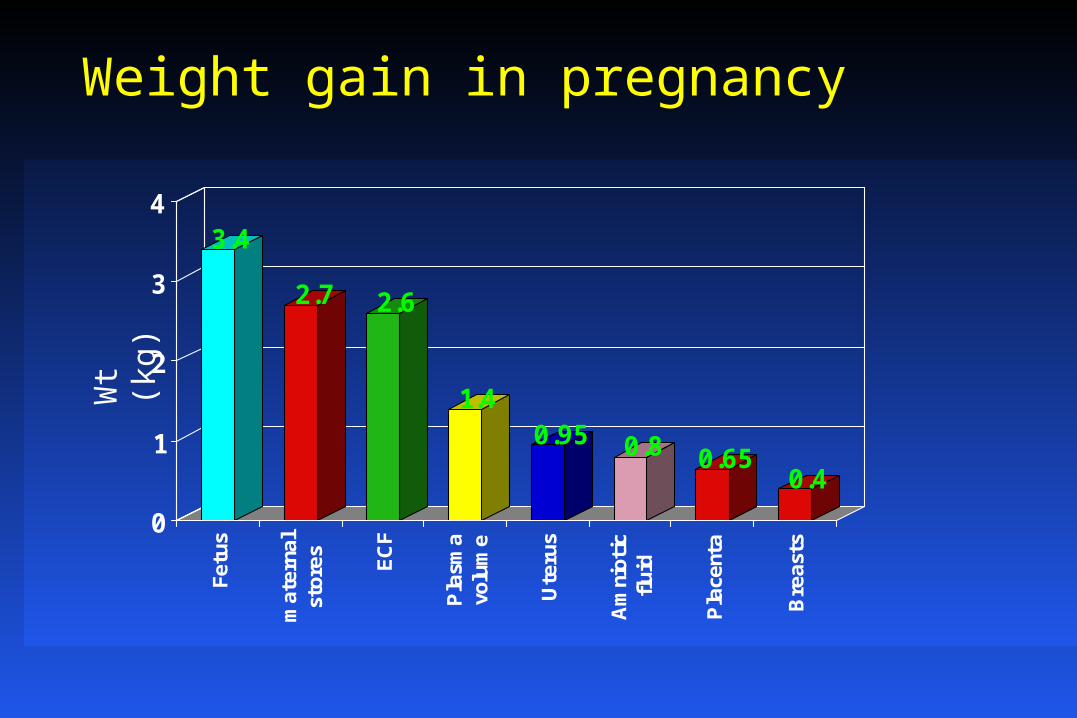
Weight gain in pregnancy
3.4
2.7 2.6
1.40.95 0.8 0.65
0.4
0
1
2
3
4Fe
tus
mat
erna
lst
ores ECF
Pla
sma
volu
me
Ute
rus
Am
niot
icflui
d
Pla
cent
a
Bre
asts
Wt
(kg
)
Genito-urinary system
~ 50% in RBF
~ 50% in GFR
~ 40% in [creatinine]
Glycosuria (1-10 g/d)
Proteinuria 300 mg/d
UTIs common
Osmoregulation during pregnancy
Plasma osmolality to 280 - 290 mosmol / kg
No decrease in ADH secretion
Decrease in thirst threshold
Fluid ingestion > diuresis
Gastrointestinal systemStomach Stomach displaced upwards
changes angle of GO junction
reflux (in 50 - 80%)
progesterone
gastrin and pepsin
No difference in gastric volumes > 25ml *
No difference in gastric pH< 2.5*
* relative to non-pregnant women
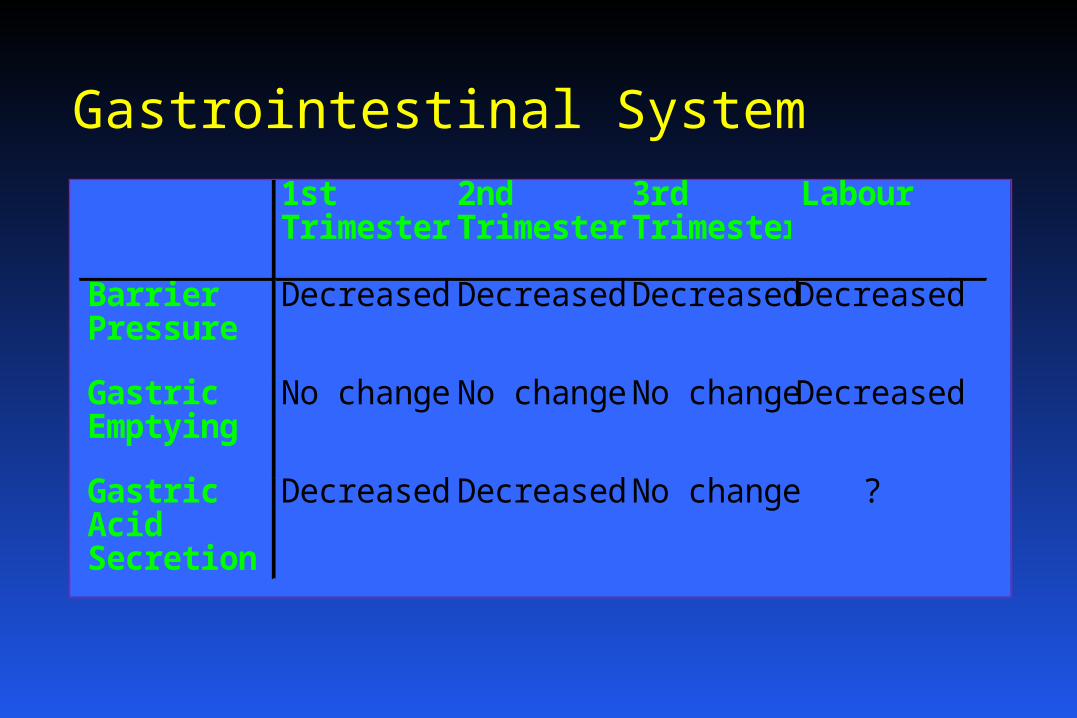
Gastrointestinal System
1stTrimester
2ndTrimester
3rdTrimester
Labour
BarrierPressure
Decreased Decreased Decreased Decreased
GastricEmptying
No change No change No change Decreased
GastricAcidSecretion
Decreased Decreased No change ?
Dept of Obstetric Anaesthesia / Royal Free Hospital
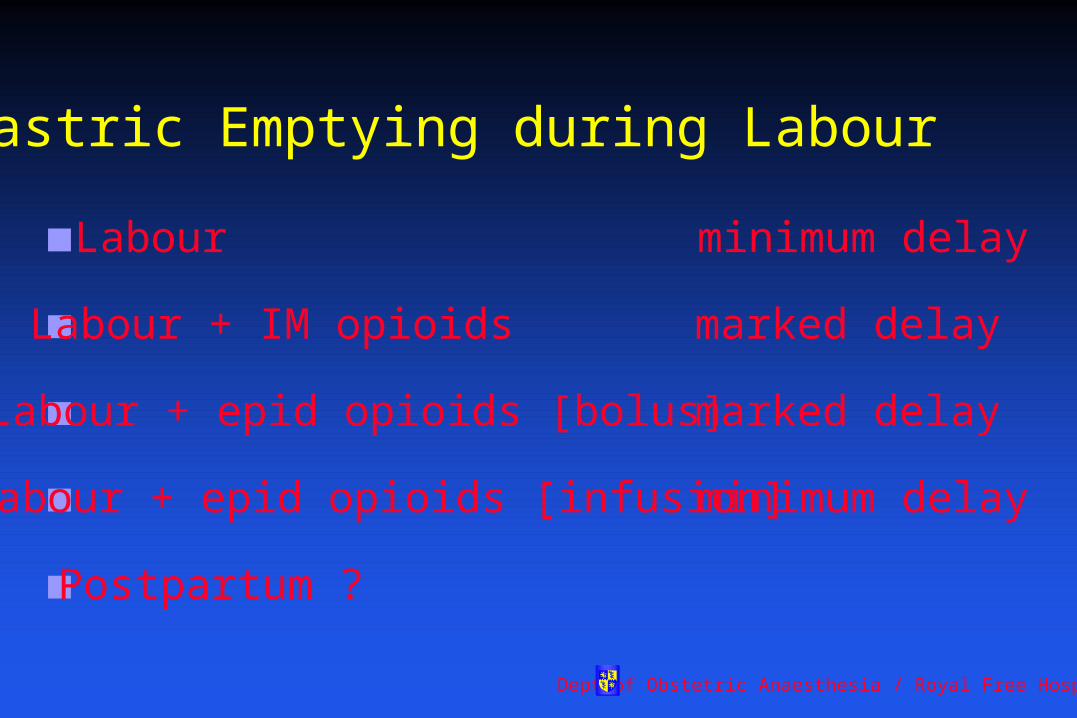
Gastric Emptying during Labour
Labour minimum delay
Labour + IM opioids marked delay
Labour + epid opioids [bolus] marked delay
Labour + epid opioids [infusion] minimum delay
Postpartum ?
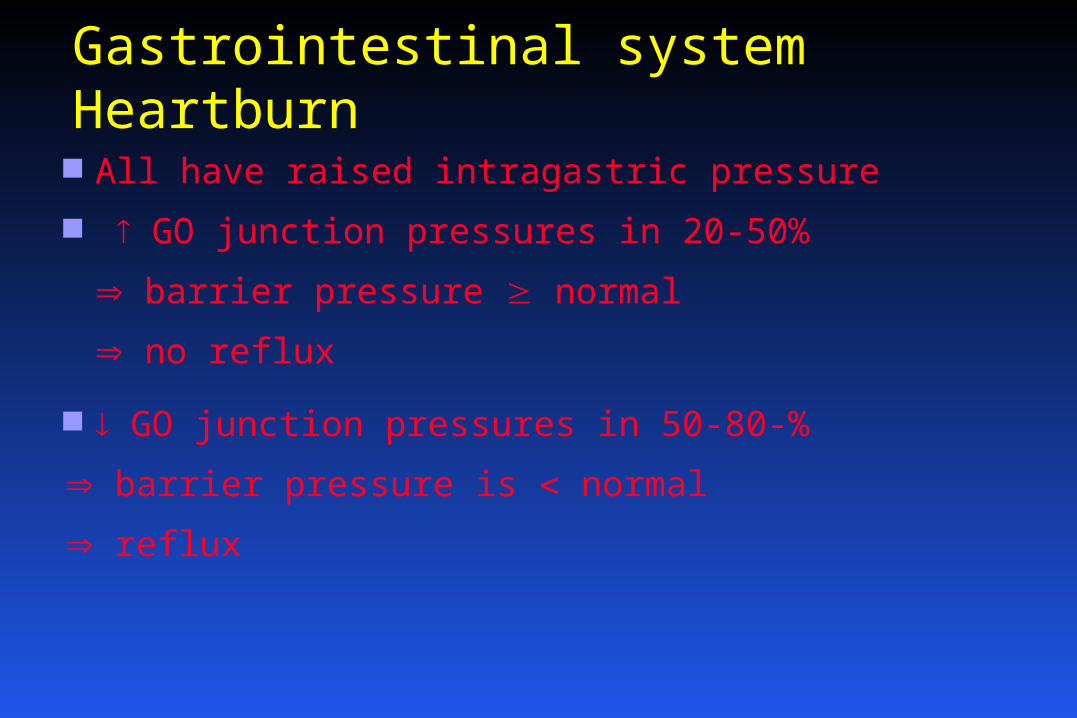
Gastrointestinal systemHeartburn All have raised intragastric pressure
GO junction pressures in 20-50%
barrier pressure normal
no reflux
GO junction pressures in 50-80-%
barrier pressure is normal
reflux
Gastrointestinal systemAcid aspiration prophylaxis
?? Need
Sodium citrate
H-2 antagonist
Metoclopramide
RSI / cricoid pressure
Gastrointestinal systemLiver and bowel
Normal hepatic blood flow
bilirubin / ALT / AST / LDH
gallbladder emptying / gallstones
intestinal motility / constipation
Nonplacental endocrinology
Thyroid total T3 and T4
Normal free T3 and T4
Adrenal cortex 200% in free / total cortisol
Pancreas tissue sensitivity to insulin
GTT
fasting [glucose]
ketosis
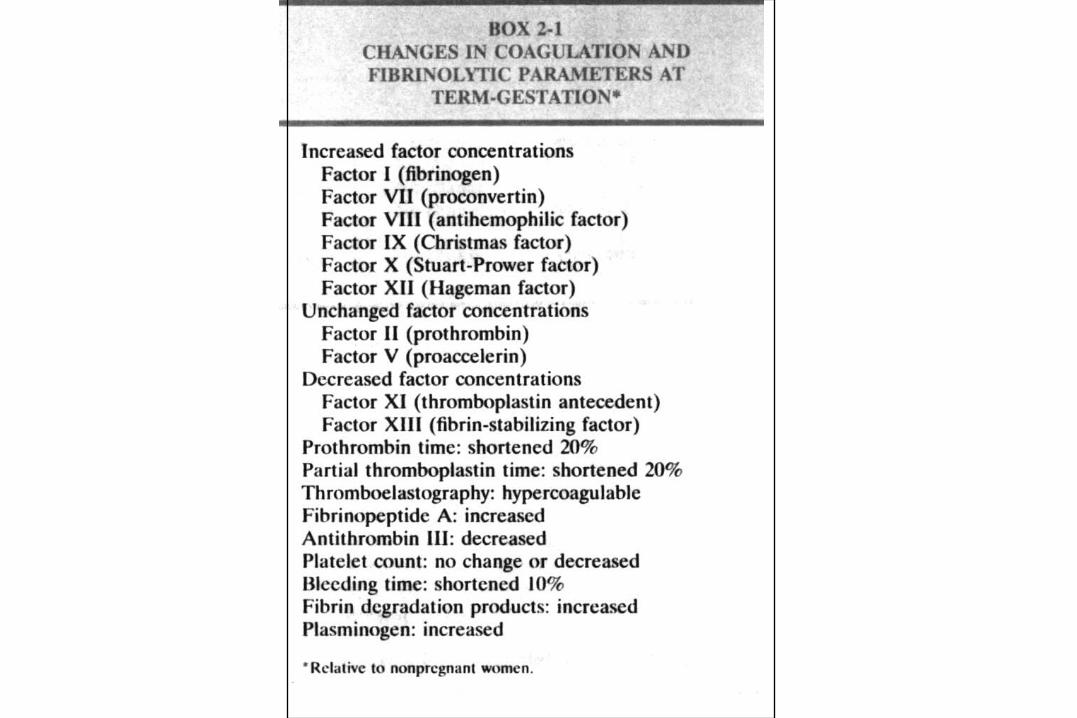
Haematological SystemClotting
20% reduction of PT and PTTK
fibrin deposition (esp. uteroplacental circulation)
Fibrinolysis ( FDPs)
Platelets 15%
Haematological SystemWhite cells
PMNs (max at 30/40)
Lymphocyte count normal
cell-mediated immunity
Normal humoral immunity
Conclusion
Pregnancy is associated with multiple
physiological adaptations
Clinical implications for the anaesthetist
Avoid the supine position / think laterally