predicting surgical compliance in a cohort of women with trichiasis
TRANSCRIPT
International Ophthalmology 18:105-109, 1994. 105 @ 1994 KluwerAcademic Publishers. Printed in the Netherlands.
Section: Geographical ophthalmology
P r e d i c t i n g s u r g i c a l c o m p l i a n c e in a c o h o r t o f w o m e n w i t h t r i ch ias i s
Sheila West, 1 Matt Lynch, 1 Beatriz Munoz, a Sidney Katala, 2 Scan Tobin ~ & B.B.O. Mmbaga 2 1 Dana Center for Preventive Ophthalmology, Johns Hopkins School of Medicine. 2 Central Eye Health Foundation, Dodoma, Tanzania
Accepted 26 March 1994
Key words." trichiasis, trachoma, chlamydia infection-ocular
Abstract
Trichiasis/Entropion are the severe consequences of chronic trachoma during early life. Blindness and vision loss is preventable with timely lid surgery to correct trichiasis. In a trachoma hyperendemic region of Central Tanzania, a two year follow-up survey was conducted among 205 women with trichiasis to determine the proportion who had had surgery and the barriers to having surgery. Only 18% of the women had undergone surgery by the 2 year follow-up. Those who had surgery tended to report more eye problems at baseline and have more corneal opacities at baseline. Barriers preventing women from going to surgery were costs, problem of children left at home alone, and difficulties in identifying someone to accompany them to the health center. Over 2/3 of those who had surgery reported a significant decrease in pain, improvement of vision, and improved ability to carry out activities of daily life. Ways to improve compliance with recommendations for trichiasis surgery need to be developed.
Introduction
Trachoma is the second leading cause of blindness worldwide [1]. In areas hyperendemic for trachoma, active disease begins in pre-school children with tarsal scarring appearing in children as young as six [2]. With repeated episodes of re-infection, severe scar- ring can result, leading to trichiasis and entropion in young adulthood and middle age [2]. Left untreated, trichiasis/entropion can result in corneal.damage and irreversible vision loss.
For reasons not clearly understood, women are more likely to develop trichiasis/entropion and more likely to be blind from trachoma [2]. Blindness is pre- ventable with timely lid surgery to correct the trichi- asis. A simple procedure which can be taught to non- physicians has been shown to be safe and effective [3, 4].
In the Kongwa sub-district of Central Tanzania, tra- choma is an important cause of blindness [5]. A survey was conducted among 205 women with trichiasis to determine risk factors for trichiasis. At that time wom- en were made aware of the availability of trichiasls
surgery [6]. Thus, we had a unique opportunity to con- duct a two year follow-up on these 205 women with trichiasis. The purpose of the follow-up was to deter- mine how many women had surgery for their trichiasis over the next two years, and to determine barriers to having surgery.
Methods
The methods of identifying and recruiting the women with trichiasis have been described extensively else- where [6]. Basically, all women aged 18 to 60 in eleven villages were examined by an eye nurse for evidence of trichiasis/entropion. Trichiasis was defined using 'the W.H.O. simplified grading scheme as at least one eyelash rubbing on the eyeball, or evidence of recent removal of inturned eyelashes, or surgery to correct trichiasis/entropion [7]. Any women with at least one eye with trichiasis/entropion was eligible for the 1989 risk factor survey [6]. As part of that survey, a series of questions were asked on socioeconomic factors and other potential risk factors for trichiasis. Trained inter-

106
viewers conducted the questionnaires after the eye examination determined eligibility. An opportunity to receive lid surgery was offered at that time, including transportation to the rural health center.
In 1991, two years after the original survey, each woman with trichiasis was traced to determine whether or not she had had surgery. Each woman was asked a series of questions concerning perceived barriers to trichiasis surgery, and perceived benefits to having surgery. More than one answer was permitted.
Trichiasis surgery in Kongwa
It is important to understand the context in which lid surgery is carried out in Kongwa. The health system in Tanzania guarantees free surgery and accommodation, which would normally occur at the rural health center. The rural health center is still far from the villages. Transport to the rural health center was offered free of charge during the time of the 1989 survey, over the few days the survey team was in the village. In general, transport must be arranged by the patient. Lid surgery requires a 3 to 5 day stay in the center. Therefore, the surgical candidate needs someone to cover her affairs at home in her absence, and someone to accompany her to the center. Food and water are not always available at the rural health center, and must be procured by the patient's friend over the 3 to 5 day period. Occasionally lid surgery is actually carried out in the village using trained eye nurses, but these opportunities were rare during the two-year follow-up period.
Data analyses
Results are presented as proportions. Chi-squared or Fisher's exact test were used to test for differences between groups. Multiple logistic regression analyses were carried out to determine independent predictors of compliance with surgery; odds ratios and 95% con- fidence intervals are reported.
Results
A total of 205 women were identified in the 1989 sur- vey with trichiasis/entropion. For this follow-up study, we excluded 5 women of the 205 who had already had lid surgeryibefore the 1989 survey. Of the remain- ing 200, 80% (164) were followed-up and contacted
205 Women identified in 1989
--5 surgery prior to 1989
--22 moved out of district
--i death
--13 lost to follow up
164 (80%) followed up in 1990
Fig. 1. Two year follow-up status of 205 women with trichia- sis/entropion in 1989.
Table 1. Comparison of 200 women by follow-up status.
Follow up No follow up (n = 164) (n = 36)
Median age 45 40 % Comeal opacity 27% 22% % With tin roof 7% 11%
in 1991 (Fig. 1). A comparison showed no significant difference between the 164 women with follow-up and the 36 with no follow-up (Table 1).
A total of 29 women, or 18% of the 164, had under- gone lid surgery during the 2 year follow-up. There were no significant differences in age, education, reli- gion, or socio-economic status markers between those who had surgery and those who did not (Table 2).
Those who had surgery tended to report 'eye prob- lems' in 1989, had corneal opacities in 1989, and were 'more likely to have had epilated their eyelashes (Table 3). Interestingly, almost 20% of those who did not have surgery reported they had no eye problems in 1989, although, by definition, all had at least one eyelash touching the globe.
All women at follow-up were asked a general ques- tion of 'Why do you think some women in your village who need eyelid surgery do not go for eyelid surgery?'
107
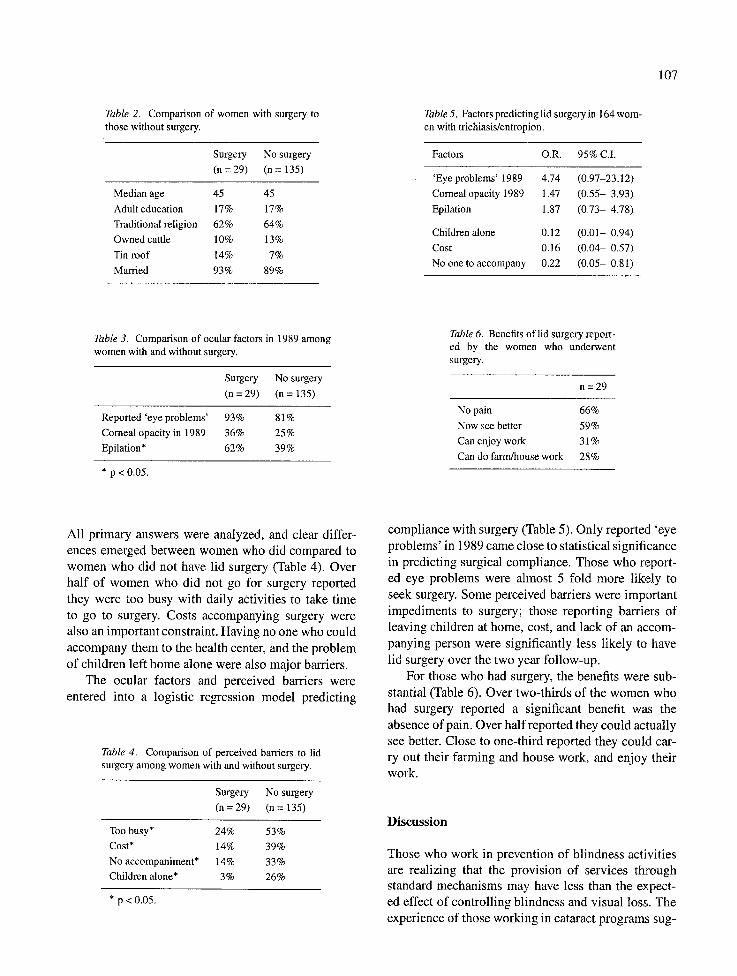
Table 2. Comparison of women with surgery to those without surgery.
Surgery No surgery (n = 29) (n = 135)
Median age 45 45 Adult education 17% 17% Traditional religion 62% 64% Owned cattle 10% 13 % Tin roof 14% 7% Married 93% 89%
Table 5. Factors predicting lid surgery in 164 wom- en with trichiasis/entropion.
Factors O.R. 95% C.I.
'Eye problems' 1989 4.74 (0.97-23.12) Corneal opacity 1989 1.47 (0.55- 3.93) Epilation 1.87 (0.73- 4.78)
Children alone 0.12 (0.01- 0.94) Cost 0.16 (0.04- 0.57) No one to accompany 0 .22 (0.05- 0.81)
Table 3. Comparison of ocular factors in 1989 among women with and without surgery.
Surgery No surgery (n = 29) (n = 135)
Reported 'eye problems' 93% 81% Corneal opacity in 1989 36% 25% Epilation* 62% 39%
* p < 0.05.
Table 6. Benefits of lid surgery report- ed by the women who underwent surgery.
n=29
No pain 66% Now see better 59% Can enjoy work 31% Can do farm/house work 28%
All primary answers were analyzed, and clear differ-
ences emerged between women who did compared to women who did not have lid surgery (Table 4). Over
half of women who did not go for surgery reported
they were too busy with daily activities to take time
to go to surgery. Costs accompanying surgery were also an important constraint. Having no one who could
accompany them to the health center, and the problem
of children left home alone were also major barriers.
The ocular factors and perceived barriers were
entered into a logistic regression model predicting
Table 4. Comparison of perceived barriers to lid surgery among women with and without surgery.
Surgery No surgery (n = 29) (n = 135)
Too busy* 24% 53% Cost* 14% 39% No accompaniment* 14% 33% Children alone* 3% 26%
*p<O.05.
compliance with surgery (Table 5). Only reported 'eye
problems' in 1989 came close to statistical significance
in predicting surgical compliance. Those who report-
ed eye problems were almost 5 fold more likely to
seek surgery. Some perceived barriers were important
impediments to surgery; those reporting barriers of leaving children at home, cost, and lack of an accom-
panying person were significantly less likely to have
lid surgery over the two year follow-up.
For those who had surgery, the benefits were sub-
stantial (Table 6). Over two-thirds of the women who had surgery reported a significant benefit was the
absence of pain. Over half reported they could actually
see better. Close to one-third reported they could car-
ry out their farming and house work, and enjoy their work.
D i s c u s s i o n
Those who work in prevention of blindness activities are realizing that the provision of services through standard mechanisms may have less than the expect-
ed effect of controlling blindness and visual loss. The experience of those working in cataract programs sug-

108
gest 30% or more of people who need cataract surgery and are offered service do not come for surgery [8- 11]. Severity of visual loss [9-11], age and sex [8, 11] were predictors of compliance with cataract surgery. Major constraints to surgery have included fear of the procedure, resignation about visual loss, and concern for cost and lack of transport [8-11]. In general, socio- demographic characteristics, apart from age and sex, have not been reliable predictors of compliance. There may well be more incentive to undergo cataract surgery than surgery for lid repair, because cataract surgery offers the possibility of restoration of sight. Lid surgery is preventive surgery.
For those with trachomatous trichiasis/entropion, timely lid surgery is the only strategy to prevent visual loss. Despite the fact that trachoma is the second lead- ing cause of blindness, to our knowledge, there are no data on compliance with recommendations for lid surgery.
In our population, only 18% of women had lid surgery over the two-year follow-up. The compliance rate with surgical recommendation was low. The most important predictors for not having surgery were the reported barriers to going for surgery. One-third of women without surgery reported no one who could take the time to accompany them to the rural health center, and one-fourth reported concern over leaving their children alone. These barriers can be addressed by carrying out the surgery in the villages, where the women wouldn't need to be away from their homes for the prescribed 3 to 5 day period. Such a shift in location requires a mobile eye nurse or surgeon who can be scheduled to operate in the villages, with appropriate follow-up. Where the village population is small, such an approach may not be cost-efficient unless several villages can be visited at the same time, or the patients can be pooled. In large villages, however, this approach could be considered.
Cost was also reported as a major barrier to surgery. These costs include purchasing food, possibly water, and supplies for the stay in the rural health center. The problems are compounded for those families who are self sufficient, or operate mostly outside the cash economy and thus have difficulty actually acquiring cash. Again, an approach which brings surgery to the village may well alleviate this perceived barrier.
There is a trend for women to wait for surgery until the trichiasis is severe. Those women coming to surgery after 1989 were more likely to report previ- ous epilation, some 'eye problems', and corneal opac- ity obscuring the pupillary margin in the 1989 sur-
vey. Increasing severity may well drive women to seek surgery; however, for the third who had corneal opac- ity in 1989, any subsequent surgery was too late to prevent corneal damage. We are concerned that anoth- er factor may also be delaying surgery. Most blind- ness prevention programs emphasize cataract surgery, and people in these villages know that they must wait for substantial visual loss from cataract before surgi- cal intervention can be considered. However, it may be unrealistic to suppose that villagers can differenti- ate for themselves the difference between visual loss from cataract, which is reversible, and visual loss from corneal opacity, which is not. We did not collect any data on this, so we do not know the extent to which these women might be delaying lid surgery because they assume they are not eligible until they suffer visu- al loss. However, cataract programs operating in areas with hyper-endemic trachoma should consider exer- cising caution about impressions that only people with visual loss should present to the health workers. Pro- grams may wish to provide education for the people in the villages about epilation and the need for an eye consultation early in the trichiasis process.
Acknowledgements
This project was funded by a grant from the Edna McCornell Clark Foundation. The Kongwa Trachoma Project is conducted under the auspices of the National Prevention of Blindness Committee in Tanzania. Dr. West is a Research to Prevent Blindness Senior Scien- tific Investigator.
References
1. Thylefors B. Primary eye care and the design of the WHO Programme for the Prevention of Blindness. Intl Ophth Clinics 30-1, Winter 1990.
2. West S, Munoz B, Turner V, Mmbaga BBO, Taylor HR. The epidemiology of trachomain Central Tanzania. Int J Epidemiol 1991; 20: 1088-92.
3. Reacher MH, Munoz B, Alghassany A, Daar AS, Elbualy M, Taylor HR. A controlled trial of surgery for trachoma- tous trichiasis of the upper lid. Arch Ophthalmol 1992; 100: 667-74.
4. Reacher M, Foster A, Huber J. Trichiasis SurgeryJbr Trachoma The Bilamellar Tarsal Rotation Procedure. WHO/PBL/93.29.
5. Rapoza PA, West S, Ktala SJ, Taylor HR. Prevalence and canses of vision loss in central Tanzania. Int Ophthalmol 1991; 15: 123-9.
6. Turner VM, West S, Munoz B, Katala S J, Taylor HR, Halsey N, Mmbaga BBO. Risk factors for trichiasis in women in Kongwa,
Tanzania: a case control study. Int J Epidemio11993; 22: 341- 7.
7. Thylefors B, Dawson CR, Jones BR, West S, Taylor HR. A simple system for the assessment of trachoma and its compli- cations. Bull WHO 1987; 65: 485-8.
8. Brilliant G, Lepkowski J, Zurita B, Thulasiraj RD and MBA. Social determinants of cataract surgery utilization in South India. Arch Ophthalmol 109(4): 584-9, 1991.
9. Kara Newton J, Contrera E Campos M, Delgado A, Mowery R, Ellwein L. Screening and surgical intervention results from cataract-free zone projects in Campinas, Brazil and Chimbote, Peru. Int Ophthalmo114: 155-64, 1990.
109
10. Vicencio C, Verdaguer JI, VerdaguerJT, Vargas Get al. Proyec- to San Vicente de Tagua Tagua: Zona Libre de catarata. Archivos Chilenos de Oflalmologia 48(1 ): 56-64, 1991.
11. Concha M. The natural history of senile cataract in the Chilean Health System. Ph.D. Thesis. Johns Hopkins School of Hygiene and Public Health, May, 1993.