predictable progressive doppler deterioration in iugr: does it really exist?
TRANSCRIPT

Research www.AJOG.org
OBSTETRICS
Predictable progressive Doppler deterioration inIUGR: does it really exist?Julia Unterscheider, MD; Sean Daly, MD; Michael Patrick Geary, MD; Mairead Mary Kennelly, MD;Fionnuala Mary McAuliffe, MD; Keelin O’Donoghue, PhD; Alyson Hunter, MD; John Joseph Morrison, MD;Gerard Burke, FRCOG; Patrick Dicker, PhD; Elizabeth Catherine Tully, PhD; Fergal Desmond Malone, MD
OBJECTIVE: An objective of the Prospective Observational Trial to had an abnormal UA, 300 (27%) had an abnormal MCA, and 129
Optimize Pediatric Health in IUGR (PORTO) study was to evaluatemultivessel Doppler changes in a large cohort of intrauterine growthrestriction (IUGR) fetuses to establish whether a predictable progres-sive sequence of Doppler deterioration exists and to correlate theseDoppler findings with respective perinatal outcomes.STUDY DESIGN: More than 1100 unselected consecutive ultrasound-dated singleton pregnancies with estimated fetal weight (EFW) lessthan the 10th centile were recruited between January 2010 and June2012. Eligible pregnancies were assessed by serial Doppler interro-gation of umbilical (UA) and middle cerebral (MCA) arteries, ductusvenosus (DV), aortic isthmus, and myocardial performance index (MPI).Intervals between Doppler changes and patterns of deterioration wererecorded and correlated with respective perinatal outcomes.
RESULTS: Our study of 1116 nonanomalous fetuses comprised 7769individual Doppler data points. Five hundred eleven patients (46%)
From the Departments of Obstetrics and Gynecology (Drs Unterscheider, TuCollege of Surgeons in Ireland; Department of Obstetrics and Gynecology (D(Dr Kennelly), Coombe Women and Infants University Hospital; Departmentof Obstetrics and Gynecology, University College Dublin School of MedicineDepartments of Obstetrics and Gynecology, University College Cork, Cork UnHospital, Belfast (Dr Hunter); National University of Ireland, Galway (Dr Morris(Dr Burke), Ireland.
Received May 30, 2013; revised Aug. 12, 2013; accepted Aug. 27, 2013.
The Prospective Observational Trial to Optimize Pediatric Health in IUGR Stunationwide collaborative research network comprising the 7 largest academicBoard and Friends of the Rotunda.
The authors report no conflict of interest.
Presented at the 33rd annual meeting of the Society for Maternal-Fetal Medi
Reprints: Julia Unterscheider, MD, Department of Obstetrics and GynecologDublin 1, Ireland. [email protected].
0002-9378/$36.00 � ª 2013 Mosby, Inc. All rights reserved. � http://dx.doi.org/10.1
See Journal Club, page 589
(11%) had an abnormal DV Doppler. The classic pattern fromabnormal UA to MCA to DV existed but no more frequently than any ofthe other potential pattern. Doppler interrogation of the UA and MCAremains the most useful and practical tool in identifying fetuses atrisk of adverse perinatal outcome, capturing 88% of all adverseoutcomes.
CONCLUSION: In contrast to previous reports, we have demonstratedmultiple potential patterns of Doppler deterioration in this largeprospective cohort of IUGR pregnancies, which calls into questionthe usefulness of multivessel Doppler assessment to inform fre-quency of surveillance and timing of delivery of IUGR fetuses. Thesedata will be critically important for planning any future interventiontrials.
Key words: Doppler, intrauterine growth restriction, sequentialchanges, umbilical artery
Cite this article as: Unterscheider J, Daly S, Geary MP, et al. Predictable progressive Doppler deterioration in IUGR: does it really exist? Am J Obstet Gynecol 2013;209:539.e1-7.
progressive predictable sequence
A of placental and fetal Dopplerchanges has been described as an adaptivemechanism to a suboptimal intrauterineenvironment in pregnancies affected byintrauterine growth restriction (IUGR).The surveillance and management ofIUGR secondary to placental dysfunctionis facilitated by umbilical artery (UA)Doppler assessment, and this is widelyaccepted as the primary ultrasound sur-veillance tool in such pregnancies.1-3
lly, and Malone) and Epidr Daly) and University Colof Obstetrics and Gynecoand Medical Science, Naiversity Maternity Hospitaon); and Graduate Entry
dy was conducted by theobstetric centers in Irelan
cine, San Francisco, CA,
y, Royal College of Surgeo
016/j.ajog.2013.08.039
DECEMBER 2013 Ameri
Several studies have contributed to theunderstanding of longitudinal Dopplerchanges occurring in IUGR.4-6 Knowl-edge about temporal deterioration inmaternal and fetal vessels is desired toinform frequency of surveillance and
emiology and Public Health (Dr Dicker), Royallege Dublin Center for Human Reproductionlogy, Rotunda Hospital (Dr Geary); Departmenttional Maternity Hospital (Dr McAuliffe); andl, Cork (Dr O’Donoghue); Royal Jubilee MaternityMedical School, University of Limerick, Limerick
Perinatal Ireland Research Consortium, ad. The study was funded by the Health Research
Feb. 11-16, 2013.
ns in Ireland, Rotunda Hospital, Parnell Square,
can Journal of Obstetrics & Gynecology 539.e1
TABLEMaternal demographics and fetal characteristics (n [ 1116)Characteristic n (%)/mean ± SD
Age, y 30 � 6
Ethnicity (white European) 907 (83%)
Spontaneous conception 1100 (99%)
Maternal height, cm 162 � 12
Maternal weight at booking, kg 64 � 13
BMI, kg/m2 24.1 � 4.7
Smokers 261 (23%)
Hypertensive disease/preeclampsia 134 (12%)
GA at enrolment, wks 30.1 � 3.9
GA at delivery, wks 37.8 � 3.0
Weight at delivery, g 2495 � 671
NICU admission 312 (28%)
Adverse perinatal outcome 57 (5%)
Apgar score <75 13 (1%)
Stillbirths 3 (1:370)
Neonatal deaths 3 (1:370)
Continuous variables are summarized with mean � SD and categorical variables with n (percentage).
BMI, body mass index; GA, gestational age; NICU, neonatal intensive care unit.
Unterscheider. Doppler deterioration in IUGR. Am J Obstet Gynecol 2013.
Research Obstetrics www.AJOG.org
timing of delivery. However, thesestudies have been either retrospectiveor comprised small patient numbers.Furthermore, it is important to note thatin fact most of these papers describing atemporal sequence refer to Doppler ab-normalities within a population of IUGRfetuses rather than a predictable pro-gressive sequence occurring within theindividual fetus. It is plausible thereforethat such prior population data may notactually be applicable to the longitudinalsurveillance of the individual fetus inclinical practice.
Longitudinal cumulative-onset timecurves of Doppler abnormalities des-cribing a time-dependent change ofvarious vessels are thought to follow onecertain predictable pattern from thefollowing: (1) abnormal blood flow in theuterine arteries, (2) increased resistance inthe umbilical arteries, (3) compensatoryflow in the middle cerebral artery (MCA)indicating cerebral redistribution, (4) ab-sent end-diastolic flow in the UA, whichis followed by (5) absent a-wave in theductus venosus (DV), (6) abnormalities in
539.e2 American Journal of Obstetrics & Gynecol
the pulmonary and aortic outflow tracts,and finally (7) reversed a-wave in the DV.4
These compensatory and decompen-satory changes have resulted in debate onthe benefit of assessing vessels other thanthe UA in the setting of IUGR. Althoughsome data suggest a role for DV Dopplerto inform timing of delivery in severeIUGR, evidence from a large random-ized trial is still awaited.7
Similarly, although reports suggest arole for abnormal aortic isthmus (AoI)Doppler in the setting of IUGR,8 therecently published Society for Maternal-Fetal Medicine clinical guideline onDoppler assessment of the IUGR fetus9
states that Doppler studies other thanthe UA should be reserved solely forresearch protocols. The same guidelineacknowledges that there “does appear tobe a natural progression of changes inthe Doppler of UA, MCA, and DV witha large variability in manifestation.”The goal of the prospective multi-
center Prospective Observational Trialto Optimize Pediatric Health in IUGR(PORTO) study was to evaluate the
ogy DECEMBER 2013
optimal surveillance of fetuses with anestimated fetal weight (EFW) less thanthe 10th centile.10 The objective of thisparticular analysis was to study Dopplerchanges in multiple vessels includingUA, MCA, DV, AoI, and myocardialperformance index (MPI) and to estab-lish whether a predictable progressivesequence of Doppler deterioration existsat the level of the individual fetus andto determine any added benefit in ap-plying these Doppler assessments inIUGR informing surveillance intervalsand timing of delivery.
MATERIALS AND METHODS
The PORTO trial is a multicenter pro-spective study conducted at 7 academicobstetric centers in Ireland. For thepurpose of the study, IUGR was definedas an EFW below the 10th centile basedon sonographic measurements of fetalbiparietal diameter, head circumference,abdominal circumference, and femurlength (Hadlock-4).11
Between January 2010 and June 2012,the PORTO study recruited 1200 co-nsecutive ultrasound-dated singletonpregnancies. Dating occurred either bycrown-rump length measurement priorto 14 weeks’ gestation or by compositemeasurement of biparietal diameter(BPD), head circumference, abdominalcircumference, and femur length from14 0/7 to 22 0/7 weeks’ gestation. In-clusion criteria were a gestation between24 0/7 and 36 6/7 weeks and an EFW of500 g or more. Fetuses with majorstructural and/ or chromosomal abnor-malities were excluded from the finalanalysis. Institutional review boardapproval was obtained at each partici-pating site, and all study participantsgave written informed consent.
Referral for consideration for enroll-ment to the study occurred if small fetalsize was suspected because of clinicalevaluation in the antenatal setting.A PORTO research sonographer thenconfirmed that the EFW was below the10th centile and performed a detailedevaluation of the fetal anatomy anduterine artery Doppler at enrollment. Alleligible pregnancies underwent serialsonographic evaluation of fetal weightat 2 weekly intervals until birth, and
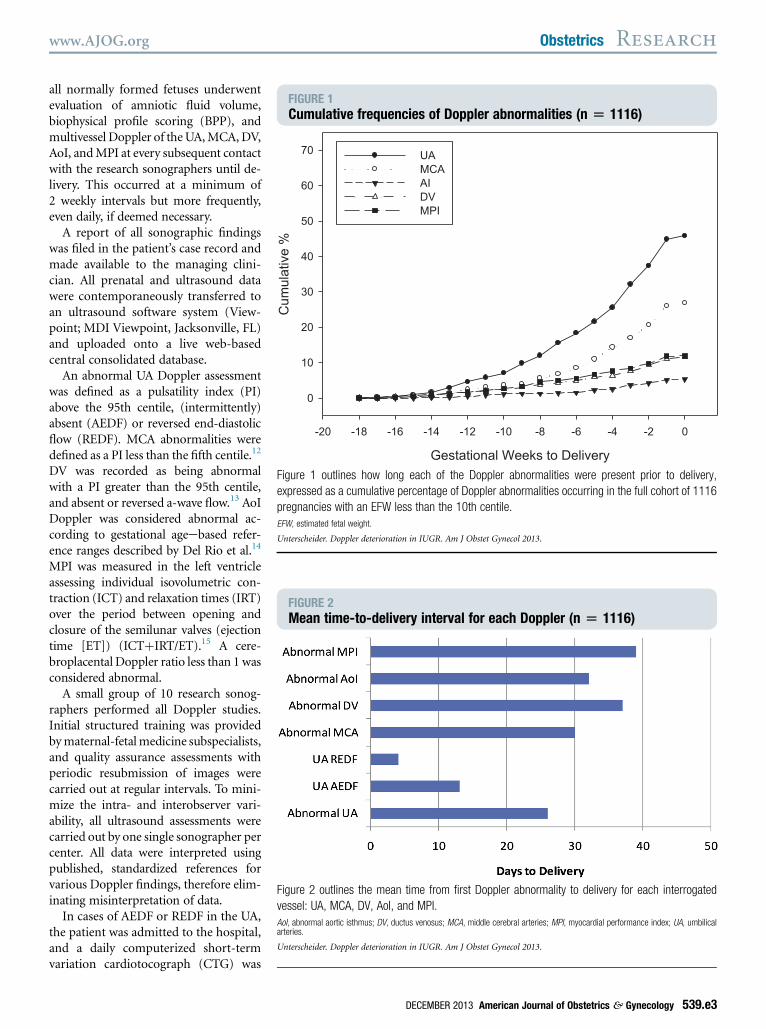
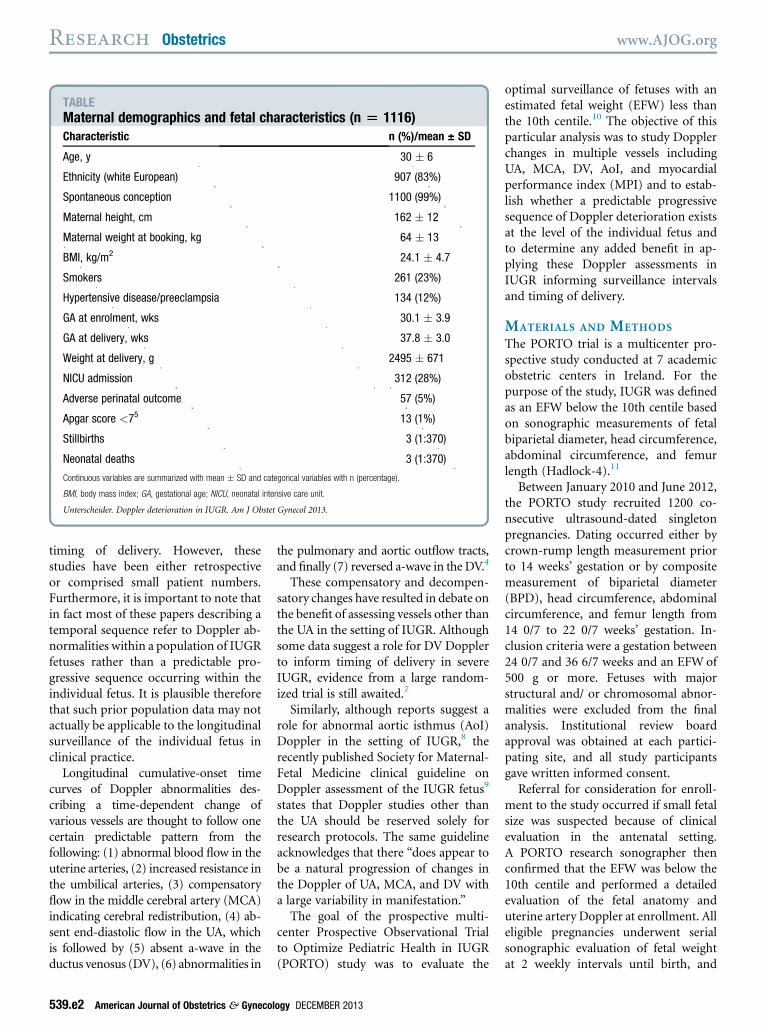
FIGURE 1Cumulative frequencies of Doppler abnormalities (n [ 1116)
Gestational Weeks to Delivery
-20 -18 -16 -14 -12 -10 -8 -6 -4 -2 0
Cum
ulat
ive
%
0
10
20
30
40
50
60
70 UAMCAAIDVMPI
Figure 1 outlines how long each of the Doppler abnormalities were present prior to delivery,
expressed as a cumulative percentage of Doppler abnormalities occurring in the full cohort of 1116
pregnancies with an EFW less than the 10th centile.
EFW, estimated fetal weight.
Unterscheider. Doppler deterioration in IUGR. Am J Obstet Gynecol 2013.
FIGURE 2Mean time-to-delivery interval for each Doppler (n [ 1116)
Figure 2 outlines the mean time from first Doppler abnormality to delivery for each interrogated
vessel: UA, MCA, DV, AoI, and MPI.
AoI, abnormal aortic isthmus; DV, ductus venosus; MCA, middle cerebral arteries; MPI, myocardial performance index; UA, umbilicalarteries.
Unterscheider. Doppler deterioration in IUGR. Am J Obstet Gynecol 2013.
www.AJOG.org Obstetrics Research
all normally formed fetuses underwentevaluation of amniotic fluid volume,biophysical profile scoring (BPP), andmultivessel Doppler of theUA,MCA,DV,AoI, andMPI at every subsequent contactwith the research sonographers until de-livery. This occurred at a minimum of2 weekly intervals but more frequently,even daily, if deemed necessary.
A report of all sonographic findingswas filed in the patient’s case record andmade available to the managing clini-cian. All prenatal and ultrasound datawere contemporaneously transferred toan ultrasound software system (View-point; MDI Viewpoint, Jacksonville, FL)and uploaded onto a live web-basedcentral consolidated database.
An abnormal UA Doppler assessmentwas defined as a pulsatility index (PI)above the 95th centile, (intermittently)absent (AEDF) or reversed end-diastolicflow (REDF). MCA abnormalities weredefined as a PI less than the fifth centile.12
DV was recorded as being abnormalwith a PI greater than the 95th centile,and absent or reversed a-wave flow.13 AoIDoppler was considered abnormal ac-cording to gestational ageebased refer-ence ranges described by Del Rio et al.14
MPI was measured in the left ventricleassessing individual isovolumetric con-traction (ICT) and relaxation times (IRT)over the period between opening andclosure of the semilunar valves (ejectiontime [ET]) (ICTþIRT/ET).15 A cere-broplacental Doppler ratio less than 1 wasconsidered abnormal.
A small group of 10 research sonog-raphers performed all Doppler studies.Initial structured training was providedbymaternal-fetalmedicine subspecialists,and quality assurance assessments withperiodic resubmission of images werecarried out at regular intervals. To mini-mize the intra- and interobserver vari-ability, all ultrasound assessments werecarried out by one single sonographer percenter. All data were interpreted usingpublished, standardized references forvarious Doppler findings, therefore elim-inating misinterpretation of data.
In cases of AEDF or REDF in the UA,the patient was admitted to the hospital,and a daily computerized short-termvariation cardiotocograph (CTG) was
DECEMBER 2013 American Journal of Obstetrics & Gynecology 539.e3
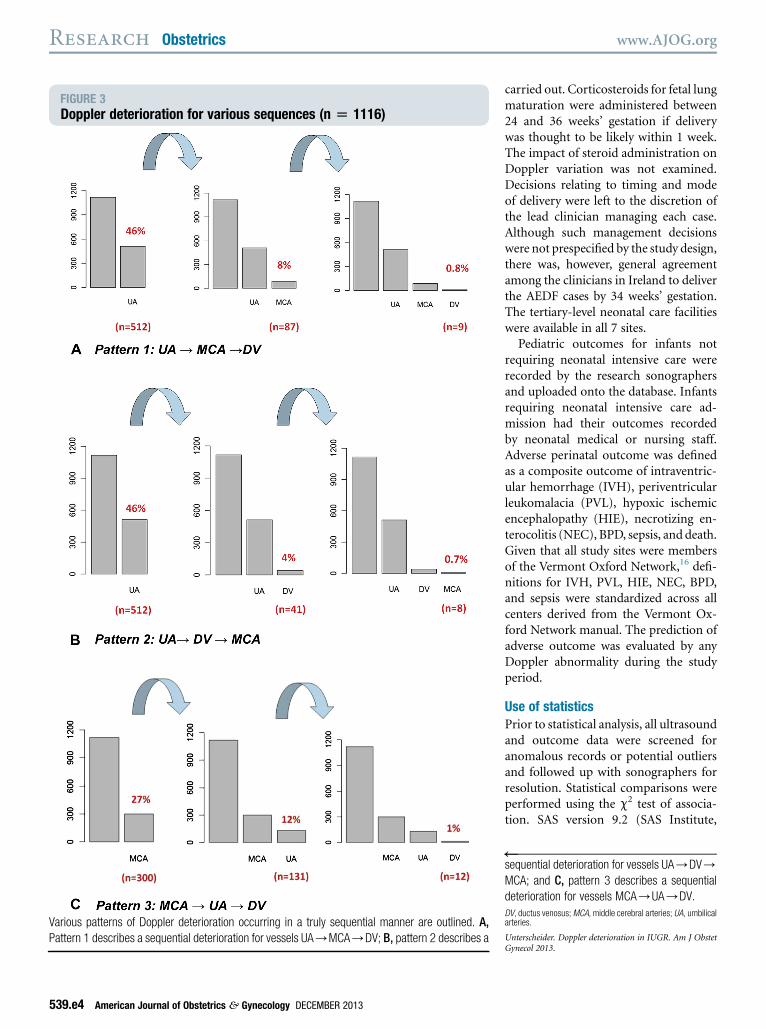
FIGURE 3Doppler deterioration for various sequences (n [ 1116)
Various patterns of Doppler deterioration occurring in a truly sequential manner are outlined. A,
Pattern 1 describes a sequential deterioration for vessels UA/MCA/DV; B, pattern 2 describes a
Research Obstetrics www.AJOG.org
539.e4 American Journal of Obstetrics & Gynecology DECEMBER 2013
carried out. Corticosteroids for fetal lungmaturation were administered between24 and 36 weeks’ gestation if deliverywas thought to be likely within 1 week.The impact of steroid administration onDoppler variation was not examined.Decisions relating to timing and modeof delivery were left to the discretion ofthe lead clinician managing each case.Although such management decisionswere not prespecified by the study design,there was, however, general agreementamong the clinicians in Ireland to deliverthe AEDF cases by 34 weeks’ gestation.The tertiary-level neonatal care facilitieswere available in all 7 sites.
Pediatric outcomes for infants notrequiring neonatal intensive care wererecorded by the research sonographersand uploaded onto the database. Infantsrequiring neonatal intensive care ad-mission had their outcomes recordedby neonatal medical or nursing staff.Adverse perinatal outcome was definedas a composite outcome of intraventric-ular hemorrhage (IVH), periventricularleukomalacia (PVL), hypoxic ischemicencephalopathy (HIE), necrotizing en-terocolitis (NEC), BPD, sepsis, and death.Given that all study sites were membersof the Vermont Oxford Network,16 defi-nitions for IVH, PVL, HIE, NEC, BPD,and sepsis were standardized across allcenters derived from the Vermont Ox-ford Network manual. The prediction ofadverse outcome was evaluated by anyDoppler abnormality during the studyperiod.
Use of statisticsPrior to statistical analysis, all ultrasoundand outcome data were screened foranomalous records or potential outliersand followed up with sonographers forresolution. Statistical comparisons wereperformed using the c2 test of associa-tion. SAS version 9.2 (SAS Institute,
sequential deterioration for vessels UA/DV/MCA; and C, pattern 3 describes a sequential
deterioration for vessels MCA/UA/DV.
DV, ductus venosus;MCA, middle cerebral arteries; UA, umbilicalarteries.
Unterscheider. Doppler deterioration in IUGR. Am J ObstetGynecol 2013.
)

www.AJOG.org Obstetrics Research
Cary, NC) was used for data manage-ment and statistical analysis.
RESULTS
Of 1200 recruited pregnancies with anEFW below the 10th centile, 32 (2.7%)were excluded because of chromosomaland/or structural abnormalities, 13 (1%)withdrew their consent, and 13 (1%)delivered outside Ireland, whereas afurther 26 (2.2%) were lost to follow-up.This resulted in 1116 patients com-pleting the study protocol.
The mean maternal age was 30 years,the mean body mass index was 24 kg/m2,and the vast majority of women were ofwhite European descent. This is consis-tent with the demographic profile of theoverall obstetric population attending forantenatal care in Ireland,17 reflecting anunselected group of recruited pregnan-cies. Twenty-three percent were smokersand 12% were affected by hypertensivedisease or preeclampsia. The mean ges-tational age (GA) at enrollment to thestudy was 30.1 weeks and themean GA atdelivery was 37.8 weeks. The Table out-lines maternal demographics and fetalcharacteristics.
Our study of 1116 fetuses withan EFW less than the 10th centilecomprised 7769 individual Doppler datapoints gathered for as long as 17 weeksof surveillance on some patients, withan average of 7.7 weeks. Five hundredeleven patients (46%) had an abnormalUA Doppler waveform in the study;70 patients had an UA AEDF and 8 hadan UA REDF. The mean time to deliveryfor patients with abnormal UA Doppler,(intermittent) AEDF, and REDF was 26,13, and 4 days, respectively. Three hun-dred of the study population (27%) hadan abnormal MCA, 133 (12%) had anabnormal MPI, 129 (11%) had an ab-normal DV, and 59 (5%) had anabnormal AoI.
The frequency of Doppler deteriora-tion for each vessel and the timing todelivery is outlined in Figure 1. It isimportant to point out that these arecumulative frequencies seen in the entirestudy population of 1116 fetuses, andgiven that there may or may not be asignificant overlap between these ab-normalities, we cannot conclude that
this represents the main sequence ofprogressive deterioration at the individ-ual fetal patient level.To emphasize this point further,
Figure 2 represents the mean time fromfirst diagnosis of Doppler abnormalityuntil delivery. If there was a singledominant sequence of deterioration inDoppler abnormalities in the setting ofIUGR, we would have expected to see agradual shortening in the time from firstdiagnosis to delivery for each of therelevant Doppler findings. In contrast,what we actually found was no overallpattern of Doppler deterioration in eachof these vessels. For example, althoughthemean time from diagnosis to deliveryfor an abnormal UA was 26 days, themean time from diagnosis to delivery forabnormal DV was 37 days and 39 daysfor an abnormal MPI.Our data demonstrate that there are in
fact various patterns of Doppler deterio-ration occurring in a truly sequentialmanner,meaning that an initial abnormalDoppler finding was followed by anotherand another in one and the same fetusover time. Given that we interrogated5 fetal vessels in our study, there are120 different potential sequences; wehave, however, restricted our descriptionof this point to 3 patterns to illustrate thisconcept (Figure 3, A-C).If we analyze the classic sequence
(pattern 1: UA/MCA/DV), thoughtto be the single most common patternof deterioration in IUGR, our datashow that 46% (n ¼ 511) of the overallcohort developed an abnormal UADoppler. Eight percent (n ¼ 87) had asequence of an abnormal UA and MCADoppler, and only 0.8% (n ¼ 9) in ourcohort showed a sequential change in all3 vessels. A similar sequence applies forpatterns 2 (UA/DV/MCA) and 3(MCA/UA/DV).To summarize these findings, Figure 4
combines various patterns of Dopplerdeterioration. If the sequence of deteri-oration from UA to MCA to DV was themost important, we would expect tosee a relatively flat line such that almostall patients with an abnormal umbilicalartery Doppler would next have anabnormalmiddle cerebral artery Dopplerand would next have an abnormal ductus
DECEMBER 2013 Ameri
venosus Doppler. In actual fact, what wefound was that all 6 possible sequencesof Doppler deterioration were similarlyrepresented in our dataset.
Interestingly, even when we focusedon a selected group of 113 fetuses whohad such severe IUGR that requireddelivery prior to 34 weeks, we still couldnot identify one single predominantpathway or sequence of deterioration.Average gestational age at presentationfor all 6 Doppler sequences was 24-27weeks, showing no statistical significancewhen analyzing the progression in rela-tion to gestational age at enrollment (P¼.1835, Kruskal-Wallis test).
Correlation of Doppler findings withrespective perinatal morbidity and mor-tality outcomes shows that an abnormalumbilical artery Doppler is by far themost likely test to be associated withadverse outcome, capturing 86% of allrecorded adverse outcomes (Figure 5).Second, the next most useful vessel is anabnormalmiddle cerebral artery Doppler,capturing 51% of all adverse outcomes.If significant time and effort are placedinto searching for other Doppler abnor-malities such as DV, AoI, and MPI, thiswill only pick up a relatively small pro-portion of remaining adverse perinataloutcomes.
COMMENT
Despite the large amount of publishedliterature on ultrasound in the setting ofIUGR, the optimal surveillance patternand timing of delivery remains the focusof much debate and research, with nointernationally accepted approach tomanagement.
In this large prospective cohort ofIUGRpregnancies, we have demonstratedmultiple potential patterns of Dopplerdeterioration. The classic sequence fromabnormal UA toMCA to DVexists but nomore frequently than any of the otherpotential patterns.
A major strength of this study is theprospective study design. It took only2 years to recruit 1200 pregnancies in7 centers, all of which were subjected toa high degree of fetal surveillance usingthe most advanced Doppler techniquesavailable, which were performed bya small group of 10 trained research
can Journal of Obstetrics & Gynecology 539.e5
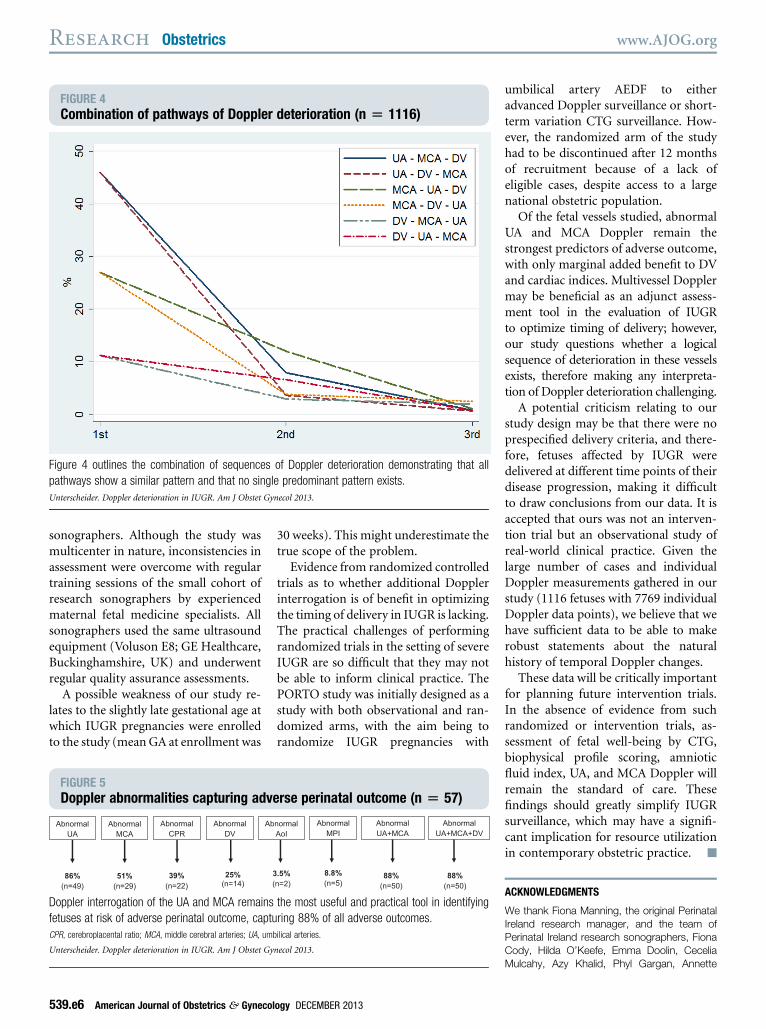
FIGURE 4Combination of pathways of Doppler deterioration (n [ 1116)
Figure 4 outlines the combination of sequences of Doppler deterioration demonstrating that all
pathways show a similar pattern and that no single predominant pattern exists.
Unterscheider. Doppler deterioration in IUGR. Am J Obstet Gynecol 2013.
Research Obstetrics www.AJOG.org
sonographers. Although the study wasmulticenter in nature, inconsistencies inassessment were overcome with regulartraining sessions of the small cohort ofresearch sonographers by experiencedmaternal fetal medicine specialists. Allsonographers used the same ultrasoundequipment (Voluson E8; GE Healthcare,Buckinghamshire, UK) and underwentregular quality assurance assessments.
A possible weakness of our study re-lates to the slightly late gestational age atwhich IUGR pregnancies were enrolledto the study (mean GA at enrollment was
FIGURE 5Doppler abnormalities capturing adv
Abnormal UA
Abnormal MCA
Abnormal DV
Ab
86%
(n=49)51%
(n=29)25%
(n=14) (
Abnormal CPR
39%
(n=22)
Doppler interrogation of the UA and MCA remains
fetuses at risk of adverse perinatal outcome, captu
CPR, cerebroplacental ratio; MCA, middle cerebral arteries; UA, um
Unterscheider. Doppler deterioration in IUGR. Am J Obstet Gy
539.e6 American Journal of Obstetrics & Gynecol
30 weeks). This might underestimate thetrue scope of the problem.Evidence from randomized controlled
trials as to whether additional Dopplerinterrogation is of benefit in optimizingthe timing of delivery in IUGR is lacking.The practical challenges of performingrandomized trials in the setting of severeIUGR are so difficult that they may notbe able to inform clinical practice. ThePORTO study was initially designed as astudy with both observational and ran-domized arms, with the aim being torandomize IUGR pregnancies with
erse perinatal outcome (n [ 57)
normal AoI
3.5%
n=2)88%
(n=50)88%
(n=50)
Abnormal MPI
8.8%
(n=5)
Abnormal UA+MCA
Abnormal UA+MCA+DV
the most useful and practical tool in identifying
ring 88% of all adverse outcomes.
bilical arteries.
necol 2013.
ogy DECEMBER 2013
umbilical artery AEDF to eitheradvanced Doppler surveillance or short-term variation CTG surveillance. How-ever, the randomized arm of the studyhad to be discontinued after 12 monthsof recruitment because of a lack ofeligible cases, despite access to a largenational obstetric population.
Of the fetal vessels studied, abnormalUA and MCA Doppler remain thestrongest predictors of adverse outcome,with only marginal added benefit to DVand cardiac indices. Multivessel Dopplermay be beneficial as an adjunct assess-ment tool in the evaluation of IUGRto optimize timing of delivery; however,our study questions whether a logicalsequence of deterioration in these vesselsexists, therefore making any interpreta-tion of Doppler deterioration challenging.
A potential criticism relating to ourstudy design may be that there were noprespecified delivery criteria, and there-fore, fetuses affected by IUGR weredelivered at different time points of theirdisease progression, making it difficultto draw conclusions from our data. It isaccepted that ours was not an interven-tion trial but an observational study ofreal-world clinical practice. Given thelarge number of cases and individualDoppler measurements gathered in ourstudy (1116 fetuses with 7769 individualDoppler data points), we believe that wehave sufficient data to be able to makerobust statements about the naturalhistory of temporal Doppler changes.
These data will be critically importantfor planning future intervention trials.In the absence of evidence from suchrandomized or intervention trials, as-sessment of fetal well-being by CTG,biophysical profile scoring, amnioticfluid index, UA, and MCA Doppler willremain the standard of care. Thesefindings should greatly simplify IUGRsurveillance, which may have a signifi-cant implication for resource utilizationin contemporary obstetric practice. -
ACKNOWLEDGMENTS
We thank Fiona Manning, the original PerinatalIreland research manager, and the team ofPerinatal Ireland research sonographers, FionaCody, Hilda O’Keefe, Emma Doolin, CeceliaMulcahy, Azy Khalid, Phyl Gargan, Annette

www.AJOG.org Obstetrics Research
Burke, Edel Varden, Wendy Ooi, and AmandaAli.
REFERENCES
1. Alfirevic Z, Stampalija T, Gyte GM. Fetal andumbilical Doppler ultrasound in high-risk preg-nancies. Cochrane Database Syst Rev 2010:CD007529.2. American College of Obstetricians and Gy-necologists. Intrauterine growth restriction.AJOG practice bulletin no. 12. Washington, DC:American College of Obstetricians and Gyne-cologists; 2000.3. Royal College of Obstetricians and Gynae-cologists (RCOG). Green-top guideline. Theinvestigation and management of the small-forgestational-age fetus. London, UK: RCOGPress; 2002.4. Ferrazzi E, Bozzo M, Rigano S, et al. Tem-poral sequence of abnormal Doppler changes inthe peripherals and central circulatory systemsof the severely growth-restricted fetus. Ultra-sound Obstet Gynecol 2002;19:140-6.5. Baschat A, Gembruch U, Harman C. Thesequence of changes in Doppler and biophysicalparameters as severe fetal growth restrictionworsens. Ultrasound Obstet Gynecol 2001;18:571-7.
6. Hecher K, Bilardo CM, Stigter RH, et al.Monitoring of fetuses with intrauterine growthrestriction: a longitudinal study. UltrasoundObstet Gynecol 2001;18:564-70.7. Lees C, Baumgartner H. The TRUFFLEstudy—a collaborative publicly funded projectfrom concept to reality: how to negotiate anethical, administrative and funding obstaclecourse in the European Union. UltrasoundObstet Gynecol 2005;25:105-7.8. Kennelly MM, Farah N, Turner MJ, Stuart B.Aortic isthmus Doppler velocimetry: role inassessment of preterm fetal growth restriction.Prenat Diagn 2010;30:395-401.9. Society for Maternal-Fetal Medicine Publica-tions Committee Berkley E, Chauhan SP,Abuhamad A. Doppler assessment of the fetuswith intrauterine growth restriction. Am J ObstetGynecol 2012;206:300-8.10. Unterscheider J, Daly S, Geary MP, et al.Optimizing the definition of intrauterine growthrestriction—results of the Multicenter Prospec-tive PORTO study. Am J Obstet Gynecol2013;208:290.e1-6.11. Hadlock FP, Harrist RB, Sharman RS,Deter RL, Park SK. Estimation of fetal weightwith the use of head, body, and femurmeasurements—a prospective study. Am JObstet Gynecol 1985;151:333-7.
DECEMBER 2013 Ameri
12. Ebbing C, Rasmussen S, Kiserud T. Middlecerebral artery blood flow velocities and pulsa-tility index and the cerebroplacental pulsatilityratio: longitudinal reference ranges and terms forserial measurement. Ultrasound Obstet Gynecol2007;30:287-96.13. Kessler J, Rasmussen S, Hanson M,Kiserud T. Longitudinal reference ranges forductus venosus flow velocities and waveformindices. Ultrasound Obstet Gynecol 2006;28:890-8.14. Del Rio M, Martinez JM, Figueras F, et al.Reference ranges for Doppler parameters of thefetal aortic isthmus during the second halfof pregnancy. Ultrasound Obstet Gynecol2006;28:71-6.15. Friedman D, Buyon J, Kim M, Glickstein JS.Fetal cardiac function assessed by Dopplermyocardial performance index (Tei Index).Ultrasound Obstet Gynecol 2003;21:33-6.16. Horbar JD. The Vermont Oxford Network:evidence based quality improvement forneonatology. Pediatrics 1999;103:350-9.17. National Perinatal Reporting System(NPRS). Perinatal Statistics Report, Economicand Social Research Institute (ESRI) on behalf ofthe Department of Health and the Health ServiceExecutive Ireland, June 2010. Available at: www.esri.ie. Accessed Sept. 16, 2013.
can Journal of Obstetrics & Gynecology 539.e7