preconception health policy and finance 2007 citymatch urban mch leadership conference august 26-28,...
TRANSCRIPT

Preconception Health Preconception Health Policy and Finance Policy and Finance
2007 CityMatCH Urban MCH Leadership Conference2007 CityMatCH Urban MCH Leadership ConferenceAugust 26-28, 2007August 26-28, 2007Denver, ColoradoDenver, Colorado
Anne Rossier Markus, JD, PhD, MHS
Associate Research Professor, Department of Health Policy
The George Washington University

Outline - Access to Outline - Access to Quality Preconception Quality Preconception CareCare
CDC Select Panel’s Workgroup on CDC Select Panel’s Workgroup on Financing of Preconception CareFinancing of Preconception Care
CDC Action StepsCDC Action Steps– Improving the Design of Medicaid Family Improving the Design of Medicaid Family
Planning WaiversPlanning Waivers– Monitoring, and Tying Payment to, Quality of Monitoring, and Tying Payment to, Quality of
Preconception Care through the HEDIS Preconception Care through the HEDIS Measurement SystemMeasurement System
CDC Recommendation: CDC Recommendation: To Improve Health Insurance Coverage of Preconception To Improve Health Insurance Coverage of Preconception
CareCare
especially for low-income women who may be at especially for low-income women who may be at higher risk for adverse birth outcomeshigher risk for adverse birth outcomes
CDC Select Panel’s Workgroup on Financing of Preconception Care:
Findings and Recommendations
March 9, 2007

Workgroup Membership Co-ChairsCo-Chairs: :
– GWU SPHHS Department of Health Policy GWU SPHHS Department of Health Policy – Dartmouth-Hitchcock Medical Center Department of Dartmouth-Hitchcock Medical Center Department of
PediatricsPediatrics– CDC Workgroup LeadCDC Workgroup Lead
MembersMembers: : – JIWH; KFFJIWH; KFF– AGI; ACOG; MODAGI; ACOG; MOD– NACCHONACCHO– ASTHO; NCSLASTHO; NCSL– AMCHP; NACHC; National Healthy Start AssociationAMCHP; NACHC; National Healthy Start Association– CDC; HRSA-MCHB; CMSCDC; HRSA-MCHB; CMS

Working Parameters1. Vision for Preconception Care 1. Vision for Preconception Care
2. Definition of Preconception Care2. Definition of Preconception Care
3. Standard of Preconception Care3. Standard of Preconception Care
BUT BUT
4. Mixed private and public 4. Mixed private and public financing system with lack of financing system with lack of universal coverage of women of universal coverage of women of reproductive agereproductive age

1. Vision for Preconception Care All women of childbearing age have All women of childbearing age have
health coveragehealth coverage All women of childbearing age are All women of childbearing age are
screened prior to pregnancy for risks screened prior to pregnancy for risks related to outcomesrelated to outcomes
Women with a prior adverse Women with a prior adverse pregnancy outcome have access to pregnancy outcome have access to intensive preconception care to intensive preconception care to reduce their risksreduce their risks

2. Definition of Preconception Care
A set of interventions that aim to A set of interventions that aim to identify and modify biomedical, identify and modify biomedical, behavioral, and social risks to a behavioral, and social risks to a woman’s health or pregnancy woman’s health or pregnancy outcome through prevention and outcome through prevention and management, emphasizing those management, emphasizing those factors which must be acted on factors which must be acted on before conception or early in before conception or early in pregnancy to have maximal impact.pregnancy to have maximal impact.

3. Standard of 3. Standard of Preconception Care & Core Preconception Care & Core Components Components
Assessment & Screening
Medical & reproductive history; Genetic & family history;
Environmental & occupational exposures; Family planning and
pregnancy spacing; Nutrition, folic acid intake, and weight
management; Medications; Substance use (alcohol, tobacco
and illicit drugs); Infectious diseases; Psycho-social (e.g.,
depression, domestic violence, housing)
Health Promotion & Counseling
Healthy weight; Nutrition; Preventing STD & HIV
infection; Family planning methods; Abstaining from tobacco, alcohol, and illicit drug use before and during pregnancy; Consuming folic
acid; Controlling pre-existing medical conditions (e.g.,
diabetes); Risks from prescription drugs; Genetic
conditionsBrief Interventions
ImmunizationSmoking cessation
Alcohol misuseWeight management
Family planningFolic acid
Source: Kay Johnson, March 2007

4. Mixed Financing & Lack of Universal Coverage of Women of Reproductive Age
All Women Ages 15-44(N = 61.7 million, 2003)
12%
64%
21%
3%
Medicaid
Private
Uninsured
Other
Poor Women Ages 15-44 (N = 9.1 million, 2003)
37%
20%
41%
2%
Sources: US Current Population Survey, AGI, KFF.

March 9 March 9 Meeting Objectives Objectives
Discuss and reach consensus on key attributes of Discuss and reach consensus on key attributes of
a high performing system of preconception care a high performing system of preconception care
financing (public and private)financing (public and private)
Discuss options for Medicaid coverageDiscuss options for Medicaid coverage
Discuss the roles of public health programs (i.e., Discuss the roles of public health programs (i.e.,
Health Centers, Title X Family Planning, Title V Health Centers, Title X Family Planning, Title V
MCH Block Grant, Healthy Start)MCH Block Grant, Healthy Start)
Discuss next stepsDiscuss next steps
Eligibility Enrollment and Transition between
Financing Arrangements Benefits and Coverage Rules Cost-Sharing Access to Community Providers Privacy, Confidentiality and Access to
Health Information Quality and Provider Compensation
Key Attributes of a High Performing System of Preconception Care Financing

Eligibility (consensus)
Cover all women during their reproductive life Cover all women during their reproductive life span (from menarche to menopause)span (from menarche to menopause)
Cannot set arbitrary limits based on ageCannot set arbitrary limits based on age
Cannot impose coverage limits or waiting periods Cannot impose coverage limits or waiting periods based on pre-existing conditionsbased on pre-existing conditions
Cannot use an asset testCannot use an asset test
Must provide subsidies for women whose family Must provide subsidies for women whose family incomes are considered low (e.g., < 200% FPL)incomes are considered low (e.g., < 200% FPL)

Enrollment & Enrollment & TransitionTransition
Public financing: – Enrollment at the point of care, through
outstationing, and in other locations convenient to consumers
– Continuous enrollment until circumstances change, requiring review (e.g., change in income)
– Loss of private coverage should be an immediate qualifying event for public coverage
Private financing:– Portability of coverage

Benefits & Coverage Rules
Equivalent to the existing standard of preconception care– Screening/assessment– Counseling/health education and promotion– Interventions/treatment
No arbitrary limits or exclusions
Provided by any licensed HCW within scope of practice
Medical necessity standard promotes (i) attainment and maintenance of optimal health in reproductive years and (ii) correction and amelioration of physical or mental conditions that could adversely affect reproductive health

Cost-Sharing
No deductibles for services identified as No deductibles for services identified as primary preventive careprimary preventive care
Use of co-payments and/or coinsurance only Use of co-payments and/or coinsurance only if affordableif affordable
Availability of direct subsidies for community-Availability of direct subsidies for community-based providers that serve low-income based providers that serve low-income women to help offset the cost of cost-sharing women to help offset the cost of cost-sharing and to furnish enabling servicesand to furnish enabling services

Access to Community Providers
Provider network in the community should Provider network in the community should be adequate to furnish covered services be adequate to furnish covered services
Participation of community health Participation of community health providers should be allowedproviders should be allowed

Privacy, Confidentiality and Access to Health Information
Patients and health care providers should have full and ready access to health information necessary for treatment and payment, in a secure and interoperable environment
Systems should exchange essential information to measure population health with public health agencies

Quality & Provider Compensation Appropriate compensation for providers up Appropriate compensation for providers up
to their scope of practiceto their scope of practice
Compensation guided by principles of Compensation guided by principles of quality performance, with regular and quality performance, with regular and systematic measurement of process and systematic measurement of process and outcome of careoutcome of care– Existing measures (e.g., HEDIS postpartum care)Existing measures (e.g., HEDIS postpartum care)– New measures (e.g., reproductive health plan, New measures (e.g., reproductive health plan,
minimum number of visits, screening tools) minimum number of visits, screening tools)

Options for Medicaid CoverageOptions for Medicaid Coverage

Federal and State Levels
““Women” as a new optional eligibility Women” as a new optional eligibility category category
State’s choice to (i) cover some or all women State’s choice to (i) cover some or all women not currently covered and (ii) determine not currently covered and (ii) determine scope of benefits essential to wellness – e.g.,scope of benefits essential to wellness – e.g.,
Full Medicaid benefitsFull Medicaid benefits Preventive preconception packagePreventive preconception package Family planning Family planning

Roles of Public Health ProgramsRoles of Public Health Programs

Public Health Public Health ProgramsPrograms
Title X FP programs serve ~4.6 million Title X FP programs serve ~4.6 million women of childbearing age (FP education; women of childbearing age (FP education; contraceptives; pregnancy tests)contraceptives; pregnancy tests)
Title V MCH services block grant programs Title V MCH services block grant programs serve ~2.5 million pregnant women serve ~2.5 million pregnant women ((prenatal, delivery, and postpartum care for low income, at-risk pregnant women)
Health centers serve ~4.5 million women Health centers serve ~4.5 million women of childbearing age and provide prenatal of childbearing age and provide prenatal care to some 330,000 pregnant womencare to some 330,000 pregnant women

Other Programs Other Programs (Cont.)(Cont.) HRSA’s Healthy Start program serves
high-risk pregnant women in 99 99 communities in 38 States, the District of communities in 38 States, the District of Columbia, and Puerto Rico Columbia, and Puerto Rico (interconception activities)
WIC serves ~8 million women during WIC serves ~8 million women during pregnancy and postpartum (nutrition pregnancy and postpartum (nutrition screening and counseling; supplemental screening and counseling; supplemental food; referrals to health services)food; referrals to health services)

Federal and State Levels Programs need augmented federal Programs need augmented federal
appropriationappropriation
Within existing funds, opportunities to embed Within existing funds, opportunities to embed preconception care into existing servicespreconception care into existing services
Need to monitor and disseminate promising Need to monitor and disseminate promising practices at the state and local levelpractices at the state and local level

Next StepsNext Steps

Revise and distribute principles for financing Revise and distribute principles for financing preconception carepreconception care
Develop prototype fact sheets for federal and Develop prototype fact sheets for federal and state advocatesstate advocates
Prepare an update on preconception benefits Prepare an update on preconception benefits within Medicaid family planning waivers within Medicaid family planning waivers
Publish a special issue of Publish a special issue of Women’s Health Women’s Health Issues Issues
Work with selected state/local leaders on Work with selected state/local leaders on advocacyadvocacy
Products and Activities

Improving the Design of Medicaid Family Planning Waivers

US Women of Child-Bearing Age, 2006
According to the US Census Bureau, there are nearly 62 million women age 15-44
34% are low-income (<200% of poverty)
US Women Age 15-44, By Poverty Level
16 1866
0
50
100
< 100% 100-200% > 200%
Source: http://www.census.gov/hhes/www/cpstc/cps_table_creator.html

Insurance Coverage of US Insurance Coverage of US Women of Child-Bearing Age, Women of Child-Bearing Age, 20032003
All Women Ages 15-44(N = 61.7 million, 2003)
12%
64%
21%
3%
Medicaid
Private
Uninsured
Other
Poor Women Ages 15-44 (N = 9.1 million, 2003)
37%
20%
41%
2%
Sources: US Current Population Survey, AGI, KFF.

Uninsured Women by Age, Uninsured Women by Age, 20042004
17%
26%
27%
30%
18-24
25-34
35-44
45>
Total: 19.5 million
Source: Salganicoff, A., Ranji, U., and Wyn, R. Women and Health Care: A National Profile, Kaiser Family Foundation, Washington, DC, July 2005

Uninsured Women of Uninsured Women of Childbearing Age (15-44) by Childbearing Age (15-44) by Educational Attainment, 2006Educational Attainment, 2006
29%
34%
26%
11%
No high schooldiploma
High school orequivalent
Some college, lessthan 4-year degree
Bachelor's degree orhigher
Total: 12.4 million
Source: US Census Bureau, Current Population Survey, Annual Social and Economic Supplement, 2006 http://www.census.gov/hhes/www/cpstc/cps_table_creator.html

Uninsured Women of Uninsured Women of Childbearing Age (15-44) by Childbearing Age (15-44) by Parental Status, 2006Parental Status, 2006
59%
41%Parent
Non-parent
Total: 12.4 million
Source: US Census Bureau, Current Population Survey, Annual Social and Economic Supplement, 2006 http://www.census.gov/hhes/www/cpstc/cps_table_creator.html
Parent is defined as having 1 or more related children under age 18

Uninsured Women of Uninsured Women of Childbearing Age (15-44) by Childbearing Age (15-44) by Income, 2006Income, 2006
61%
39%
<200% FPL
> 200% FPL
Total: 12.4 million
Source: US Census Bureau, Current Population Survey, Annual Social and Economic Supplement, 2006 http://www.census.gov/hhes/www/cpstc/cps_table_creator.html

Uninsured Women of Uninsured Women of Childbearing Age (15-44) by Childbearing Age (15-44) by Employment, 2006Employment, 2006
39%
55%
6%
Children/ArmedForces/Not in LaborForce
Employed
Unemployed
Total: 12.4 million
Source: US Census Bureau, Current Population Survey, Annual Social and Economic Supplement, 2006 http://www.census.gov/hhes/www/cpstc/cps_table_creator.html

Girls, Adolescent Girls, and Women’s Eligibility for Medicaid
Children below federal minimum income levels
– Ages 1-6: 133% FPL– Ages 6-19: 100% FPL
Adults in families with children (Section 1931 and TMA)
Pregnant women <133% FPL
Disabled SSI beneficiaries
Children above federal minimum income levels
Children ages 19-21
Adults in families with children (above Section 1931 minimums)
Pregnant women >133% FPL
Disabled (above SSI levels)
Disabled (under HCBS waiver)
Medically needy
Mandatory Populations Optional Populations

Income Eligibility Levels for Income Eligibility Levels for Medicaid for Pregnant Medicaid for Pregnant Women, 2006Women, 2006
Number of States
8
41 1
20
2 1
13 and DC
133% 150% 166% 175% 185% 200% 250% 275%
Source: Kaiser Family Foundation, 2006 http:www.statehealthfacts.org

Income Eligibility Levels for Income Eligibility Levels for Medicaid for Women as Medicaid for Women as Parents, 2006Parents, 2006
Number of States
30
94
0
14
23
5 61
6 &DC
1
1&DC
<50%FPL
51-100%FPL
101-150%FPL
151-200%FPL
201-250%FPL
275%FPL
Non-working parents Working parents
Source: Kaiser Family Foundation, 2006 http:www.statehealthfacts.org

Medicaid Defined BenefitsMedicaid Defined Benefits
Physicians services Laboratory and x-ray
services Inpatient hospital services Outpatient hospital services Early and periodic
screening, diagnostic, and treatment (EPSDT) services for individuals under 21
Family planning and supplies
Federally-qualified health center (FQHC) services
Rural health clinic services Nurse midwife services Certified nurse practitioner
services Nursing facility (NF) services
for individuals 21 or over
Prescription drugs Medical/remedial care furnished by licensed
practitioners Diagnostic, screening, preventive, and rehab services Clinic services Dental services, dentures Physical therapy Prosthetic devices, eyeglasses TB-related services Primary care case management ICF/MR services Inpatient/nursing facility services for individuals 65
and over in an institution for mental diseases (IMD) Inpatient psychiatric hospital services for individuals
under age 21 Home health care services Respiratory care services for ventilator-dependent
individuals Personal care services Private duty nursing services Hospice services
“Mandatory” Items and Services “Optional” Items and Services
Source: KFF, 2005.

Purposes of Family PlanningPurposes of Family Planning
Provide individuals with personal choice in determining the number and spacing of their children and in preventing unintended pregnancies
Ensure individuals’ reproductive health and well-being (through, e.g., prevention of STDs and HIV, routine cancer screenings)

Unintended pregnancy in Unintended pregnancy in the USthe US
Unintended pregnancy includes “Mistimed” (wanted to become pregnant in the future, but not yet) and “Unwanted” (did not want to become pregnant now or in the future)
Associated with delayed PNC and substance abuse during pregnancy, which may lead to adverse birth outcomes

Unintended pregnancy in Unintended pregnancy in the US (Cont.)the US (Cont.)
Of the 6.4 million pregnancies in US in 2001, 49% were unintended; of the 4 million births, 1.4 million were from an unintended pregnancy40% of women who had an unplanned
birth had used contraception during the month of conception
More prevalent in poor and low-income women

Rates of Unintended Rates of Unintended Pregnancy, by Race/Ethnicity Pregnancy, by Race/Ethnicity and Income, 2001and Income, 2001
0
20
40
60
80
100
120
140
160
180
All <100% FPL >100% FPL
AllWhiteHispanicBlack
Unintended Pregnancies per 1,000 Women
Source: Finer & Henshaw, 2006 Finer & Henshaw, 2006 Perspectives on Sexual and Reproductive Perspectives on Sexual and Reproductive Health, 38(2)Health, 38(2)

Basics of Medicaid FP Basics of Medicaid FP Waiver ProgramsWaiver Programs
Under Section 1115 of SSA Allows states to expand eligibility to
women who otherwise do not qualify for Medicaid specifically for Medicaid FP services– Can be based on loss of eligibility of women
postpartum or for any reason (e.g., starting a job)
– Ineligibility due to income levels First waiver approved by HHS in 1993
(SC)

26 States Have Medicaid 26 States Have Medicaid Family Planning Waivers Family Planning Waivers
5 states—for women who have lost Medicaid eligibility postpartum
2 states—for women who have lost Medicaid eligibility for any reason
19 states—based on income; ~200% FPL
(2001: ~ 1.7 million clients served in 13 states)
Source: Guttmacher Institute, 2007 SPIB: State Medicaid Family Planning Guttmacher Institute, 2007 SPIB: State Medicaid Family Planning Eligibility Expansions; Gold, 2003 Eligibility Expansions; Gold, 2003 “Medicaid Family Planning Extensions Hit Stride”
Services Provided Through Services Provided Through Medicaid Family Planning Medicaid Family Planning Waiver ProgramsWaiver Programs Coverage of FP services and
supplies available to Medicaid enrollees in the state
No cost-sharing FP services and supplies
reimbursed 90% by federal government; other services (e.g. STD testing) reimbursed at usual matching rate for the state
Source: Frost et al., 2006 “Estimating the impact of expanding Medicaid Frost et al., 2006 “Estimating the impact of expanding Medicaid eligibility for family planning services”eligibility for family planning services”

Evidence of Impact of FP Waivers Evidence of Impact of FP Waivers
on Program Costs and on Program Costs and Unintended PregnanciesUnintended Pregnancies Budget neutral but not always reduction in
number of unintended pregnancies (Edwards, Bronstein & Adams, 2003)
CA program prevented 108,000 unintended pregnancies in 1997-98 (Foster et al., 2004)
Simulation of income-based expansions to 200% and 250% of FPL found it would be cost-effective if implemented nationally (Frost, Sonfield and Gold, 2006)
Income-based expansions are effective at reducing births; save money or are at least budget neutral for states; and are at least budget neutral nationally (Lindrooth and McClullough, 2007)

Strengthening the Design of Strengthening the Design of Family Planning Waivers in Family Planning Waivers in Relation to Preconception CareRelation to Preconception Care

A. Coverage & Payment of Quality FP and Preconception Care
What are the guidelines for a quality FP and preconception care benefit (e.g., CMS, CDC, ACOG/AAP)?
What are the services covered and paid by States (e.g., survey of preconception benefits and CPT codes recognized by states for reimbursement within FP waivers)?
To what extent does state coverage and payment reflect the standard of care and are there opportunities for a core benefit to increase ability to ensure quality?
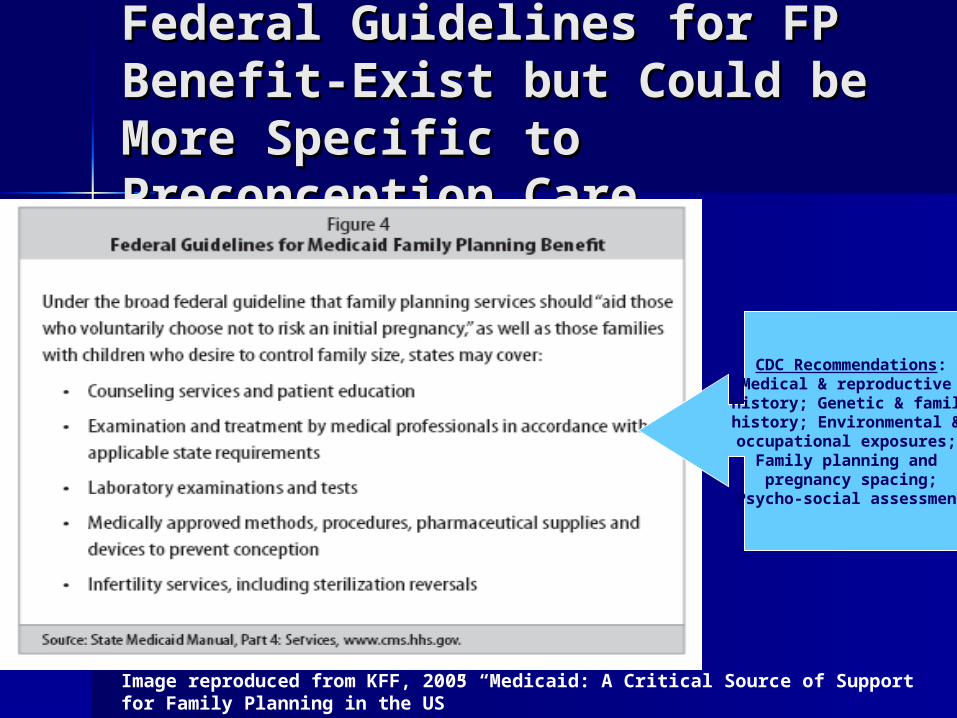
Federal Guidelines for FP Federal Guidelines for FP Benefit-Exist but Could be Benefit-Exist but Could be More Specific to More Specific to Preconception CarePreconception Care
Image reproduced from KFF, 2005 “Medicaid: A Critical Source of Support for Family Planning in the US”
CDC Recommendations:Medical & reproductive history; Genetic & familyhistory; Environmental & occupational exposures;
Family planning and pregnancy spacing;
Psycho-social assessment

Examples of CPT Codes
99384/94 (12-17 yrs); 385/95 (18-39 yrs); 386/96 (40-64 yrs) -Preventive (no symptoms), new/established patient
99420: Health risk assessment instrument for MH/SA services
99501-Home visit for postnatal assessment and follow-up care
96152- Health and behavior intervention

B. Coordination of FP B. Coordination of FP with Health Centerswith Health Centers 2001 requirement for states with FP waivers to set
up formal arrangements with CHCs to provide primary care services to enrollees in the FP programs
Enrollees must also be informed of how to access primary care services at CHCs
Arrangements could be used to increase link between family planning and preconception services– Is coordination happening?– What services are provided?– How about primary care providers other than health
centers?

C. Seamless Coverage C. Seamless Coverage with SCHIPwith SCHIP
In FY06, 671,000 adults (parents, pregnant women, and childless adults) were covered through SCHIP
In 2004, 17% (~3.3 million) of uninsured women were ages 18-24, some of whom may be “aging out” of SCHIP (>19) or Medicaid (>21)
SCHIP reauthorization– What will become possible with the reauthorization
statute?– Medicaid expansion for children (e.g., 300% FPL)
coordinated with a new SCHIP option to cover young adults?

Monitoring, and Tying Payment to, Quality of Preconception Care through the HEDIS Measurement System

CDC RecommendationCDC Recommendation
Maximize public health surveillance and related research mechanisms to monitor preconception health. Examples:– National PRAMS, BRFSS, NSFG– State and local PRAMS, Perinatal Periods of
Risk, Fetal-Infant Mortality Review, YRBS– Title V performance indicators– KFF survey
Maximize quality assurance mechanisms to monitor and improve preconception health– HEDIS

Receipt of Family Planning Receipt of Family Planning and Reproductive Health and Reproductive Health Services Among US Women Services Among US Women Ages 15-44Ages 15-44 According to the
2002 NSFG, the majority of US women ages 15-44 (72.7%) received at least one family planning or medical service in the past year
Receipt of services by type of provider, 2002
8.812.6
2
56
Title Xclinic
Otherclinic
PrivateMD/ HMO
Other
Source: Chandra et al., 2005 Chandra et al., 2005 2002 National Survey of Family Growth2002 National Survey of Family Growth

Receipt and Provider of Receipt and Provider of Family Planning and Family Planning and Reproductive Health Services Reproductive Health Services Vary by Poverty LevelVary by Poverty Level
Percent of women age 15-44 who received at least one
family planning or reproductive health service in
the past year, by poverty
73 74 83
0-149% FPL 150-299%FPL
300% + FPL
Provider of services, by poverty level
1520
43
28
12
60
28
24
74
Title Xclinic
Otherclinic
PrivateMD/ HMO
Other
0-149% FPL 150-299% FPL
300% + FPL
Source: Chandra et al., 2005 Chandra et al., 2005 2002 National Survey of Family Growth2002 National Survey of Family Growth

Survey of MCH programsSurvey of MCH programs

Content of Health Care Content of Health Care Among US Women, 2004Among US Women, 2004
Discussed with provider in the Discussed with provider in the past 3 years:past 3 years:31% had discussed their sexual 31% had discussed their sexual
historyhistory28% had discussed STDs 28% had discussed STDs 31% had discussed HIV/AIDS31% had discussed HIV/AIDS14% had discussed EC14% had discussed EC
Source: Kaiser Family Foundation, 2005 Women and Health Care: A National Profile

HEDIS Measurement HEDIS Measurement SystemSystem “The Healthcare Effectiveness Data and
Information Set (HEDIS) is a tool used by more than 90 percent of America's health plans to measure performance on important dimensions of care and service” – 3 main areas: Access/Availability of Care,
Effectiveness of Care, Use of Services Voluntary reporting to NCQA by commercial,
Medicaid and Medicare plans (> 73% of all 73% of all HMOs/POS plans, and 80 PPOs), which serve HMOs/POS plans, and 80 PPOs), which serve 80 million Americans80 million Americans, with national benchmark
Source: http://web.ncqa.org/tabid/59/Default.aspx

Measures Reflect Measures Reflect Evidence-and/or Evidence-and/or Consensus-Based Clinical Consensus-Based Clinical Practice Practice ACOG Guidelines
– To give practitioners the chance to offer advice and assistance, women should see their health care provider at least once between four and six weeks after giving birth. The first postpartum visit should include a physical examination and an opportunity for the health care practitioner to answer parents' questions and give family planning guidance and counseling on nutrition.
Guidelines for Perinatal Care – AAP & ACOG– All health encounters during reproductive years
should include counseling on appropriate medical care and behavior to optimize pregnancy outcomes.

CDC RecommendationsCDC Recommendations
Specifically focused on pre-and inter-conception care
Essential part of primary and preventive care
Not just a single visit/multiple visits, but the process of care and interventions, which can include a pre-pregnancy visit, multiple postpartum visits, PNC, and an array of other services and procedures (i.e., assessment, counseling, brief treatment)

Measures Link to Health Measures Link to Health Risk Factors, Women, Risk Factors, Women, Ages 18-44, 2002Ages 18-44, 2002 6% had asthma6% had asthma 50% were overweight/obese50% were overweight/obese 3% had cardiac disease3% had cardiac disease 3% were hypertensive3% were hypertensive 9% had diabetes9% had diabetes 1% suffered from thyroid disorder1% suffered from thyroid disorder >80% (ages 20-39) had dental carries >80% (ages 20-39) had dental carries
and other oral diseases and other oral diseases
Source: CDC, 2006.

Measures Link to Behavioral Risk Factors, Women, Ages 18-44, 2003 & 2005 21.7% smoked (2005) and 11% of
pregnant women smoked (2003) 11% reported binge drinking in the last
month (2005) and 10% of pregnant women drank alcohol (2003)
84% reported hearing of folic acid (of those aware of folic acid, 19% knew it prevents birth defects, 7% knew it should be taken before pregnancy); 33% took a daily multivitamin with folic acid (2005)
49% have unplanned pregnancies (2005)Source: March of Dimes, www.marchofdimes.com/peristats, 2005; CDC, 2003
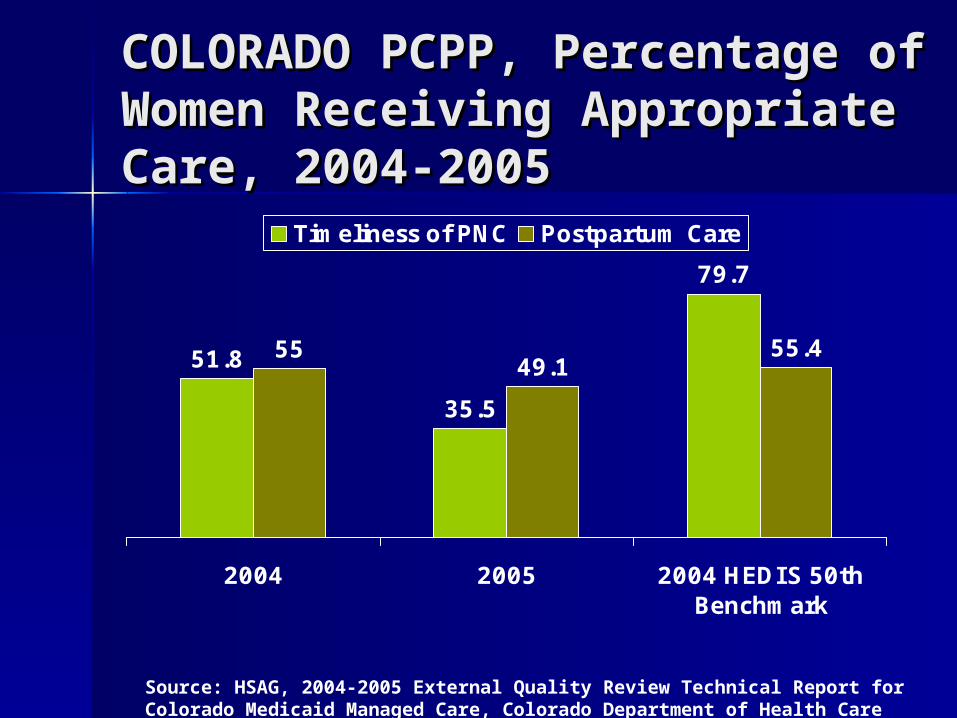
COLORADO PCPP, Percentage COLORADO PCPP, Percentage of Women Receiving of Women Receiving Appropriate Care, 2004-2005Appropriate Care, 2004-2005
51.8
35.5
79.7
5549.1
55.4
2004 2005 2004 HEDIS 50thBenchmark
Timeliness of PNC Postpartum Care
Source: HSAG, 2004-2005 External Quality Review Technical Report for Colorado Medicaid Managed Care, Colorado Department of Health Care Policy and Financing

COLORADO Perinatal Focused Study, Percentage of Women Receiving Appropriate Care, 2004
0102030405060708090
100
Timeliness ofPNC
SA Screening TobaccoCessationScreening
TobaccoCessationEducation
Urinalysiswith Culture
Testing
PriorPreterm
Delivery andHistory
Evaluation
PretermBirth Risk
Assessment
ChlamydiaScreening
PostpartumCare
CO Access RMHP PCPP
Source: HSAG, 2004-2005 External Quality Review Technical Report for Colorado Medicaid Managed Care, Colorado Department of Health Care Policy and Financing

NEW YORK QARR, Percentage of Women Receiving Appropriate Care, 2004
0
10
20
30
40
50
60
70
80
90
100
Timeliness of PNC Postpartum Care Cervical CancerScreening
Chlamydia Screening(ages 16-20)
Chlamydia Screening(ages 21-25)
Commercial2004 Commercial National AverageMedicaid2004 Medicaid National Average
Source: HSAG, 2004-2005 External Quality Review Technical Report for Colorado Medicaid Managed Care, Colorado Department of Health Care Policy and Financing

NEW YORK QARR, Percentage of Medicaid Women Receiving Appropriate Care, 2002-2004
0102030405060708090
Timeliness of PNC Postpartum Care Cervical CancerScreening
Chlamydia Screening(ages 16-20)
Chlamydia Screening(ages 21-25)
2002 2004 2004 Medicaid National Average
Source: HSAG, 2004-2005 External Quality Review Technical Report for Colorado Medicaid Managed Care, Colorado Department of Health Care Policy and Financing

Using Existing HEDIS Measures –Postpartum Visit
Postpartum care (access/availability of care): % of deliveries that had a postpartum visit on or between 21 days and 56 days after delivery
– 2005: Average % of women who received a post-partum visit 21-56 days after delivery was 81.5% for commercial and 57% for Medicaid health plans
Chance to provide preconception advice in preparation for subsequent pregnancy
Source: National Committee for Quality Assurance, 2006 National Committee for Quality Assurance, 2006 The State of The State of Health Care Quality 2006Health Care Quality 2006

Modifying Existing HEDIS Measures for Preconception Care – Preventive Visits
Ambulatory or Preventive Visit (access/ availability of care): Percentage of adults ages 20-44 who had an ambulatory or preventive visit – 2005: Average % of adults who received a
ambulatory or preventive visit was 92.7% for commercial and 76.4% for Medicaid health plans
Stratification by gender
Chance to provide preconception advice in preparation for initial and/or subsequent pregnancy

Other Possible HEDIS Measures for Preconception Care CDC recommendations list preconception risk
factors, these could be linked with existing HEDIS measures. E.g., Alcohol misuse: HEDIS measure Initiation and
Engagement of Alcohol and Other Drug Dependence Treatment (stratified by ages 20-44 and gender?)
Hep B: HEDIS measure Adolescent Immunization Status (extended to ages 20-44 and stratified by gender?)
STD: HEDIS measure Chlamydia Screening, Ages 16-25 (extended to age 44 and stratified by gender?)
Smoking: HEDIS measure Medical Assistance with Smoking Cessation (stratified by ages 20-44 and gender?)
Source: National Committee for Quality Assurance, 2006 National Committee for Quality Assurance, 2006 The State of The State of Health Care Quality 2006Health Care Quality 2006

Other Proposed Measures of Preconception Care Quality
Working group of OB/GYNs and perinatologists proposed 90 potential indicators for maternal quality of care
Indicators chosen for preconception/interconception care:Rubella statusPap smear testingDiabetic screeningFolic acid use
Korst et al., 2005 Maternal and Child Health Journal, 9(3)

NCQA Process to Add a HEDIS Measure 7 months: Initial selection and
development
9 months: Field testing
12 months: Revision, public comment, vote, and addition to existing set of measures
TOTAL: 28 months

State Medicaid/SCHIP EQRO Contracting Development and validation of new
performance measures of preconception and interconception care, as defined by state
Focus study on perinatal care, preconception care, interconception care, as defined by state
PIP on perinatal care, preconception care, interconception care, as defined by state

P4P – Definition
Payor (public and private) strategies to reorient payment incentives and instill accountability by rewarding efforts to improve quality
Part of broader quality improvement effort
Both financial and nonfinancial incentives may be used to improve measurable performance
Incentives should encourage and reinforce use of evidence-based practices that promote better outcomes efficiently Source: Abramson, S. & Younger, K. Pay-for-Performance Literature
Review, Washington, DC: Department of Health Policy, GWU, SPHHS, May 2006.

P4P - GoalsP4P - Goals
Improve quality of careImprove quality of care Reduce variation in patterns of careReduce variation in patterns of care Facilitate access to careFacilitate access to care Integrate evidence-based medicineIntegrate evidence-based medicine Improve efficiencyImprove efficiency Ensure accountability Ensure accountability
Source: Abramson, S. & Younger, K. Pay-for-Performance Literature Review, Washington, DC: Department of Health Policy, GWU, SPHHS, May 2006.
P4P – Evidence of Impact on Quality Limited evidence of direct impact on quality
One study by Rosenthal (2005)– No impact of financial incentives for
hemoglobin A1c testing and mammography; small positive increase in cervical cancer screening
– Lowest performers at baseline improved the most, but received smallest share of bonus payments; best performers at start were biggest winners
Source: Abramson, S. & Younger, K. Pay-for-Performance Literature Review, Washington, DC: Department of Health Policy, GWU, SPHHS, May 2006.
P4P - Incentive/Penalty Arrangements Financial
– Challenge/bonus pools for performance rewards– Withhold/recoupment from payments– Auto-assignment– Enrollment frozen– Health plan non-renewal
Non-Financial – Public reporting (e.g., report cards, newspaper articles)– Public acclamation (e.g., public awards by Mayor)– Partnership between MCO’s and DHS staff with commitment to
quality– Waiver of administrative requirementsSource: Abramson, S. & Younger, K. Pay-for-Performance Literature
Review, Washington, DC: Department of Health Policy, GWU, SPHHS, May 2006.

HEDIS and P4P
Good starting point for P4P measures
Nationally validated and comparable measures
However, limited measures of preconception and interconception care
Focus is on process, not outcomeSource: Abramson, S. & Younger, K. Pay-for-Performance Literature Review, Washington, DC: Department of Health Policy, GWU, SPHHS, May 2006.