pre operative cardiac assessment dr sadany-1
TRANSCRIPT

Guidelines for pre-operative cardiac
assessment

Introduction Pre-operative evaluationRisk reductionSpecific conditions

Introduction

LT .coronary artery

RT.coronary artery

Cardiac patient has a potential source of complications during surgery
The risk of peri-operative complications depends on the condition of the patient prior to surgery, the prevalence of co-morbidities, and the magnitude and duration of the surgical procedure.
Introduction
Within the next 20 years, the acceleration in ageing of the population will have a major impact on peri-operative patient management.
It is estimated that elderly people require surgery four times more often than the rest of the population.
Introduction

Pre-operative evaluation
An emergency procedure:It is one in which life or limb is threatened if
not in the operating room where there is time for no or very limited or minimal clinical evaluation (within <6 hours).
An urgent procedure: It is one in which there may be time for a
limited clinical evaluation, usually when life or limb is threatened if not in the operating room (between 6 and 24 hours).
Definitions

Time-sensitive procedure:It is one in which a delay of >1 to 6 weeks to
allow for an evaluation and significant changes in management will negatively affect outcome. (oncologic procedures).
An elective procedure:It is one in which the procedure could be
delayed for up to 1 year.
Definitions

Every operation elicits a stress response. This response is initiated by tissue injury
and mediated by neuroendocrine factors, and may induce tachycardia and hypertension.
Fluid shifts in the peri-operative period add to the surgical stress leading to myocardial O2 imbalance.
Surgical risk for cardiac events

High-risk ≥1%

Recently surgical interventions have been divided into two categories :
1. Low-risk (<1%) Operations without significant fluid shifts
and stress (plastic and cataract).2. High-risk(≥ 1%) Operations including supra-inguinal
vascular, intra-peritoneal, or intra-thoracic.
Surgical risk for cardiac events

Major predictor:1. Unstable coronary syndromes: unstable or
severe angina or recent MI2. Decompensated HF3. Significant arrhythmias4. Severe valvular disease.
Patient-related risk factor
Intermediate predictors:1.History of ischemic heart disease2.History of HF3.History of cerebrovascular disease4.Diabetes mellitus requiring treatment
with insulin5.Preoperative serum creatinine >2.0
mg/dL
Patient-related risk factor

Minor predictor:1. Advanced age (greater than 70 years).2. Abnormal ECG (LV hypertrophy, left
bundle-branch block, ST-T abnormalities).3. Rhythm other than sinus.4. Uncontrolled systemic hypertension.
Patient-related risk factor

1. Myocardial infarction.2. Pulmonary edema.3. Ventricular fibrillation .4. Primary cardiac arrest.5. Complete heart block.6. Undergoing supra-inguinal vascular, intra-
peritoneal, or intra-thoracic surgery. A patient with 0 or 1 predictor(s) of risk would
have a low risk of MACE. Patients with ≥2 predictors of risk would have
elevated risk.
Revised Cardiac Risk Index

Coronary Artery Disease CAD
Patient-related risk factor
Mortality rate (%) MI rate (%) Timing (days)
14.2 32.8 0 -30
11.5 18.7 31-60
10.8 8.4 61-90
9.9 5.9 91-180

Patient’s age Adults aged > 55 years have a growing
prevalence of CVD, CVS, and diabetes mellitus.
Adults aged > 65 years have a higher reported incidence of acute ischemic stroke.
Aged > 70 years have more postoperative complications, increased length of hospitalization, and inability to return home alone after hospitalization.
Patient-related risk factor

Heart failure Survival after surgery for those with a LVEF
≤ 29% is significantly worse than for those with a LVEF >29%.
In a meta-analysis using individual patient data, patients with HF and preserved LVEF had a lower all-cause mortality rate than that of those with HF and reduced LVEF (the risk of death did not increase notably until LVEF fell below 40%)
Patient-related risk factor
Functional capacity is measured in metabolic equivalents (METs).
One MET equals the basal metabolic rate. 1 MET represents metabolic demand at rest. Climbing two flights of stairs demands 4
METs Strenuous sports such as swimming
represents >10 METS
Functional capacity


Stepwise Approach to Peri-operative Cardiac Assessment


Class I Patients who have a need for emergency
non-cardiac surgery should proceed to the operating room and continue peri-operative surveillance and postoperative risk stratification and risk factor management. (Level of Evidence: C)
Emergency surgery
Cardiac assessment
Patients with active cardiac conditions should be evaluated and treated per American Chest Coleuge/American Heart Association ACC/AHA guidelines and, if appropriate, consider proceeding to the operating room. (Level of Evidence: B)
Decompensated Active management
Cardiac assessment

Patients undergoing low risk surgery are recommended to proceed to planned surgery. (Level of Evidence: B)
Low surgery proceed to surgery Patients with poor (less than 4 METs) or
unknown functional capacity and no clinical risk factors should proceed with planned surgery. (Level of Evidence: B)
Poor function + No risk proceed to surgery
Cardiac assessment

It is probably recommended that patients with poor (less than 4 METs) or unknown functional capacity and ≥ 2 clinical risk factors consider testing if it will change management.(Level of evidence:B)
Poor function + ≥ 2 risk factors Non-invasive test
Cardiac assessment

It is probably recommended that patients with poor (less than 4 METs) or unknown functional capacity and < 2 clinical risk factors proceed with planned surgery with heart rate control. (Level of Evidence: B)
Unknown function + Low-Risk Proceed with HR control
Cardiac assessment

Pre-operative non-invasive testing aims at providing information on three cardiac risk markers:
1.LV dysfunction2.Myocardial ischaemia3.Heart valve abnormalities
Non-invasive testing

LV function is assessed at rest, and various imaging modalities:
1. Echocardiography2. Thallium imaging3. Radionuclide angiography For myocardial ischaemia detection,
exercise ECG and non-invasive imaging techniques may be used.
Echocardiography is preferred for evaluation of valve disease.
Cardiac assessment

Level Class Recommendations
B IIa Preoperative resting 12-lead electrocardiogram (ECG) is reasonable for patients with known coronary heart disease, significant arrhythmia, peripheral arterial disease, cerebrovascular disease, or other significant structural heart disease, except for those undergoing low-risk surgery
B IIb Preoperative resting 12-lead ECG may be considered for asymptomatic patients without known coronary heart disease, except for those undergoing low-risk surgery
B III Routine preoperative resting 12-lead ECG is not useful for asymptomatic patients undergoing low-risk surgical procedures
Recommendations on ECG
Level Class Recommendations
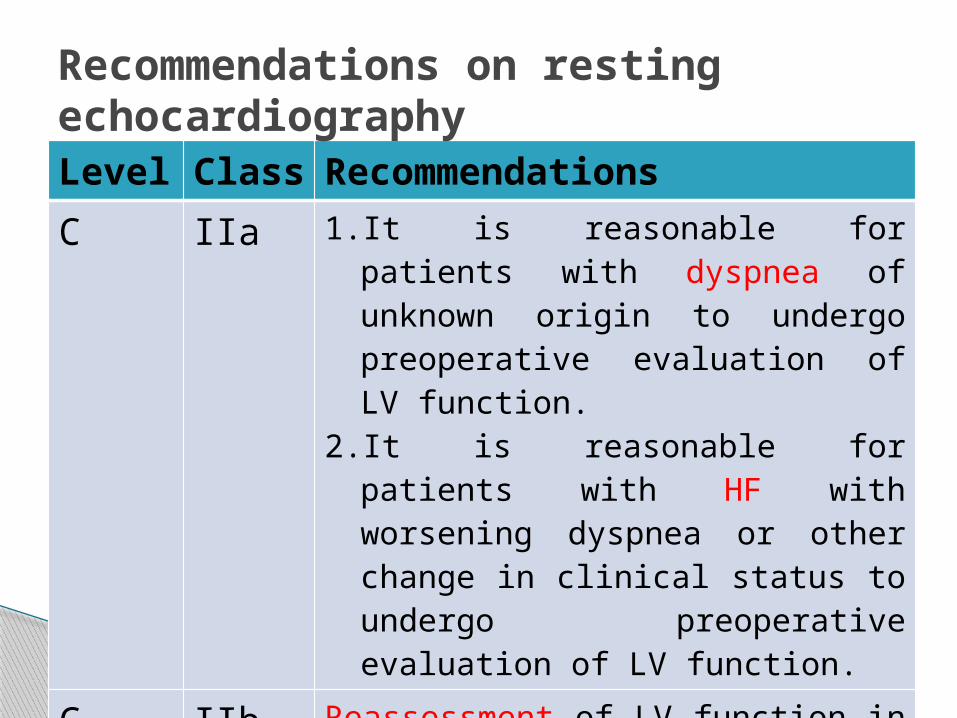
C IIa 1. It is reasonable for patients with dyspnea of unknown origin to undergo preoperative evaluation of LV function.
2. It is reasonable for patients with HF with worsening dyspnea or other change in clinical status to undergo preoperative evaluation of LV function.
C IIb Reassessment of LV function in clinically stable patients with previously documented LV dysfunction may be considered if there has been no assessment within a year.
B III Routine preoperative evaluation of LV function is not recommended
Recommendations on resting echocardiography

Exercise Stress Testing for MI & Functional Capacity
Level Class RecommendationsB IIa For patients with elevated risk and excellent (>10 METs)
functional capacity, it is reasonable to forget further exercise testing with cardiac imaging and proceed to surgery.
B
B
C
IIb
IIb
IIb
1. For patients with elevated risk and unknown functional capacity, it may be reasonable to perform exercise testing to assess for functional capacity if it will change management.
2. For patients with elevated risk and moderate to good (≥4 METs to 10 METs) functional capacity, it may be reasonable to forget further exercise testing with cardiac imaging and proceed to surgery
3. For patients with elevated risk and poor (<4 METs) or unknown functional capacity, it may be reasonable to perform exercise testing with cardiac imaging to assess for myocardial ischemia if it will change management.
B III Routine screening with noninvasive stress testing is not useful for patients at low risk for non-cardiac surgery

Recommendations on non-invasive pharmacological stress testing
Level Class RecommendationsC IIa It is reasonable for patients who are at an
elevated risk for non-cardiac surgery and have poor functional capacity (<4 METs) to undergo noninvasive pharmacological stress testing (either dobutamine stress echocardiogram [DSE] or pharmacological stress myocardial perfusion imaging [MPI]) if it will change management.
B III Routine screening with non-invasive pharmacological stress testing is not useful for patients undergoing low-risk non-cardiac surgery.

Recommendation for Cardiopulmonary Exercise TestingLevel Class Recommendations
B IIB Cardiopulmonary exercise testing may be considered for patients undergoing elevated risk procedures in whom functional capacity is unknown

Cardiopulmonary exercise testing (CPET) provides a global assessment of the integrated response to exercise involving the pulmonary, cardiovascular, and skeletal muscle systems.
CPET is a programmed exercise test on either a cycle ergometer or a treadmill during which inspired and expired gases are measured through a facemask or a mouthpiece.
This test provides information on oxygen uptake and utilization.
Integrated assessment of cardiopulmonary function

The thresholds for classifying patients as low risk are usually taken as VO2 >15 mL/kg/ min and AT > 11 mL/kg/min
A VO2 < 12 mL/kg/min was associated with a 13-fold higher rate of mortality.
Integrated assessment of cardiopulmonary function

CLASS I Coronary revascularization before non-
cardiac surgery is useful in patients with stable angina who have significant left main coronary artery stenosis. (Level of Evidence: A)
Coronary revascularization before non-cardiac surgery is useful in patients with stable angina who have 3-vessel disease. (Survival benefit is greater when LVEF is less than 50%) (Level of Evidence: A)
Recommendations on preoperative coronary angiography

Coronary revascularization before noncardiac surgery is useful in patients with stable angina who have 2-vessel disease with significant proximal LAD stenosis and either EF less than 50% or demonstrable ischemia on noninvasive testing. (Level of Evidence: A)
Coronary revascularization before non-cardiac surgery is recommended for patients with high-risk unstable angina or non–St segment elevation MI. (Level of Evidence: A)
Recommendations on preoperative coronary angiography

Coronary revascularization before non-cardiac surgery is recommended in patients with acute ST-elevation MI. (Level of Evidence: A)
Recommendations on preoperative coronary angiography

Recommendations for Timing of Elective Non-cardiac Surgery in Patients With Previous PCILevel Class RecommendationsC
B
B
I
I
I
1. Elective non-cardiac surgery should be delayed 14 days after balloon angioplasty
2. Elective non-cardiac surgery should be delayed 30 days after BMS implantation
3. Elective non-cardiac surgery should optimally be delayed 365 days after drug-eluting stent (DES) implantation.
C IIa In patients in whom non-cardiac surgery is required, a consensus decision among treating clinicians as to the relative risks of surgery and discontinuation or continuation of anti-platelet therapy can be useful.
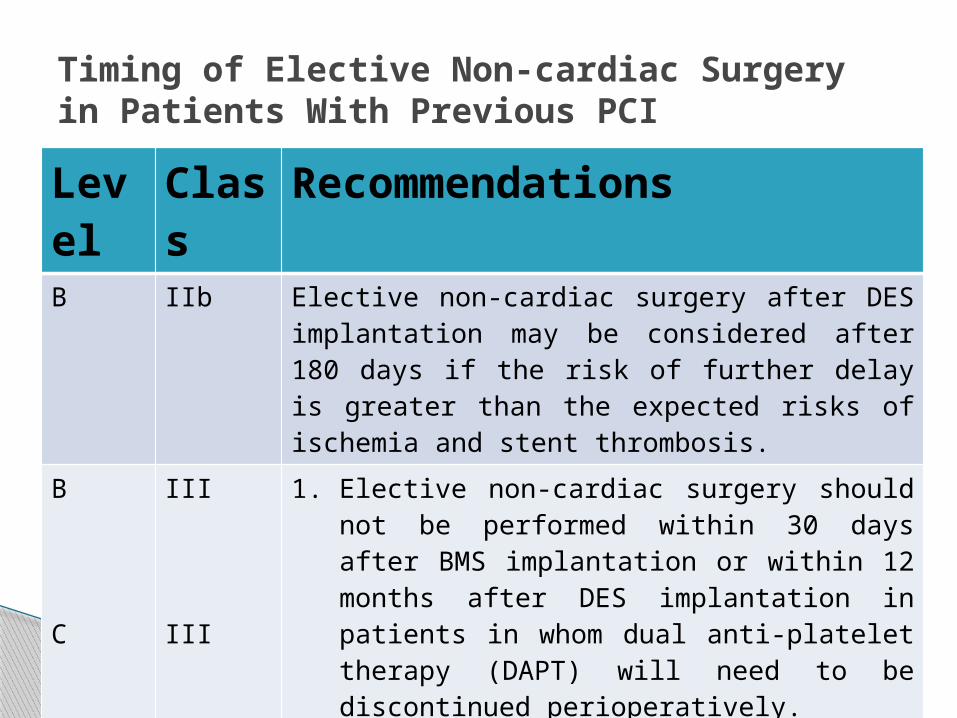
Timing of Elective Non-cardiac Surgery in Patients With Previous PCI
Level Class RecommendationsB IIb Elective non-cardiac surgery after DES implantation may
be considered after 180 days if the risk of further delay is greater than the expected risks of ischemia and stent thrombosis.
B
C
III
III
1. Elective non-cardiac surgery should not be performed within 30 days after BMS implantation or within 12 months after DES implantation in patients in whom dual anti-platelet therapy (DAPT) will need to be discontinued perioperatively.
2. Elective non-cardiac surgery should not be performed within 14 days of balloon angioplasty in patients in whom aspirin will need to be discontinued perioperatively.

Level Class RecommendationsB I Beta blockers should be continued in patients undergoing
surgery who have been on beta blockers chronically.
B IIa It is reasonable for the management of beta blockers after surgery to be guided by clinical circumstances, independent of when the agent was started.
C
B
Iib
IIb
1. In patients with intermediate- or high-risk myocardial ischemia noted in pre-operative risk stratification tests, it may be reasonable to begin peri-operative beta blockers.
2. In patients with 3 or more RCRI risk factors (e.g., diabetes mellitus, HF, CAD, renal insufficiency, cerebrovascular accident), it may be reasonable to begin beta blockers before surgery.
b-Blockers

b-Blockers (continued)Level Class Recommendations
B
B
Iib
IIb
3. In patients with a compelling long-term indication for beta-blocker therapy but no other RCRI risk factors, initiating beta blockers in the perioperative setting as an approach to reduce perioperative risk is of uncertain benefit.
4. In patients in whom beta-blocker therapy is initiated, it may be reasonable to begin perioperative beta blockers long enough in advance to assess safety and tolerability, preferably more than 1 day before surgery.
B III Beta-blocker therapy should not be started on the day of surgery

Level Class RecommendationsB I Statins should be continued in patients currently
taking statins and scheduled for non-cardiac surgery.
B IIa Perioperative initiation of statin use is reasonable in patients undergoing vascular surgery.
C IIb Perioperative initiation of statins may be considered in patients with clinical indications according to GDMT who are undergoing elevated-risk procedures.
Perioperative Statin Therapy

Level Class Recommendations
B III Alpha-2 agonists for prevention of cardiac events are not recommended in patients who are undergoing non-cardiac surgery.
Alpha-2 Agonists

Angiotensin-Converting Enzyme InhibitorsLevel Class Recommendations
B
C
Iia
IIa
1. Continuation of angiotensin-converting enzyme (ACE) inhibitors or angiotensin-receptor blockers (ARBs) perioperatively is reasonable.
2. If ACE inhibitors or ARBs are held before surgery, it is reasonable to restart as soon as clinically feasible postoperatively.

Level Class RecommendationsC
C
C
I
I
I
1. In patients undergoing urgent non- cardiac surgery during the first 4 to 6 weeks after BMS or DES implantation, DAPT should be continued unless the relative risk of bleeding outweighs the benefit of the prevention of stent thrombosis.
2. In patients who have received coronary stents and must undergo surgical procedures that mandate the discontinuation of ADP platelet receptor–inhibitor therapy, it is recommended that aspirin be continued if possible and the ADP platelet receptor–inhibitor be restarted as soon as possible after surgery.
3. Management of the perioperative antiplatelet therapy should be determined by a consensus of the surgeon, anesthesiologist, cardiologist, and patient, who should weigh the relative risk of bleeding versus prevention of stent thrombosis.
Antiplatelet agents

Level Class RecommendationsB IIb In patients undergoing non-emergency/non-urgent non-cardiac
surgery who have not had previous coronary stenting, it may be reasonable to continue aspirin when the risk of potential increased cardiac events outweighs the risk of increased bleeding
B III Initiation or continuation of aspirin is not beneficial in patients undergoing elective non-cardiac non-carotid surgery who have not had previous coronary stenting.
C III Unless the risk of ischemic events outweighs the risk of surgical bleeding, initiation or continuation of aspirin is not beneficial in patients undergoing elective non-cardiac surgery
Antiplatelet agents (continued)

Specific conditions

It is recommend the use of ACE inhibitors (or ARBs in patients intolerant of ACE inhibitors) and b-blockers as primary treatment in chronic heart failure patients, to improve morbidity and mortality.
Chronic heart failure

In patients with an LV ejection fraction < 35% who remain severely symptomatic the addition of a low dose of aldosterone antagonist should be considered.
Diuretics are recommended in heart failure patients with signs or symptoms of congestion.
Chronic heart failure

It has been concluded that the perioperative use of ACE inhibitors, b-blockers, statins, and aspirin is independently associated with a reduced incidence of in-hospital mortality in patients with LV dysfunction who are undergoing major non-cardiac vascular surgery.
Chronic heart failure

In hypertensive patients with concomitant IHD who are at high risk of cardiovascular complications, peri-operative administration of b-blockers is recommended.
In patients with hypertension, anti-hypertensive therapy should be continued up to the morning of surgery.
Arterial hypertension

In patients with severe hypertension (SBP > 180 mmHg and/or DBP > 110 mmHg), the potential benefits of delaying surgery to optimize the pharmacological therapy should be weighed against the risk of delaying the surgical procedure.
Arterial hypertension
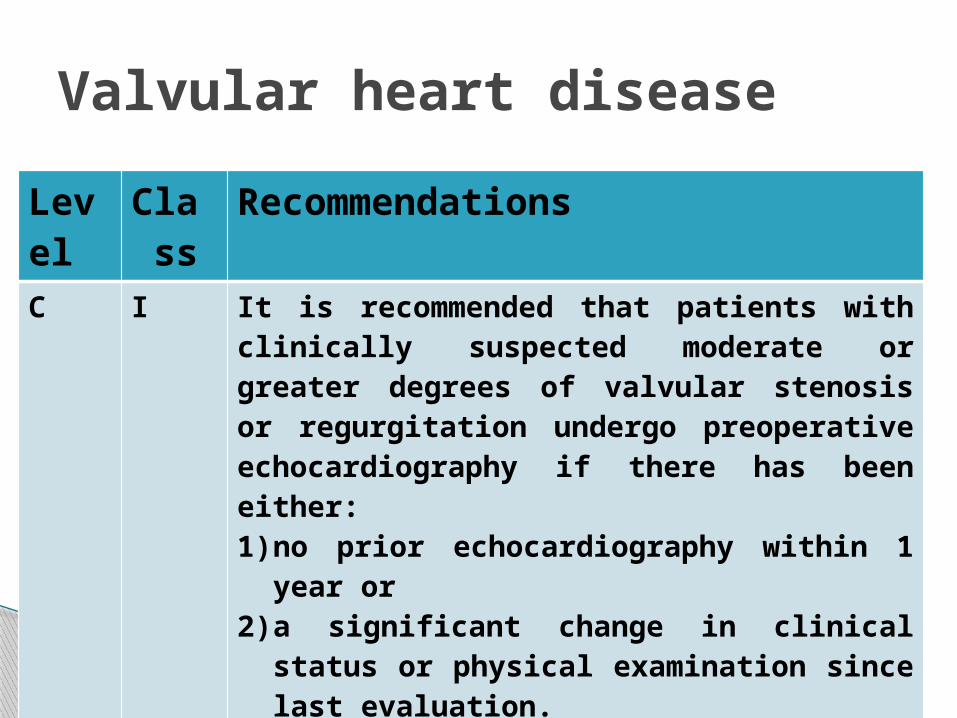
Valvular heart disease
Level Class Recommendations
C I It is recommended that patients with clinically suspected moderate or greater degrees of valvular stenosis or regurgitation undergo preoperative echocardiography if there has been either:1) no prior echocardiography within 1 year or 2) a significant change in clinical status or physical
examination since last evaluation.C I For adults who meet standard indications for valvular
intervention (replacement and repair) on the basis of symptoms and severity of stenosis or regurgitation, valvular intervention before elective non-cardiac surgery is effective in reducing perioperative risk.

Elevated-risk elective non-cardiac surgery with appropriate intra-operative and postoperative hemodynamic monitoring is reasonable to perform in patients with asymptomatic severe aortic stenosis (AS)
Class IIa (Level of Evidence: B)
Aortic stenosis

Maintain normal sinus rhythm Avoid bradycardia or tachycardia(60-90) Avoid hypotension Optimize intravascular fluid volume to
maintain venous return and left ventricular filling
Aortic stenosis
Elevated-risk elective non-cardiac surgery using appropriate intra-operative and postoperative hemodynamic monitoring may be reasonable in asymptomatic patients with severe mitral stenosis if valve morphology is not favorable for percutaneous mitral balloon commissurotomy. Class IIb (Level of Evidence: C)
Mitral stenosis

Patients with mitral stenosis who meet standard indications for valvular intervention (open mitral commissurotomy or percutaneous mitral balloon commissurotomy) should undergo valvular intervention before elective non-cardiac surgery.
If valve anatomy is not favorable for percutaneous mitral balloon commissurotomy, or if the non-cardiac surgery is an emergency, then non-cardiac surgery may be considered with invasive hemodynamic monitoring and optimization of loading conditions.
Mitral stenosis

Avoid sinus tachycardia or AF(60-90 beat / minute).
Avoid marked increase in central blood volume.
Avoid vasoactive drugs or use it cautiously. Avoid hypoxemia and/or hypercarbia that
may exacerbate pulmonary hypertension and evoke right ventricular failure.
Mitral stenosis

Proceed with non-cardiac surgery:1. In asymptomatic patients with severe
AR/MR and preserved LV function(mortality< 0.2%)
Proceed cautiously with non-cardiac surgery if so necessary in:
1. Asymptomatic with EF < 30%2. Symptomatic Optimize pharmacological therapy
(Nefidipine or hydralazine)
Aortic & Mitral Rregurgitation

Avoid bradycardia (keep above 80 beat/min)
Avoid increases in systemic vascular resistance
Minimize myocardial depression (if occurred it is treated by vasodilator with inotrope)
Aortic regurgitation

Mitral regurgitation

Prevent bradycardia (keep above 80 beat/min)
Prevent increases in systemic vascular resistance
Minimize drug-induced myocardial depression
In severe MR, monitor the magnitude of regurgitant flow with a pulmonary artery catheter and/or echocardiography
Maintenance of intravascular fluid volume
Mitral regurgitation

Symptomatic patients should undergo mitral valve surgery even if they have a normal ejection fraction.
Mitral valve repair is preferred to mitral valve replacement because it restores valve competence, maintains the functional aspects of the mitral valve apparatus, and avoids insertion of a prosthesis.
Mitral regurgitation

Patients with an ejection fraction of less than 30% or left ventricular end-systolic dimension more than 55 mm do not improve with mitral valve surgery
Mitral regurgitation

Cardiac patient has a potential source of complications during surgery
Revised cardiac risk index is the most reliable risk assessment.
Emergency operation has a higher morbidity and mortality.
b-blockers reduce peri-operative myocardial ischaemia.
Peri-operative use of ACE inhibitors, b-blockers and statins reduce mortality.
Summary

Postpone only patients with severe hypertension (> 180/110)
Avoid hypotension and treat it aggressively in severe AS.
Avoid sinus tachycardia or AF in severe MS In AR minimize myocardial depression (treat
by vasodilator with inotrope) In MR prevent increases in systemic
vascular resistance
Summary
Thanks