practicing to win
TRANSCRIPT


bcc consulting was founded in 2004 with the goal of integrating the art and science of healthcare. Despite healthcare’s dependence on technology, far too few organizations understand how to integrate new technologies into clinical practice - beginning with challenges related to system evaluation, selection, and contract negotiation, and finally culminating in system implementation.
Over the last few years, client necessity has required us to expand our offerings into business operations, primarily related to financial management and strategic planning, but also encompassing key tactical projects, such as sales and marketing campaigns.
The bottom line: results.

Copyright © 2008 bcc: Consulting. All Rights Reserved. 3
Practicing to Win
I have spent the last three years running my own “lab”— actually, it’s a primary care medical office. I describe it as a “lab” because I am first an owner in the business, and second the sole arbiter of our operational methodologies – or at least for all things business-related.
Having spent several years working for a successful healthcare IT start-up, before starting my own healthcare consulting company, I thought it was a perfect opportunity to put my money with mouth and help my wife start her own Family Medicine practice. She was hesitant, having only practiced for a year following residency, but was eager to “do things her way,” at least regarding all things medical. I say this, because unlike the majority of physicians I have worked with, she has a healthy appreciation of her strengths and weaknesses.
Other than the typical challenges – such as contractors who miss their time and budget estimates by more than 20% - I don’t think there was anything uniquely difficult about our situation. We were opening our practice between two of the country’s largest academic medical centers, one about 5 minutes away in one direction, and the other about 10 minutes in the opposite. My wife’s former practice was a good 30 minute drive away, so, other than a few die-hard patients, we were starting from scratch.
Luckily the debt markets were much friendlier back then. Despite a few sideways looks about starting a new practice between the two monolithic academic medical centers, the banks were all-too-happy to lend us the money to start the practice.

w w w . h i t b c c . c o m4
Our most important front-end decisionsEMR/PMSMy wife, having always used them, was more than comfortable employing one. Furthermore, other than a few reasonable parameters, she left the decision mostly up to me. I was very comfortable making this decision because I had worked very closely with many of the companies we were evaluating and knew their products quite well. In all honesty, the decision was a fairly simple one. We selected eClinicalWorks (eCW), a very small company in 2004, and today probably the dominant company in the integrated EMR/PMS market.
MarketingRelative to most medical offices, we have done a lot of it.
IPA MembershipAs an existing member in an independent physician association (IPA), my wife was able to bring her membership with her to the new practice.
ResultsWe started our practice with less than 30 patients, and 1 physician. Today, we have 3 physicians working an approximate 2.5 FTE (full-time equivalent) schedule, and a rapidly expanding patient-base currently around 4,500.
Supporting our physicians, we have 1 LPN, 1 clinical assistant, 1.5 FTE front-office staff, and a part-time office manager (me).
Our practice was cash flow positive with the physicians averaging 12.5 patients/day on their work days; this occurred approximately 19 months into operation. Our third year in business was profitable, and we expect our profitability to continue to grow. Our physicians currently average over 16 patients/day and we will continue to grow until we reach about 20 patients/day.
Early AssumptionsI earned an MBA with a concentration in Finance from the University of Chicago, Graduate School of Business. I say this simply to give credibility to my financial assumptions and to further add that becoming an “Office Manager” was never my ultimate goal.
With the continuing pressure on medicine, particularly primary care, it seems a fair question to ask why anyone would choose to start a primary care medical practice. My instinctive beliefs are founded in Albert Einstein’s famous saying, “In the midst of chaos lies opportunity.”
To explain that a little more clearly, I think it is impossible to graduate from Chicago (a bastion of conservative financial theory) and not walk
“In the midst of chaos
lies opportunity.”
— Albert Einstein

Copyright © 2008 bcc: Consulting. All Rights Reserved. 5
Practicing to Win
away with a firmly ingrained belief in efficient markets. A principle that does not say markets are always efficient, but that they tend towards efficiency…in the long run. Short-term inefficiencies frequently exist.
To go a little further, while there are clearly pressures on medicine, and primary care in particular, I was betting that the markets would eventually correct themselves. Furthermore, as bad as things get, neither the government nor the larger society will allow the 600,000 or so primary care physicians working in small practices to go out of business. That’s not to say that none will, but not all or even most.
In a deranged sort of way, it’s like the joke about the two campers in the woods who hear a Grizzly outside their tent. One starts to put his running shoes on and the other says, “You know, you can’t outrun a bear.” To which his sneaker-donning “friend” replies, “I know, I just have to outrun you.”
The System allows for poor management. If it didn’t, there would be far fewer doctors. In fact, I was willing to bet that if we performed in the top 5%, we could make a very good living. Nothing I have seen or learned has changed this impression.
Medical Practice as FactoryFirst off, I am advocating for no such thing. I think comparing a medical practice to a factory may help explain things in a way people can more intuitively understand.
To start with, let’s go ahead and call medical treatment, or care, the omnipresent “widget”. For arguments sake, let’s assume that every widget is exactly the same, regardless of who the physician or where the practice.
In order to produce widgets, medical practices are assembled as factories. Just as factories incur operating costs, so too do medical practices. We generally refer to these operating costs as our overhead, which is broken into two distinct categories: fixed costs, and variable costs.
As long as we are in the business of making and selling undifferentiated widgets, we are completely subject to the price the market sets for widgets—in economic terms, we are “price-takers.” Our goal in making widgets is not to make “better” widgets, but rather to reduce our cost for producing widgets, to sell more of them, or better, a combination of the two – make them cheaper and sell more.
The System allows for
poor management. If it
didn’t, there would be
far fewer doctors.
w w w . h i t b c c . c o m6
Before I explain how to accomplish this, I have to address the cacophony of upset readers who are protesting that, “We are most certainly not in the business of making widgets!”
Let me assure you, you are. Who sets your prices? Do they differentiate the same type and level of service based on quality? If you are inclined to ask why payers reimburse different physicians and groups differently for the same service, I assure you it has nothing to do with quality. It is entirely driven by volume. Those with the most leverage, in terms of most physicians treating the most number of patients, will nearly always be paid more, regardless of quality.
Without getting into a completely separate discussion of pay for performance, let me just say that it’s not happening any time soon, and it will not be led by the government or by payers. I will get back to this point later.
Certainly not all physicians are equal, and in turn not all service is equal. No one would dispute that. Is quality a necessary component of the product? Undeniably; however, this is a world of business, and in the world of business no one is currently placing a premium on quality1.
1 Or at least no one participating in the traditional system of healthcare. New models such as concierge medicine, arguably come much closer to a quality-based reward system.
S
D
P*
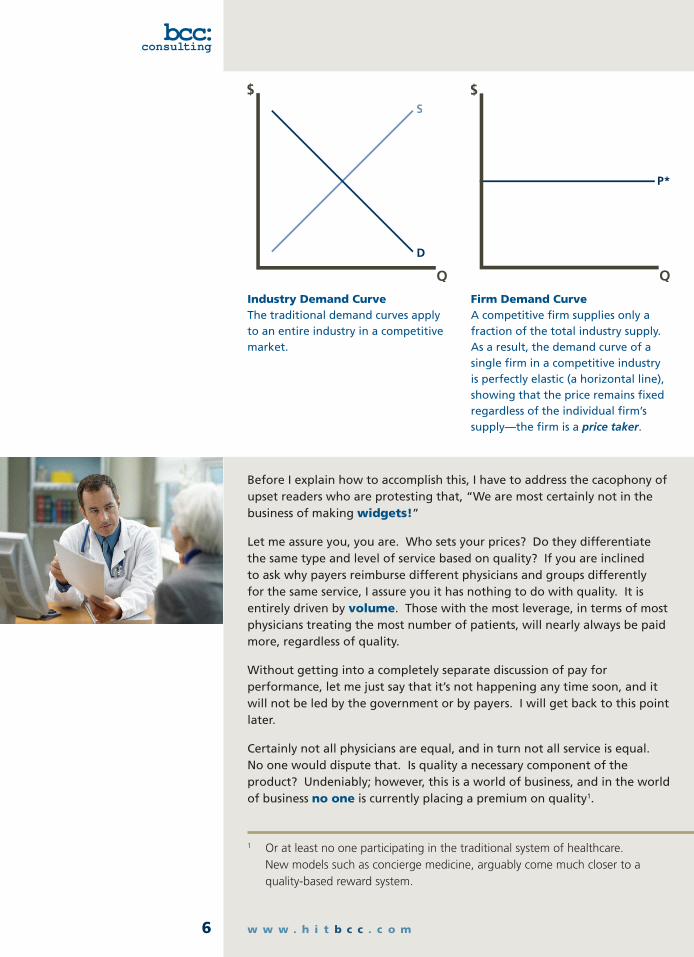
Industry Demand Curve The traditional demand curves apply to an entire industry in a competitive market.
Firm Demand Curve A competitive firm supplies only a fraction of the total industry supply. As a result, the demand curve of a single firm in a competitive industry is perfectly elastic (a horizontal line), showing that the price remains fixed regardless of the individual firm’s supply—the firm is a price taker.

Copyright © 2008 bcc: Consulting. All Rights Reserved. 7
Practicing to Win
In fact, while it may sound cruel and heartless, any physician who offers more than the “standard of care” and spends any extra time evaluating or discussing anything outside of the current billable visit is a bad businessman. By this measure, our physicians, like nearly all others are bad business people. Again and again, physicians – and none more than primary care – are asked to subsidize the larger system by freely making sacrifices. Give us quality while we pay you in bulk.
So, in our widget producing factory, we are left with many, many imperfections – areas that we cannot systematize or automate, chiefly the machine otherwise known as physician. Luckily there are a number of other areas that we can improve to 1: reduce the cost of the widget, and 2: sell more.
Fewer PeopleThe greatest cost component of any practice’s overhead is staff. I have met so many practices that are quick to lament the current state of medicine while trying to run their office as though they were in the 1970’s. Even small offices have staff dedicated to pulling charts. Multiple front-office, back-office, you name it.
I am a huge proponent of technology and electronic medical records (EMRs) in particular. Overall EMR adoption is finally taking off, but just as quickly we are hearing distressing reports of the growing number of failed implementations and practices removing “useless” systems. I would readily argue that any practice who has failed with an EMR has failed with their deployment execution.
Any of the top 20 systems on the market are very good, and all have been implemented in at least several hundred medical practices (the larger vendors, in several thousand). Despite that every physician and every office thinks they are singly unique, they are not. A deployment failure is a commitment failure. And most frequently, the commitment failing is a practice or a physician’s decision not to pay for good help.
A good integrated EMR and practice management system (PMS) exists in the small office for one reason – to reduce office overhead. It is a tool that helps you accomplish more with less.
I would readily argue
that any practice who
has failed with an EMR
has failed with their
deployment execution.
w w w . h i t b c c . c o m8
Offices that have been in practice for a number of years will spend the money on an EMR, and because of loyalty to their staff, will not eliminate positions. Again, I understand the loyalty, but please do not turn around and complain that you are not getting the return on your investment.
Almost as annoying is to hear physicians talking about how electronic medical records should improve patient care, or the patient experience – with complete obliviousness to the business implications. Do not buy an EMR to yet further improve the quality of the widgets you are selling—this makes no sense, economically. Worse, it leads to the idiotic conclusion that payers or hospitals or employers should pay for your EMR. Good luck with that.
The fact is that EMRs do much to improve healthcare quality, but that is an added benefit, and in today’s environment, not a reason to buy one. First and foremost, they allow you to do more with less…Less people, which is the best thing you can do to decrease the cost of a widget.
To give you an example, I submit most claims on the same day patients are seen, though from time to time, I have to ask the providers to finish an outstanding note. As part of the note, each physician is responsible for their own coding. Again, no extra personnel dedicated to roles handled by our system. In addition to the administrative edits, eClinicalWorks now offers access to CodeCorrect’s knowledge base (a company focused on automating the overwhelming ICD-9, CPT, and HCPCS changes along with government and private payer rules related to them). I had petitioned eClinicalWorks for 2
years to incorporate CodeCorrect’s edits and am glad they finally did as I find it invaluable.
It takes me about 15 minutes a day to submit all of our charges (approximately 40-60 claims). Each claim goes through the following process before it reaches the payer: coded by physician, checked for administrative errors by eCW, checked for potential coding violations by CodeCorrect, reviewed and edited by me if necessary and sent to our clearinghouse, Emdeon (formerly WebMD Envoy); the clearinghouse performs an additional edit before submitting to the payer. If the clearinghouse detects any errors, it will send a message to the office within a few hours so the claim can be corrected and resubmitted before it is sent to the payer, thus reducing a lengthy denial cycle.
Do not buy an EMR
to yet further improve
the quality of the
widgets you are selling
— this makes no sense,
economically.
Copyright © 2008 bcc: Consulting. All Rights Reserved. 9
Practicing to Win
The amazing efficiency of this process ensures claims are submitted promptly and accurately, minimizing later follow up. It’s a great concept: if you do it correctly the first time, you don’t have to have a dedicated staff to follow up on denials.
The corollary to this is that when we do have denials, I can make the decision to follow up or not. It’s a crazy notion, but not all denials are worth following up on. I have no doubt that many other practices are better chasing down every cent, but our goal is to optimize our resources and return on investment.
Less SpaceRent or mortgage payments are likely any given practice’s second largest regularly recurring cost item. In theory, as is true with leasing vs. buying cars, there really shouldn’t be a financial difference between renting vs. owning. Of course, as with all things, short-term inefficiencies abound. Additionally, there are subtle trade-offs between owning and renting that generally come with implicit price tags. For instance, renting offers the added flexibility of moving later if you need additional space to grow into. Therefore, you may be willing to pay more for the “option” that renting offers.
For simplicity’s sake, let’s just assume that it’s a zero sum gain, monthly rent vs. monthly mortgage. Let’s assume that you have a fixed amount of space for which you pay a fixed monthly amount. Are you fully utilizing that space? Are you maximizing your office’s ability to generate revenue?
I was recently informed that the average physician should have about 1,500 sq. ft. So, in other words, a 3 physician practice should be about 4,500 sq. ft. Don’t get me wrong, I love data, lots of it. I love doing analysis on data. But this underscores a problem that is so typical of practice management.
It reminds me of the story I once heard from a McKinsey or BCG consultant who, in complete admiration of his boss, told the story of how she informed a client that “on average, every person has one testicle and one breast,” clearly admonishing the use of meaningless statistics.
Our office that originally supported a solo physician can now support 3 FTE physicians. We occupy a whopping 2,000 sq. ft. – that’s less than 700 sq. ft. per provider. Furthermore, we have ample space. I give my wife full credit for the office design. She is inherently a utilitarian and designed 6 exam rooms around a central work area. The back office that used to belong to just me, is now shared by the 3 physicians and me.
The truth is that the physicians do not need an office, or at least an office in the traditional sense. If anything, an office gives one an opportunity to accumulate junk and personal odds and ends that are not even good enough to be kept at home. If the providers are seeing patients – in the exam rooms – they really do not need an office to hang out in. A chair, a
It’s a crazy notion,
but not all denials are
worth following up on.

w w w . h i t b c c . c o m10
desk, a computer to document ongoing encounters… not much else.
In fact, while the 4 of us share a single office, you will rarely find more than 2 people in the office at any given time. I suspect the average occupancy is about 1.3.
Of course, we do not have hundreds of square feet dedicated to paper charts. We also do not transcribe notes. I know that most EMRs support transcription – no doubt an early concession to those physicians who refused to change their ways – but it flies in the face of EMRs and adds a completely unnecessary cost.
Perhaps one of the reasons that the office accommodates the four of us so easily is that I actually spend very little time in the office at all. I perform most of my management responsibilities from home or on the road via VPN (virtual private network) access. Additionally, each of our physicians has remote access to the server from home. If anyone is at the office after 5:15pm, it is because they choose to finish their notes in the quiet of the office.
Greater ProductivityThus far, we have reduced the cost of our widget by minimizing support staff and maximizing the production capacity of our factory. There are a number of other things that we can do to minimize additional cost elements, but rather than address them individually, I would prefer to address them as one group under the heading — When to Spend vs. When to Skimp.
In general, both my wife and I are big believers in sweat equity – a roll-up the sleeves, can-do attitude that can save money at just about every turn. For example, we purchased the majority of our office equipment, including exam tables, exam lights, a baby scale, and an autoclave, among other items, from a defunct medical practice in town. We bought most of our office furniture from an unfinished wood furniture store, that we subsequently finished ourselves. Trust me, there was real sweat involved in this.
But knowing when to roll up the sleeves, and when to take out the check book is imperative. In fact, I lump so many different cost items into this header because it is probably the one area where most practices make their biggest mistake.
When we built-out our office, I paid the builders to pull Cat 5 cable through our space, but I did all the technical work to punch down the cable and ultimately build out our entire network – the heart and soul of our operation. As soon as I was finished putting the whole thing together, I immediately contracted with an excellent network support group, UnlimitedPlus, to manage my network, specifically to provide continuous monitoring and disaster recovery services. Why? Because I am not an
Knowing when
to roll up the sleeves,
and when to take
out the check book is
imperative.
Copyright © 2008 bcc: Consulting. All Rights Reserved. 11
Practicing to Win
expert network administrator. Furthermore, it took me 2 weeks, with help, to get the network up and running. If it fails, I want it up and running within 6 hours. This means having contingency servers, client PCs, network switches, and routers on hand, and the ability to recreate my network environment. I am proud of myself for putting the network together in the first place. I am much smarter and more effective in troubleshooting and solving problems on my own as a result; however, I recognize when to call in the experts.
For not a whole lot more than we spend on our cleaning service, we have remote data back-up and a solid contingency plan in place. What’s more, I sleep comfortably each night knowing that if anything goes wrong with either our system or our network, we will have it all up and running within a day. Many practices are reluctant to pay for this type or level of service.
Another common problem I’ve already alluded to, and one that I speak about often, is EMR/PMS vendor selection. When it comes to selecting an EMR and practice management system (PMS), offices seem to think that as long as they choose “the right” vendor, all of their problems will be solved. In truth, any of the top vendors’ systems are adequate, some better than others, and some much more expensive. The success or failure of an EMR/PMS implementation has much more to do with the office’s network (IT infrastructure) and its staff’s willingness and ability to adapt to change (change management). Do not expect that simply choosing a vendor will ensure success. It won’t.
Every decision involving resource utilization – chiefly physician and staff time – must be weighed against its opportunity cost. In other words, how else might that resource be deployed, or what else might that person be doing?
Physicians are often referred to as bad business people. While somewhat deserved, the reputation really comes from the fact that very few physicians are formally schooled in business, and many physicians have type-A personalities. They are generally intelligent, self-reliant, and confident. These are great characteristics, but do not lend well to taking advice. Even worse, they seem to imbue many physicians with the intellectual curiosity and problem-solving to want to personally undertake unnecessary challenges. Interestingly enough, this self-sufficiency does not generally spill over into menial tasks like cleaning the office, or trade-specific specialties like accounting or law.
Business acumen, strategic planning, management and to a large extent computers and computer networking, on the other hand, are all egalitarian undertakings that require no formal license or degree to practice. As a result, those with proven academic success and intelligence are wont to engage in them with surety and confidence. The cost of such erroneous misjudgment is twofold: first, subpar business performance, and second, either lost or interrupted time with patients, which hampers revenue-generation.
Every decision involving
resource utilization —
chiefly physician and
staff time — must be
weighed against its
opportunity cost.
w w w . h i t b c c . c o m12
Know when to roll-up the sleeves and when to pay for good help, and apply frequently in all business undertakings.
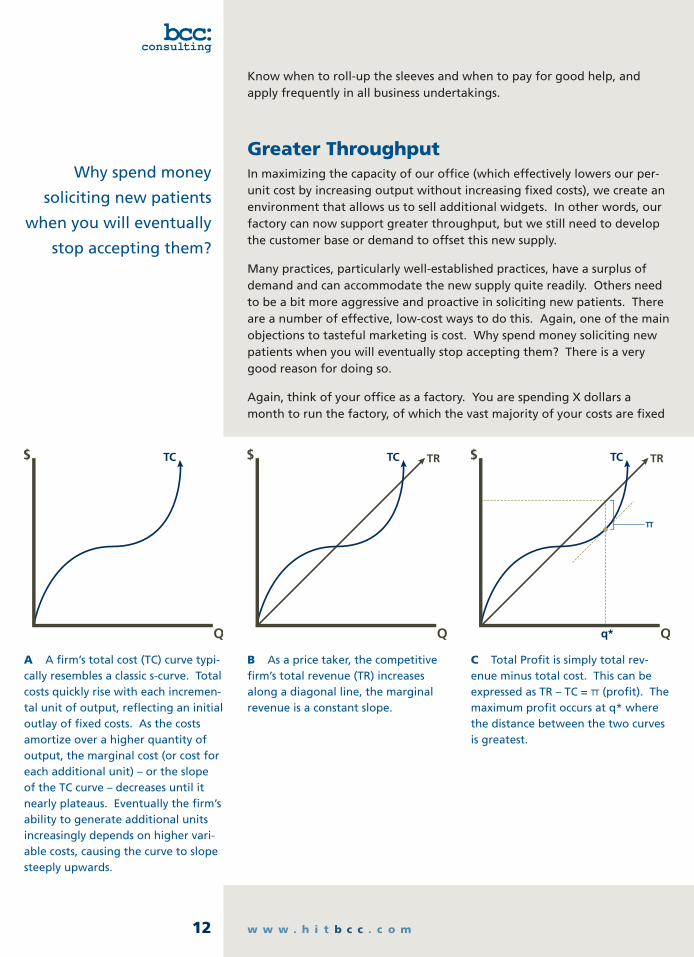
Greater ThroughputIn maximizing the capacity of our office (which effectively lowers our per-unit cost by increasing output without increasing fixed costs), we create an environment that allows us to sell additional widgets. In other words, our factory can now support greater throughput, but we still need to develop the customer base or demand to offset this new supply.
Many practices, particularly well-established practices, have a surplus of demand and can accommodate the new supply quite readily. Others need to be a bit more aggressive and proactive in soliciting new patients. There are a number of effective, low-cost ways to do this. Again, one of the main objections to tasteful marketing is cost. Why spend money soliciting new patients when you will eventually stop accepting them? There is a very good reason for doing so.
Again, think of your office as a factory. You are spending X dollars a month to run the factory, of which the vast majority of your costs are fixed
Why spend money
soliciting new patients
when you will eventually
stop accepting them?
TC TRTC TRTC
TT
A A firm’s total cost (TC) curve typi-cally resembles a classic s-curve. Total costs quickly rise with each incremen-tal unit of output, reflecting an initial outlay of fixed costs. As the costs amortize over a higher quantity of output, the marginal cost (or cost for each additional unit) – or the slope of the TC curve – decreases until it nearly plateaus. Eventually the firm’s ability to generate additional units increasingly depends on higher vari-able costs, causing the curve to slope steeply upwards.
B As a price taker, the competitive firm’s total revenue (TR) increases along a diagonal line, the marginal revenue is a constant slope.
C Total Profit is simply total rev-enue minus total cost. This can be expressed as TR – TC = TT (profit). The maximum profit occurs at q* where the distance between the two curves is greatest.

Copyright © 2008 bcc: Consulting. All Rights Reserved. 13
Practicing to Win
and not variable. This creates what is known as “stickiness.” In other words, you may be able to scale back blocks of cost to cut back the output capacity of your factory. But you probably can do this at only certain points along your supply curve. For instance, you may only be able to spend .8X to run the factory at 80%, or .5X to run it at 50%. However, your overhead is not perfectly variable like the fine tuning volume knob on your stereo. This means that you are most likely paying X dollars to support 100% capacity, even if your throughput is only 85%. Analysis of the situation might reveal that you should actually lower your capacity to 80% so that you can align your cost structure with your utilization – it may be better to spend .8X for 80% than X for 85%.
The opposite is also true. If you are spending X, but running at 85%, you should work to increase your capacity to 100%; but how hard? It depends. How much are you losing by not running at 100%? You may currently be profitable, but the inefficiency is undoubtedly costing you. The value of the ongoing loss will give you a much better understanding of the need to accelerate supply optimization. For example, how much should you be willing to spend on a 6 month marketing campaign that will reduce your under utilization from 12 months to 6?
A By comparison, if we assume that all of our costs are fixed, we can clearly see that our total cost (TC) curve looks like a staircase – a fixed level of cost supports a specific level of output, beyond which point, the marginal cost is the entire cost of the next level of fixed costs.
B Again, as a price-taker, our total revenue (TR) curve resembles the typical competitive firm.
C Unlike the typical competitive firm, which has a single point of maximum profitability, we have multiple points. This clearly shows the importance of “right-sizing” your clinical operation to match patient load.
TC TRTC TRTC
TT1
TT2
TT3
q1 q2 q3
w w w . h i t b c c . c o m14
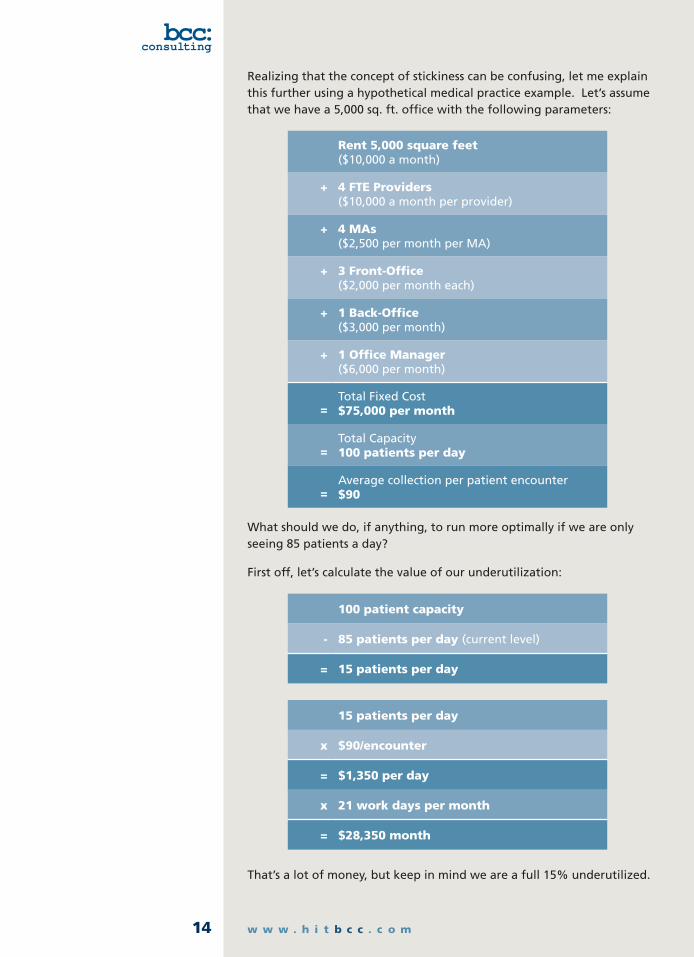
Realizing that the concept of stickiness can be confusing, let me explain this further using a hypothetical medical practice example. Let’s assume that we have a 5,000 sq. ft. office with the following parameters:
Rent 5,000 square feet ($10,000 a month)
+ 4 FTE Providers ($10,000 a month per provider)
+ 4 MAs ($2,500 per month per MA)
+ 3 Front-Office ($2,000 per month each)
+ 1 Back-Office ($3,000 per month)
+ 1 Office Manager ($6,000 per month)
=
Total Fixed Cost $75,000 per month
=
Total Capacity 100 patients per day
=
Average collection per patient encounter $90
What should we do, if anything, to run more optimally if we are only seeing 85 patients a day?
First off, let’s calculate the value of our underutilization:
100 patient capacity
- 85 patients per day (current level)
= 15 patients per day
15 patients per day
x $90/encounter
= $1,350 per day
x 21 work days per month
= $28,350 month
That’s a lot of money, but keep in mind we are a full 15% underutilized.

Copyright © 2008 bcc: Consulting. All Rights Reserved. 15
Practicing to Win
People, as with most fixed costs, are fixed in the short-term but variable in the long. In other words, if we know that we are going to be running at 85% of capacity for the foreseeable future, we can restructure our staffing to reduce costs and capacity. However, if the shortfall is only temporary, it is much more difficult to lay people off and rehire them only when they are needed (also called furloughing). Factoring in the costs of finding, hiring and training personnel, you can see why they are regarded as a fixed cost in the short-term.
In our example, if we assume each physician has the exact same level of productivity, reducing our provider staff from 4 to 3 would immediately reduce our capacity by 25%. We would then be able to reduce some of the support staff and our overall fixed monthly costs. The net effect may actually be better than our starting point, but let’s assume we are growing, and our goal is not to downsize.
A better alternative is to build-in some variability within our staffing. So, rather than having 4 providers who must maintain full-time positions, it is preferable to have at least one or two providers who have the flexibility to work a part-to-full time schedule. This gives us the ability to ratchet down our supply to better reflect demand.
The same is true of our medical assistants (MAs). So, instead of having 4 full-time MAs, we may prefer to have 3 full time and 2 part-time. The part-time employees, in addition to giving us greater work-hour flexibility, simultaneously reduce our overall benefits burden.
Basic Economic TheoryAccording to Wikipedia, “microeconomics is a branch of economics that studies how individuals, households, and firms make decisions to allocate limited resources, typically in markets where goods or services are being bought and sold. Microeconomics examines how these decisions and behaviors affect the supply and demand for goods and services, which determines prices; and how prices, in turn, determine the supply and demand of goods and services.”
In general “micro,” is extremely intuitive and explains so much about how and why people do what they do. I believe that if every physician were trained on just two simple microeconomic concepts they would be much
better business people –the first, which I have already touched upon, is opportunity cost and the second is sunk cost.
Opportunity cost is simply the cost or value that would be realized if the resources required for the contemplated undertaking were otherwise deployed. In other words, say a physician spends 30 minutes trying to configure a network printer. Had he opted instead to see 2 patients, he could have potentially billed $500 in charges, and collected $300. His opportunity cost is $300. Rather than trying to fix the printer himself, he could have hired a professional to fix the printer for $50. So, while the physician probably felt he was saving $50, he really lost $250.
As its name suggests, opportunity cost assumes an “opportunity.” The physician’s time cannot generically be expressed as $300 per 30 minutes or $600 an hour. Such reasoning would prevent our physician from doing anything but seeing patients. Just because the physician has 30 minute periods where he can earn $300, does not mean that every 30 minutes of his time is worth $300. If, for instance, he had no other patients to see at 5:30pm, it may be more advantageous to take out the garbage and sweep and mop the office floors if the only other alternative were to sit and do nothing. (Though, sitting and doing nothing, in turn, has its own value that is harder to compute and may ultimately be more valuable than the $20 of cleaning services saved.)
continued on page 16
w w w . h i t b c c . c o m16
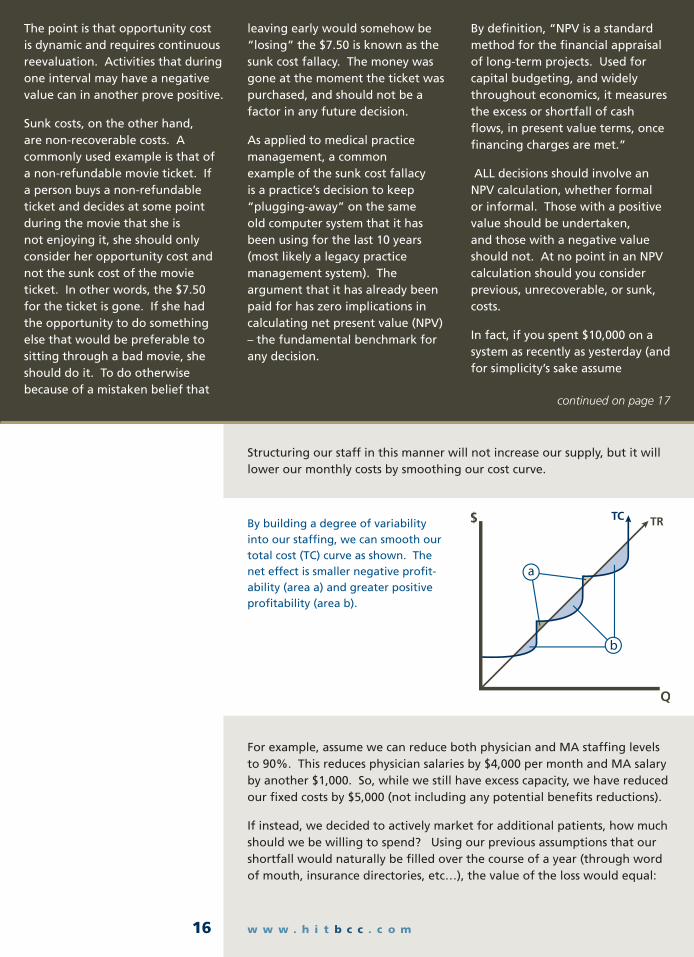
Structuring our staff in this manner will not increase our supply, but it will lower our monthly costs by smoothing our cost curve.
For example, assume we can reduce both physician and MA staffing levels to 90%. This reduces physician salaries by $4,000 per month and MA salary by another $1,000. So, while we still have excess capacity, we have reduced our fixed costs by $5,000 (not including any potential benefits reductions).
If instead, we decided to actively market for additional patients, how much should we be willing to spend? Using our previous assumptions that our shortfall would naturally be filled over the course of a year (through word of mouth, insurance directories, etc…), the value of the loss would equal:
The point is that opportunity cost is dynamic and requires continuous reevaluation. Activities that during one interval may have a negative value can in another prove positive.
Sunk costs, on the other hand, are non-recoverable costs. A commonly used example is that of a non-refundable movie ticket. If a person buys a non-refundable ticket and decides at some point during the movie that she is not enjoying it, she should only consider her opportunity cost and not the sunk cost of the movie ticket. In other words, the $7.50 for the ticket is gone. If she had the opportunity to do something else that would be preferable to sitting through a bad movie, she should do it. To do otherwise because of a mistaken belief that
leaving early would somehow be “losing” the $7.50 is known as the sunk cost fallacy. The money was gone at the moment the ticket was purchased, and should not be a factor in any future decision.
As applied to medical practice management, a common example of the sunk cost fallacy is a practice’s decision to keep “plugging-away” on the same old computer system that it has been using for the last 10 years (most likely a legacy practice management system). The argument that it has already been paid for has zero implications in calculating net present value (NPV) – the fundamental benchmark for any decision.
By definition, “NPV is a standard method for the financial appraisal of long-term projects. Used for capital budgeting, and widely throughout economics, it measures the excess or shortfall of cash flows, in present value terms, once financing charges are met.”
ALL decisions should involve an NPV calculation, whether formal or informal. Those with a positive value should be undertaken, and those with a negative value should not. At no point in an NPV calculation should you consider previous, unrecoverable, or sunk, costs.
In fact, if you spent $10,000 on a system as recently as yesterday (and for simplicity’s sake assume
TRTC
a
By building a degree of variability into our staffing, we can smooth our total cost (TC) curve as shown. The net effect is smaller negative profit-ability (area a) and greater positive profitability (area b).
continued on page 17

Copyright © 2008 bcc: Consulting. All Rights Reserved. 17
Practicing to Win
$28,350 per month
x 12 months
= $340,200
÷ 2 (assuming patient growth is equally distributed over 12 months)
= $170,100
By comparison, if we were able to reduce the shortfall from 12 to 6 months, our loss would equal only:
$28,350 per month
x 6 months
= $170,100
÷ 2 (assuming patient growth is equally distributed over 6 months)
= $85,050
This suggests that if we are able to run a marketing campaign that would reduce the period of our patient shortfall from 12 to 6 months, we would earn an additional $85,050. To put this
there are no recurring costs associated with supporting the system), and find a different system today that costs say, $50,000, but offers a positive NPV, then you should purchase it. The system you purchased yesterday has no bearing on today’s decision. In other words, you cannot make-up for a previous poor decision by “sticking it out.” The result of such thinking is a multiplication of the number and effect of your poor decisions.
These economic concepts extend well beyond easily calculable monetary decisions. For example, I would argue that the primary reason there is so much resistance to change is the sunk cost fallacy. When presented with a new system, policy, or procedure, people resist change. While people
can be pig-headed, or “irrational” as an economist would say, they generally are not. The rash of failures and challenges associated with system change is not caused by rampant irrationality, or incompetence. Something else is at play.
Whether the front-office receptionist, the office manager, or even the physician, each person learned to do their job a certain way. They invested time and energy, and likely feel they are proficient at accomplishing their responsibilities, regardless of whether true or not. The point is that they believe they are good at what they do. (Consider, for example, that research has consistently found that 9 out of 10 people believe they are smarter than the average person.)
When confronted with change, the near-universal reaction is that the effort of learning something new does not justify the cost. The problem is that the person making the decision typically overvalues their current efficiency, undervalues the potential gains to be realized by changing (thus, resulting in an understated NPV), and finally cannot let go of the original effort required to learn their job in the first place (sunk cost fallacy).
Nearly every decision in medical practice management involves these concepts and having a better understanding of their implications can greatly simplify and improve decision-making.
continued on page 18
w w w . h i t b c c . c o m18
into perspective, an aggressive marketing campaign might cost $5,000 to $10,000. So, to earn $85,000 at a cost of even $10,000 nets an additional $75,000 of income.
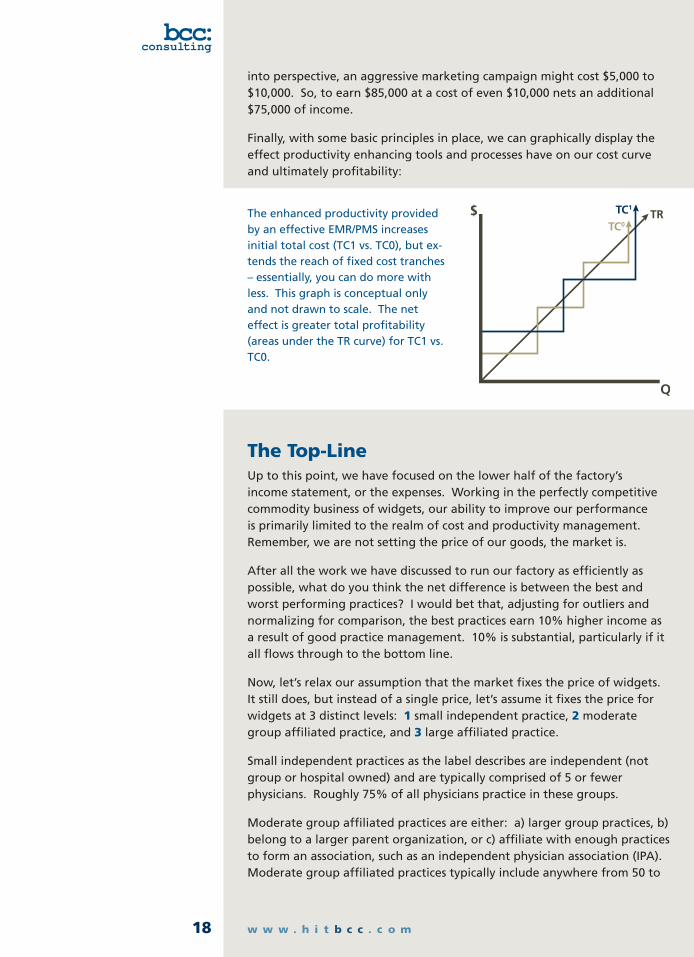
Finally, with some basic principles in place, we can graphically display the effect productivity enhancing tools and processes have on our cost curve and ultimately profitability:
The Top-LineUp to this point, we have focused on the lower half of the factory’s income statement, or the expenses. Working in the perfectly competitive commodity business of widgets, our ability to improve our performance is primarily limited to the realm of cost and productivity management. Remember, we are not setting the price of our goods, the market is.
After all the work we have discussed to run our factory as efficiently as possible, what do you think the net difference is between the best and worst performing practices? I would bet that, adjusting for outliers and normalizing for comparison, the best practices earn 10% higher income as a result of good practice management. 10% is substantial, particularly if it all flows through to the bottom line.
Now, let’s relax our assumption that the market fixes the price of widgets. It still does, but instead of a single price, let’s assume it fixes the price for widgets at 3 distinct levels: 1 small independent practice, 2 moderate group affiliated practice, and 3 large affiliated practice.
Small independent practices as the label describes are independent (not group or hospital owned) and are typically comprised of 5 or fewer physicians. Roughly 75% of all physicians practice in these groups.
Moderate group affiliated practices are either: a) larger group practices, b) belong to a larger parent organization, or c) affiliate with enough practices to form an association, such as an independent physician association (IPA). Moderate group affiliated practices typically include anywhere from 50 to
The enhanced productivity provided by an effective EMR/PMS increases initial total cost (TC1 vs. TC0), but ex-tends the reach of fixed cost tranches – essentially, you can do more with less. This graph is conceptual only and not drawn to scale. The net effect is greater total profitability (areas under the TR curve) for TC1 vs. TC0.
TC0
TC1TR

Copyright © 2008 bcc: Consulting. All Rights Reserved. 19
Practicing to Win
several -hundred physicians, or more. A small independent practice can gain leverage by joining such an association, as my wife’s practice has done.
Finally, the large affiliated practice is either part of a large hospital or group affiliation that may have many thousands of physicians.
What do you think the market pays for widgets across these 3 groups? Keep in mind that fee schedules are confidential, so not readily comparable.
When the small independent practice “opts-in” to a payer’s contract, they are given the most basic and lopsided fee schedule possible. Let’s just call this Y per widget (our baseline).
With the added leverage of a moderate group affiliation the exact same practice would likely see their fee schedule jump to somewhere between 1.15Y to 1.20Y – a 15%-20% increase.
The large affiliated practice, in turn, would likely see fee schedules in the neighborhood of 1.2Y to 1.4Y – a 20% to 40% increase over the baseline!
Again, these different fee schedules have zero correlation to quality.
It should be very clear that while it is important to run a good practice – a 10% differential is enormous ($100,000 to the bottom line for every $1,000,000 of gross revenue) – it is more critical to get on the right contracts. This should help explain to the casual observer how some apparently well run practices have difficulty staying afloat, while other clearly inefficient operations seem to thrive.
Keep in mind that this situation is not sustainable. Eventually, the market will correct itself and those providing good, quality care will be justly rewarded, and better so if they can also run a good business operation. In the interim, practices must understand the dynamics of the current environment if they are to succeed.
If the same firm, with the same cost curve, were offered three different fee schedules (total revenue curves), the impact to total profitability is represented by TT0, TT1, and TT2.
TR0TR1TR2
TC
TT0
TT1
TT2
w w w . h i t b c c . c o m20
Future ChallengesRegardless of the appropriateness of the moniker “Consumer-Driven Healthcare,” the shift of ultimate financial responsibility from employers to employees, or healthcare consumers, brings with it both good and bad. For one, quality cannot be driven by payers. There are far too many variables and unknowns to effectively benchmark clinical outcomes. Worse yet, allowing the payers to define the quality criteria and metrics is a bit like having the foxes establish security protocols at the hen houses. Payers are far more interested in and incentivized to maximize profitability than improve clinical outcomes. Don’t let the fact that the two occasionally intersect lead you to conclude otherwise.
As in all industries, the consumers of goods or services should be the ones to determine the value of that which they seek. To assume that a third party is better equipped to measure the quality of care provided than the patient receiving the care is beyond paternalistic, and has consistently proven inaccurate. I am much better equipped, for instance, to determine the quality provided by my physician than my auto mechanic. But other than industry self-regulation, which healthcare does as well, no outside organization intervenes directly on my behalf to protect me from making a bad auto repair decision or from being taken advantage of.
Ultimately, as patients become more empowered to spend their own dollars on healthcare, the tried and true laws of supply and demand will kick in. Good physicians will be highly sought after. Lesser physicians will be in less demand, and the market will adjust prices accordingly. The platforms for consumers sharing their experiences and feedback have grown exponentially over the last few years and will likely continue as patients assume more of their responsibilities as consumers.
A short-term problem with the newer healthcare financing model
is that more reimbursement is coming directly from the patient. When you consider that your worst payer is almost certainly your patients themselves (consumer spending reports generally show that consumers place medical bills somewhere between Ho-Hos and Ding-Dongs on their priority list of debt repayment), practices must become more aggressive in verifying benefit eligibility and collecting payment in advance of service.
As in all industries,
the consumers of goods
or services should be
the ones to determine
the value of that which
they seek.

Copyright © 2008 bcc: Consulting. All Rights Reserved. 21
Practicing to Win
Final ThoughtsAgain, my rationale for comparing the physician office to a factory is in no way intended to detract from the great care and sacrifice so many countless physicians make day in and day out. To the contrary, I feel that our healthcare system should reward those commensurate to the service they provide, rather than arbitrarily, or even worse, politically.
Healthcare has historically fallen into a special class of industry and business that even in the eyes of the staunchest laissez-faire economists has deservedly required government intervention and oversight. The argument has long been based on the notion of information asymmetry – the physician or provider has a disproportionate knowledge or access to information than the consumer. Thus, in protecting the rights of the consumer, the government is justified in intervening to ensure a level playing field.
It’s a reasonable concept, but in practice, does not work. The government is largely responsible for the dysfunctional system that we have today. Rather than embarking on a tirade of Medicare and Medicaid, I prefer to focus on those things that physicians and practices can do to not only survive, but thrive.
Sound economic and financial practices can greatly improve any medical practice, even in today’s managed care environment. As healthcare shifts to a more traditional free-market system, understanding of economic theory and principles will become even more pertinent and crucial.
The continued transformation of healthcare over the next decade promises yet more chaos; but rather than throwing your hands up in resignation, ponder Albert Einstein’s wisdom and appreciate the boundless opportunity before us.

Unlimited Plus is North Carolina’s premier Healthcare IT Services Provider, specializing in network management, EMR/PMS implementation and infor-mation technology consulting services. With hundreds of machines under management across healthcare organizations large and small, Unlimited Plus consistently delivers high-quality and responsive technical support.
To learn more, visit us at http://www.unlimitedplus.com/Healthcare, or call (888) 865-7587.