practical ophthalmology rough draftstorage.googleapis.com/wzukusers/user-17688629/documents... ·...
TRANSCRIPT

PRACTICAL OPHTHALMOLOGY

Also by James Y. Hung: Finding Fat Lady’s Shoe: A Memoir of Growing up in Hong Kong and Malaysia. (2013) FOB in Paradise: A Memoir. (2014) Silk Road on My Mind (2015) Available through Amazon in paperback and Kindle e-book. E-book also available through Barnes & Noble. Finding Fat Lady’s Shoe An intensely reflective tale of a family uprooted by war, cast adrift onto a sea of uncertainty.—Kirkus Review Dr. James Hung's life story echoes others that will probably never be written, and offers a fascinating perspective on Hong Kong's recent past that deserves to be widely read. [4 stars out of 5]—South China Morning Post FOB in Paradise Hung has written an absorbing and witty book. Dramatic, nuanced vignettes and vivid descriptions of people and places create a rich tapestry that shows the medical profession at its best and worst. —Kirkus Review Silk Road on My Mind Hung is an endearing mix of benevolence, wryness, and curiosity…. there is an appealing Marco Polo–ishness to his project: a boundless wonder for a society unlike his own, not for its differences but for the infinitely recognizable humanity at its center.—Kirkus Review

PRACTICAL OPHTHALMOLOGY A CONCISE MANUAL FOR THE NON-OPHTHALMOLOGIST
James Y. Hung, MD

Practical Ophthalmology: A Concise Manual for the Non-ophthalmologist Copyright © 2016 by James Y. Hung. All rights reserved. With the exception of brief quotations embodied in reviews, no part of this book may be reproduced in any form without written permission from the author. ISBN: 0692748601 EAN: 978-0692748602 (James Y Hung) Cover by Tony Ton Editing and text design by Anne Correia

CONTENTS Preface......................................................................................................vii
Author’sNote………………………….………………………………………….....ix
Chapter1:EquipmentandSupplies..............................................1
Chapter2:HistoryandExamination..........................................15
Chapter3:Anatomy...........................................................................27
Chapter4:BasicOptics....................................................................31
Chapter5:Eyelids,Conjunctiva,CorneaandSclera............39
Chapter6:Cataract.............................................................................49
Chapter7:RetinaandVitreous.....................................................55
Chapter8:Uveitis................................................................................73
Chapter9:Glaucoma..........................................................................77
Chapter10:Neuro‐ophthalmology..............................................91
Chapter11:PediatricOphthalmologyandStrabismus....111
Chapter12:OcularManifestationsofSystemicDiseases121
Chapter13:EyeDiseasesinDevelopingCountries...........129
Glossary................................................................................................141


PREFACE Ophthalmology is so specialized that it essentially has its ownlanguage,which is not easy for health careworkers outside ofthe specialty tounderstand.When I consideredwritingabookaboutophthalmology,Ifirstdebatedwhetherornottherewasaneed for anotherophthalmologybook, and concluded that oneshouldbewrittensolelywiththenon‐ophthalmologistsinmind.The population is growing older in many countries and eyeproblemsaremoreprevalentasweage;primarycareprovidersmust have a solid understanding of the more common eyedisordersinordertoservethesepatientsadequately.During the past two decades, ophthalmology has undergone agreat deal of change. Many eye surgeries are now done inoutpatient centers, away from the hospital. Some eyedepartments have their own buildings, segregating theophthalmologists from the rest of the medical community,widening the gap of communication. Many medical studentsgraduate never havinghad a rotation in ophthalmology (Iwasone), as it is only an elective inmostmedical schools and notrequired.Thisconcisebookcanbereadinadayortwo.Itwillprovidethereaderwith core knowledge on how to provide basic eye careandwhentoreferapatientelsewhere.Onlyconditionsthatarelikelytobeseenintheprimarycaresettingarediscussed.

viii
In many developing countries, only a handful ofophthalmologists serve the entire population, which cannumber in the millions. It is hoped that this book wouldencourage primary care providers to offer basic eye care andhelpthemworkbetterwithophthalmologistsandnon‐physicianeye careproviders (who, in somecountries,havebeen trainedtodoeyesurgeries).Thesubjectmatter inthebookvarieswidelyfromthesuppliesandequipmentneeded toprovidebasiceyecare, tohowtodoaneyeexamination,basicoptics,treatmentofcornealproblems,infections, glaucoma, and neurological and vascular diseasesconcerningtheeye.Myfoundationplanstodistributethisbookfreeofchargetoasmanyhealthcareprovidersindevelopingcountriesaspossible.The book, as well as photos of clinical conditions, can bedownloadedfreeofchargefrommywebsite:www.jamesyhungbooks.com.I want to thank the American Academy of Ophthalmology forgrantingmepermissiontouseafewofitsdrawingsinthebook.JamesY.Hung,MD,FACSHonolulu,Hawaii2016

AUTHOR’S NOTE WhenIspenttwoweeksinApia,WesternSamoaattheGeneralHospitalin2014,workingintheeyedepartment,ayounghouseofficer was shadowing me. We saw a patient with a strangelookingcystinhisretina,andthefirstthoughtthatcametomymindwas Toxocara canis—a parasitic infection spread by dogfeces—asthereweremanyferaldogsaroundthecity.Withboththumbsworking away on his iPhone, Salawas able to get theinformationonToxocaracaniswithintwominutes,includinganimagealmostidenticaltotheretinafindinginourpatient.Iwasimpressed.Mostyoungdoctors todayareprobably justas techsavvyasSala.My point is that ophthalmology is a visual specialty.We oftenmakeadiagnosisbyhavingseenat leastonesuchcasebefore.Ideally, this book should have been printed in color, full ofpicturesofclinicalconditions.Unfortunately,printingincolorisfivetimesasexpensiveasblackandwhite,andconcernsaboutaccessibilityandaffordabilitytookprecedence.I suggest thebestway touse this book is todownloadphotosfromtheInternetofthediseasesandconditionsdescribed.Thephotos will likely be clearer—and more abundant, providingimagesofdifferentstagesandfromvariousangles—thanthoseprinted on paper. Practically any clinical conditions can befound online; and YouTube also has videos of different eyesurgeries, demonstrations of performing tests, andmethods ofexaminingtheeye.Thisbookshouldbeusedasastartingpoint

x
tobuildingtheophthalmologyknowledgethatareaderdesirestoacquire.Thesmartphonenowhasseveraladaptersfortakingphotosofthefundus.Ifyouareuncertainofadiagnosis,suchaswhetheror not a diabetic patient’s retinopathy needs laser treatment,you can send the photos for consultation. Telemedicine hasimprovedeyecaretremendously,oftensavingpatientsandtheirfamilies the time and money required for an in‐personconsultation.Ihopeyoufindthisbookhelpfulinyourpractice.Thankyou.JamesY.Hung,MD,FACS

CHAPTER 1: EQUIPMENT & SUPPLIES THE LEVEL OF EYE CARE YOU WISH TO PROVIDE TO YOURPATIENTSDEPENDSONYOURCOMFORTLEVELANDTRAINING.If you are unsure of a diagnosis or course of treatment, neverhesitatetoreferyourpatienttoanophthalmologist.
BASICEQUIPMENT
1. Ophthalmoscope2. Handflashlight3. Binocularmagnifyingloupe4. Visualacuitychart(Snellen)5. TheRosenbaumpocketvisionscreener6. Amslergrid7. Schiotztonometer8. Smartphoneasaretinalcamera(optional)
DirectOphthalmoscopeEye examination was one of the more difficult skills I had tolearn inmedicalschool.Wepracticed looking intoeachother’seyes for hours, and still it wasn’t easy. During my internship,family practice residency andERdays, trying look at the opticdiscsofolderpatientswithsmallpupilsandcataractswastrulychallenging.During my ophthalmology residency, I realized thatophthalmologistshaveanadvantageovertheprimarycaredocsbecausetheyalwaysdilatethepupils,andtheyhaveallkindsofequipmenttohelpthemlookintotheirpatients’eyes,including

2
the indirect ophthalmoscope and special contact lenses withmirrors.Now, for those of you who are tech savvy, there are severaladaptersthatyoucangetforyoursmartphonetotakephotosofthe fundus. Your office assistant can also be taught to do this.The photos can be compared to images of similar conditions;and they can also be sent to an ophthalmologist for advice onwhetherlasertreatmentwouldbeindicated.
BinocularLoupeIf you practice in a rural area and the ophthalmologist is faraway,youmayhavetoremoveacornealforeignbody.Youwillappreciate thebinocular loupe,whichprovidesyouwithdepthperception.
VisualAcuityChartIf you do physical examinations for employers, insurance,driver’s licenses, etc., visual acuity isoneof the items that youhavetofillinontheforms.TheSnellenchart(page12)iseasytouseandtheexamcanbedonebyyourassistant.
RosenbaumPocketVisionScreenerIf it is difficult or not possible to check visual acuity with theSnellen chart, such as with a bedridden or uncooperativepatient,aRosenbaumPocketVisionScreenercanbeused.Ifthepatientnormallywearsreadingglasses,thistestshouldbedonewiththemon.Itshouldbereadoneeyeatatimeatadistanceofabout14inchesor35centimeters.
AmslerGridAs the population gets older, the incidence of maculardegenerationincreases.NowwithwonderdrugslikeLucentis,adrugthatwillstopnewvesselsfromdoingmoredamagetothe

3
central vision, early detection is more important than ever.AmslerGridtestingcanhelpwithadiagnosis(pages7‐9).
SchiotzTonometerThis is a mechanical device that you place on the cornea tomeasure the intraocular pressure. It’s unlikely that youwouldbe taking care of glaucoma patients, but if someone comes inwitheyepainandyouseenosignofinfectionandthecorneaisintact—and the ophthalmologist is far away—you can easilycheckthepressuretoruleoutglaucoma,especiallyoftheangleclosurevariety.This tonometer (page 10) lasts forever and is easy to use. Itcostsaround$200intheUS,andmuchlessinsomedevelopingcountries.
BASICMEDICATIONSANDSUPPLIES
1. Topicalanesthetics:proparacaine0.5%ortetracaine0.5%
2. Sterilefluoresceinpaper3. Mydriatics:phenylephrine2.5%and/ortropicamide
(Mydriacyl)1%4. Miotics:pilocarpine1%5. AntibacterialAgents6. Sterilesolutionsforirrigation7. Eyepads8. Eyeshields9. Sterilecotton‐tippedapplicators10. Corticosteroiddropsorointment(or
corticosteroid/antibioticcombination)
TopicalAnestheticsProparacaine and tetracaine are most commonly used fortopical anesthesia. They are said to have equivalent anesthetic

4
potency. Anesthesia beginswithin 1minute of application andlasts for 15 to 20 minutes. It numbs both the cornea andconjunctiva.Thecorneahasextensivenerveendingsandisoneof themostsensitive organs in the body, making it ideal for topicalanesthetics.
FluoresceinPaperThese come as single use sterile paper strips. The dye on thestripswilldetectcornealinjuryaswellaslocateforeignbodies.
MydriaticsDilatingthepupilforfundusexaminationisworrisomeforthosewhohavenevertakenanophthalmologyrotation(likeme).Theprimary concern is causing angle closure glaucoma in thepatient.Of the tens of thousands of eyes dilated inmy clinic, Icannotrecallonepatientwhosufferedthatcomplication.Inonecase,Icarefullywatchedanelderlywomanafterdilationbecause of her narrow angle, and she did have a rise of herintraocular pressure and further narrowing of the angle. Shewasdiagnosedwithnarrowanglewithintermittentclosureandwas treated with one drop of 1% pilocarpine q.h.s. (4%pilocarpinemaycauseheadache.Thetreatmentofangleclosureglaucomaiswithlaseriridotomy—a15‐minuteprocedureintheoffice.)Tropicamide1% (Mydriacyl) is themost commonly useddropfor dilating the pupil. It takes 20 to 25 minutes for maximaldilationandthedurationoftheeffectis4to8hours.Phenylephrine 2.5% can also be used for dilation. The effectbegins within 30 minutes and lasts 2 to 3 hours. Over thedecades,severalcasesofelderlypatientswerereportedtohave

5
sufferedmyocardial infarctionthatmightbe linkedto the10%phenylephrine, so it is now rarely used. Phenylephrine shouldnotbeusedwithknowncardiacpatients.
AntibacterialAgentsThe drug I recommend for the primary care provider issulfacetamide, which comes in 10% and 30% ophthalmicsolutionaswellas10%ophthalmicointment.Sulfonamidesarethe most commonly used drugs for bacterial conjunctivitisbecausetheyareeffectiveagainstbothgram‐positiveandgram‐negative organisms. It is very inexpensive and few people areallergic to it. Its use is not complicated by secondary fungalinfectionascanoccurwithsomeotherantibiotics.A bottle of drops or a tube of ointment of 10% sulfacetamidecosts less than a dollar in many developing countries and isfreelyavailablewithoutprescription.Other antibiotics include tetracycline, erythromycin,aminoglycosides and fluoroquinolones.Ophthalmicointment ismuch easier to use on a child than drops. Topicalchloramphenicolisanextremelyeffectiveantibacterial,whichiscommonlyusedoutsidetheUSandisveryinexpensive.
IrrigationSolutionsAny contact lens solution will do. If a patient has a chemicalburn, the eyewould need to be irrigated copiously. In case ofemergency,anycleanwatercanbeused.
EyePadsIfapatienthasacornealabrasion,afirmeyepadkeepstheeyefrommovingunderthelid.Acornealabrasioncanbeextremelypainful,andbedrestandtheeyepadwillhelpkeepthepatientcomfortableaswellasspeedupthehealingprocess.

6
EyeShieldIfapatienthasbeenhittingmetalagainstmetalandapieceofitissuspectedtohaveenteredtheeye,ashieldshouldbeplacedover the eye to prevent further damage. Immediate referral toanophthalmologistisindicated.
SterileCotton‐tippedApplicatorThis isan itemthateverymedicalofficeshouldhave. It canbeused to remove a corneal foreign body as well as check thecorneafor leaksifaninjuryissuspected.Italsocanbeusedtoexamineandexploretheextentofinjurytotheconjunctivaandlid.
CautionforCorticosteroidandTopicalAnestheticUseTopical corticosteroids are very effective for severe allergicconjunctivitis and ocular inflammation, but they also havesevereadverseeffectsontheeye.Theyshouldneverbeusedtotreat herpes simplex, bacterial or fungal infections. They maylead to fungal keratitis following a corneal foreign body ofvegetable matter, and can also cause posterior subcapsularcataractandsecondaryopen‐angleglaucoma.Usecorticosteroidstotreatallergicconjunctivitisonlywhenyouarecertainthatitisallergicandnotsomethingelse.Useonlyforashortperiod.Neversendapatientwithacornealinjuryhomewithabottleoftopicalanesthetic. Ifused inappropriately, itcan leadtoseverecomplicationssuchascornealulcerandevenblindness.
OTHERMEDICATIONSDiamox(Acetazolamide)500mgtabletsGlycerinInjectableanestheticwithepinephrine1:10,000

7
THEAMSLERGRIDWiththis testanyonecanchecktheircentralvisionathome.Apatient should use the Amsler grid to test the central visionevery day to detect any changes that may be caused byworsening age‐related macular degeneration (AMD) or othermaculardisorders.Follow these steps while looking at the grid on the followingpage:
1. Ifyouusuallywearreadingglasses,putthemon.2. Holdthegridatanormalreadingdistance,about12‐14
inchesawayfromyourface.3. Usingonlyyourrighteye(lefteyeclosed),lookatthedot
inthecenterofthegrid.Makesurethatyoucanseetheentiregrid.
4. If any of the lines in the grid look distorted, blurry, ormissing,writedownwhatyousee.
5. Repeat these steps with your left eye while your righteye isclosed. Ifanyof thesechangesarenew,callyourretinadoctorthesameday.

8

9
If the patient sees the lines as wavy, seeming to bend orappearinggray,fuzzyormissingincertainareasofthegrid(oneexample is shownabove), this indicates that somedamagehasbeendonetothemacula,andthepatientshouldbereferredtoaretinalspecialistforfurtherevaluation.

10
TECHNIQUEOFSCHIOTZTONOMETRY
Anesthetizethecorneawithtopicalproparacaineortetracaine.Ask the patient to lie in a supine position looking directlyupward,fixingonaspotintheceiling.Separatethelidstokeepthemfromtouchingtheeyeball,takingcarenottoputanypressureontheeye.Placethetonometergentlyinaverticalpositionoverthecorneawiththeplungerexertingitsfullweight.Thepointerwill givea steady readingwithin0.5mm ineitherdirection.Keepthepartofthetonometerthattouchesthecorneasterile.

11
IPHONEWITHATTACHMENTFORFUNDUSPHOTOGRAPH
There are several models on the market that are compatiblewith other smartphones. (Search Google for, “iPhone,smartphone for fundus photography” and you will find thedifferentoptions.)Anassistantcanbetrainedtodothisjob.Thisisespeciallyusefulfordiabeticpatients.Thephotoscanbecomparedforpossibleprogressionoftheretinopathy.ThephotoscanbestoredintheEMRsystemorcanbesenttoacolleagueforconsultation,especiallyifthepatientiselderlyandlivesfarawayfromanophthalmologist.

12
SNELLENCHART

13
NEARVISIONCARD
This card is used to measure near visual acuity. Although it is close to the correct size, a true-to-scale copy can be printed from the Internet. The card is held in good light 40 cm (16 inches) from the eye. Record vision for each eye separately with and without glasses. Presbyopic patients should read through bifocal segment. Check myopes with glasses only.


CHAPTER 2: HISTORY AND EXAMINATION As this book has been written mainly for primary carepractitioners, it is assumed that examinations will be donewithout the benefit of a slit lamp, using amagnifying glass orloupe.Weallknowhowimportantagoodhistoryandexaminationarein the care of a patient. When a patient shows up in a non‐ophthalmologist’s office with an eye problem, the practitionerhas to be selective and realize that he or she is not providingvision care or complete eye care, but just addressing the eyeproblemforthatvisit.HISTORYThehistorynodoubtrelates to thereasonthepatient is in theoffice,suchasredeye,eyepainordiscomfort,aforeignbodyinthe eye, seeing double, seeing floaters and so on. Thepractitioner needs to know how long this condition has beengoingon,ifitisgettingworse,betterorremainsunchanged,andother things that might be related to the presenting problem.Thepractitionershouldbeasaccurateandpreciseaspossible.A history of eye injuries and the use of eye drops such ascorticosteroid would be pertinent information to gather whendealingwithmosteyeproblems.Itcanalsobeusefultolearnifanyherbshavebeentakenorallyorappliedtopically.

16
THEOCULAREXAMINATION(selectiveandrelevantpertainingtoeachvisit)Hands and fingernails should be clean, and after each patient,especiallythosewithinfections,thehandsshouldbewashed.Trytodevelopthehabitofalwaysexaminingtherighteyefirstand the lefteyesecond,even if thepatientonlycomplainsofaproblem in the left eye.This routineensures that theeyewiththeproblemcanbecomparedtothe“healthy”eye.Visual acuity measurement should usually be done with anypatientwho comes to a primary care provider’s officewith aneyeproblem.Cross‐confrontation visual field testingmayneed tobedone ifthe patient is running into things or experiencing other visualperceptionproblems.Eye movement may be tested to evaluate the integrity of theextra‐ocularmuscles.Examinationof theeyelids, sclera, corneaandconjunctivamaybeneeded.Pupillaryreactivityandsizemayberecordedifrelevant.Theanteriorchambermaybeexamined.Checkforopacityofthelensorvitreousifneeded.Examinationofthemacula,opticnerveandretinamaybedone.Measurementoftheintraocularpressuremaybedone.

17
As the comfort levels of primary care practitioners varies somuch,Irecommendthatcommonsensebeusedastohowmuchexamination is needed for a particular visit. In the case of apatientwitharedeye,whichcouldbecontagious,thelongerheor she is kept in the office, the greater the chances of theinfection spreading to the staff and other patients. Myphilosophyiswhenapatientcomesinwithaneyeinfection,seehim or her as soon as possible, prescribe the appropriatemedication, and don’t keep him or her around to spread theinfection.Ausefulacuitytestisthepinhole(PH)test.Thepinholetestisperformed on a patient with diminished visual acuity, todetermine whether it is due to a refractive error or from anorganicdiseasesuchasmaculardegeneration.Ifyoudon’thavea pinhole occluder, you can create one by making severalpinholes, 0.5–2 mm in diameter, in a card. The patient looksthrough one of the holes one eye at a time without wearingcorrective lenses. If the visual acuity is improved by lookingthrough the pinholes, the problem is refractive. If not, it isorganic. The pinhole effect works by blocking peripheral lightwaves,whicharemostdistortedbyrefractiveerror.Many primary care offices have assistants who can do theSnellen chart test (page 12), which consists of letters ornumbers printed in decreasing sizes according to aninternationalstandard.IntheUS,thedistanceatwhichapatientreadsthechartismeasuredinfeet,i.e.20/20;andintheEU,itismeasured inmeters, as in6/6. If the examination room is lessthan20 feet long, thenuseadistanceof ten feetandmake theadjustmentaccordingly.Ifapersoncanseethe20/40lineat20feet, thenheor she shouldbeable to see the20/20 lineat10feet,andsoon.If the patient’s vision is so poor that the figures on the chartcannotberead,directthepatient’sattentiontotheoutstretched

18
fingersonyourhandandaskthepatienttocountthenumberoffingersyouareholdingupatvariousdistances,suchasat2feet,4feet,etc.Recordthedistanceofthebestfinger‐countingvision.Ifthepatientcannotcountfingersevenatcloserange,thenthelightprojectiontestmaybeused.Testthepatienttodetermineif focal light from a flashlight can be seen in each of the fourretinal quadrants by holding the light about 4 inches from theeyein frontofthe faceandpointing intowardtheeye.Askthepatient to point to the direction of the light. If the patient iscorrect in inall fourquadrants, record theresultsas “accuratelightprojection.”Ifthepatientmakesamistakeinoneormorequadrants, then record it as “inaccurate light projection.” Thistestisusefulifthepatientisbeingscreenedforpossiblecataractsurgery. If the patient has accurate light projection, cataractsurgerywouldmostlikelybenefitthepatient.Ifthepatienthasinaccuratelightprojection,itmaymeanaproblemintheretina.If the patient has NLP (no light perception), cataract surgerymaynotbenefitthispatientandfurthertestingshouldbedone.Even for a patient with extremely dense cataracts, some lightusuallypassesthrough.Commonabbreviationsusedforrecordingvisualacuity:
V(vision) RE(righteye)orOD(oculusdexter) LE(lefteye)orOS(oculussinister) NV(nearvision) PH(pinhole) CF(countingfingers):example,CFat2ft.,4ft.,etc. NLP(nolightperception)
RedReflexTheredreflexteststhelightreflectedfromthebloodvesselsofthe choroid. With a +5 diopter lens in the aperture of the

19
ophthalmoscope,atadistanceofabout8inchesfromthecornea,check to see if the pupil appears red, and is identical in botheyes.A good red reflexmeans that everythingalong the visualaxisisclear.Anymediaopacity,i.e.,cornea,lensorvitreous,willinterrupttheredreflexandgiveabnormalresults.ExaminationoftheRetinaAfter examining formediaopacities,move slowly closer to thepatient’seyewhiledialinginsmallerplus(+)lensnumbersuntilthe ophthalmoscope is a few centimeters from the eye. Adjustthe distance until the retina becomes clear. Then examine theopticnervehead(opticdisc)first,followedbythesmallarteriesand veins. Then examine the macula by asking the patient tolookdirectlyatthelight.Use of the handheld ophthalmoscope to examine the inside ofthe eye through an un‐dilated pupil is not easy and requirespractice. Keep working with it and eventually it will becomemoreroutine.

20
DIRECTOPHTHALMOSCOPE
Therearedifferentmodelsofdirectophthalmoscope.Theneweroneshavesomefunctionsthatareseldomneeded,manyofwhichyoucanignore.The black numbers on the lens selection disc represent pluslenses—tocorrecthyperopia.

21
Therednumbersrepresentminuslenses—tocorrectmyopia.Thesmallerwhiteroundbeamisforsmallpupils.Thelargerroundbeamismostfrequentlyusedandprovidesthelargestviewof the fundus,but it isonlygood fora largepupil,i.e.,usuallydilated.Mostoftheotherbeamshapesareseldomused.Befamiliarwithallthefunctionsoftheophthalmoscope.APERTURES(viewingholes):
SmallAperture:Provideseasyviewofthefundusthrough an undilated pupil. Always start theexamination with this aperture and proceed tomicro aperture if pupil is particularly smalland/orsensitivetolight.Large Aperture: Standard aperture for dilatedpupilandgeneralexaminationoftheeye.MicroSpotAperture:Allowseasyentry intoverysmall,undilatedpupils.Slit Aperture: Helpful in determining variouselevations of lesions, particularly tumors andedematousdiscs.
22
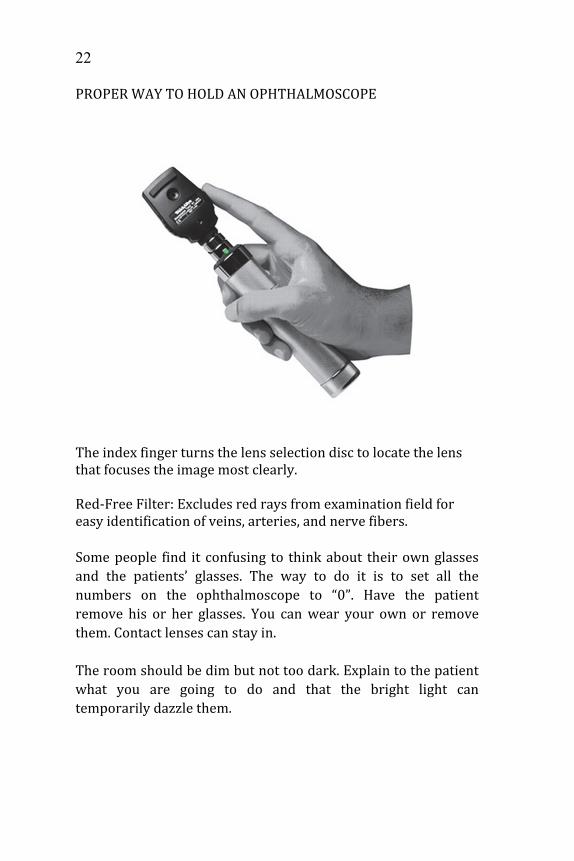
PROPERWAYTOHOLDANOPHTHALMOSCOPE
Theindexfingerturnsthelensselectiondisctolocatethelensthatfocusestheimagemostclearly.Red‐FreeFilter:Excludesredraysfromexaminationfieldforeasyidentificationofveins,arteries,andnervefibers.Somepeople find it confusing to thinkabout theirownglassesand the patients’ glasses. The way to do it is to set all thenumbers on the ophthalmoscope to “0”. Have the patientremove his or her glasses. You canwear your own or removethem.Contactlensescanstayin.Theroomshouldbedimbutnottoodark.Explaintothepatientwhat you are going to do and that the bright light cantemporarilydazzlethem.

23
Positionthepatientsothatheorshe iscomfortablebutsittingup—ifpossible.If you decide to dilate, put one drop of 1% tropicamide(Mydriacil) in each eye and wait 15 to 30 minutes. MaximaldilationcanbeobtainedbyusingMydriacilandNeo‐Synephrinesimultaneously.Evenwith dilation, only about a third of the fundus is visible.The areamost visible is the posterior pole (including the discandthemacula).Youshouldbeabletoseetheocularfindingsofmanysystemicdiseasessuchasdiabetesandhypertension.Yourpatientshouldfixateonaspecifictargetsuchasapieceofpaperwith a big “X” on thewall. This is important so that thepatientdoesnotmovehisorhereyes.Examine the patient’s right eye with your right eye and viceversa.Trytokeepyourothereyeopen,whichmaynotbeeasyandtakespractice.Ifyoucan’t,dowhateveryouarecomfortablewith.Beginatarm’s lengthbyshining theophthalmoscope light intothepatient’spupil;youwillseethered‐reflex(thepupilappearsred instead of black when the ophthalmoscope is not used).Mediaopacities(cornealscar,cataract,vitreoushemorrhageandasteroidhyalosis)obscuretheredreflex.Restyourhandonthepatient’sforeheadanduseyourthumbtohold his or her lid open. Follow the red reflex until yourforeheadrestsonyourthumb–youshouldseetheopticdisc.Ifitisoutoffocus,withoutmovingyourhead,turnthelensselectiondisc eitherway. If the disc becomes clearer, keep turning. If itbecomesblurrier,turnthedialtheotherway.Itisdifficulttoseemore than one disc diameter with the visual field of a directophthalmoscope.Youhavetotilttheinstrumentsimultaneously

24
with your head to different positions to have a compositepictureofthefundus.Look for the optic disc size, color, cup disc ratio, margins,hemorrhages, new vessels and collaterals. Pale and clearlydemarcateddiscindicateopticatrophy.Newvesselsonthediscsuggest proliferative diabetic retinopathy (there are othercauses of new vessels). Yellow‐gray discwith blurredmarginswithorwithouthemorrhagessuggestspapilledema.Look for venous pulsation. If it is present, it strongly suggeststhatthereisnopapilledema,becausevenouspulsationisoneofthe first things to disappearwith papilledema. The absence ofvenouspulsationdoesnotmeanmuchsinceitmaybedifficulttodetectinnormalpeople.Fromthedisc,followthevesselstolookforarterioscleroticandhypertensive changes. Look as far as the mid‐peripheral forhemorrhages, exudates, scars and pigmented lesions. Examinethe arteries andveins (slightly thicker); theA/V ratio is about3/5.Checkthearteriolesfornormallightreflex.Lookforcopperor silver wiring—a sign of thickening of the arteriolar mediafound in eyes with long standing hypertension. Examine thearea adjacent to these vessels for micro‐aneurysms, exudates,venousbeading,venousloopsandabnormalnewvessels.To examine the macula, have the patient look into your light.Thefovealreflexisseenbetterwithagreen(red‐free)filterandistwodiscdiametersawayfromthediscand1.5degreesbelowthe horizontal. Look for hard exudates, hemorrhages andpigmentarychangesinthemacula.Iwillagaindiscussdilationoftheeyelater.IntheUS,1in1000ofthepopulationover40willdevelopangleclosureglaucoma. It isveryunlikelythatbydilatingyourpatients’eyes,youwilltrigger

25
anattackofangle closure. If that shouldhappen, the symptomsareobviousandeasilytreated(seechapteronglaucoma).INDIRECTOPHTHALMOSCOPYThis isa techniqueusedbyophthalmologists involvingahead‐mounted,prism‐directed lightsourcecoupledwiththeuseofacondensing lens, usually +20 or +28. The image is real andinverted,aswellasstereoscopic,coveringtentimestheareaofadirectophthalmoscope.Ithasmanyadvantagesoverthedirect,but the learningcurve issteepandtheequipment isexpensiveand cumbersome; and, in addition, the eye is usually viewedthroughadilatedpupil.PROPERTECHNIQUETOINSTILLEYEDROPS
1. Washyourhands.2. Have thepatientseated,with thehead tiltedback,eyes
lookingup.3. Pull the lower lid down gently to expose the palpebral
conjunctiva.4. Instillthedrop(s)intothelowerconjunctivalfornixbut
not on the cornea directly. Do not touch the tip of theapplicatororallowittotouchthepatient’scornea.
5. Havethepatientclosebotheyesforafewseconds.6. Go over the above stepswith the patient. If necessary,
thetechniquemaybemodifiedtosuitthepatient.


CHAPTER 3: ANATOMY
Cornea: The clear circular part of the front of the eyeball. Itservesasarefractivesurface(makinglightchangedirection)tohelp focus the object on the retina. It is avascular and gets itsnutrientsfromtheaqueous.

28
Pupil:Theroundopening in thecenterof the iris thatcontrolstheamountoflightenteringtheeye.
Iris:Thecoloredpartoftheeyethatdeterminesthesizeofthepupil.Itiscontrolledbytwomuscles:The sphincter muscle is responsible for closing the pupil inbright light and is innervated by the parasympathetic system.Whenaparasympathomimeticdrug likePilocarpine is instilledon the eye, it will cause the sphincter around the pupil tocontract,makingitsmall.The other muscle in the iris, the radial or iris dilator muscle,runsfromtheedgeofthepupiltoitsbaseandisinnervatedbythe sympathetic system. When Phenylephrine, asympathomimetic drug, is instilled on the eye, it causes thismuscletocontract,thuspullingthepupilopen.
Anterior chamber: The space between the cornea and the iris,whichisfilledwithaqueoushumor.
Posteriorchamber:The small space filledwithaqueoushumorbehindtheirisandthefrontofthelens.
Conjunctiva: The almost transparent vascular mucousmembrane covering the sclera (bulbar conjunctiva) and theinnersurfaceoftheeyelids(palpebralconjunctiva).
Lens: The biconvex clear structure behind the iris and pupilresponsibleforfocusingtheimageontheretina.
Aqueoushumor:Theclearfluidthatfillsthespacebetweenthecorneaand iris (anteriorchamber) thatnourishes the lensandcorneaandgivestheeyeitsshape.

29
Ciliarybody:Thestructurethatproducestheaqueoushumor.Italso connects the lens—via suspensory ligaments—to thechoroid.Itcontainstheciliarymuscles,andwhenitcontracts,itreduces the tension on the lens, making it more convex andfocusinglightclosertothelens,i.e.,accommodation.
Suspensory ligaments: Ligaments between the lens and ciliarymuscles.
Sclera:Thethickwhiteoutercoatof theeyethat iscoveredbytheconjunctiva.
Choroid: The middle layer of the eye wall. It is vascular andpigmented.Itprovidesbloodsupplytotheouterretinallayers.
Retina:Theinnermostwalloftheeyeconsistingofneuraltissue.It sends visual signals to the brain via the optic nerve to beinterpreted.
Macula:Theareaoftheretinaadjacenttotheopticnervethatisresponsibleforcentral,finevision.
Fovea:Thecenterofthemacularesponsibleforthefinestvision.
Blind spot:The areawhere theopticnerve enters the eye andpassesthroughtheopticdiscwherethereisnoretina,hencetheeyedoesnotseeanythingatthatspot.
Opticdisc:Alsocalledtheopticnervehead.Theusuallyyellow,circular junction, nasal to themacula, where the ganglion cellaxons exit the eye, pick up a myelin sheath, and become theopticnerve.Theopticnerveconnectstheeyetothebrain.
Vitreoushumor:Atransparent,jelly‐likesubstancethatfillstheeye behind the lens, extending to the retina and measuringabout4.5ccinvolume.

30
Uvea:Thepigmented,vascularmiddlelayeroftheeyeconsistingofthechoroid,ciliarybodyandiris.

CHAPTER 4: BASIC OPTICS MYOPIAANDHYPEROPIAAn emmetropic eyeball is one with no refractive error. Theabsolutesizeoftheeyeballisimmaterialaslongasitistherightlengthtogoalongwiththeothercomponentsofeyerefraction,i.e.,cornealcurvatureandlenspower.
MyopiaMyopia is also called near‐sightedness because myopes havegoodnearvisionbutpoordistantvision.Theeyeballistoolongfor the refractivepowerof the corneaand lens. In general,wetend to associate a large eyewithmyopia. It is correctedwithconcave(minus)lenses.Theconcavelensbringstheimageintofocusinfrontoftheretina.
Withanemmetropiceye,visionisconsidered“normal”anddoesnot require corrective lenses.Theimagefocusesdirectlyontotheretina.
Amyopiceye(left).Theimageformstoofarinfrontoftheretina.Theconcavelens(right)lengthensthefocalpointoftheimagetofocusontheretina.

32
Highmyopiaisdiagnosedwhenthelensrequiredtocorrectthenear‐sightedness is greater than 6 diopters. The elongation ofthe eyeball can be progressive throughout life, leading todegenerationoftheretina.Thereisahigherincidenceofretinaldetachmentinhighmyopes.LASIK (Excimer laser in situ keratomileusis) for correction ofmyopia
HyperopiaHyperopia or far‐sightedness is corrected with convex (plus)lenses.Itiscalledfar‐sightednessbecauseonecanseewellatadistancebutthenearvisionispoor.Theeyeballistooshortforthecorneaandthepowerofthelens.
1. Cornealflapopened.
2. Ablationofstromalbed.Tissueremoved(grayarea).
3. Flapreplaced.Centralcorneaisnowflatter(lessmyopic).

33
For hyperopes, symptoms of eyestrain tend to have an earlieronsetthanmyopes,andtheyoftenneedreadingglassesearlierthanmyopesbecauseofthelossofaccommodation.Becauseofthe smaller eyeball, primary angle‐closure glaucoma is morecommoninpeoplewithhyperopia,somethingoftenseeninEastAsians,especiallyamongtheChinese.Presbyopiaoccurswhenthelenslosesitsaccommodationwellenough to focus on near images as a result of age‐relatedprocesses,ratherthantheanatomicalfactorsthatcausenear‐orfar‐sightedness.Thisoccursearlier(aroundageforty)inpeoplewithhyperopiaandlaterinmyopiceyes.Bifocal glassesmaybeneeded forpeoplewhoneed correctionforbothdistantandnearvision.Reading glasses with power from +1.00 to +3.00 can bepurchased inmost drug stores. Suggest that your patients trythemoutandfindtheone(orones)thatmeettheirneeds.Usingdrugstorereadingglasseswillnotdamagetheeyes.APHAKIAAphakiareferstoaneyethatnolongerhasitsownnaturallens,usuallyfollowingcataractsurgery.Agenerationago,manyofthepatientsindevelopingcountrieswhohadcataractsurgerywere
Inahyperopiceyeball(left),thefocalpointislocatedbehindtheretina.Aconvexlens(right)isrequiredtoaccommodate.

34
fittedwiththickglassestoreplacetheopticalpowerofthelensremoved.Theproblemwithsuchacorrectionisthattheimagethepatientseesisabout30%largerthanthatofthelensinsidethe eye. This is a big concern for patients who are active,becausethemagnificationofvisioncancausethemtomisjudgetheirsteps,resultinginfalls.
Visioninanaphakiceyewithoutcorrectionisextremelyblurryandthepatientisusuallyconsideredessentiallyblind.Pseudophakiaisthetermusedtodescribeaneyewithanintra‐ocular lens (IOL). The quality of the intra‐ocular lens hasimprovedgreatlyoverthelasttwentyyears,andtheirpricehasreduced drastically. Now most patients even in the poorestcountries receive an IOL following cataract surgery. The IOLusuallycorrectsdistantvision,but thepatientstillhas towearreading glasses.However, there arenowall sorts of new IOLs,some ofwhich enable the patient to see clearly at distance aswellasnear.ASTIGMATISMAstigmatism occurs when the cornea is not symmetricallyround. Instead of being like a basketball, it is shaped like afootball, with one meridian more curved than the meridianperpendiculartoit.Imaginethefrontoftheeyeasthefaceofaclock.Thelinefrom12to6isthe90‐degreemeridianandfrom
Imageis30%largerinaphakicpatientscorrectedwithspectacles.

35
3to9isthe180‐degree.Thesteepestandflattestmeridiansarecalled the principalmeridians and are always 90 degree fromeach other. The irregular shape of the cornea in astigmatismpatientscauses light to focusonmultiplepoints (eitherbehindorinfrontoftheretina,orboth)insteadofasinglefocuspoint,andtheresult isblurryordistortedvision.Eyestrain,squintingandheadachescanalsobesymptomsofastigmatism.Correction forregularastigmatismcanusuallybe incorporatedintoeyeglasses.Refractivesurgerycanalsosometimesbeusedtocorrectregularastigmatism.Irregularastigmatismisfarlesscommonandisusuallycausedby diseases such as keratoconus, or by scarring after an eyeinjury. It is usually treated with rigid gas permeable contactlensesinsteadofcorrectivelenses.TypesofAstigmatismHyperopic astigmatism. One or both principal meridians arefar‐sighted, i.e., at least one focal point is located behind theretina.Theimageontheleftissimplehyperopicandtheoneonthe right is compound hyperopic. The short lines in thefollowingdiagramsindicatepointsoffocus.

36
Mixedastigmatism.Oneprincipalmeridianisnear‐sighted,andtheotherisfar‐sighted.
Myopic astigmatism. One or both meridians of the eye arenear‐sighted.Theone on the left is compoundmyopic and theoneontherightissimplemyopic.
Thisisanexampleofsimplemyopicastigmatism:
Thevertical(90degree)beam(AB)isfocusedontheretinaandneedsnocorrection.The horizontal (180 degree) beam (CD) is focused anterior totheretinalikethatinamyopiceye.

37
The horizontal beam (CD) can be corrected with a myopiccylindricallens.
CONTACTLENSESContact lenses reston the cornea.Theyhave someadvantagesoverregularglasses.
Theyareoftencosmeticallymoredesirable. Inpatientswithveryhighrefractiveerrorsuchasaplus
10, strong convex lenses are needed. This hyperopicpatient’s glasses would be very thick and theenvironmentwouldappearmagnified.Thefieldofvisionis also restrictedwith pronounced distortionwhen thepatient looks through the edges of the glasses. Thepatient’s eyes also appearmagnified to the observer. Apatient with high myopia sees the environment assmaller than normal and also experiences distortionwhenlookingthroughtheedgeoftheglasses.Theireyesappear small to theobserver.A contact lens eliminatestheseproblems.
Thevisionofapatientwithirregularastigmatismcanbecorrectedwithcontactlenses.

38
Thenegativeaspectsofcontactlensesare: Many people find them difficult to wear or hard to
handle. Ifnotwornproperly,theeyecanbedamaged. Theyaregenerallymoreexpensivethanglasses. The contact lens wearer must live in a clean
environment, which is not always possible in somedevelopingcountries.
There are many types of contact lenses and they continue toimprove.Itisaspecialtyinitself.

CHAPTER 5: EYELIDS, CONJUNCTIVA, CORNEA AND SCLERA COMMONEYELIDCONDITIONSBlepharitisBlepharitis is a common inflammationof theeyelids. Itusuallyinvolves the lashes, lidmargin and themeibomian glands (oilglandsliningthelidmarginthatpreventdryingoftheeye’stearfilm).Itisafrustratingconditionforthepatientasitcanbeveryuncomfortable and include irritation, redness and tearing. It isalso frustrating for the physician because it is a recurringcondition,andpatientsoftenfailtounderstandwhyitcannotbecured.In anterior blepharitis, the meibomian glands are notprimarilyinvolved.Itoccursalongtheoutsideedgeoftheeyelidwhere the eyelashes attach, and symptoms can includeirritation,itching,crustingalongthelidormissingeyelashes.Inposteriorblepharitis, themeibomian glands are inflamed,leadingtoblockageandcystformation.Itoccursalongtheinneredge of the eyelid where it touches the eyeball, and can alsocausecrusting,irritationandmissingeyelashes.Therapy is essentially life‐long as it recurs frequently ifmeticulous lid hygiene is not followed. Lid hygiene involvesscrubbing the eyelids with baby shampoo followed by warmcompressesseveraltimesaday.Topicalantibioticdropsand/orointment may be needed. If the inflammation is severe,

40
corticosteroid drops or ointment may be required. Acombinationof corticosteroidandantibioticdropsorointmentisoftenused.In severe cases—when the condition recurs and there isexcessiverednessandirritation—inadditiontothe lidhygieneand topical treatment,oraldoxycyclineorminocycline100mgq.d. for 3 weeks may be prescribed. Longer courses may beneeded in persistent cases. For pregnant women and childrenunder 10, erythromycin 250 mg p.o. q.d may be substituted.Usually, when blepharitis becomes severe, the patient shouldseeanophthalmologist.
HordeolumAHordeolum(orstye)isanacuteinfectioninvolvingtheeyelashfollicles(externalhordeolum)ormeibomianglands(internalhordeolum) and is commonly caused by Staphylococcus. It isusually painful and includes purulent discharge (pus).Treatmentisthesameasforblepharitis.ChalazionChalazion is a chronic infection of a meibomian gland, whichmay be the result of a chronic hordeolum. It is usually notpainful for the patient. Initial treatment is the same as forblepharitis. If the lesiondoesnot resolve ina coupleofweeks,incision and curettage from the inside of the lid through theconjunctivamaybeneeded.

41
CONJUNCTIVARedEyeRedEyeorconjunctivitisisoneofthemostcommonconditionsseenintheoffice.Itisageneraltermthatactuallycoversmanydifferent conditions. It is important to make the correctdiagnosisbeforeappropriatetreatmentscanbeinitiated.Conjunctivitiscanbedescribedaspurulentornon‐purulent.BacterialConjunctivitisBacterial conjunctivitis is usually characterized by pus(purulent) discharge. It can be bilateral or unilateral. Noenlargedpre‐auricularlymphnodesareusuallyfound.ThemostcommoncauseofmildconjunctivitisandblepharitisisStaphylococcusaureus.Mostmild conjunctivitis canbe treatedwith topical antibiotic drops and/or ointment. Any of thefollowing antibiotics can be used for mild conjunctivitis:sulfacetamide, erythroymycin, bacitracin, tetracycline andothers.Iftheinfectionissevere,cultureforidentificationofthebacteriashould be done. Infection by Pseudomonas and Klebsiella cancause severe corneal destruction and can lead to blindness. Ifeitherofthesebacteriumarepresentintheculture,thepatientshouldbetreatedbyanophthalmologist.ViralConjunctivitisViral conjunctivitis is non‐purulent and can be caused by anumber of viruses. It is usually bilateral and enlarged pre‐auricular nodes are present. The conjunctiva is diffusely red

42
because of the vascular reaction, and it may have waterydischarge.The infectionmay be spread by coughing or sneezing. Amaskmust be worn when examining this group of patients. Theinfection usually clears in a week to ten days. If the infectionappears to be severe, an antibiotic drop or ointment such astetracycline1%twiceadayforfivedaysmaybeusedtopreventsecondaryinfection.EpidemicHemorrhagicConjunctivitisEpidemic hemorrhagic conjunctivitis or adenoviralconjunctivitis (pink eye) is an extremely contagious viralinfection. It is usually bilateral and enlarged lymph nodes aretypically not found. The cornea is usually not affected. Thepatient looks terrible because of the diffuse sub‐conjunctivalhemorrhage.Maskandglovesmustbewornwhenexaminingapatientwiththis infection. If there is an epidemic, such patients should bediscouraged from coming to the office, as they can spread thediseasefurther.Tetracycline 1% ointment twice a day for seven days may beusedtopreventsecondarybacterialinfection.AllergicConjunctivitisAllergicconjunctivitisisnon‐purulentandmaybeseasonal.Theprimarysymptomisitching,andthepatientmaygiveahistoryof“hayfever”andbronchialasthma.Visualacuityisusuallynotaffected, and enlarged pre‐auricular lymph nodes are notpresent. Careful examination of the bulbar (covering the eye)andtarsal(thefibrousconnectivetissuethatsupportstheedge

43
of the eyelid) conjunctivamay showpapillae (small bumps)ofvascularreaction.Topical corticosteroid is the treatment in the acute phase, butthediagnosismustbecorrectbeforesuchtreatment isstarted.Long‐term use of topical corticosteroid use can cause cataractandsecondaryglaucoma.Patients with chronic allergic conjunctivitis may use anantihistamine or non‐steroidal drops to prevent recurrence.Zaditor(ketotifen) isnowavailableasanOTCeyedrop. Itactsasamast‐cellstabilizerandantihistamineandisveryeffective.Combinationofpheniramineandnaphazolinedrops (OTC) canprovide relief of itching and redness associated with seasonalallergicconjunctivitis.Patients should be warned against over‐use of oculardecongestants(usuallyaweakadrenergicstimulatingdrugsuchas phenylephrine hydrochloride 0.12%), which can result inreboundvasodilationofconjunctivalvessels.SubconjunctivalHemorrhageThisisadeepredhemorrhageundertheconjunctiva,whichcanappear spontaneously or as a result of coughing, sneezing orstraining. In theabsenceof traumaoradenoviralconjunctivitis(pink eye), no treatment is necessary. The patient should bereassuredthatthebloodwillclearin2to3weeks.If the condition is frequent and recurrent, a medical workupmay be necessary to rule out hypertension or a bleedingdisorder.

44
CORNEACorneal foreign bodies are among the most common eyeinjuries. They should be addressed as soon as possible toprevent permanent damage. The foreign body could beanything:sand,ametalfragment,vegetablematter,etc.A corneal foreignbodyusually causespainand interfereswiththe vision. Topical anesthetic and sometimes fluorescein dyemay be applied before performing the examination under abright light with a loupe. Lid eversion may be necessary toexposeaforeignbodyembeddedinthetarsusoftheupperlid.A cotton‐tipped applicator should be tried first, and if theforeign body cannot be removed with the cotton‐tippedapplicator, a 25‐gauge needle with the bevel up can be triednext.If the foreign body is a metal fragment that has been on thecornea for a few days and a rust ring has formed, the patientmay need to be referred to an ophthalmologist for removal oftherust ring.A rust ringmaycause scarring; and if it is in thevisual axis, it may interfere with the vision. If it is in theperipheral cornea, and referral to an ophthalmologist is notpossible, the rust ring may be left alone. A primary carephysician comfortable at the slit lamp may be able to use abattery operated handheld burr (e.g., the Alger Brush CornealRustRingRemover)toremovetherustring.Anantibioticointmentwithoutcorticosteroidshouldbeinstilledin the inferior fornix (the space in the fold of the lower lid)followed by an occlusive eye patch. The patient should be re‐examined in 24 hours to confirm epithelial healing. A non‐healing epithelial defect can lead to a corneal ulcer. Thesepatientsmustseeanophthalmologistbecausethedefectcanbeblinding.

45
CornealChemicalInjuriesA corneal chemical injury is an emergency. Copious amountofclean water should be used to irrigate the eye(s). A drop oftopicalanestheticmaybenecessarytohelpthepatientkeeptheeye(s) open while being irrigated. If a tap is available, thepatient’s head should be placed under runningwaterwith theeye(s) open for at least five minutes. Examination withfluoresceindyeisthendonetoevaluatetheextentoftheinjury.Theworstinjuriesarecausedbyalkaline(basic)chemicalswithapHofgreaterthan7.0,whichincludemanycleaningfluidsandlye (sodium hydroxide compounds). These chemicals canpenetrate the cornea in seconds. Irrigation of the eye shouldcontinue until the pH (tested with a litmus paper) becomesneutral.Ultraviolet(UV)BurnsWelding arcs and sun lamps are the most common causes oflight‐induced injury to the cornea. These can be prevented bywearingUV‐blockingplasticspectaclesorshieldswhenexposedtotherays.AneyewithaUVburnmayshowedemaonthelid,conjunctivalhyperemia,andcornealpunctaterougheningoftheepithelium.The patient may come in with severe pain, photophobia andspasmofthelid.Treatment is a short‐acting cycloplegic drop such ascyclopentolate1%torelieveciliaryspasm,andtopicalantibioticointment. A semi‐pressure dressing with the eyes well closedunderneathshouldbeappliedandleftonfor24hours.Apatientinseverepainmayneedanalgesicsandsedatives.Theburnwillusuallyhealwithin24to48hours.

46
HyphemaHyphemaorbloodintheanteriorchamberisusuallycausedbyaseverecontusiontotheeyeball,suchasbeinghitintheeyebya baseball. It is treated with bed rest and, in some cases,sedation to preventmovementof the eye,which can cause re‐bleeding.Ifthebleedingdoesnotresolve,itcanstainthecornealendothelium.Itcanalsocausesecondaryglaucomabyblockingtheaqueousdrainage.Surgicalremovaloftheclottedbloodmaybenecessary.CornealUlcerThisisaveryseriousconditioncausedbyerosionandinfectionofthecornea.Itcanproducepermanentscarringandblindness.Theinfectingagentcanbebacterialorfungalorboth.Thisisanemergency and early identification of the organism(s) willreduceorpreventseriousscarring.The common bacterial agents include: Staphylococcus,Streptococcus pneumonia, Haemophilus and Moraxella.Pseudomonas and Klebsiella are less common but are muchmoredestructive.DiagnosisPus is usually associated with a corneal ulcer. The ulcer canoccur anywhere on the cornea and appears as a yellowish orwhitish depression or defect. The patient usually complains ofpain, loss of vision and tearing. The entire eye looks veryinflamed with injection of the blood vessels. In severe cases,hypopyon (abnormal cells) may be present in the anteriorchamber.A patientwith a corneal ulcer should be under the care of anophthalmologist. If that is not possible, consultation should be

47
done remotelyunder theguidanceof theophthalmologist, andthepatientshouldbeadmittedtothehospitalforintensetopicalantibioticand/orantifungaltreatment.The eye should not be patched, as patching an infected eyewouldonlymakeitwarmer,darkerandmoremoist,allofwhichwouldmaketheinfectionworse.HerpesSimplexKeratitisThisisaseriouscondition.Thevirusinitiallyinfectsthecornealand conjunctival epithelium, and can invade deep into thecornealstroma.Secondarybacterialinfectionmayoccurandcanlead to corneal perforation and permanent blindness. Densecornealscarringcanoccurinsomeherpessimplexinfections.Thediagnosiscanbemadebythetelltaledendritic(branching)patternofcornealepithelialdefectwhenexaminedwiththeaidoffluoresceindye.Otherstainingpatternsmayalsooccur.Topical corticosteroids should never be used to treat thiscondition.Itcanleadtodeeperinvasionbythevirus,worseningtheinfection.The treatment is ganciclovir 0.15%ophthalmic gel, trifluridine1%(Viroptic)orvidarabine3%ointment.Oralanti‐viralagents(acyclovir400mgp.o.fivetimesperdayfor7to10days)maybeprescribedtoavoidthetoxicityoftopicalanti‐viraldropsorwhendropscannotbegiven,suchaswhentreatingchildren.When no anti‐viral agent is available, treatment with anantibiotic drop or ointment should be given to preventsecondarybacterialinfection.

48
PterygiumPterygium is a conjunctival growth extending onto the cornea,usuallyonthenasalside. It ismorefrequent insunny,hot,dryanddustyplaces.Ifthegrowthbeginstoencroachonthevisualaxis, itshouldbesurgicallyremoved.Therecurrencerateusedto be high, but now, with the help of antimetabolite drugs,recurrenceislessfrequent.
SCLERAScleritisThisisaninflammationofthescleraandmaybeasignofsystemdisease such as rheumatoid arthritis. The patient usuallycomplainsofanachingpainintheeye,andtheeyeballisusuallytendertothetouch.Thelesionispinkishandseemstoliedeepintheconjunctiva.Visionisusuallynotaffected.Topical corticosteroid is the treatment. The patient should befollowedcloselytowatchforcomplicationsofthecorticosteroid,and it should be stopped as quickly as possible. Non‐steroidalanti‐inflammatory drugs may be substituted to preventexacerbation of the condition. Chronic scleritis can lead toscleralthinning.

CHAPTER 6: CATARACT Cataractisdefinedasanyopacityinthenaturalcrystallinelens.AnatomyoftheCrystallineLens
The crystalline lens is enclosed by a clear elasticmembrane.
Theanteriorcapsulesitsimmediatelybehindtheiris. The epithelium is a layer of cells beneath the anterior
capsule. The cortex is a clear protein substance inside the
capsule. Thenucleusisthecenterofthelens. Theposteriorcapsulefacesthevitreous.
When we are young, the nucleus is soft. As we get older, itbecomesprogressivelyharder.
NucleusCortexAnteriorcapsuleEpithelium

50
It is generally believed that excessive exposure to ultravioletlightcancausecataract,asdemonstratedbythehighincidenceof the condition in countries close to the equator and at highaltitudes. Poor nutrition and smoking may be contributingfactorsinthedevelopmentofcataract,andcertaindrugssuchascorticosteroids,eitheroralortopical,canalsocausethedisease.Some other well‐known causes include trauma, diabetesmellitus,andinflammation.In addition, cataract can be congenital secondary tometabolicdiseases such as galactosemia. Fetal infectionwith the rubellavirus before the ninth week of gestation can also cause thedisorder.A patient with a cataract will complain of blurry vision. Thecataractcanbeseeneasilywithaslitlamp;orapocketflashlightor direct ophthalmoscope canbe used to detect the opacity aswell. If the lens appears cloudy, a cataract is present. In earlystages, before surgery is indicated, primary care physiciansshould recommend that their patients follow a healthy diet,exercise, avoid smoking, and protect their eyes from UV light.Onceacataractissuspected,thepatientshouldbereferredtoanoptometristorophthalmologistforfurtherevaluation.SurgicalTreatmentofCataractWhen I didmyophthalmology residency in the late1970s,wealmost entirely performed intracapsular cataract extraction(ICCE) for the treatmentof cataract.This is the removalof theentirelens,usuallywithacryoprobe.Theprobeisconnectedtoa cryo (freezing)machine,whichmakes it extremely cold, andwhen theprobe touches the lens, the lens becomes an ice ballandisthenremovedfromtheeye.The problemwith thismethodwas that it hadmany potentialcomplications, some of which were severe. The anterior

51
chamberIOL(intraocularlens)implantedafterthelensremovalalso caused many complications. Patients were usually fittedwith thick spectacles following surgery,which caused them tosee objects about 30% larger. They had to be careful gettingaround, as they had to learn to judge their new spatialrelationship.
WhenIbeganmypracticeintheearly1980s,theextracapsular(ECCE) method was gaining popularity. This had manyadvantagesovertheICCEbecauseitrequiredasmallerincision.Only the opaque portions of the lens were removed. Theintegrity of the posterior capsule and anterior vitreous facewerenotdisturbed.This significantly reduced the incidenceofcomplications, which included retinal detachment and cystoidmacularedema(CME).With the ECCE method, intraocular lenses had become muchsaferbecausetheycouldnowsitontheposteriorcapsuleawayfromthevascularstructuresintheanteriorchamber.
Aphakicvisionwithoutcorrectionislikebeingblind(left).Correctionwiththickglassesmakestheimageabout30%larger(right).

52
ECCEMethod
Theanteriorcapsuleisopenedandremoved. Thehardnucleusisremoved. Theloosecortexisthenremovedby
aspiration/irrigation. Theposteriorcapsuleremainsintact. TheIOLisplacedinsidethecapsularbag,restingonthe
posteriorcapsule.Thephacoemulsificationmethod (usingultrasonicenergytoremove the cataract before placing the IOL) is now generallyused in developed countries. In developing countries, mostcataract surgeries are donewith the ECCEmethod, which hasproventobejustassafeandeffectiveasthephacoemulsificationmethod.Thephacoemulsificationmethodismoreexpensive,asit is done with an expensive machine, and extra costs areincurred in each case with disposable supplies such as tubingandfluid.Cataract surgerywith femtosecond laser is a newmethod ofremoving the cataract using ultra‐fast energy pulses to breakapartthecataractatthemolecularlevel.Thisinvolvesamachineevenmoreexpensivethanthephacoemulsificationmachine.Themajority of cataract surgeries in the US are done using thephacoemulsificationmethod.

53
Whenshouldthecataractberemoved?Itdependsonthevisualneedsofthepatient.Whenthevisionisblurryenoughtointerferewithactivitiesofdailylivingsuchasreadingprintandseeingsignswhiledriving,surgeryshouldbeconsidered.IntheUS,theDMVrequires20/40visioninatleastone eye for a driver’s license, although sometimes exceptionsmaybemadefollowingadrivingtest.Someprofessions,suchasairlinepilots,requirebettervision.Cataractsurgeryisoneofthesafestsurgicalprocedures,andupto 95% of patients will find an improvement in their vision.However, it is a surgery and it carries some risks. Infection isveryrare,about1to2inathousand,butwhenitoccurs,itcanbeveryserious.Congenital cataracts should be treated as soon as possible toprevent amblyopia (lazy eye). When a baby is born, the eyeshavetolearntoworkwiththebraininordertosee.Ifthevisionisblockedbyacataract,theeyeisunabletosendclearimagestothebrainanditmayneverlearntoseeclearly.Whenthatchildbecomesanadult,evenafterthecataractisremoved,thevisionwouldstillbeveryblurry.


CHAPTER 7: RETINA AND VITREOUS This isanexcitingtimetobearetinaspecialistbecausewehaveso many more options for treatment. When I finished myfellowship in the early 1980s and beganmy practice, laser hadonlybeenusedtotreatdiabeticretinopathyforafewyears.Therewas essentially no treatment for macular degeneration. In theearly2000s,anew classofdrug calledanti‐VEGFwasavailablefor treatment in macular degeneration, and this totallyrevolutionizedthemanagementofthisdisablingdisease.Primary care doctors need to know the most common retinalconditions so that they can make appropriate and timelyreferrals. Any abnormality observed in the retina should bereferred to an ophthalmologist. Practice with theophthalmoscopewillmake recognizing the difference betweennormalandabnormaleasierwithtime.DIABETICRETINOPATHYDiabetesmellitus can be such a devastating disease because itcanaffectalmosteveryorganinthebody,especiallythosewithsmall blood vessels such as the eye, the kidneys and theperipheralnerves.Diabetic retinopathy is one of the top causes of blindness allover the world. With developing countries becoming moreprosperous and the people taking in more calories, there hasbeen a drastic increase in diabetes mellitus among thesepopulations.WhenIspenttwoweeksinWesternSamoain2014treatingpatients,Iwasdistressedtoseesomanypeoplecoming

56
into theclinicwithadvanceddiabetic retinopathy.Someof theeyeswerebeyondlasertreatmentandwentblind.Theincidenceof diabetes in Western Samoa is between 20% and 25%. InChina, which we don’t usually associate with a high rate ofdiabetes, I was surprised to learn that the incidence of thediseasehasgoneupto10%inrecentyears.The duration of diabetes is the major risk factor in theappearanceofdiabeticretinopathy.After25yearsasadiabetic,a patient has a 26% chance of developing the severe form ofretinopathy, the proliferative type that can cause blindnesswithouttreatment.Pathogenesis:After prolonged periods of exposure to high levels of glucose,the capillaries are damaged from the loss of intramuralpericytes.Theblood‐retinalbarrier is compromised, leading tocapillaryclosure.Ifthecapillaryclosureisextensive,itcanleadtotheproductionofachemicalsubstancecalledVEGF(VascularEndothelialGrowthFactor).Ascapillaryclosurecauseshypoxia,the body tries to grow new vessels to repair the damage.Unfortunately, this can cause serious complications in the eye.Instead of helping the hypoxia, the production of new vesselscanbleedinsidetheeyeorgoontofibrosis,pullingontheretinaandleadingtoretinaldetachment.

57
Blindnessistheendresultofuntreatedneovascularization.Management:Good control of the patient’s glucose levels will reduce theseverityoftheretinopathy.Hypertension is associated with 20% of diabetics, and theelevatedbloodpressurecanfurthercomplicatearetinopathy.
Abnormal new vessels on the retinal surface, caused byhypoxia in the tissue, which produces VEGF andstimulates the growth of neovascularization. Theseabnormal vessels can cause bleeding in the eye. If nottreatedwith laser, they can go on to fibrosis and causetractionretinaldetachment.

58
Treatment:Lasertreatmenthasproventobeaveryeffectivetreatmentfordiabetic retinopathy. By destroying the neovascularization, thecomplication of bleeding into the eye is eliminated, and thevesselsarealsopreventedfromgoingontothefibroticstage.Bydestroyingpartoftheretinathatislessimportantforourvision,wesavethecentralretina,i.e.,theareaaroundthemaculathatisessential. Once the sick retinal vessels are destroyed, they nolonger require oxygen. This helps the hypoxic situation andprevents further release of VEGF and the production ofneovascularization.TYPESOFDIABETESTypeI(juvenileonset)Thisisbelievedtobeanautoimmunedisease,usuallytriggeredby an illness that leads to the destruction of the insulin‐producing cells in the pancreas. This grouphas a high risk fordevelopingsevereproliferativeretinopathy.TypeII(adultonset)Themajorityofpatientswithdiabetesbelongtothisgroup.Itiscaused by insulin‐resistant receptor cells. The insulin level isusuallynormalandcanevenbeelevated.TYPESOFDIABETICRETINOPATHY
1. Background retinopathy (non‐proliferative): This isan early stage of retina damage caused byconstricting capillaries in diabetics. The patient’svision will not be affected at this stage. Findingsinclude intra‐retinal hemorrhages, dilated veins,hardexudates,microaneurysms,retinaledema,CWS(CottonWoolSpots)anddot‐blothemorrhages.

59
2. Pre‐proliferativeretinopathy:Thisisthemostsevere
stageofbackgroundretinopathyinwhichsymptomshave increased in severity, but new vessels are notyet forming. It can include venous beading, asignificantindicatorthatthesepatientswilllikelygoontotheproliferativestage.
3. Proliferativediabeticretinopathy:Thisoccursin5%of patients with diabetic retinopathy. New bloodvessels (neovascularization) grow on the surface ofthe retina and the optic nerve, and sometimes intothe vitreous. This can lead to vitreous hemorrhageand/ortractionretinaldetachment.
4. Diabetic maculopathy: This finding may be seen inanyphaseofretinopathyexcepttheveryearlyphaseofbackgroundretinopathy.Macularedemabuildsupduetoincreasedvascularpermeability,wherebythebloodvesselsleakfluidontothemacula.
LASERTREATMENTThis is usually done in the office and takes from 15 to 30minutes, depending on the type and extent of the treatment.Onlytopicalanestheticsarerequiredinmostcases.In proliferative diabetic retinopathy, pan‐retinalphotocoagulation (PRP) is needed. This usually requiresmorethanone session. Inone session,up to500 laser spotsmaybeappliedtotheperipheralretina.In macular edema secondary to any phase of the retinopathy,small focal laser spots areapplied todiscrete areasof leakage.

60
Lowpowerlaserspotsmaybeappliedinagridpatterntoareasofdiffuseleakage.Lasertreatmentfordiabeticretinopathyisoneofthesafestandmost effective treatments inmedicine. It doesnot improve thevision,andthebestitcandoispreservetheexistingvision.Oneofthesideeffectsofextensivelasertreatmentisdecreasednightvision.Without laser treatment, a person with severe proliferativediabeticretinopathywilleventuallygoblind.Inthe21stcentury,withlasertreatmentreadilyavailableinmostcountries,thereisnoreasonwhyapersonwithdiabetesshouldgoblind.Every diabetic patient should be educated about the disease’scomplications,especiallythoserelatingtotheeye.Dependingonthe duration and severity of the diabetes, or if diabeticretinopathy is already present, the patient should have eyeexaminationsatregularintervals,suchasonceayear.Thepatientshouldseeanophthalmologistifthereisanysuddenchange in vision, such as distortion in the central vision orsuddenonsetoffloaters.

61
Pan‐retinal laser photocoagulation (PRP) for treatment ofproliferativediabeticretinopathy(PDR)
Each spot is a laser burn. This area of the retina has beendestroyed and no longer requires oxygen, thus alleviating thehypoxiccondition.Nonewbloodvesselswillgrowaftersuchatreatment.Theareaaroundthemaculaisspared.Withthisareaintact,thereading vision will remain the same. Night vision may bedecreasedafteranextensivetreatment.
MACULARDEGENERATIONAMD or age‐relatedmacular degeneration is grouped into dryand wet forms. AMD is the main cause of loss of vision inpatientsover50yearsoldintheUSandWesternEurope.Itisadisease mainly found in light‐complexioned persons andsometimes can be inherited. But the pattern of inheritance israrelyproven.

62
DryAMDDrusen(yellowdepositsdeep in theretina)andatrophyof theRPE(retinalpigmentepithelium)areassociatedwith this formof AMD. It can cause loss of vision if the atrophy involves thecenterofthemacula.The Age‐Related Eye Disease Study (AREDS) showed thatpatientswith dry AMD could reduce the risk of visual loss bytakinghighdosesofvitaminsandzinc.Commerciallypreparedcombinations of vitamins and minerals for this purpose areavailable.WetAMDIn this condition, the retina and RPE are detached from theunderlyingstructuresbyserousfluid.ThespaceundertheRPEisinvadedbyabnormalbloodvesselsfromthechoroidformingthe choroidal neovascular membrane (CNV), which can bleed.These hemorrhages eventually form fibrovascular diskiformscars,whichareofteninthemaculararea,leadingtoseverelossofvision.

63
AfluoresceinangiogramshowingaCNV(choroidalneovascularmembrane)inthemacula.
A fluorescein angiography is done by injecting the fluorescentdye into thebloodstream,highlighting thebloodvessels in thebackoftheeyesotheycanbephotographed.Patientswith either form of AMD should be instructed to testtheirowneyeswiththeAmslergrid.Ifanydistortionofthelinesis noted, the patient should see a retina specialist as soon aspossible.TreatmentofWetAMDUntil theearly2000s, therewasnoeffective treatment forwetAMD, i.e., the CNV that causes the damage. For the occasionalCNVs that are not inside themacula, wewould try to destroythem with laser treatment. But they often returned andeventuallyextendedintothemacula.Nowwehaveanewclassofdrugcalledanti‐VEGFthatcanblockthechemicalthatcausesthe CNV to form in the first place, preventing further loss ofvision.

64
Anti‐VEGFTherapyVEGFstimulatestheformationofCNV,andbyblockingtheeffectof this protein, it is prevented from further stimulating thegrowthofCNV.There are several anti‐VEGF drugs on the market. Lucentis(ranibizumab) is the first to be approved by the FDA for thetreatmentofwetmaculardegeneration.The drug is injected directly into the vitreous, which thendiffusesthroughouttheretinaandchoroid.Bybindingstronglyto the VEGF proteins, it prevents further growth of unwantedbloodvessels.Ithasbeentoutedasthemiracledrugformaculardegeneration because, for so long, there was essentially notreatment. For the majority of patients, the drug stops thedisease from progressing. In some patients, there is actually asmall gain of vision. This treatment is time consuming, as theinjection has to be done almost monthly. It is also expensive,eachdosecostingabout$2,000.Avastin (bevacizumab) was developed for the treatment ofmetastatic colon cancer. It has a similar but larger molecularstructurethanLucentis.Thetwodrugsaremanufacturedbythesamecompany.AvastinhasbeenwidelyusedforthetreatmentofwetAMDbymanyophthalmologists in theUS, even thoughtheFDAhasnotapprovedittodate. IthasbeendeterminedtobejustaseffectiveandsafeasLucentis.Thecostofeachdoseofthisdrugisabout$50,i.e.,2.5%ofthepriceofLucentis.So why do ophthalmologists still use Lucentis? This is a hotlydebated,complicated issue.Thoseofyouwhoare interestedmaygetontheInternetforfurtherreading.

65
FLASHESANDFLOATERSWhenwe are young, the vitreous is a clear jell‐like substancewithmillionsoffinefibers.Aswegetolder,itshrinks,andpartof it becomes liquefied, causing a posterior vitreousdetachment.Thetuggingofthevitreouswhereitisattachedtothe retina causes the brain to interpret this as flashes of light.This process also causes the formation of strands and stringsappearing as spots, small circlesor fine threads floating insidetheeye.Mostofthetime,thereisnorealthreattothevisionandthe patient will learn to live with these floaters. If they aresevereenough,someretinalspecialistsmightrecommendtheirremovalwithvitrectomy(surgicalremovalofthevitreous).Thisformoftreatmentiscontroversialandisnotgenerallyacceptedasstandardprocedure.
RETINALTEARInsomeareas,thevitreousmaybeverystronglyattachedtotheretina. If these areas happen to containweak or thin retina, apieceof it canbe tornoff. If there is a bloodvessel across thetear,bleedingmayoccur.Thisiscalledavitreoushemorrhage.Ifthereisagreatdealofhemorrhage,itmayreducethevision.Ifaretinaltearoccurs, itcanbeaseriousproblem,asitcangoon to a retinal detachment. A retinal tear can be treatedwithlaser photocoagulation or cryo therapy. The area treated willformascararoundthetear,whichwillpreventtheretinafromdetaching.

66
This is a so‐called “horseshoe” tear because it is shaped like ahorseshoe.Thepatientsitsinfrontoftheslitlamp.Aspecialcontactlensisplacedonthecornea.Thelaserisappliedaroundtheedgesofthetearintwoorthreerows.A firm adhesion forms around the tear, preventing a detachedretina.

67
Thesameretinaltearcanalsobetreatedbycryotherapy.Under direct visualization, the cryo probe is placed under theareaoftheretinaltear.Aniceballforms,freezingtheareaaroundthetear,creatinganadhesion and preventing the tear from becoming a detachedretina.
RETINALDETACHMENTWhen fluid collects in thepotential spacebetween thesensoryretinaandRPE,itbecomesadetachedretina.Thereareseveraltypes of retinal detachment. Here we will only discuss therhegmatogenous type, which is invariably caused by a retinalholeortear(break)intheretina.This type of retinal detachment occurs more frequently inpeople with myopia or after trauma, such as in the case ofboxers.

68
Thesymptomwouldbelossofsidevision,whichmanypatientsdescribe as a curtain. If themacula is also detached, then thecentralvisionwouldbelostaswell.Ifthedetachedretinahasalargeamountoffluidunderneathit,itwouldberecognizablebyitsmarkedelevation.Thedetachedretina appears opaque andmayundulate. It is very difficult toexamine a detached retina with a handheld ophthalmoscope.Ophthalmologists use the indirect ophthalmoscope, whichprovidesstereopsisandanentire360‐degreeviewoftheretinaincludingtheextremeperiphery,whichistheusuallocationofaretinal hole or tear. The first thing in the repair of a detachedretinaistofindthehole(s)ortear(s),whichhavetobesealedinordertohaveasuccessfuloutcome.RepairofRetinalDetachmentUntil about two decades ago, the usual treatment for retinaldetachment was the scleral buckling procedure. As thetechnology for vitrectomy improves, become less invasive andinvolves fewer complications, most detached retina surgeriesdoneintheUSnowusethevitrectomymethod.Thescleralbucklingprocedureisstillveryuseful,especiallyindeveloping countries where the very expensive vitrectomymachine is not available. I have done scleral bucklingproceduresinseveraldevelopingcountrieswithsuppliesthat Ibroughtwithme.TheonlyadditionalsupplyIneededwasatankof gas (carbon dioxide or nitrous oxide are available in mostdevelopingcountries)fortheportablecryomachine.Aportablelaser(whichIoftenbringalongaswell)canalsobeusedtotreattheretinaltear.A piece of silicone sponge is sutured onto the sclera over theareaoftheretinaltear.Thiscreatesanindentation,pushingthechoroidagainsttheretinaatthelocationofthetear.Thetearis

69
then treated with cryo therapy to cause an inflammation thatencouragesanadhesiontoformbetweentheretinaandchoroid.Depending on the size and location of the retinal tear, thesilicone sponge canbe trimmed to fit the size requirements oftheareatobetreated.
Pneumaticretinopexyisusedinselectcaseswheretheretinaldetachment is limited and the tear is in a superior location. Inthesecases,agasbubbleisinjectedintothevitreouscavity.Thepatient is then positioned so that the gas pushes the retinaaround the break, creating a tamponade and sealing the tear.The area around the tear is then treatedwith cyro therapy orlaser. After 1 to 2weeks, the special gas,which is usually SF6(sulfurhexafluoride), is resorbedanddisappears from theeye.Bythen,achorioretinaladhesionwouldhaveformedtokeeptheretinaattached.
All retinal breaks are localized and treatedwith cryotherapy.Asiliconespongeisthensuturedtothesclera,makinganindentationthatpushesthechoroidagainsttheretina.Thefluidunderneaththeretinaisresorbedby the RPE. The area treated with the cryo therapyformsachorioretinaladhesion.

70
In vitrectomy, the vitreous pulling on the retinal break isremoved. A gas bubble is usually injected to push the retinaaround the break against the choroid. In more complicateddetached retinas, more extensive surgery such as removal ofscartissueontheretinamaybeneeded.A vitrectomy is performed under microscopic control byinserting tiny instruments (25 or 27 gauge) through the parsplanaoftheeye.Thisisanareaofthesclerabehindthelimbusand is usually avascular. Visualization inside the eye is madepossible with fiber‐optic illumination. Instruments that canperform vitreous cutting and aspiration and tiny scissors areused.Atinyfiber‐opticprobeattachedtoalasermachinecanbeinserted into the eye for laser photocoagulation during thesurgeryunderdirectvisualization.Vitrectomy is used for other indications such as non‐resolvingvitreoushemorrhageandpenetratinginjuriestotheeyeball.
OCCLUSIONSCentralRetinalArteryOcclusion(CRAO)—alsoincludedintheneuro‐ophthalmologychapter.CRAOismanifestedasasuddenlossofvision.Prolonged(over45 minutes) interruption of retinal arterial blood flow causespermanentdamageto theganglionandothercells, resulting inpermanent loss of vision. The typical feature is a so‐called“cherry‐redspot.”

71
BranchRetinalArteryOcclusion(BRAO)Whenonlyabranchofthecentralretinalarteryisinvolved,thearea of the retina supplied by this branch becomes ischemicwithacorrespondinglossofvisioninthevisualfield.CentralRetinalVeinOcclusion(CRVO)The fundus picture of CRVO is dramatic, with acutehemorrhages and disc swelling, the so‐called “blood andthunder” picture. Visual loss is usually not acute and thecondition is not an emergency; there is generally no acceptedacute management. The hemorrhages and disc swelling mayimprovewithtime,alongwithimprovementofthevision.This condition is most often found in older people withhypertension and arteriosclerotic vascular disease. Carotidarteryocclusionmayproducesimilarbutlessseverefindings.NeovascularglaucomacanbealatecomplicationofCRVO.Laserphotocoagulationcanpreventthiscomplication.BranchRetinalVeinOcclusion(BRVO)Obstructionofoutflowcancauseretinalveinocclusion,whichinturn causes edema, abnormal leakage and hemorrhage to theareaoftheretinainvolved.Prolonged obstruction can cause ischemia, which in turn canlead to the growth of neovascularization. Again,neovascularization, if allowed to proliferate untreated (withlaser photocoagulation), can lead to vitreous hemorrhage andtractionretinaldetachment.


CHAPTER 8: UVEITIS
Theuveal tract includes the iris, ciliarybody and choroid.Theprimaryfunctionof theuveal tract is tosupplynourishmenttotheocularstructures.Uveitisisageneraltermforinflammationoftheuvealtract,i.e.,iritis, cyclitis (inflammation of the ciliary body), irido‐cyclitisandchoroiditis.Uveitisisadifficultareaevenforophthalmologists,becauseitisnoteasy topinpoint the cause, andoftenextensive studies arerequired. Frequently, the adjacent structures such as retina,sclera and cornea are also involved secondary to theinflammatoryprocess.

74
Uveitis is divided into 3 types: anterior, intermediate andposterior.Inthisbook,wewillconcentratemainlyontheanteriorvariety,as it is themost common and can be treated atmostmedicalclinics.SymptomsofUveitis:
Redness Pain Photophobia Tearing Visualdisturbance Floaters
Anterioruveitis can be acute or chronic. Blunt trauma to theeyeball can cause anterior uveitis with acute onset of pain,hyperemia, photophobia andblurry vision.Thepupil ismiotic.Flare (a foggy appearance) and cells (WBCs) are found in theanterior chamber, which can only be seen with the slit lampunderhighmagnification.SomeCausesofAnteriorUveitis:
Idiopathic Traumatic Juvenilerheumatoidarthritis Sarcoidosis Syphilis AIDS Tuberculosis
Treatment is corticosteroid drops (for the inflammation) anddilationof thepupilwithacycloplegicdrop torelax theciliarymuscle. Corticosteroids should be used with great cautionbecause of their serious side effects. If the condition is not

75
resolved in less than aweek, the patient should be sent to anophthalmologist.Somediseasesinvolvemorethanonesegment.SomeCausesofIntermediateUveitis:
Idiopathic Lymedisease Sarcoidosis Multiplesclerosis Juvenilerheumatoidarthritis
SomeCausesofPosteriorUveitis:
Idiopathic Toxoplasmosis Sarcoidosis AIDS Candidiasis
SomeCausesofPanuveitis(involvingtheentireuvealtract):
Idiopathic Sarcoidosis Vogt‐Koyanagi‐Harada Behcetsyndrome
Panuveitis tends to be a chronic disease with a fair to poorprognosis.Except formild anterioruveitis, patients shouldbe referred toanophthalmologist.Thiscanbeablindingdisease.

76
The lists of causes are far from complete, as I have chosen toinclude only diseases that primary care practitioners aregenerallyfamiliarwith.Treatmentofsevereuveitisisbeyondthescopeofthisbook.

CHAPTER 9: GLAUCOMA Glaucomaisagroupofdiseasesthatdamagestheopticnerve.Atits simplest and most useful for the purposes of this book,glaucoma is a condition in which the optic nerve has beendamagedbyelevatedintraocularpressure.Thenormalrangeof IOP(intraocularpressure) isbetween10‐21mmHg. In some eyes, damage can occurwithin this range.Whenthathappens,itiscalled“lowtension”or“normotensive”glaucoma.AnIOPofover21mmHgdoesnotalwaysmeanthatthenervewillbedamaged.Theanteriorchamberoftheeyecontainsaqueousfluid,whichisconstantly produced by the ciliary body. In a healthy eye(below), the fluid drains out of the eyeball through thetrabecular meshwork located at the periphery of the anteriorchamberjustanteriortotheiris.

78
The “angle” discussed in glaucoma diagnoses consists of thebase of the iris, the trabecular meshwork and the supportingscleralandcornealtissue.Iftheproductionofthefluidexceedstheoutflow,theIOPrises.PRIMARYOPEN‐ANGLEGLAUCOMAThis is the most common type of glaucoma, usually found inolderpeople.Aspeopleage,thetrabecularmeshworkbecomesless efficient and IOP builds up.As its name implies, the anglebetween the base of the iris, trabecular meshwork and thesupporting scleral and corneal tissue is open. It is usuallybilateral and may be inherited. Good central vision is usuallypreserved until late in the disease, which makes this type ofglaucomaverydangerous,as it is initiallyasymptomaticunlessvisualfieldtestingisdone.Patients with advanced glaucoma may have difficulty gettingaroundbecauseoftheconstrictedvisualfield.Examinationoftheopticnervemayrevealenlargedcuppinganditscolorcanappearlesspinkthannormal.THEOPTICNERVE
The healthyopticnerve ispinkish in color. Thecenter of the optic nerve(physiologic optic cup) orthe cup/disc ratio isusually30%or lessof thediameteroftheopticdisc.

79
For a patient with a cup/disc ratio of 0.9, the visual field isusuallyseverelyconstricted.Therearevariousvisualfieldmachines,someofwhichareverysensitive,thatcandetectearlylossofperipheralvision.
Thecup/discratiohereis0.6.The pinkish nerve tissue,especially on the temporalsideof theopticdisc,maybedamagedandthin.Glaucomaissuspected.Thecup/discratiois0.9here.The optic cup becomeswhitish and deeper. Tinyhemorrhages may appear ontheopticdisc.

80
VISUALFIELDS
Thisisanormalvisualfield.Cup/discratiois0.3.Field shows enlarged blind spotand superior nasal scotoma. Inglaucoma, the cup usuallyenlargesmorevertically.Cup/disc ratio is 0.5 horizontallyand0.6vertically.Field shows constriction ofsuperior nasal field. There isthinningoftherimofthecup.Cup/discratiois0.8.Field shows further superiorconstriction and new inferiordefect. Cup/disc ratio is 0.9withadvancedgeneralized thinningoftherim.Field shows small central andtemporal island of visionremaining.Theopticnerveispalewithadeepcupandtotalatrophyoftherim.

81
CROSS‐CONFRONTATIONVISUALFIELDTESTING
1. Sitfacingthepatient,about3feetaway.2. Coverthepatient’slefteyewithapatch.3. Havethepatient’srighteyevisuallyfixonyournose.4. Test the right eye by holding your left hand outside of
the patient’s visual field. Slowlymove your hand (withan arbitrary number of fingers) from the patient’stemporal side. Ask the patient to tell youwhen he/shecanfirstcountthenumberoffingers.Repeatthisstepforthesuperior temporaland inferior temporalquadrants.Switchhandsandcheck thesuperiornasaland inferiornasalquadrants.Mapyour findingsontoa roughvisualfieldchart.
5. Covertherighteyeandtesttheleft.This visual field test can also be used for patients withneurologicalproblemssuchaspituitaryglandtumor.
MEDICALTREATMENTThegoalofglaucomatreatmentistopreventfurtherdamagetothe optic nerve and retina. The desired IOP may vary frompatient to patient. Medical treatment is usually life long andrequiresthediligenceandcooperationofthepatient.MedicationsCholinergic‐stimulatingdrugs:Miotics help to drain the aqueous through the trabecularmeshwork more rapidly. Pilocarpine 1% to 6%, one droptopically every 6 hours, may be prescribed. Pilocarpine gel isalsoavailable.

82
Becauseofitssideeffectsandtheavailabilityofbetterdrugs,itisnolongeracommondrugforthetreatmentofprimaryopen‐angle glaucoma. Its side effects include blurry vision, frontalheadaches,andsometimesnausea.Betablockers(beta‐adrenergicblockingagents):These reduce the IOP by reducing aqueous production by theciliary body. Timoptic (timolol maleate) was the first betablockertobeapprovedfortreatmentofglaucoma.Itisusuallyusedtwiceaday.Onedailydoseiseffectivefor70%ofpatients.Beta‐blockersareusuallyexcellentforloweringIOP.Patientswithasthma,chroniclungdiseaseandcongestiveheartfailureshouldnotusethisgroupofmedication.Otherbeta‐blockers:Betagan,Betoptic‐S,Optipranolol,Ocupress.Prostaglandininhibitors:Xalatan(Latanoprost),aprostaglandininhibitor,lowerstheIOPbyincreasingtheaqueousfluidoutflowbyapathwayotherthanthemeshwork.Itisveryexpensiveandrequiresrefrigeration.Otherprostaglandininhibitors:Lumigan,Travatan,Rescula.Alpha‐adrenergicagonists:These drugs lower the IOP by decreasing the aqueousproduction. They are: Iopidine (apraclonidine) and Alphagan(brimonidine).Adrenergicstimulatingdrugs:EpinephrinehydrochlorideandPropine(dipivefrin).Carbonicanhydraseinhibitors:Diamox(Acetazolamide) lowerstheIOPbydecreasingaqueousproductionbytheciliarybody.Itiswidelyavailableinoralform,250mg every 6 hours or 500mg sequel every 12 hours. It is

83
rarelyused for the treatmentof chronicglaucoma inoral formbecause of the side effects, which include kidney stones, bodychemistry disturbance (loss of potassium), gastrointestinalupsets,lossofappetiteandweightloss.Othercarbonicanhydraseinhibitors:Neptazane(methazolamide)andDaranide(dichlorphenamide).Topicalcarbonicanhydraseinhibitors:Trusopt(dorzolamide)andAzopt(brinzolamide).Combinationdrops:Cosopt=(timolol+dorzolamide)Combigan=(timolol+brimonidine)Hyperosmotics:Glycerin(glycerol)maybegivenorallytodehydratethevitreousand lower the IOP. Mannitol and urea are intravenoushyperosmotics. These agents are usually used in a hospitalsetting.
SURGICALMANAGEMENTWhen medical or laser treatments fail, or when they becomeimpractical,surgeryshouldbeconsidered.In the UK, surgery is often undertaken early in glaucomatreatmentinsteadofcommittingthepatienttoalifeofdrugsthatcanbe inconvenientandexpensive.IntheUS,possiblybecauseoffearoflawsuits,surgeryisonlyofferedasaverylastresort.LaserTrabeculoplastyUsing a high‐intensity beam of light (laser), several evenlyspaced tiny burns are made in the trabecular meshwork,allowing the aqueous to drain better, lowering the pressure.

84
Only topical anesthesia is needed for this usually painlessprocedure,whichtakesabout15minutes.ThedropinIOPisnottypicallyverygreataftersuchaprocedure,andthepatientmaystillneedtousemedicateddrops.TrabeculectomyThis is the most common external filtration surgery. A tinysectionof the scleraand trabecularmeshworkat the limbus isremoved. The opening is then covered with a loosely suturedscleralflap,andtheareaisrecoveredwiththeconjunctiva.Theaqueous flows through the fistula under the conjunctiva,creating a bleb. If the surgery works well, the IOP becomesnormal because of the constant flow of aqueous leaving theeyeball.ThisprocedureisnotdonemorefrequentlyintheUSbecauseofpotential complications such aswound leakage and prolongedlow IOP. The most dreaded complication is infection(endophthalmitis).

85
Trabeculectomy
A tiny block of sclera and trabecular meshwork is
removed. The opening is covered with a loosely sutured scleral
flap. Aqueousflowsthroughafistula. A bleb (small rounded mound) is created under the
conjunctiva. A constant amount of aqueous leaves the eye,
normalizingtheIOP.

86
PRIMARYANGLE‐CLOSUREGLAUCOMAWhen the iris suddenly blocks the trabecular meshwork,interruptingtheoutflowofaqueous,itcausesamarkedincreasein the IOP, which can cause pain and decrease vision. It isusually bilateral, but acute attacks of angle‐closure do nottypicallyoccuratthesametime.Thisconditionismostcommonamong Asians, because of their typically smaller eyes (i.e.,narrower angle), and uncommon in people of African descent,becausetheyoftenhavelargereyes(i.e.,widerangle).
The iris is up against the angle, blocking the trabecularmeshwork, stopping the aqueous fluid from leaving theeye. ThesuddenriseofIOPcancausepain,lossofvisionandcoloredringsorhalosaroundlights.Thepaincanbeverysevere.ThelossofvisionissecondarytothecornealedemafromthehighIOP.

87
The IOPmay be as high as 50 to 60mmHg. Palpation of theeyeballovertheuppereyelidwillfeelfirm.Inanacuteattack,medical therapyshouldbe initiatedas soonas possible because the elevated IOP can cause permanentdamagetotheopticnerve.MedicalTreatmentofAcuteAngleClosure
1. Pilocarpine 4% drop every half hour until the pupilconstricts.
2. Beta‐blocker such as Timolol Maleate 0.5%, one dropevery 10 minutes until the IOP is lowered to anacceptablelevel.
3. Diamox500mgorally.4. Glycerin50%solutiongivenorally,1.5gperkgofbody
weight.LaserIridotomyorSurgicalIridectomyOnce the IOP and inflammation have been brought undercontrol,andthecorneaisclear,alaseriridotomyshouldbedoneas soonaspossible.Laser iridotomy (using the laser toburnaholeintheiris)canbedoneintheofficeandismuchsaferthansurgical iridectomy. Eitheranargon laserorNd:YAG lasercanbeusedtomakethisopening.Surgical iridectomy (surgical removal of a tiny piece ofperipheral irisnear theangle)maybeneeded if the iridotomykeeps closingoff orwhen the laser isnot available. It involvescutting into theeyeandcarries therisksandcomplicationofadelicatesurgery.

88
Creating an opening in the peripheral iris allows the aqueousfluid to flow from the posterior chamber to the anteriorchamber.Thiswill keep the iris frombulging forward toblockoffthetrabecularmeshwork.The unaffected eye will generally benefit from a prophylacticlaser iridotomy or surgical iridectomy; otherwise, it will be amatteroftimebeforeitsuffersanangle‐closureattackaswell.
SECONDARYGLAUCOMASystemic diseases such as diabetes can cause the dreadedneovascularglaucoma,whichcanbeverypainfulandcanleadtoblindness.Advancedcataractoradislocated lenscancause the IOP togoup.Uveitis(inflammationinsidetheeye)cancauseanacuteriseinIOP.

89
InjurytotheeyecancausetheIOPtogoupindifferentways.
GLAUCOMAINDEVELOPINGCOUNTRIESIf a patient in a developing country has chronic glaucoma, itwould be difficult for him or her to shoulder the cost of alifetime of medication and the follow‐up needed for such acondition. The patient may live far away from any medicalfacility, and may not understand the natural history of thedisease.Glaucomaisadifficultdiseasetomanagewhentryingtomakealiving is a problem. Early surgery would be recommended.Otherwise, thesepatientswillalmostcertainlygoblind,as it isunlikely that they will consistently follow the daily routine ofapplyingthenecessaryeyedrop(s).


CHAPTER 10: NEURO-OPHTHALMOLOGY The process of human vision is incredibly complex. There aretwo main components: the eye, which is responsible forcollecting information, and the brain, which is responsible forinterpretingit.Theeyeislikeacamera,andallthepartshavetobeingoodconditionforaclearimagetoformontheretina. Ifanypartoftheeye,suchasthecornea,thelens,thevitreousortheretina,isnotperfect,thenaclearimagecannotbeobtained.The image captured by the retina is converted toelectrochemicalsignals,whichare thensentalongtheaxonsofthe ganglion cells in the retina. The ganglion cells all meet toformtheopticnerve,whichisalsoknownastheopticdisc.Please refer to the Visual‐Sensory System and Visual Pathwaydiagramsonpages93‐94.Fibersfromthemaculaenterthetemporalsideoftheopticdisc.Afterperforatingthesclera,theopticnervefiberspassdirectlytotheopticchiasm.Fibers from the nasal halves of each retina cross to the otherside.Opticfibersfromthetemporalhalvesofeachretinamovetowardthechiasm, leavingitwithoutcrossing.Theopticfibersbehind the chiasm form the optic tract, which goes to thegeniculatebody(therightandleft)ofthethalamus.Thefibersinfrontofthechiasmarecalledtheopticnervesandthosebehindaretheoptictracts.

92
Thevisualsensoryinformationissenttotheoccipitallobe(thevisual cortex) to be interpreted. From the visual cortex, thevisualsensoryinformationissimultaneouslysenttothe“what”and “where” pathways, which are located primarily in thetemporallobeandparietallobe,respectively.The “what” pathway is a pattern recognition center,whichwedevelopfromthetimewearebabies,learningforms,shapesandfaces in our surroundings. Initially, babiesmake little sense oftheworldaroundthem,butgraduallytheybecomefamiliarwiththeirenvironments.ThebookTheManWhoMistookHisWife for a Hat isaboutamanwhohastroublerecognizinghisstudentsuntiltheyspeaktohim.This isanexampleofbraindamage in the“what”pathway,wherebyheisno longerabletorecognizeobjectsthatusedtobefamiliartohim.The“where”pathway, locatedintheparietal lobe, iswherethevisual stimuli are judged against their relationship with otherobjects three‐dimensionally, giving the viewer the object’sspatiallocation.Thesetwopathwaysworksimultaneouslytoprocessthevisualsensory information so thatwe knowwhatwe are seeing andalsoknowitsexactlocation,whichisessentialforoursurvival.

93
THEVISUAL–SENSORYSYSTEM
Theleftcerebralhemispherehasbeenremoved.Note the relationshipof theopticnerve to the internal carotidandanteriorcommunicatingarteries.Notethelocationoftheparietallobe(the“where”pathway).Thetemporal lobe (the “what” pathway) is not displayed here inorder to show the structures between the two cerebralhemispheres.

94
THEVISUALPATHWAYHerearesomeexamplesofhowthingscangowrongwhenanypartofthevisualpathwayisinterrupted.
1. Iftherightopticnerveisdamaged,suchasseveredinaninjury, the eye becomes blind. The nerve can also bedamagedbystrokeoratumor.
2. In the case of a pituitary gland tumor orcraniopharyngiomanearthemidlinebehindthechiasm,the decussating fibers of the optic nerve are damagedandthevisualimpulsesofthenasalhalvesofeachretinaare blocked, resulting in a bitemporal hemianopia.(Thelefteyedoesnotperceiveimagesinthelefthalfof

95
its visual field, and the right eye does not perceiveimagesintherighthalfofitsvisualfield.)
3. Iftherightoptictractweredestroyed,itwouldresultinlossof function in therighthalvesofbothretinas,withcorresponding blindness in the left half of each visualfield.Thisiscalledlefthomonymoushemianopia.
CorticalBlindnessThisisanextremelyrareconditioninwhichextensivebilateraldamagehasbeendonetothecerebralvisualpathwaysresultingin complete loss of vision. Patients with this condition havenormal pupillary reactions because of the different pathwaysserving the pupillary light reflex and those carrying visualinformation.Examinationofthefundusisnormal.Aneurysm
TheopticchiasmalieswithinthecircleofWillis.

96
Aneurysms commonly arise from this arterial circle and causefielddefectsbycompressing theopticnerves,opticchiasmaoroptictracts.Tumor
Thepituitaryglandsitsbehindtheopticchiasma.Atumormaycause ischemia by squeezing small nutrient arteries, or edemaandcongestionbyconstrictingtheveins.There are numerous other examples of visual field defects.Sometimes when the destruction of the tissue is incomplete,patientscanhaveunusualvisualfields.

97
BeforeMRIandCTscanswerecommonplaceandaccurate, theclinician often had to depend on the visual fields and otherneurological findings to localize a lesion. Some neuro‐ophthalmologists became very famous because they were sogoodatlocalizingthelesions.Fewer ophthalmologists now go into the field of neuro‐ophthalmologybecausesuchexpertiseisnotascrucialasitusedtobe, asmachines candoanexcellent job localizing lesions inthebrainandaroundtheeye.
DIPLOPIA (Also read thepediatric chapteron the treatmentofdiplopia.)Diplopia, or double vision, is a common complaint in medicalpracticeandmaybemonocularorbinocular.Binocular double vision occurs when the images of the twoeyesdonotcoincidesothattheimagesproducedaremisalignedrelativetooneanother. Itdisappearswhenoneeye iscovered.Cranialnervepalsiesarethemostcommoncause,withmanyofthese cases brought on by diabetes mellitus and/orhypertension.Monoculardoublevisionisuncommon.Itaffectsoneeyeonlyandcanbecausedbyabnormalitiesofthelens,corneaorretina,resultinginsplittingoftheimage.Muscle disorders that can be accompanied by double visioninclude myasthenia gravis, Graves’ disease and myotonicdystrophy.Nerveproblemsassociatedwithdiplopiaincludeconditionsthataffect the cranial nerves #3, #4 and #6 controlling the eye

98
muscles. These conditions include diabetes mellitus,hypertension, multiple sclerosis and Guillain‐Barre syndrome,withthefirsttwobeingthemostcommon.Brainproblemsthatcanbringondoublevisionincludevascularconditionssuchasstrokesoraneurysms,oratumorintheorbitorskull.Raisedintracranialpressurecanaffectcranialnerve#6(abducent)asithasthelongestintracranialcourse.Itmayalsobe a side effect of some drugs such as ketamine, opioids andphenytoin.
STRABISMUSInmedicalschool,IusedtheformulaLR6SO4torememberhowthesixexternalocularmusclesareinnervated.The lateral rectus is supplied by nerve #6 (abducent), i.e.abduction(causingtheeyetoturnout),whichisrepresentedbyLR6.Thesuperiorobliqueissuppliedbynerve#4(trochlear)whichisrepresentedbySO4.The other four external muscles (the superior rectus, inferiorrectus,medialrectusandinferioroblique),theinternalmusclesandtheeyelidaresuppliedbythenerve#3(oculomotor).By remembering just #6 and #4, i.e., LR6SO4, I knew that therestareinnervatedbynerve#3.The four rectimusclespulldirectlyon theeyeball so that theymove in thedirectionof theirnames: superior, inferior, lateralandmedial.

99
Theobliquemusclesmove theeyeoutwardsaswellasupanddown.Eachmusclehooksarounda“pulley”sothatitmovestheeye the opposite direction to which its name implies. Thesuperior oblique muscle moves the eye down and out. Theinferiorobliquemusclemovesitupandout.Paralysisofamusclemeansthattheeyedoesnotmovefullyinthedirectioninwhichitpulls.Theeyethereforedeviatesintheoppositedirectionfromthepulloftheaffectedmuscles.
PrimarypositionCorneal light reflex is centrally (symmetrically) locatedineacheye.
Leftesotropia, i.e.,thelefteyeisturnedinward.Thisisbecause the left lateral rectus is weak and the eye ispulledinbythemedialrectus.Cranialnerve#6oftheleftside is affected. The most common cause of 6th nervepalsyisdiabetesmellitus.Becauseofitslongcourse,the6thnervepalsyhasnolocalizingvalue.Whichgazemakesthediplopiaworse?

100
Leftexotropia,i.e.,thelefteyeisturnedoutward.Themedialrectusisweakandtheeyeispulledoutbythelateral rectus. The medial rectus is innervated by abranchofcranialnerve#3.Ifthepupilisnotinvolved,it is likely to be of vascular origin such as diabetes,ratherthanaspaceoccupyinglesioninthebrain.Whichgazemakesthediplopiaworse?
Lefthypertropia,i.e.,thelefteyeisturnedupward.Theinferiorrectusisweakandtheeyeispulledupwardbythesuperiorrectus.Theinferiorrectusisinnervatedbya branch of the cranial nerve #3. If the pupil is notinvolved,thistooismostlikelyvascularinorigin.Whichgazemakesthediplopiaworse?

101
If theleft lateralrectusisparalyzeditcannotabduct, i.e.,movetheeyehorizontallyawayfromthenose.The left medial rectus contracts unopposed and adductionoccurs, i.e., the eye moves horizontally toward the nose,resulting in left esotropia as shown in the second drawing onpage99.Cranial nerve #3, with itsmany branches, is a very importantnerve and should be discussed further here. The intrinsic eyemusclesareinnervatedbytheautonomicsystemsandincludetheiris sphincter (constriction of the pupil) and the ciliarymuscle(controls the accommodation of the lens), which are bothinnervated by the parasympathetic component of cranial nerve#3. The radial pupillodilatormuscles (dilation of the pupil) areinnervated by the ascending cervical sympathetic system. Thisinformation will be useful at the end of the chapter whenneurologicalpupildisordersarediscussed.

102
Since thischapter isonneuro‐ophthalmology, Iwould like togooverwhatshouldbeincludedinsuchanexamination.Muchoftheneuro‐ophthalmologyexaminationistoevaluatecranialnerve#3.Examination/Signs:
Check for ptosis (drooping eyelid) to identify theaffected side. Eyelid elevation is partly controlled bycranialnerve#3(oculomotornerve).
Check the pupils to see if both are equal and react tolight.Thepupilisalsocontrolledbycranialnerve#3.
Pupil abnormalities may indicate the problem isintracranial.
Checktheopticnerveforpapilledema. Identify which eye is affected and which direction of
gazeislimited.FourthNerve(SuperiorOblique)Palsyisrare.Symptoms include binocular vertical or oblique diplopia,difficultyreadingandasensationthatobjectsappeartilted.Ifitismild,itmaybeasymptomatic.It is difficult to evaluate fourth nerve palsy and the list ofdifferentialdiagnosesislong.SixthNerve(Abducens)PalsyThe intracranial course of the abducens nerve (#6) is long,whichmeansthatitispronetodamageatmanysites.Therefore,it has minimal localizing value. Isolated #6 nerve palsy isrelativelycommon,especiallyinpatientswithdiabetes.Inchildren,secondarystrabismusmayfollowtraumatooneorboth eyes. Opacity of the media such as corneal scars orcataractscancausetheeye(s)ofachildtodeviate.Ascarinthemaculacanalsocausestrabismusinachild.

103
In adults, secondary strabismus may be due to cranial nervepalsyfromanyofthefollowing:
Braininjury Intracranialmasssuchasbraintumororabscess Stroke Diabetesmellitus Systemichypertension Heartdisease
Inpatientswithrecentonsetofstrabismus,aneurologistshouldbeconsulted.FifthNerve(Trigeminal)PalsyThis nerve transmits sensation from the eye, particularly painandtouchfromthecornea.Theblinkreflexpreventsthecorneafrombeingdamaged.Damagetothisnervemayresultincornealerosionsfromexposureanddrying.Herpes zoster may affect this nerve. When the ophthalmicdivision of the fifth nerve is involved, the patient develops atypicalherpeticvesicularrashaffectingtheeyelidsandforeheadtothemidline.SeventhNerve(Facial)PalsySymptoms: weakness or paralysis of one side of the face,excessivedroolingandinabilitytoclosetheeye.The most common cause is Bell’s palsy, which is idiopathic.Almost 90% of patients with Bell’s palsy recover completelywithobservationalonewithin2months.Other causesof facialnerve palsy should be ruled out. The list is long and includesneoplasm,stroke,infectionsandneurologicaldiseases.

104
Theprimaryocularcomplicationiscornealexposure,whichcanbe treatedwithartificial tears, lubricatingointmentand tapingoftheeyelids.PAPILLEDEMAThisisatermusedtodescribepassivediscswellingassociatedwithincreasedintracranialpressure. It isoftenusedtosuggesttheassociationofbraintumor.Thistermisintendedtopreventcommunicativeconfusionwhenotherformsofdiscswellingareconsidered.Someothercausesof“swollen”disc:Metabolic:proliferativeretinopathies,etc.Inflammatory:papillitis,neuroretinitisSystemicDisease:anemia,hypoxia,hypertensionVascular:ischemicneuropathy,cranialarteritisInfiltrative:lymphomaOcularDisease:uveitis,veinocclusionElevated Intracranial Pressure: mass lesion, pseudotumorcerebri,andhydrocephalus.ClinicalCharacteristicsofPapilledemaandOpticNeuritisPapilledema:
Novisualloss Noeyepain Alwaysbilateral Noabnormalityofpupil Normalvisualacuity Variabledegreeofdiscswellingandhemorrhages Visual prognosis is good after relief of intracranial
pressure

105
OpticNeuritis: Lossofcentralvision Tenderglobe,painonmotion Canbeinoneorbotheyes Diminishedlightreactiononsideofneuritis Variabledegreeofdiscswelling Visionusuallyreturnstonormalorfunctionallevels
GRADEIIIPAPILLEDEMA
Blurringofdiscmargin Hyperemiaofthedisc Obscurationofthewallofvesselscrossingdiscmargin Elevationofdisc Hemorrhagesonorneardisc SpontaneousvenouspulsationsinsomepatientsIdiopathicIntracranialHypertension(IIH):This condition is also known as Pseudotumor Cerebri. IIH is acondition of unknown cause characterized by elevatedcerebrospinal fluid (CSF) pressure and papilledema. It ismostcommonlyfoundinobesewomenofchildbearingage.

106
Themainsymptomsareheadache,transientvisualobscuration,blurredvisionandhorizontaldiplopia.VisuallosscausedbydiscswellingisthemajorpermanentsequelofIIH.Diagnosis is by elimination of other causes of elevated CSFpressure such as viral, bacterial and fungal infections, tumors,andinflammatoryormetabolicconditions.Use of vitamin A or multivitamins in high doses may beassociatedwiththiscondition.Treatment with a carbonic anhydrase inhibitor such asacetazolamide(Diamox)hasbeengenerallyeffective.
AMAUROSISFUGAXAmaurosis Fugax (fleeting darkness in Greek) is not anuncommon complaint in a primary care provider’s office. It isalwaysvascularinorigin.If thepartialblindness is transient, itmaybecausedbyretinalarteriolarspasm.Whentheblindnessispermanent,itiscausedbyblockageoftheretinalarteriesbycholesterolplaque.If the cholesterol plaque leads to Central Retinal ArteryOcclusion, examination will show a “cherry‐red spot” in thecenterofthemacula.Iftheproblemissystemic,itmaybeassociatedwith:
Carotidarterystenosis Malignanthypertension Patientswithlonghistoryofheavysmoking

107
Vascular insufficiency of the vertebral‐basilar arterialsystem
PrecedingacerebrovascularaccidentTreatment:Ifthelossofvisioniscausedbyablockageofthecentralretinalartery by a cholesterol embolus (Hollenhorst plaque), and theblockageislessthanhalfanhourinduration,thepatientshouldbeasked tobreathe intoabag, in thehope that increasing theconcentration of carbon dioxide in the bloodstreamwill causedilationofthearteryandallowtheembolustoflowawayfromthe center, thus sparing themacula (centralvision).Massagingthe eyemay also sometimesdislodge theplaque. If thesenon‐invasivemethods do notwork, then amore drastic proceduremaybeneeded.Paracentesis(removaloffluidfromtheanteriorchamberoftheeye—the space between the cornea and iris) is the last resort.This is done using a #30 gauge (short) needle attached to asmall plastic syringe. Only topical anesthesia is required. Aftergoingthroughthecornea,withdraw0.2mlofaqueousfluid.Thisshould be done under sterile conditions and with goodvisualizationwiththeloupeorslitlamp.Permanentblindnessoccursafter90minutesiftheplaqueisnotdislodged.Iamnotadvocatingthatprimarycareprovidersdoparacentesis.However,Ithinkitisimportanttobeawareofwhatprocedureisavailable in theunlikely event that theprimary careprovider ispresented a patientwith such a problem and no help iswithinreach. During my internship, I determined that should I bepresented with a patient who was dying from a subduralhematoma, and I was in a remote area without any surgeonnearby, I was willing to do a burr hole surgery to save thepatient’s life even though I was not a neurosurgeon. (I had

108
assisted in several such surgeries.) It is important toalwaysbeawareandprepared.
TEMPORALARTERITISAlso known as giant cell arteritis or cranial arteritis, temporalarteritisisasystemicvasculitisofunknowncausethatcanleadto blindness, stroke and death. It typically occurs in patientsaged60yearsorolder,andsymptomsincludepainonchewing,headache, temporal artery tenderness or scalp tenderness.Anorexia, weight loss, fever, malaise or depression may beassociated.ElevatedESRisassociatedwithmostcases.Diagnosisismadebypositivebiopsyofthetemporalartery,buta normal temporal artery biopsy does not rule it out. Ifuntreated, it can lead to blindness and death. This conditionshouldalwaysbeconsideredifanelderlypatientcomesinwithheadache and visual loss. Treatment is with large doses ofcorticosteroids.
MIGRAINEThethrobbingheadacheofamigraineisusuallyunilateral.It isoften associated with nausea and preceded by visualdisturbances and other symptoms. The visual aura is oftendescribedaswave‐likerippling,which isbelieved tobecausedby vasoconstriction followed by a phase of vasodilation. Theheadache phase is believed to be caused by the edema of thearterial wall. This conditionmust be distinguished from othermoreseriousconditionssuchasischemicattacks.Treatmentsincludepropranolol(abeta‐adrenergicblocker)andothermore standarddrugs such as antidepressants, analgesics

109
and sedatives. Use of ergot derivatives (vasoconstrictors) forprophylaxismustbedonewithgreatcaution,as itmayworsentheneurologicdeficit.Aserotoninagonist,Sumatriptan,actsasaselectcerebralvasoconstrictorandhasbeeneffectiveintreatingmigraine.
NEUROLOGICALPUPILDISORDERSHorner’sSyndromeThis rare syndrome results from an interruption of thesympatheticnervesupplytotheeyeandischaracterizedbytheclassic triad of miosis (constricted pupil), partial ptosis(droopingeyelid)andlossofhemi‐facialsweating(anhidrosis).Causesincludebrainstemstrokeortumor,tumororinfectionofthelungapex,andcarotidarteryischemia.Adie’sTonicPupilHere,theparasympathetic(constrictor)pathwayisdamagedonits way to the iris sphinctermuscles. The pupil is dilated anddoesnotconstricttolight.Thepupilwillconstrictslowlytonearvision. Unlike Horner’s Syndrome, the potential causes fordamage to the parasympathetic pathway are usually morebenignsuchasaviralinfection.ArgyllRobertsonPupilThis condition refers to a form of light‐near dissociation inwhich the pupils are small and respond poorly to light butpromptlytonearvisiontesting.Bothpupilsarealwaysinvolvedand respond poorly to dilating agents. This abnormality isprobablyduetoalesioninthelightreflexpathofthemidbrain.

110
It has been seen in patients with diabetes, but it is generallyassociated with neurosyphilis and workup for such should beinitiatedwiththepatient.Iamnotsuggestingthatthebusyprimarycareproviderevaluateevery abnormal pupil. It is important to be aware of suchabnormalities and take the entire clinical picture intoconsiderationastowhatshouldbedone.

CHAPTER 11: PEDIATRIC OPHTHALMOLOGY AND STRABISMUS Like many medical fields, the examination and treatment ofchildren is often more difficult than it is with adults. In somesituations,suchasacornealforeignbody,thechildmayneedtoberestrainedinordertoperformanadequateexaminationortoprovidethenecessarytreatment.EXAMINATION:Visualacuitytestingmayormaynotbenecessaryorpossible.Checkeyelidsforptosis.Checkpupilsforsymmetryandresponsetolight.Awhitepupil(leukocoria) may indicate a serious problem such asretinoblastomaorcataract.Checkcorneaforsizeandclarity.Acloudy,enlargedcorneaandtearingmayindicateinfantileglaucoma.Photophobiamay indicatekeratitis (herpessimplex),uveitisorinfantileglaucoma.Checkeyes fordeviation.Theeyewith thedeviationshouldbeassumed to have an organic lesion such as retinoblastoma ortoxoplasmosis involving the macula until proven otherwise.Strabismus is common in childhood. Untreated, the child candevelopamblyopia(lazyeye).

112
Checkfornystagmus(involuntaryeyemovement).Ifpresent,itwould indicate poor visual acuity caused by disorders such asmacular scars, macular hypoplasia or optic nerve hypoplasia.Therearealsoothercausesfornystagmus.Look for theredreflexasdescribed inChapter2.Absenceofaredreflexmaysuggestthepresenceofcataract,retinoblastoma,ROP(retinopathyofprematurity)orvitreousopacity.Check the optic nerve and retina if possible. Method ofexaminationisdescribedinChapter2.Ophthalmic ointment generally works better than drops forchildren.
ShakenBabySyndromeWhenababypresentswith retinalhemorrhages, abuse shouldberuledout.Thehemorrhagescanbecausedbyviolentshaking,chokingordirecteyeorheadtrauma.Papilledemaandvitreoushemorrhage may occur in association, along with subdural orsubarachnoidhemorrhageorcerebralcontusion.It is required by law in many countries to report suspectedabusetotheauthorities.Gooddocumentationof the findings isessential.
RetinopathyofPrematurity(ROP)The formation of the retinal vasculature begins at aboutweek16 of gestation from the optic disc outwards. This vasculaturereaches the nasal retinal‐edge at about 36weeks. If a baby is

113
born premature, there are areas in the peripheral retina thathave not yet developed a good blood supply and can becomeischemic, which can produce VEGF, which in turn promotesneovascularization. These new vessels can bleed and caneventuallycauseretinaldetachment.Ifneovascularizationisdetected, itcanbetreatedwithlaserorcryotherapy to prevent such a complication. Anti‐VEGF drugsarealsobeingusedtostopneovascularization.Examination of the premature infant for ROP is difficult andshouldbedonebyaretinalspecialist.
StrabismusParalytic strabismus usually occurs in older people, withdiplopia being a common complaint. Good vision is usuallyfoundinbotheyes.Neurologicwork‐upisusuallyrequired.Non‐paralytic strabismus usually occurs in infants andchildren. Diplopia rarely occurs because the child suppressesthedeviatedeye,whichisoftenamblyopic.Ophthalmicwork‐upisrequired.Common causes of neural paralytic strabismus (Cranialnerves#3,#4and#6):Inpatients younger than40, the causes are congenital defects,head trauma, cranial artery aneurysms, multiple sclerosis andothers.In patients over 40, the causes are diabetes, cerebral vascularaccidentandothers.

114
When the paralysis is in the muscle, it can occur at any age.Some of the causes are: myasthenia gravis, hyperthyroidism,blowoutfractures,andmuscularinjuries.Esotropia(ET)meansdeviationofoneeyenasally.Exotropia(XT)meansdeviationofoneeyeoutward.Hypertropia(HT)meansdeviationofoneeyeupward.Hypotropia(HoT)meansdeviationofoneeyedownward.Ocular deviations aremeasured in prism diopters.When lightpassesthroughaprism,itisbenttowardthebaseoftheprism.The prism diopter is not the same as the lens diopter, whichmeasuresmyopiaorhyperopia.Diplopiacanbecorrectedwithprisms.This isusuallydone forpatients whose diplopia is caused by diabetes or strokes andwillimprovewithtime.Prismisusuallyatemporarytreatment.Diplopia can also be relieved by patching one eye. Botulinumtoxin (Botox) can be injected into one of the muscles to treatdiplopiatemporarily.

115
PRISMS
FresnelPrismsTheseare thin, transparent sheetsofplastic.Onesidesticks tothepatient’sglassesandtheothersidehasspecialgroovesinitthatcreateaprismeffect,changingthewaylightenterstheeye.As the deviation lessens with time, the amount of prisms canalso be reduced, making this a simple, safe and effectivetreatmentfordiplopia.
Inthispatientwitharightesotropia,therightfoveaisturnedtemporally. In order to focus the light on the right fovea, aprism (with the apex nasally) is placed in front of the righteye,eliminatingthediplopia.If the patient had an exotropia, the apex would be pointedtemporally,i.e.,theprismapexalwayspointsinthedirectionofthedeviation.

116
When the deviation is felt to be permanent, surgery on themuscles canbe considered.Eacheyemuscle canbeweakened,strengthenedormoved.StrabismusSurgeryStrabismus is treatedsurgicallyearly in theUS,whichexplainswhy we hardly see any children with this condition anymore.UntilIwentintoophthalmology,itwasamysterytomehowthesurgeoncouldgettothemuscles!RECTI

117
LEFTEYE
RIGHTEYE
Resectionoftheleftmedialrectusmuscles. Themuscleisreattached about 5 mm behind the original insertion,essentiallymakingitabout5mmlonger.
Resectionoftherightlateralrectusmuscle.Themuscleisdetachedfromtheoriginalinsertion.A5mmsegmentiscut and reattached to the original insertion, essentiallymakingitabout5mmshorter.

118
Amblyopia(lazyeye)Amblyopia is decreased vision in an eye from disuse duringchildhood development. The visual pathway is plastic duringchildhood until around 6 to 9 years of age. During the plasticphase,theconnectionsbetweentheretinaandvisualcortexarestilldeveloping.Animagesentfromtheeyetothevisualcortexhastobeclearinorderforthechildtolearntosee.Iftheeyehasa severe refractive error, is misaligned, or has a cataract or
LeftesotropiaWhichmuscleneedstoberecessedandwhichoneshouldberesectedinthelefteye?(Lateralrectusresectionandmedialrectusrecession)
LeftexotropiaWhichmuscleneedstoberecessedandwhichoneshouldberesectedinthelefteye?(Medialrectusresectionandlateralrectusrecession)
119
anythingthatpreventsaclearimagefromforming,itcouldleadto permanent visual loss that can’t be corrected. This is thereasonwhyababywithcongenitalcataractmusthavesurgeryearlyon.Withamisalignedeye, thechildsimply ignoresthateye,and itcan become amblyopic. This is why the “normal” eye issometimespatched:toforcethechildtousethemisalignedeyeand prevent amblyopia. Sometimes parents don’t understandwhytheophthalmologistpatchesthechild’sgoodeye!
RetinoblastomaThis is a tumor of the primitive retinal photoreceptors thatgrowson theretina, formingawhitemass thatcancompletelyfill the eye. It is the most common primary malignant oculartumor in children, but it is very rare, with less than 500 newcasesreportedeachyearintheUS.Ifundetected,itcouldresultinthedeathofachild.Thetumorspreadsbygrowingdowntheoptic nerve toward the brain. If detected early, the overallsurvivalrateintheUSisabout90%.


CHAPTER 12: OCULAR MANIFESTATIONS OF SYSTEMIC DISEASES Ocular conditions canarise secondary to systemicdisease, andknowing their connection will often help with diagnosis. Thefirst section below discusses the most common conditions,followedbyalistoflesscommonlyencounteredconditions.Thethird section covers ocular side effects or adverse reactions tovariousdrugs.MORECOMMONDISEASESWITHOCULARMANIFESTATIONSAIDS:“Cotton wool” spots on retina; uveitis; candida chorioretinitis;cytomegalovirus (CMV) retinitis; keratitis; herpes zoster;Kaposi’ssarcomaofeyelidsandconjunctiva.AIDS usedtobeafataldiseaseandthecomplicationslistedusedto be seen worldwide. In most developed countries thesecomplications are now much less common because most HIVpatients are adequately treated. But in some underdevelopedcountries,thesecomplicationsstillexistbecausepatientsareofteninadequatelytreatedornottreatedatall.HypertensiveRetinopathy:In the less severe form, the vessels show attenuation andincreasedlightreflex,thereddishbrownoftheso‐called“copperwire” reflex. Focal and diffuse constriction and AV crossingphenomena(nicking)maybenoted.

122
In the more severe form, retinal edema, hemorrhages, andcotton‐woolspotsarepresent.Theopticdiscmayshowedema,which canbemistaken for papilledema.But the disc edema inseverehypertensionisduetoinfarctionandhypoxiaoftheopticdisc itself. (The term papilledema is reserved for disc edemaassociatedwithelevatedcerebrospinalfluidpressures.)Aprolongedhypertensivestatemayresultintheformationofamacularstarofhardexudates,whichcanpermanentlydamagethecentralvision.Thepresenceofhardexudatesinthemaculasuggests that these patientsmay also have involvement of thekidneyandotherorgans.Lupuserythematous:Retinal vasculitis is a complication associated with lupus. Theinflammation in the vessels causes leakage in the vesselwalls,macularedema,andalltheothersignsassociatedwithischemicresponseoftheretina.Toxoplasmosis, Crohn’s inflammatory bowel disease, multiplesclerosis, sarcoidosis, syphilis and Eales Disease are alsoassociatedwithretinalvasculitis.Lymedisease:Causedby thespirocheteBorreliaburgdorferi,Lymedisease isan immune‐mediated inflammatory disease with numerousocular,neuro‐ophthalmic,andsystemicmanifestations.Eye findings may include optic neuritis, papilledema, pseudo‐tumor cerebri, diplopia secondary to third and sixth nerveatrophy,andBell’spalsy.Othereyemanifestationsmayincluderetinalhemorrhages,exudativeretinaldetachmentsandiritis.Treatmentiscontroversialandbeyondthescopeofthisbook.

123
Sickle‐celldiseaseorsickle‐cellanemia:This disease may lead to various acute and chroniccomplicationsthroughoutthebody,severalofwhichhaveahighmortalityrate.Itiscausedbysickle‐shapedredbloodcellsthatobstructcapillariesandrestrictbloodflowtoanorgan,resultinginischemia.Thecomplicationintheeyeisretinalneovascularization,whichismost common at about the equator plane supra‐temporally.Thisareaisverydifficulttoseewiththedirectophthalmoscope.Thecomplicationofneovascularizationisvitreoushemorrhage.If allowed to proliferate, it can cause traction retinaldetachment.The treatment is laser photocoagulation to the areas ofneovascularization.LESSCOMMONSYSTEMICDISEASESWHICHMAYBEASSOCIATEDWITHOCULARCONDITIONSAlbinism:Nystagmus;poorvisionsecondarytopoormaculardevelopmentand refractive error; choroidal vessels visible with theophthalmoscope because of hypopigmentation of RPE; lightsensitivitybecauseoflightirisAnemia:Conjunctiva appears pale. In severe cases retinal hemorrhagesmaybepresent.AtopicDermatitis:CataractsandkeratoconusCysticFibrosis:Papilledemaandretinalhemorrhages

124
Down’sSyndrome(Trisomy21):The typical up‐slanted palpebral fissures; cataract; myopia;strabismus; amblyopia; degenerative changes in the corneasometimesleadingtokeratoconus;glaucomaandretinovascularanomaliesGalactosemia:CataractGlomerulonephritis:HypertensiveretinopathyGout:Uveitis;episcleritisHerpesZoster:Uveitis;keratitis;dermatitisoftheophthalmicbranchofthe5thcranialnerveHyperthyroidism:Proptosis(protrusionoftheeyeball);papilledemaLeadPoisoning:Papilledema;opticatrophyMigraine:Eye pain; transient visual disturbance (e.g., flashing lights,hemianopia,waves);smallpupilMultipleSclerosis:Retrobulbar (behind the eyeball) optic neuritis; optic atrophy;diplopiaMyastheniaGravis:Extraocularmuscleweakness;ptosis

125
Neurofibromatosis:Optic gliomas (usually slow‐growing and non‐cancerous);orbitalandlidtumorsNiacindeficiency(pellagra):OpticneuritisPolycythemia:Papilledema;dilatedretinalveinsRheumatoidArthritis:Thinningofthesclera;uveitisRubella(congenital):Cataract;uveitis;retinopathySarcoid:Uveitis;perivenousinfiltratesinretinaSjogren’sSyndrome:Dryeyes;cornealerosionsSyphilis:Uveitis;opticneuritis;cataracts;lensdislocation;chorioretinitis(inflammationofchoroidandretina);ArgyllRobertsonpupilTemporalArteritis:Severevasculitisaffectingtheopticnerve,leadingtotransientorpermanentvisuallossThiaminedeficiency(beriberi):Opticneuritis;weaknessoftheextraocularmusclesToxemia:Hypertensiveretinopathy

126
Toxoplasmosis:ChorioretinitisTuberculosis:Uveitis;chorioretinitisTuberousSclerosis:RetinaltumorsVitaminCdeficiency(scurvy):Hemorrhagesoftheeye—insideandoutside.VitaminDDeficiency:Papilledema;cataractVonHippel‐LindauDisease:RetinalhemangiomasWilson’sDisease:Kayser‐Fleischer ring (copper deposits in the peripheralcornea);cataractsecondarytocopperdepositsinthelensDRUGSTOXICITY:Amiodarone:PigmentwhorloncorneaChloramphenicol:OpticneuritisChloroquine/Hydroxychloroquinetoxicity:These are used in the long‐term treatment of lupuserythematosus and rheumatoid arthritis. A total dose of 100‐300g ormore of chloroquine can lead to a toxic effect on themaculaattheRPE.Hydroxychloroquinecanbetoleratedbetter.

127
Theearliest functionalchangesaredecreasedsensitivity to thered‐green on the Ishihara color test. The so‐called “bull’s eye”maculopathycanbedetectedbyfluoresceinangiography.Chlorpromazine(Thorazine):Pigmentaryretinopathy;blurredvisionContraceptiveHormones:Centralveinocclusion;opticneuritis;migraineDigitalis:YellowvisionEthambutol:Decreased color vision and visual acuity secondary toretrobulbaropticneuritisHaloperidol(Haldol):Blurredvision;oculogyriccrises(prolongedinvoluntaryupwarddeviation)Steroids:Both topical and systemic steroids can cause cataract andglaucoma;papilledemafromsystemicsteroidsTamsulosin(Flomax):Floppyirissyndrome—maycausecomplicationsduringcataractsurgeryTetracycline:PapilledemaThioridazine(Mellaril):Pigmentaryretinopathy

128
Topiramate(Topomax)—Anti‐convulsive:MaycauseangleclosureglaucomaViagra(sildenafil),Cialis(tadalifil)andLevitra(vardenafil):Some patients may experience transient, mild impairment ofcolor discrimination, which has been described as a blue‐coloredtingeofvision.Nolong‐termeffectscanbeidentifiedsofar. Therehavebeen a few casesof ischemicopticneuropathyandcentralserousretinopathyreported,buttheassociationhasnotbeenconfirmed.VitaminAIntoxication:PapilledemaVitaminDIntoxication:Bandkeratopathy

CHAPTER 13: EYE DISEASES IN DEVELOPING COUNTRIES Insomedevelopingcountries,eyeconditionsthatarenolongerseen in more developed countries are still prevalent, andsometimes in advanced stages. The main problem is poverty,whichoften leads topoorandunhygienic livingconditions (nowater or bathroom in many cases), lack of education,malnutrition, and poor infrastructurewith inadequatemedicalcare.Thischapterhelpshealthcareprovidersindevelopingcountriesunderstand what they should look for, and helps volunteerhealth care providers from developed countries be aware ofwhattheymayencounter. TRACHOMATrachomaisacontagiousbacterial(Chlamydia)infectionoftheeye. If left untreated, repeated trachoma infection can causesevere scarring of the inside of the eyelid and can cause theeyelashes to scratch the cornea (trichiasis). In addition tocausing pain, trichiasis permanently damages the cornea andcan lead to irreversible blindness. Almost 8millionpeople arevisually impaired by this disease; 500 million are at risk ofblindnessthroughout57endemiccountries.The World Health Organization has targeted trachoma foreliminationby2020throughapublichealthstrategyknownasS.A.F.E.:

130
Surgerytocorrecttrichiasis; Antibioticstotreatactiveinfection; Facialcleanliness;and Environmental improvements in endemic areas to
reducediseasetransmission.Trachomaisspreadfrompersontopersonandfromeyetoeyeby poor hygiene and contaminated fingers. Houseflies areimplicatedastheyseekthemoistureofmucousmembranes(theconjunctiva).Diagnosis:Examinationcanbedonewitha loupeandflashlight.Checkforinturned eyelashes and corneal opacity. Examine the inside ofthe upper eyelid for follicles, inflammation or scarring. Thepatient may complain of pain or itching, or, if scarring hasoccurred,afeelingofsandbehindtheeyelids.Treatment:Tetracycline 1% ointment is very effective. Topicalerythromycin may be substituted if topical tetracycline is notavailable.Oral tetracyclinemay be given against trachoma. Children andpregnantwomen are contraindicated. A one‐time 1‐gramdoseofAzithromycinisalsoeffectiveandseemstohavefewseriousadversesideeffectsinchildrenover6monthsofage.Surgicalmanagement:Surgerycanbeperformedtocorrectthedeformityofentropionandtrichiasistopreventfurtherdamagetothecornea.Thegoalistokeepthediseasefromprogressingtothisstage.

131
VITAMINADEFICIENCYVitaminA is needed for the growth and functioning of surfacetissues, which include the skin’s epithelium and the mucousmembranes, and of ocular tissues, especially the cornea andretina.Keratomalacia(softeningandmeltingofthecornea)isthemostsevereformofvitaminAdeficiency.Inmybook,SilkRoadonMyMind,IdescribeaninfantIexaminedinXinjiang(northwestChina).Shewasfromaremoteareaoftheprovinceandwasseenatthehospitalwithmultipleproblems,oneofwhichwasmeltingofhercorneaduetovitaminAdeficiency.Even mild vitamin A deficiency can reduce the chances ofsurvival in early childhood. Chronic vitamin A deficiency cancausenightblindness.TreatmentandPrevention:Alleviationofpovertyis themainprevention.VitaminAoccursineggs,milk,liverandfish.Italsooccursintheprecursorformindarkgreenleafyandyellowvegetables,tubersandfruits.VitaminA capsules (200,000 IU) are inexpensiveandavailablealmostanywhere.
ONCHOCERCIASIS(RIVERBLINDNESS)Thisisachronicparasiticinfectionthatcancausedamageinsidetheeye fromuveitis, andblindnessby scarring the corneaandretina.Over100millionpeopleareatriskofinfectioninAfricaandafewsmallareasinSouthAmericaandYemen.

132
Onchocerciasis is caused by a filarial nematode worm,Onchocercavolvulus.It istransmittedbythebiteofablackfly,which breeds in fast‐flowing rivers. Mircrofilarial prelarvaeoccurinhumanskin,whichareingestedbythefemaleblackflyand transmitted to another human host when she bites. Thelarvae then develop into adult worms in the skin, formingnodules.Themicrofilariaecanmigratethroughoutthebodyandcan be found in the bloodstream, and are found in highconcentration in the eye. The parasite causes blindness bydamagingandscarring in thecornea, retina,choroid,andopticnerve.Patientswithactiveinfectionoftheparasitesuffergreatlywitheye pain and loss of vision aswell as pain caused by the skinnodules.Diagnosiscanbemadefromaskinbiopsy.MedicalManagement:Ivermectin (Mectizan), a broad‐spectrum anti‐parasitic drug issafeandhasbeensuccessful in treatmentof thedisease,but itonlykillsthelarvae,nottheadultworms.AclinicaltrialofanewdrugcalledMoxidectin,whichnotonlykills the larvae but also sterilizes the adult worms, has beenlaunched. If successful, it could eliminate this dreadful diseasethathasplaguedsomanycountriesforcenturies.ManagementofOcularOnchocerciasis:Management of the active disease involves controlling thekeratitis,chorioretinitisanduveitis.Thedamagedonecannotbereversed.Prevention:
Reduce the number of infected individuals throughtreatment.
Interrupt the transmission by controlling the Simuliumblackfly.

133
LOALOA(LOIASIS)ORAFRICANEYEWORMThisdiseaseiscausedbythenematode(roundworm)Loaloa.Itis spreadby repeatedbites fromdeerflies inWest andCentralAfrica.Theadultwormslivebetweenlayersofconnectivetissue.It is most dramatic when a worm can be seen movingunderneath the conjunctiva or inside the eye. (If you areinterested, check YouTube for video of surgical removal of theworm.)Itlooksscary,butthewormusuallydoeslittledamagetotheeye,unlikeonchocerciasis,whichoftenleadstoblindness.Localpeopletypicallydon’tgetloiasisasseverelyasvisitorsdo.Mostpeoplewiththeinfectiondonothaveanysymptoms.There are areas where onchocerciasis and loiasis are co‐endemic. This has complicated the attempt to eradicateonchocerciasis,becauseifIvermectinisgiventoapatientwithaheavyLoaloaworminfectioninthebrain,itcancausecomaorevendeathduetothesevereinflammationthatoccurswhenthewormsdie.
HANSEN’SDISEASE(LEPROSY)Inmedical school Idida researchpaper on somepatientswithHansen’s disease and used the term “leprosy.” The professoradvisedmenever touse thewordagainbecause it carries suchstigma,andtosayHansen’sdiseaseinstead.Hansen’s disease is caused by mycobacterium leprae. It is achronic disease that affects the skin, peripheral nerves, andextremities.Whenitinvolvesthefaceandnervesoftheface,theeyescannotclosecompletely,leadingtoexposurekeratitiswith

134
corneal scarring. It can also cause uveitis and secondaryglaucoma. Blindness may result. Ocular complications can bepreventedbyearlydetectionofthedisease.Patients with this condition can be ostracized by their owncommunities because of their appearance and fear ofcontractingthedisease.Itistransmittedbyprolongedexposuretothoseinfectedwiththemycobacterium.Thisdiseaseisfoundinseveralregions:sub‐SaharanAfrica,theMiddle East, the Indian subcontinent, Indochina and islands oftheWestern Pacific. (In2014,onamedicalmission toWesternSamoa, I examined some patientswithHansen’s disease for eyecomplications.)Corneal opacity can occur if themycobacterium leprae invadethe cornea along the pathway of the corneal nerves,making itinsensitive. Without sensation, corneal injuries are not noted,leadingtocornealerosion,ulceration,andscarring.Medical treatment involves long‐term multidrug therapy withDirampicin once monthly, Clofazimine once monthly and amaintenancedosedaily,andDapsonedaily.Patients with Hansen’s disease are usually under the care ofproviderswithspecializedtraininginthisareatocoordinatethedifficult management of multiple problems, especially thoseinvolvingtheeye.
EBOLAVIRUS(EBOV)Ebola is a small, single stranded RNA virus. The vector is thefruitbat.Largemammals includinghumans,apes,andpigsaresusceptible. It is spread by direct contact with body fluids

135
including saliva, vomit, urine, blood, feces, semen, and intra‐ocularfluids.Theviruscausesaseverehemorrhagicfeverwithhematemesis,bloody diarrhea, abdominal cramping, severe dehydration anddeath in over 80% of the caseswithin a few days. During the2013‐2015 epidemic in Western Africa, it primarily affectedSierra Leone, Liberia and Guinea. About 30,000 people wereinfected;manywerehealthcareworkers.Survivorswereshowntohavethevirusremaininginthesemenandeyes(aqueousandvitreous).Treatment (as of 2015) is primarily supportive, withintravenous therapy to treat dehydration, blood pressuresupport, and oxygenation. There is no known antiviraltreatment. Some patients have been treated systemically withserum from infected surviving individuals, which containsantibodieseffectiveagainsttheEbolavirus.Late ocular manifestations include uveitis, wherein patientspresentwithblurredvision,eyepain, retinalhemorrhagesandphotophobia.About40%ofsurvivorshaveblindsspotsintheirvisualfields.Because the aqueous and vitreous may contain the virus insurvivors,great caremustbe taken toavoidexposure to thesefluids, such aswhen treatingpatientswithpenetrating traumaorthoserequiringeyesurgery,includingcataractsurgery.

136
These diseases are also found in developed countries, butpatientsaremorelikelytobeadequatelytreatedandlesslikelytosufferfromopportunisticinfections.AIDSAssociatedretinopathies:
Cytomegalovirus Pneumocystiscarinii Syphilis Acuteretinalnecrosis(herpeszosterorherpessimplex) Toxoplasmosis Cryptococcus
SYPHILISIt is especially important for primary care providers to knowthatthisdiseasecanaffectthepatient’seye.Theinfectionoccursin phases.Primary syphilis is characterized by a chancre, anerythematous papule that evolves into a painless ulcer at thesite of inoculation. If untreated, those with primary syphilisprogress to secondary syphilis 4 to 10 weeks after theappearanceofthechancre.Secondary syphilis (untreated or inadequately treated) isknowntocauseretinitisthatcanleadtoblindness.Usuallythereis evidence of anterior segment inflammation, such as cells inthe anterior chamber. Lymphadenopathy and amaculopapularrash, which often presents on the palms and soles, typifysecondarysyphilis.Tertiarysyphilismaydevelopafteravariableperiodoflatencyif untreated. The central nervous system may be involved. Intertiary syphilis, chorio‐retinitis, neuro‐retinitis and occlusivevasculardiseasemaybeobserved.

137
The presence of ocular disease warrants treatment with IVpenicillinfor10to14days.The diagnosis of syphilis necessitates testing for HIV, as co‐infectioniscommonduetosimilarriskfactors.Allpatientswithsyphilitic retinitis should be presumed to also haveneurosyphilis.TOXOPLASMOSISThis condition is spread by cat feces and is one of the mostcommon causes of posterior uveitis worldwide. The parasiteToxoplasma gondii is another one of the many opportunisticinfectionsoftenfoundinimmunocompromisedpatients.Standard treatment consists of pyrimethamine, sulfa drugs orclindamycin,oracombination.TUBERCULOSISOne third of the world’s population has latent infection withmycobacteriumtuberculosis.Onlyaverysmallportionoftheseindividuals willmanifest signs of the disease. In patientswithtuberculosis,itisrareforthediseasetoinvolvetheeye.Whenitdoes,itcausesuveitis.
STRABISMUSINCHILDRENIt is estimated that 2% of theworld’s population suffers fromstrabismus.IntheUSandotherindustrializednations,patientswith this condition are treated early. In developing countries,this is one of the leading causes of vision loss. Many of theseindividualsbecomesocietaloutcastsandhavedifficulty finding

138
spousesorjobs.Becauseitisnotlife‐threateningoradangertothesight,itisfrequentlylowontheprioritylistfortreatment.More technicians shouldbe trained todo this sortof surgery indevelopingcountries.
COMMENTSONEYECAREINDEVELOPINGCOUNTRIESInadditiontoprogramssuchastheWorldHealthOrganization’sS.A.F.E. initiative mentioned at the beginning of the chapter,therearemanyothergroupsworkingoneyecareissuesaroundtheworld.TheAravindEyeHospitals is ahospital chain in India foundedby Dr. G. Venkataswamy. It has grown into a network of eyehospitals and has had a major impact in eradicating cataract‐related blindness in India and some other parts of the world.This model has been copied in other countries. The companyproducesitsownintra‐ocularlensesatapriceof$2each.AtitsMadurai, Tamil Nadu campus, it regularly trains surgeons andtechniciansfromaroundtheworld,includingsomeprovincesinChina.Aravindisfocusedonefficiencyandhygiene.ItcandoacataractsurgerywithanIOLforaslittleas$35.Itsinfectionrateisabout4/1000 in contrast to the international norm of 6/1000surgeries.TheFredHollowsFoundationwasfoundedbyDr.FredHollowsin 1992 and is based in Australia. The Foundation focuses ontreatingandpreventingblindnessallovertheworld(sofar,over19 countries), particularly in the Pacific, South and SoutheastAsia and Africa. It also provides training for local eye careproviders and has built hospitals in several countries. It has

139
provided extensive training of medical staff and screening forpoorvisionandeyedisease,andhassubsidized treatmentandprovisionofequipmentandinfrastructuresincountriessuchasEritrea,Kenya,Rwanda,SouthAfrica,andTanzania.Orbis International is a non‐profit organization dedicated tosaving sight worldwide. It is well known for its “Flying EyeHospital,” an ophthalmic hospital and teaching facility locatedon board a jumbo jet. Its entire staff, including the pilot andflightcrew,arevolunteers. Ithasservedinover100countries.Orbis is headquartered in New York with offices in Toronto,Dublin,HongKong,Macau,Shanghai,Taipei,andCapeTown.Itnow has a telemedicine program called Cybersight(http://www.cybersight.org), which uses the Internet toconnecteyecareprofessionalsforone‐on‐onecollaborationandmentoring.The Hawaiian Eye Foundation, based in Honolulu, has madenumerous expeditions to Pacific Basin countries to providehumanitarianeyesurgeryandtraining,includingrecenttrainingprograms in Vietnam and Myanmar to teach advancedtechniques toeyesurgeons. Italso fundsresearchprojectsandoperates outreach programs that include training scholarshipsanddonationsofequipmentandsupplies.Thesearejustafewofthemanyorganizationsthatprovideeyeservices to different parts of the world. In some countries,because of the brain drain of professionals to wealthiercountries, there are tremendous shortages of physicians, andophthalmologistsinparticular.Somecharityorganizationshavetrainednon‐physiciantechnicians todoeyesurgeries. Itseemsthat thesepioneeringprogramshavehelpeda largenumberofpatientswhowouldotherwisenothaveaccesstosurgery.

140
WhenIwasinWesternSamoain2014,Iwasagainremindedofthe human and economic costs of blindness. (Iam referring topeoplewho become blind late in life.Most blind people, just aswith sighted people, lead very productive liveswhen they haveaccess to education and opportunities.) The daughter (a youngschoolteacher)ofawomaninherearlyfiftieswhohadrecentlygoneblindfromdiabeticretinopathysadlytoldmethatafterhermother lost her sight, she had to quit her job to take care ofher—atleastuntilhermothercouldlearntogetaroundandbeleftalone.Whenapersongoesblind,itaffectsthewholefamily.This casewasespecially tragicbecause thewoman’sblindnesscouldhavebeeneasilypreventedthroughlasertreatment.Similarly, the thousands of patients affected by thecomplications of trachoma could have been spared theirsufferingby using a small tubeof ointment costing less than adollar!The goal of this book is to educate both health care providersand patients so that they are aware of eye disorders andpossible treatments and understand that in almost all cases,people do not have to go blind. Life is already a challenge formany in developing countries without preventable blindnessaddingtotheirdifficulties.

GLOSSARY Accommodation: The adjustment of the eye for seeing atdifferent distances, by changing the shape of the lens via theactionoftheciliarymuscles,thusfocusingaclearimageontheretina.
Agnosia:Inabilitytorecognizecommonthingsdespiteanintactvisualapparatus.
Albinism: A hereditary deficiency of pigment in the retinalpigmentepithelium,iris,andchoroid.
Amaurosisfugax:Transientlossofvision.Amblyopia:Reducedvisualacuitythatcannotbecorrectedwithlenses,intheabsenceofdetectableanatomicdefectintheeyeorvisualpathways.
Aniridia:Absenceoftheiris.Aniseikonia:Whenthe imageseenbyoneeyediffers insizeorshapefromthatseenbytheother.
Anisometropia:Differenceinrefractiveerroroftheeyes.Anophthalmos:Absenceofatrueeyeball.Anterior chamber: The space filled with aqueous bounded bythecorneaanteriorlyandbytheirisposteriorly.

142
Aphakia:Absenceofthelens.Aqueous:Clear,wateryfluidthatfillstheanteriorandposteriorchambers.
Asthenopia:Eyefatiguecausedbytiring.Astigmatism:Refractiveerror thatprevents the lightrays fromcoming to a single focus on the retina because of differentdegreesofrefractioninthevariousmeridiansofthecornea.
Binocularvision:Abilityof theeyes to focusononeobjectandfusethetwoimagesintoone.
Blepharitis:Inflammationoftheeyelids.Blepharoptosis:Droopingoftheeyelid.Blepharospasm:Involuntaryspasmoftheeyelids.Blindspot:Blankarea in thevisual field,whichcorrespondstothelightraysthatcometoafocusontheopticnerve.
Blindness: In the US, the usual definition of legal blindness iscorrectedvisualacuityof20/200orlessinthebettereye,oravisualfieldoflessthan20degreesinthebettereye.
Buphthalmos:Largeeyeballininfantileglaucoma.Canal of Schlemm:A circularmodified venous structure in theanteriorchamberangle.
Canaliculus: Small tear drainage tube in the inner aspect ofupperand lower lids leading fromthepuncta to thecommoncanaliculusandthentothetearsac.

143
Canthus: The angle at either end of the eyelid aperture—specifiedasinnerorouter.
Cataract:Lensopacity.Cataract extraction: Removal of a cataract by one of severalmethods.
Chalazion:Inflammationofameibomiangland.Chemosis:Conjunctivaledema.Choroid:Vascularmiddlecoatbetweentheretinaandsclera.Ciliarybody:Portionoftheuvealtractbetweentheirisandthechoroidincludingtheciliaryprocessesandtheciliarymuscle.
Coloboma:Congenitalcleftduetothefailureofsomeportionoftheeyeorocularadnexatocompletegrowth.
Color blindness: Diminished ability to perceive differences incolor.
Concavelens:Lenshavingthepowertodivergeraysoflight.Itisalsoknownasnegative,myopic,orminuslens,denotedbythesign(–).
Cones and rods: Twokinds of retinal receptor cells. Cones areconcerned with visual acuity and color vision; rods, withperipheralvisionunderdimillumination.
Conjunctiva:Mucousmembrane that lines theposterior aspectoftheeyelidsandtheanteriorsclera.
Convergence:Theprocessofdirectingthevisualaxesoftheeyestoanearpoint.

144
Convexlens:Lenshavingpowertoconvergeraysoflightandtobringthemintofocus;alsoknownasmagnifying,hyperopic,orpluslens,denotedbythesign(+).
Cornea: Transparent portion of the outer coat of the eyeballformingtheanteriorwalloftheaqueouschamber.
Cornealcontactlenses:Thinlensesthatfitdirectlyonthecorneaundertheeyelids.
Corneal graft (keratoplasty): Surgery to restore vision byreplacingasectionofopaquecornea,either involving the fullthickness of the cornea (penetrating keratoplasty) or only asuperficiallayer(lamellarkeratoplasty).
Crystalline lens (or just the lens):A semi‐transparentbiconvexstructure suspended in the eyeball between the aqueous andthevitreous.Itsfunctionistobringraysof lighttoafocusontheretina.
Cycloplegic:Adrug that temporarily relaxes theciliarymuscle,paralyzingaccommodation.
Cylindricallens:Asegmentofacylinder,therefractivepowerofwhichvariesindifferentmeridians.
Dacryocystitis:Infectionofthelacrimalsac.Dark adaptation: The eyes’ ability to adjust to decreasedillumination.
Diopter: Unit of measurement that refers to the strength ofrefractivepowerinlensesorprisms.
Diplopia:Seeingoneobjectastwo.

145
“E” test: A system of testing visual acuity in illiterates,particularlypreschoolchildren.
Drusen:Smallroundyellowspots inoraroundthemacula justoutsidethepigmentepithelium.Whenintheopticnervehead,drusen appear as bumpy excrescences, which should not beconfusedwithpapilledema.
Dry‐eyesyndrome:Irritationsecondarytodecreasedtearing.Ectropion:Turningoutoftheeyelid.Emmetropia:Absenceofrefractiveerror.Endophthalmitis:Severeintraocularinfectionorinflammation.Enophthalmos:Abnormalretro‐displacementoftheeyeball.Entropion:Aturninginwardoftheeyelid.Enucleation:Completesurgicalremovaloftheeyeball.Episcleritis: Benign inflammation of the tissue between theconjunctivaandsclera.
Epiphora:Tearing.Esophoria:Atendencyoftheeyestoturninward.Esotropia:Amanifestinwarddeviationoftheeyes.Evisceration:Removalofthecontentsoftheeyeball.Exenteration: Removal of the entire contents of the orbit,includingtheeyeballandlids.

146
Exophoria:Atendencyoftheeyestoturnoutward.Exophthalmos:Abnormalprotrusionoftheeyeball.Exotropia:Amanifestoutwarddeviationofoneorbotheyes.Farsightedness:SeeHyperopia.Fieldofvision:theentireareathatcanbeseenwithoutshiftingthegaze.
Floaters:Smalldarkparticlesinthevitreous.Focus: The point to which rays are converged after passingthroughalens.Focaldistanceisthedistancebetweenthelensandthefocalpoint.
Fornix:Thejunctionofthepalpebralandbulbarconjunctiva.Fovea: The center of the macula adapted for the most acutevision.
Fundus: The posterior portion of the eye, visible through anophthalmoscope.
Fusion:Coordinating the images receivedby the twoeyes intooneimage.
Glaucoma: Disease usually caused by elevated intraocularpressure,resultinginopticatrophyandlossofvisualfield.
Gonioscopy:Atechniqueofexaminingtheanteriorangle,usingaspecialcornealcontactlens.
Hemianopia: Blindness of onehalf the field of vision in one orbotheyes.

147
Hordeolum,external(sty):Infectionofahairfollicle.Hordeolum,internal:Infectionofthemeibomiangland.Hyperopia, hypermetropia (farsightedness): A refractive errorinwhich the focal point of light rays from a distant object isbehindtheretina.
Hyperphoria:Atendencyoftheeyestodeviateupward.Hypertropia:Amisalignmentoftheeyeswherebythevisualaxisofoneeyeishigherthanthefellowfixatingeye.
Hyphema:Bloodintheanteriorchamber.Hypopyon:Pusintheanteriorchamber.Hypotony:Abnormallysofteyefromanycause.Injection:Congestionofbloodvessels.Iris:Circularmembrane(thecolorpart,e.g.,brown,blue,green)suspendedbehindthecorneaandinfrontofthelens.
Jaegertest:Atest fornearvisionusing linesofvarioussizesoftype.
Keratoconus:Cone‐shapeddeformityofthecornea.Keratomalacia:Softeningof thecornea,usuallyassociatedwithvitaminAdeficiency.
Keratoplasty:Corneatransplant(graft).Lacrimalsac:Thedilatedareaatthejunctionofthenasolacrimalductandthecanaliculi.

148
Lesion:Injury.Lens(Crystallinelens):Arefractivemediumhavingoneorbothcurvedsurfaces.
Leukoma:Densecornealopacityduetoanycause.Limbus:Junctionofthecorneaandsclera.Macula lutea (or just macula): (Latin: macula=spot;lutea=yellow). The round or somewhat oval avascular centeroftheretinausedforcentralvision.
Metamorphopsia:Wavydistortionofvision.Microphthalmos:Abnormalsmallnessoftheeyeball.Miotic:Adrugcausingpupillaryconstriction.Mydriatic:Adrugcausingpupillarydilatation.Myokymia: Twitching of eyelids, usually a benign transientcondition, probably related to fatigue or tension. It is usuallyunilateral.
Myopia(nearsightedness):Arefractiveerrorinwhichthefocalpoint for light rays from a distant object is anterior to theretina.
Neovascularization:Formationofnewbloodvessels.Nicking(arteriovenousorAVnicking):aphenomenonwherebya small artery crosses a small vein, resulting in bulging oneithersideoftheintersection.

149
Nystagmus:Aninvoluntary,rapidmovementoftheeyeballthatmaybehorizontal,vertical,rotatory,ormixed.
Oculist:Anoutdatedtermforophthalmologist,aphysicianwhoisaspecialistindiseasesoftheeye.
Ophthalmicneonatorum:Conjunctivitisinanewborn.Ophthalmoscope: An instrument with a special illuminationsystemforviewingtheinsideoftheeye,particularlytheretinaandassociatedstructures.
Opticatrophy:Opticnervedegeneration.Opticdisc:Thevisibleportionoftheopticnerveinsidetheeye.Optic nerve: The nerve that carries visual impulses from theretinatothebrain.
Optician: A person who makes or deals in glasses or otheropticalinstrumentsandwhofillsprescriptionsforglasses.
Optometrist: A non‐physician trained in the examination andmeasurementofrefractionoftheeye. Insomestatestheyarelicensedtotreatsomeeyeconditions.
Orthoptist: A person who gives training to those with ocularmuscleimbalances.
Palpebral:Pertainingtotheeyelid.Pannus:Infiltrationofthecorneawithbloodvessels.Papilledema:Swellingoftheopticdisc.Perimeter:Aninstrumentformeasuringthefieldofvision.

150
Peripheral vision: Ability to perceive the presence, motion, orcolorofobjectsoutsidethedirectlineofvision.
Photocoagulation: A method, usually involving a laser, toartificiallyburntheretinaandchoroidfortreatmentofcertaintypes of retinal disorders such as diabetic retinopathy orretinaldetachment.
Photophobia:Abnormalsensitivitytolight.Photopsia:Appearanceofflashesorsparkswithintheeyeduetoirritationof the retina,usually causedby thevitreouspullingonit.
Phthisis bulbi: Atrophy of the eyeball with blindness anddecreased intraocular pressure, due to end‐stage intraoculardisease.
Pinguecula: A benign, usually yellowish, soft, slightly elevatedareafoundtypicallynasaltothecornea,lessoftenlateral.
Posterior chamber: Space filled with aqueous, anterior to thelensandposteriortotheiris.
Presbyopia:Blurrednearvision(oldsight)usuallyevidentafterage 40, due to reduction in the ability of the lens toaccommodate.
Pseudophakia:Presenceofanartificial intraocularlensimplantfollowingcataractextraction.
Pterygium:Agrowthof tissue(usually triangular) thatextendsfromtheconjunctivaoverthecornea.
Ptosis:Droopingoftheeyelid.

151
Puncta:Externalorificesoftheupperandlowercanaliculi.Pupil:Theroundholeinthecenteroftheiris.Refraction: In relation to ophthalmology, the determination ofrefractive errors of the eye and correction by glasses. Inphysics, thedeviation in thecourseofraysof light inpassingfrom one transparent medium into another of differentdensity.
Refractive error: A defect that prevents light rays from beingbroughttoasinglefocusontheretina.
Refractive media: The transparent parts of the eye havingrefractivepower.
Retina:Theinnermostlayeroftheeye,consistingofthesensoryretina, which is composed of light‐sensitive neural elementsconnectingtootherneuralcells,andthepigmentepithelium.
Retinaldetachment:Aseparationoftheretinafromthechoroid.Retinitispigmentosa:Ahereditarydegenerationandatrophyoftheretina.
Retinoblastoma: A rare malignant retinal tumor that affectsyoungchildren.
Retinoscope: An instrument for testing the objective aspect ofrefraction.
Rods: Retinal receptor cells concerned with peripheral visionunderdecreasedillumination.
Rubeosis: Growth of abnormal vessels on the iris, signifyingischemiaoftheretina.

152
Sclera:Thetoughwhitecoveringoftheeyethat,alongwiththecornea,formstheexternalprotectivecoatoftheeye.
Scotoma:Ablindorpartiallyblindareainthevisualfield.Slit lamp: A microscope with a special light source forexaminationoftheeye,principallytheanteriorsegment.
Snellenchart:AchartdrawntoSnellenmeasurement,consistingoflettersornumbersingradedsizesfortestingcentralvisualacuity.
Strabismus(heterotropia):Amanifestdeviationoftheeyes.Sty (External hordeolum): Infection of a hair follicle along thelid.
Sympathetic ophthalmia: Inflammation in one eye followinginjury(traumaticinflammation)inthefelloweye.
Synechia:Adhesionoftheiristothecornea(anteriorsynechia)orlens(posteriorsynechia).
Syneresis:Adegenerativeprocesswithinthevitreousgel.Telangiectasia:An areawith excessivenumbers of small bloodvessels.
Tonometer:Aninstrumentformeasuringintraocularpressure.Trachoma: A serious infection of the conjunctiva and corneacausedbyachlamydialinfection.
Trichiasis:Inwardturningofeyelashesagainsttheeye,resultinginocularirritationandsometimesdamage.

153
Tropia:Strabismus.Uvea(uvealtract):Theiris,ciliarybodyandchoroid.Uveitis:Inflammationofoneorallportionsoftheuvealtract.Visualacuity:Detailedcentralvision.Vitreous:Transparent,colorlessgelfillingtheeyeballbehindthelens.
Zonule: The fine tissue strands that stretch from the ciliaryprocessestothelensequator(360degrees)andholdthelensinplace.


