practical management of anticoagulation · practical management of anticoagulation juliann horne,...
TRANSCRIPT
PRACTICAL MANAGEMENT OF ANTICOAGULATION
Juliann Horne, PharmD
PGY2 Pharmacy Resident in Ambulatory Care
UNM College of Pharmacy
“THE BLOOD THINS AND THE PLOT THICKENS…”
Disclosure
• No conflicts of interest to disclose
• Thanks to Allison Burnett, PharmD, CACP, PhC and the UNMH Inpatient Anticoagulation Service for much of the material and resources in this presentation.

Learning Objectives
• Compare and contrast available parental anticoagulants.
• Compare and contrast available oral anticoagulants.
• Design an appropriate anticoagulant bridging plan.
• Describe payment challenges and offer solutions for direct oral anticoagulants.
• Given an individual patient, recommend an appropriate anticoagulant therapy.

Outline
Review of coagulation cascade
Review of parenteral anticoagulants
Review of oral anticoagulants
Direct oral anticoagulants (DOACs)
Bridging and switching between agents
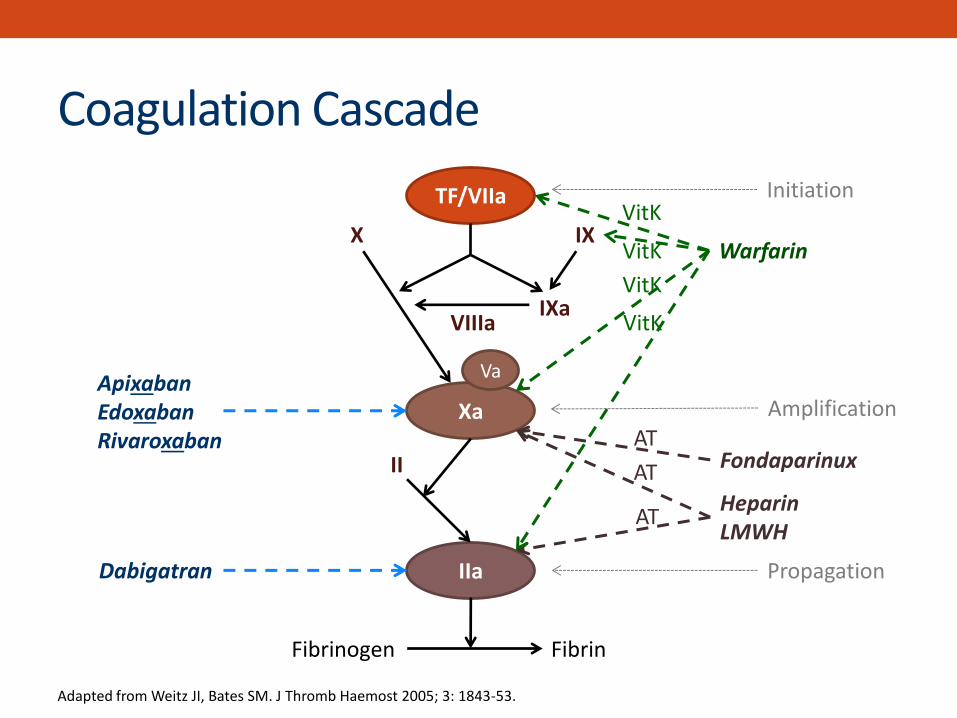
Coagulation Cascade
TF/VIIa
Xa
IIa
II
Fibrinogen Fibrin
X IX
IXa VIIIa
Dabigatran
Apixaban Edoxaban Rivaroxaban
Initiation
Amplification
Propagation
Adapted from Weitz JI, Bates SM. J Thromb Haemost 2005; 3: 1843-53.
Fondaparinux
Heparin LMWH
AT
AT
AT
Warfarin
Va
VitK
VitK
VitK
VitK
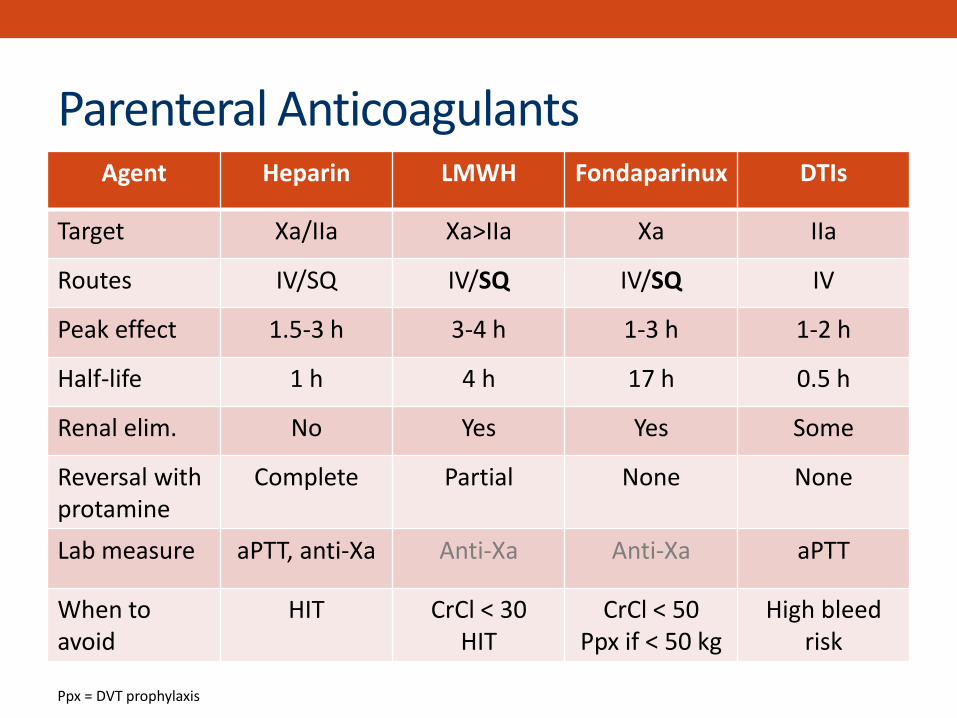
Ppx = DVT prophylaxis
Agent Heparin LMWH Fondaparinux DTIs
Target Xa/IIa Xa>IIa Xa IIa
Routes IV/SQ IV/SQ IV/SQ IV
Peak effect 1.5-3 h 3-4 h 1-3 h 1-2 h
Half-life 1 h 4 h 17 h 0.5 h
Renal elim. No Yes Yes Some
Reversal with protamine
Complete Partial None None
Lab measure aPTT, anti-Xa Anti-Xa Anti-Xa aPTT
When to avoid
HIT CrCl < 30 HIT
CrCl < 50 Ppx if < 50 kg
High bleed risk
Parenteral Anticoagulants
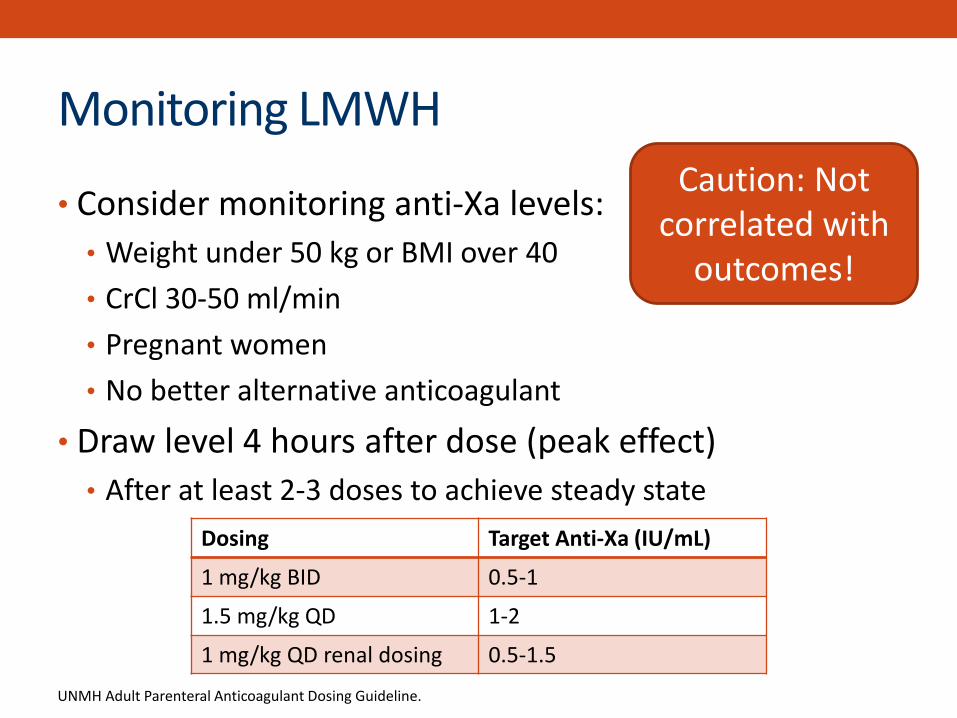
Monitoring LMWH
• Consider monitoring anti-Xa levels:
• Weight under 50 kg or BMI over 40
• CrCl 30-50 ml/min
• Pregnant women
• No better alternative anticoagulant
• Draw level 4 hours after dose (peak effect)
• After at least 2-3 doses to achieve steady state
UNMH Adult Parenteral Anticoagulant Dosing Guideline.
Caution: Not correlated with
outcomes!
Dosing Target Anti-Xa (IU/mL)
1 mg/kg BID 0.5-1
1.5 mg/kg QD 1-2
1 mg/kg QD renal dosing 0.5-1.5
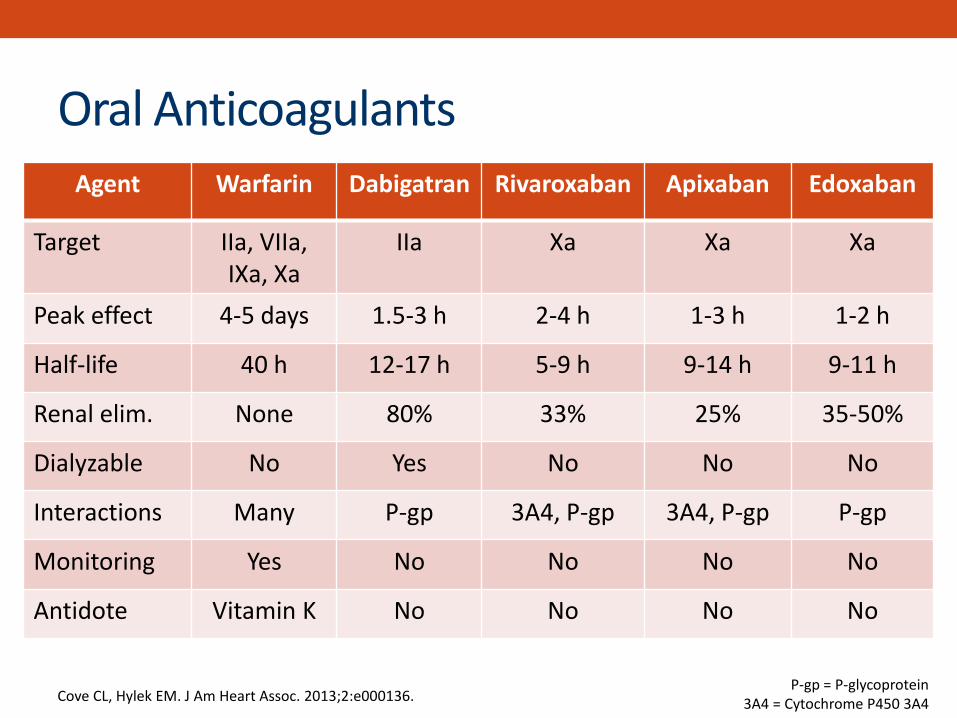
Agent Warfarin Dabigatran Rivaroxaban Apixaban Edoxaban
Target IIa, VIIa, IXa, Xa
IIa Xa Xa Xa
Peak effect 4-5 days 1.5-3 h 2-4 h 1-3 h 1-2 h
Half-life 40 h 12-17 h 5-9 h 9-14 h 9-11 h
Renal elim. None 80% 33% 25% 35-50%
Dialyzable No Yes No No No
Interactions Many P-gp 3A4, P-gp 3A4, P-gp P-gp
Monitoring Yes No No No No
Antidote Vitamin K No No No No
P-gp = P-glycoprotein 3A4 = Cytochrome P450 3A4 Cove CL, Hylek EM. J Am Heart Assoc. 2013;2:e000136.
Oral Anticoagulants
Outline
Review of coagulation cascade
Review of parenteral anticoagulants
Review of oral anticoagulants
Direct oral anticoagulants (DOACs)
Bridging and switching between agents
DOACs
Approved indications & dosing
Efficacy & safety in NVAF & VTE
Lab measurement
Patient selection
Payment challenges and solutions
DOACs
Approved indications & dosing
Efficacy & safety in NVAF & VTE
Lab measurement
Patient selection
Payment challenges and solutions
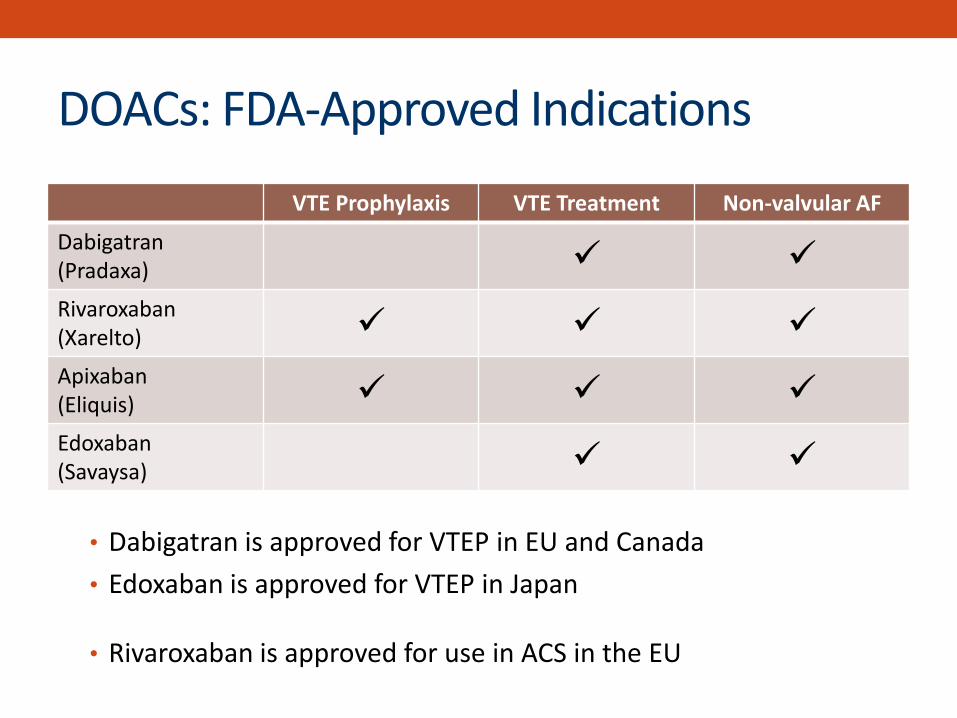
DOACs: FDA-Approved Indications
VTE Prophylaxis VTE Treatment Non-valvular AF
Dabigatran (Pradaxa)
Rivaroxaban (Xarelto)
Apixaban (Eliquis)
Edoxaban (Savaysa)
• Dabigatran is approved for VTEP in EU and Canada
• Edoxaban is approved for VTEP in Japan
• Rivaroxaban is approved for use in ACS in the EU
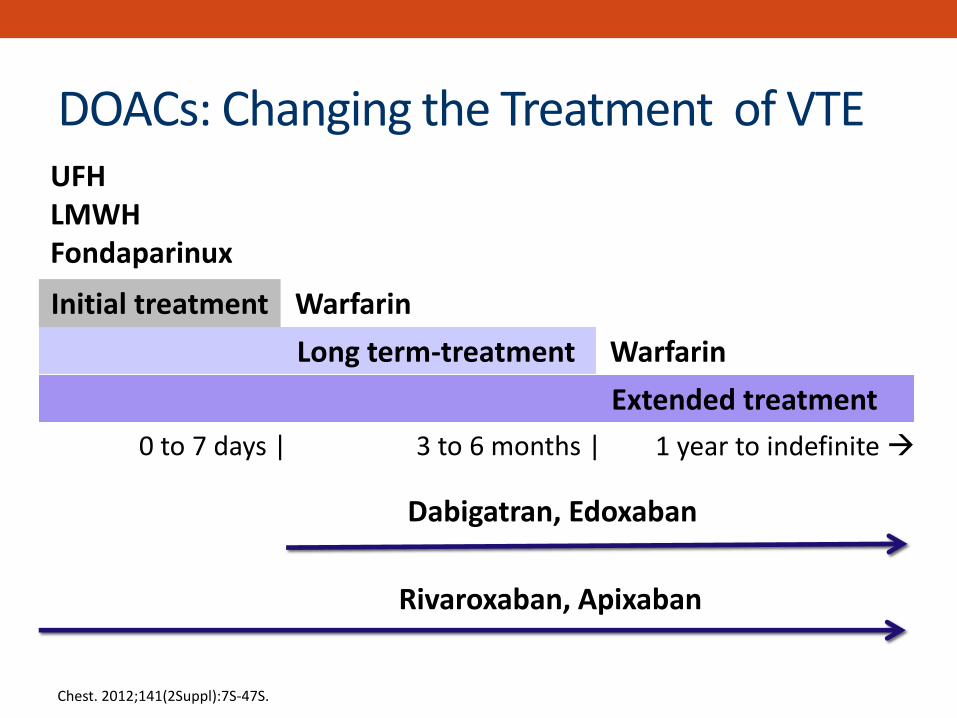
0 to 7 days |
Warfarin
UFH LMWH Fondaparinux
Initial treatment
Long term-treatment
Extended treatment
Warfarin
Dabigatran, Edoxaban
Rivaroxaban, Apixaban
3 to 6 months | 1 year to indefinite
DOACs: Changing the Treatment of VTE
Chest. 2012;141(2Suppl):7S-47S.
DOAC: Dosing
• Varies by:
–DOAC
–Indication
–Country
• May require adjustment for:
–Renal impairment
–Age
–Weight
–Drug interactions
–A combination of the above

DOACs: Dosing (FDA Labeling)
Apixaban Dabigatran Rivaroxaban Edoxaban
Non-valvular atrial fibrillation
5 mg PO BID 2.5 mg PO BID*
150 mg PO BID 75 mg PO BID* Avoid: CrCl < 15
20 mg PO daily 15 mg PO daily* Avoid: CrCl < 15
60 mg PO daily 30 mg PO daily* Avoid: CrCl > 95
VTE prophylaxis (orthopedic)
2.5 mg PO BID
Not approved in US
10 mg PO daily Avoid: CrCl < 30
Not approved in US
VTE tx & prevention of recurrence
10 mg PO BID x 7 days, then 5 mg BID 2.5 mg BID after 6 months
150 mg PO BID after parenteral Avoid: CrCl < 30
15 mg PO BID x 21 days, then 20 mg PO daily Avoid: CrCl < 30
60 mg PO daily 30 mg PO daily* after parenteral Avoid: CrCl < 15
* Adjusted for renal impairment, drug interactions, age, low weight or a combination of these factors Treatment doses of rivaroxaban should be taken with largest meal of the day
DOACs
Approved indications & dosing
Efficacy & safety in NVAF & VTE
Lab measurement
Patient selection
Payment challenges and solutions
NON-VALVULAR ATRIAL FIBRILLATION (NVAF)
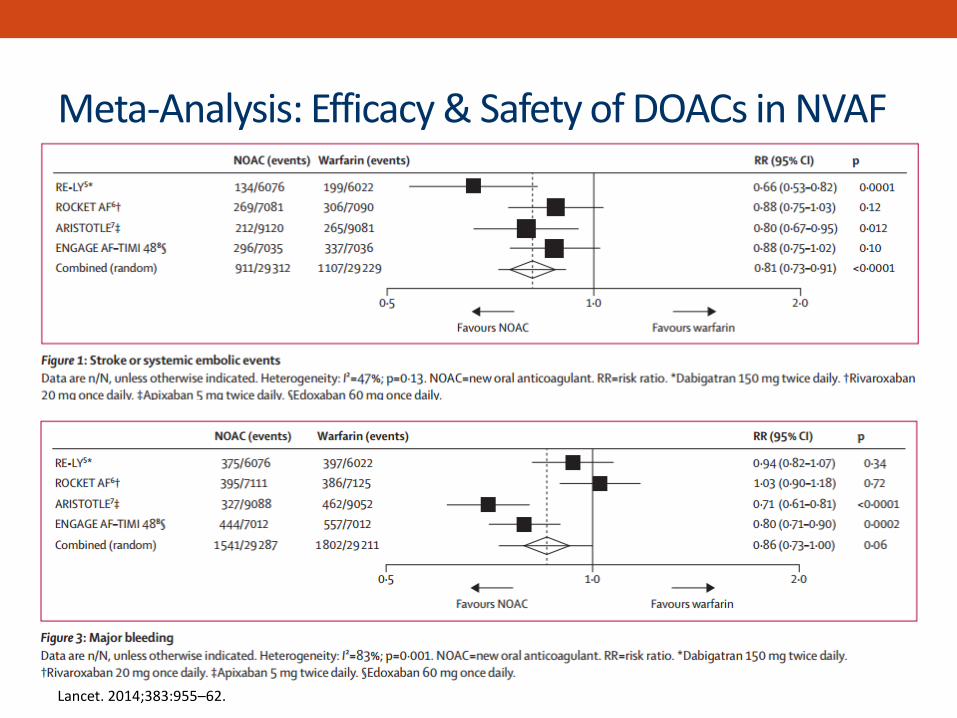
Meta-Analysis: Efficacy & Safety of DOACs in NVAF
Lancet. 2014;383:955–62.

Meta-Analysis: Efficacy & Safety of DOACs in NVAF
Lancet. 2014;383:955–62.
VENOUS THROMBOEMBOLISM (VTE) TREATMENT

Meta-Analysis: Efficacy in VTE
Prevention of Recurrent VTE
DVT
PE
Non-Fatal PE
Eur J Vasc Endovasc Surg. 2014;48(5):565-75. NOAC | VKA

Meta-Analysis: Safety in VTE
Major Bleeding
Fatal Bleeding
All-Cause Mortality
Net Clinical Benefit
Eur J Vasc Endovasc Surg. 2014;48(5):565-75. NOAC | VKA

DOACs
Approved indications & dosing
Efficacy & safety in NVAF & VTE
Lab measurement
Patient selection
Payment challenges and solutions
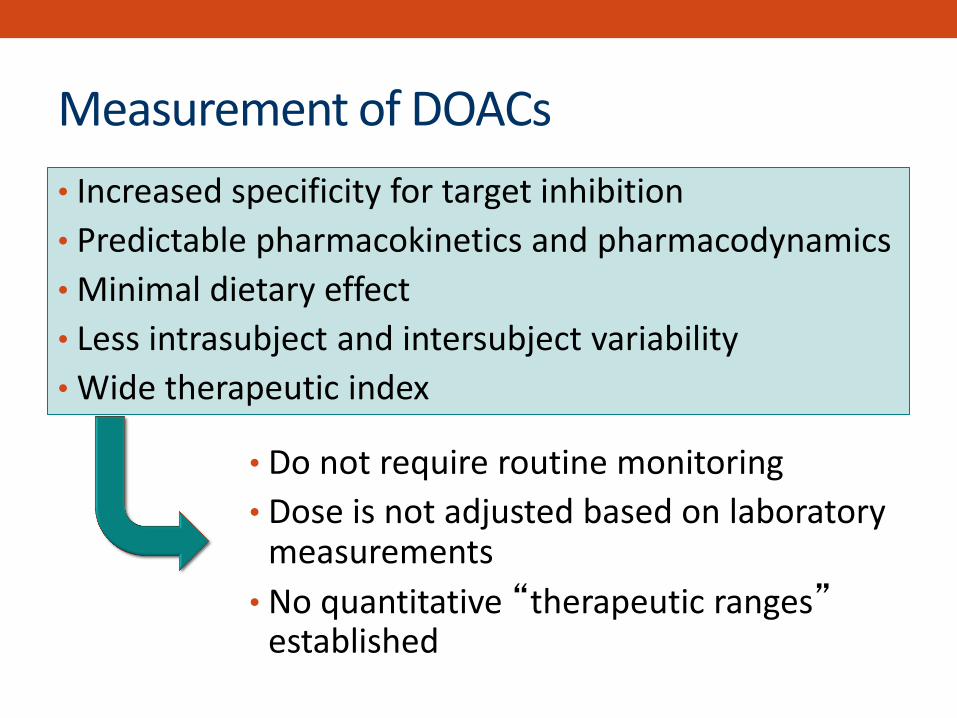
Measurement of DOACs
• Increased specificity for target inhibition
• Predictable pharmacokinetics and pharmacodynamics
• Minimal dietary effect
• Less intrasubject and intersubject variability
• Wide therapeutic index
• Do not require routine monitoring
• Dose is not adjusted based on laboratory measurements
• No quantitative “therapeutic ranges” established
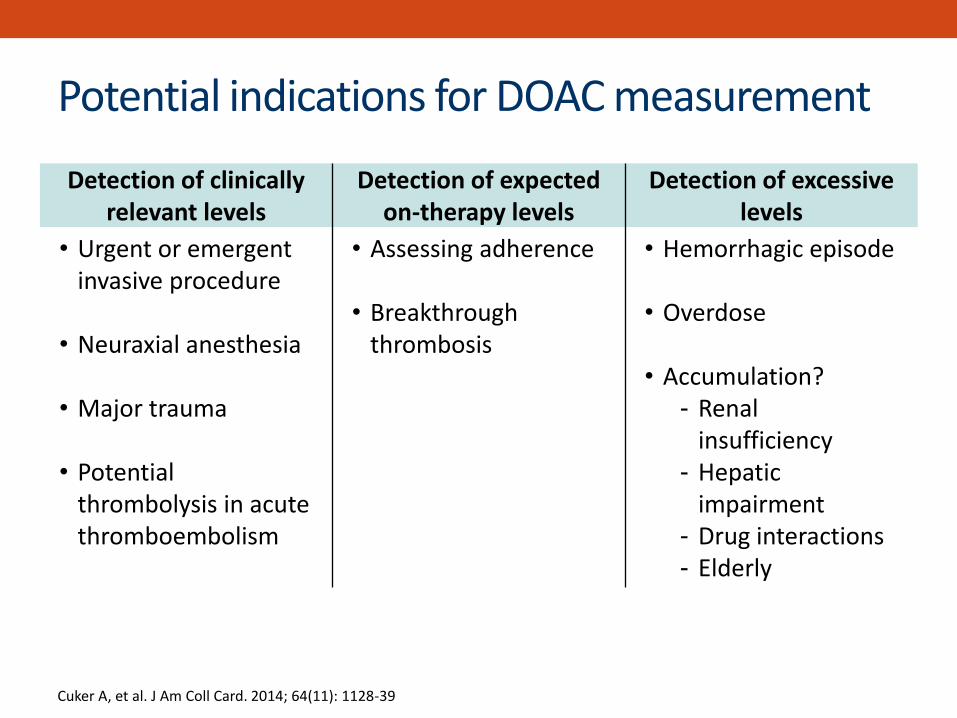
Potential indications for DOAC measurement Detection of clinically
relevant levels Detection of expected
on-therapy levels Detection of excessive
levels
• Urgent or emergent invasive procedure
• Neuraxial anesthesia
• Major trauma
• Potential thrombolysis in acute thromboembolism
• Assessing adherence
• Breakthrough thrombosis
• Hemorrhagic episode
• Overdose
• Accumulation? - Renal
insufficiency - Hepatic
impairment - Drug interactions - Elderly
Cuker A, et al. J Am Coll Card. 2014; 64(11): 1128-39
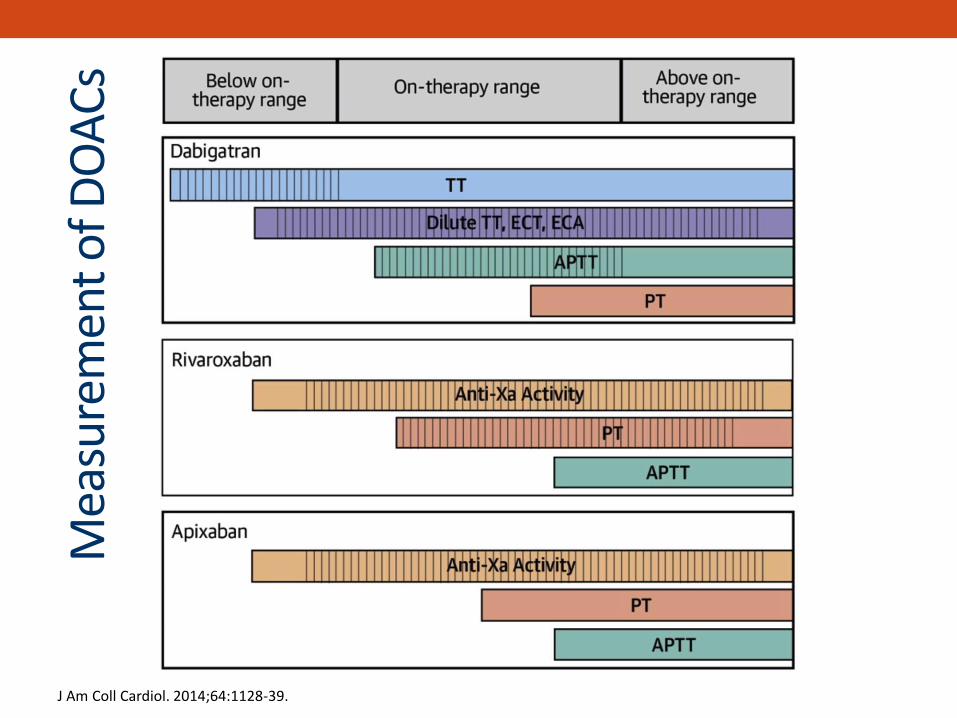
J Am Coll Cardiol. 2014;64:1128-39.
Mea
sure
men
t o
f DO
AC
s

Measurement of DOACs
• Routine coagulation assays
–aPTT, PT, anti-Xa
–Helpful in determining presence of drug (qualitative only)
–Readily available in most reference labs
• Specialty coagulation assays
–Calibrated anti-Xa, TT, dTT, ECT, drug concentration
–Not readily available nor standardized
–Research or investigational use only at this point
J Am Coll Cardiol. 2014;64:1128-39.
Do not use warfarin-based
INR

DOACs
Approved indications & dosing
Efficacy & safety in NVAF & VTE
Lab measurement
Patient selection
Payment challenges and solutions

• Which of the following patients would be considered a good candidate for DOAC therapy?
A. 68 year-old obese male on aspirin and clopidogrel for a drug-eluting stent placed 1 month ago
B. 65 year-old female with diabetes & hypertension, both well-controlled on medication, normal kidney function and new onset atrial fibrillation
C. 37 year-old female with end-stage renal disease, on hemodialysis, who has thrombosed her dialysis fistula
D. 54-year-old male with a history of recurrent VTE and labile INR due to non-compliance with warfarin therapy
Patient Case
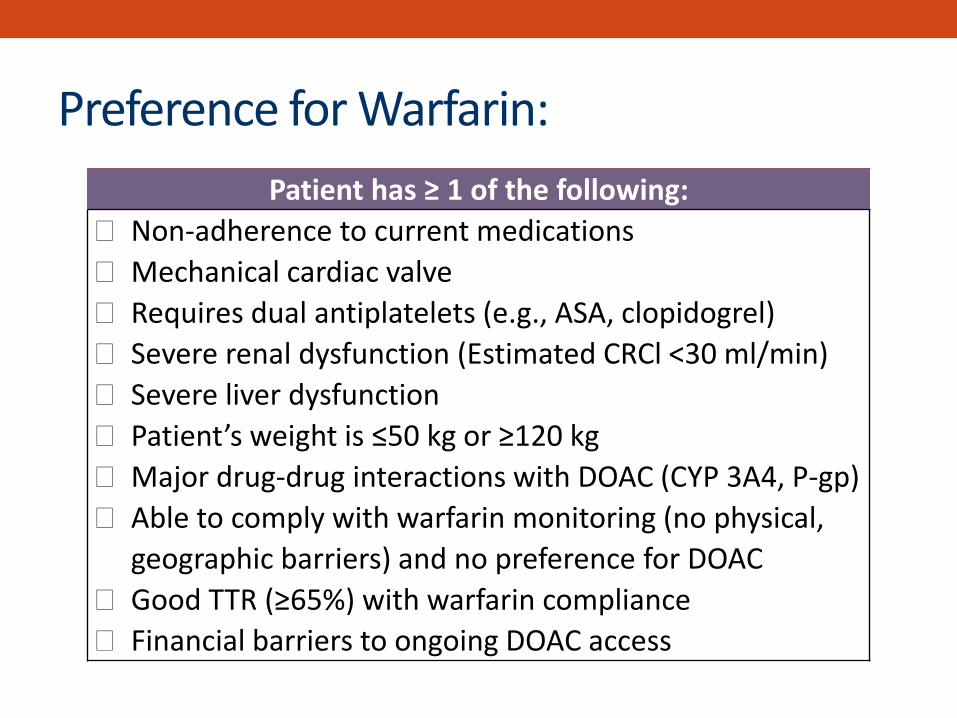
Preference for Warfarin:
Patient has ≥ 1 of the following:
Non-adherence to current medications
Mechanical cardiac valve
Requires dual antiplatelets (e.g., ASA, clopidogrel)
Severe renal dysfunction (Estimated CRCl <30 ml/min)
Severe liver dysfunction
Patient’s weight is ≤50 kg or ≥120 kg
Major drug-drug interactions with DOAC (CYP 3A4, P-gp)
Able to comply with warfarin monitoring (no physical,
geographic barriers) and no preference for DOAC
Good TTR (≥65%) with warfarin compliance
Financial barriers to ongoing DOAC access
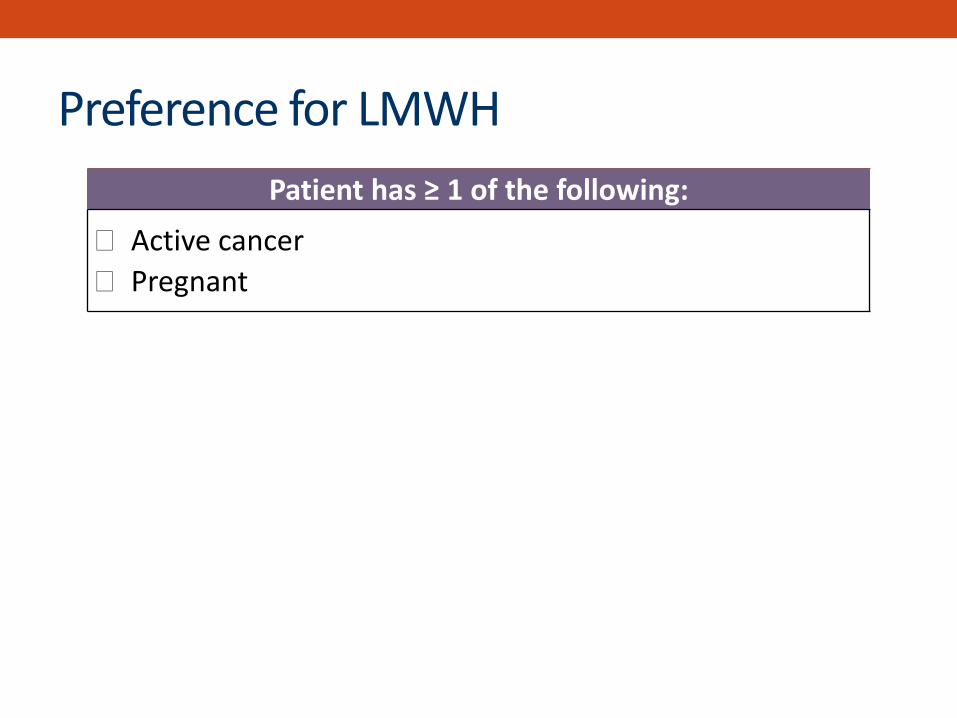
Preference for LMWH
Patient has ≥ 1 of the following:
Active cancer
Pregnant

DOAC Selection
Patient characteristic Preferred Agent
History of GI bleed Apixaban
Edoxaban (dose adjust)
Prefer once a day dosing Rivaroxaban
Edoxaban
Moderate renal
insufficiency (CrCl 30-49) Apixaban
Rivaroxaban
History of MI Apixaban
Rivaroxaban
History of stroke Apixaban
Dyspepsia Rivaroxaban/apixaban/edoxaban

• Which of the following patients would be considered a good candidate for DOAC therapy?
A. 68 year-old obese male on aspirin and clopidogrel for a drug-eluting stent placed 1 month ago
B. 65 year-old female with diabetes & hypertension, both well-controlled on medication, normal kidney function and new onset atrial fibrillation
C. 37 year-old female with end-stage renal disease, on hemodialysis, who has thrombosed her dialysis fistula
D. 54-year-old male with a history of recurrent VTE and labile INR due to non-compliance with warfarin therapy
Patient Case

DOACs
Approved indications & dosing
Efficacy & safety in NVAF & VTE
Lab measurement
Patient selection
Payment challenges and solutions
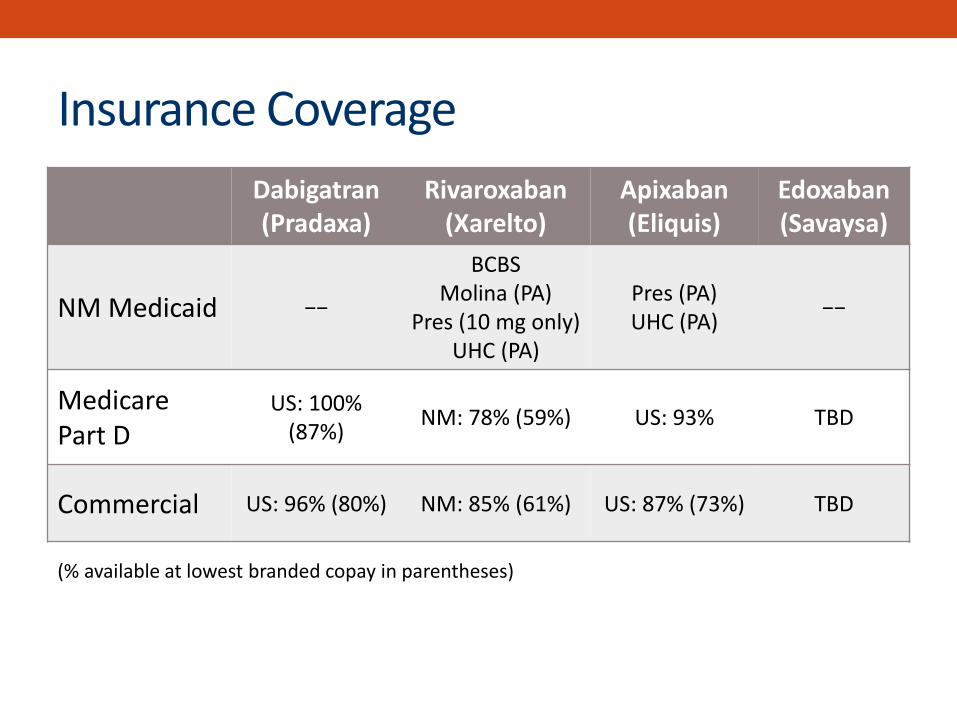
Insurance Coverage
Dabigatran (Pradaxa)
Rivaroxaban (Xarelto)
Apixaban (Eliquis)
Edoxaban (Savaysa)
NM Medicaid −−
BCBS Molina (PA)
Pres (10 mg only) UHC (PA)
Pres (PA) UHC (PA)
−−
Medicare Part D
US: 100% (87%)
NM: 78% (59%) US: 93% TBD
Commercial US: 96% (80%) NM: 85% (61%) US: 87% (73%) TBD
(% available at lowest branded copay in parentheses)

Patient Assistance Programs
Dabigatran (Pradaxa)
Rivaroxaban (Xarelto)
Apixaban (Eliquis)
Edoxaban (Savaysa)
NM Medicaid N/A N/A N/A N/A
Medicare Part D Free 30-day supply card
Free 30-day supply card
Free 30-day supply card
N/A
Commercial $10 copay card
Free 30-day + $5 copay card for 15 mg and
20 mg
Free 30-day + $10 copay card
$4 copay card
Non-insured BIpatient
assistance.com
JJpaf.org: free for those who qualify
(income)
BMSpaf.org: free for those who qualify
(income)
?

DOACs: Advantages
• Improved pharmacokinetic/pharmacodynamic profile
– Rapid onset/offset of action
– Fewer dietary and drug interactions
– Wide therapeutic window allows fixed dosing
– No need for routine monitoring
• Greater convenience and patient satisfaction
• Improved safety profile compared to warfarin
• 20-40% relative risk reduction in major bleeding
• 40-50% relative risk reduction in fatal bleeding
• 60-70% relative risk reduction in intracranial hemorrhage
• Potentially more cost-effective Chai-Adisaksopha, et al. Blood 2014; 124(15):2450-58
Bauer KA. ASH Education Book 2013; 1:464-470 Ruff CT, et al. Lancet 2013; 383 (9921): 955-62
Van Der Hulle T, et al. J Thromb Haemost 2014; 12: 320–8.
DOACs: Disadvantages
• Dose reduction or avoidance in kidney impairment
• Lack of flexibility in dosing
• Limited availability of lab assays to measure anticoagulant effect
• Short half-life mandates strict adherence
• Lack of antidote
• Higher drug acquisition costs and prior authorizations
• Fewer studied/approved indications (e.g. valves, cancer, pregnancy)
Bauer KA. ASH Education Book. 2013;1:464-470. Majeed A, et al. Circulation 2013;128(21):2325-32.
Outline
Review of coagulation cascade
Review of parenteral anticoagulants
Review of oral anticoagulants
Direct oral anticoagulants (DOACs)
Bridging and switching between agents

Steps to Developing a Bridge Plan
1. Develop plan at least 1 week prior to procedure
2. Evaluate bleeding risk of procedure
3. Evaluate patient’s thrombotic risk
4. Timing of cessation and resumption of agent is based on:
a. Patient’s renal function
b. Half-life/onset of agent
c. Type of procedure and anesthesia
Key Question: Does anticoagulation need to be interrupted?
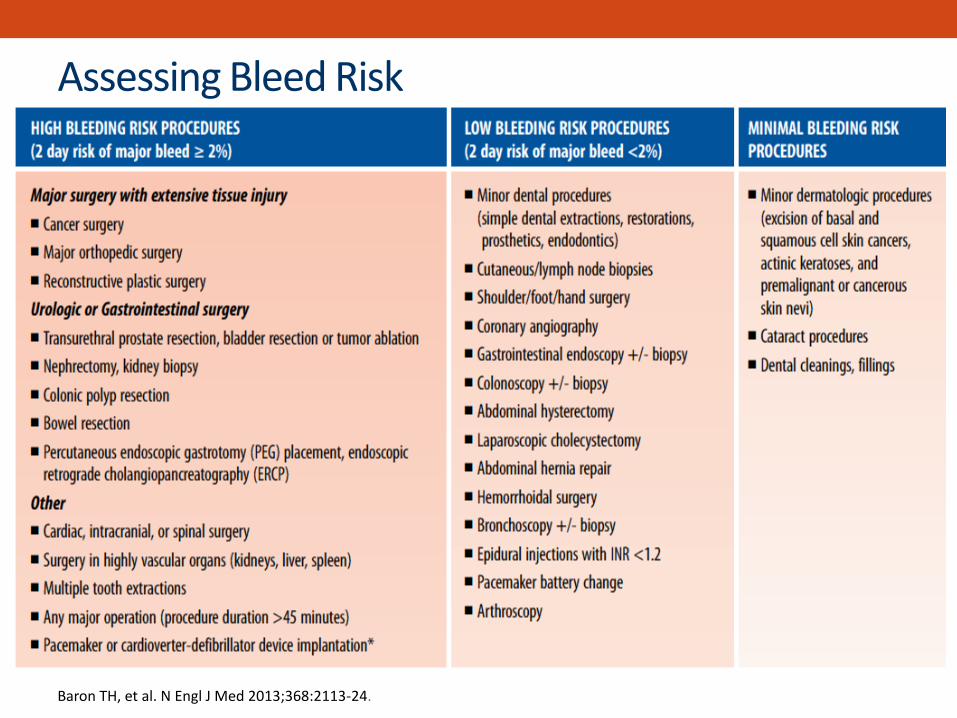
Assessing Bleed Risk
Baron TH, et al. N Engl J Med 2013;368:2113-24.
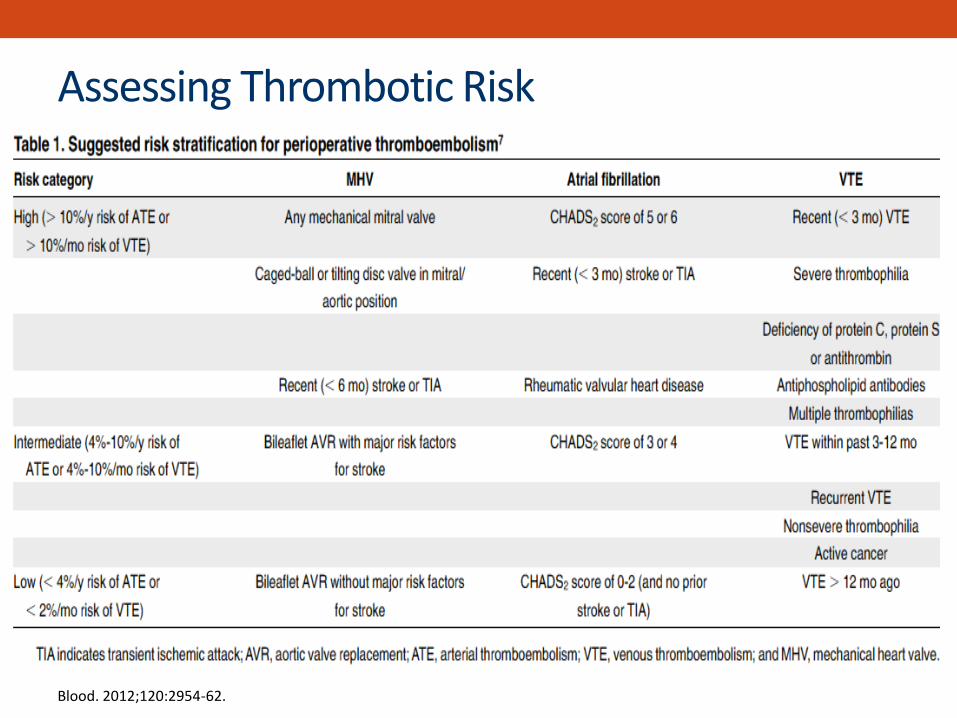
Assessing Thrombotic Risk
Blood. 2012;120:2954-62.
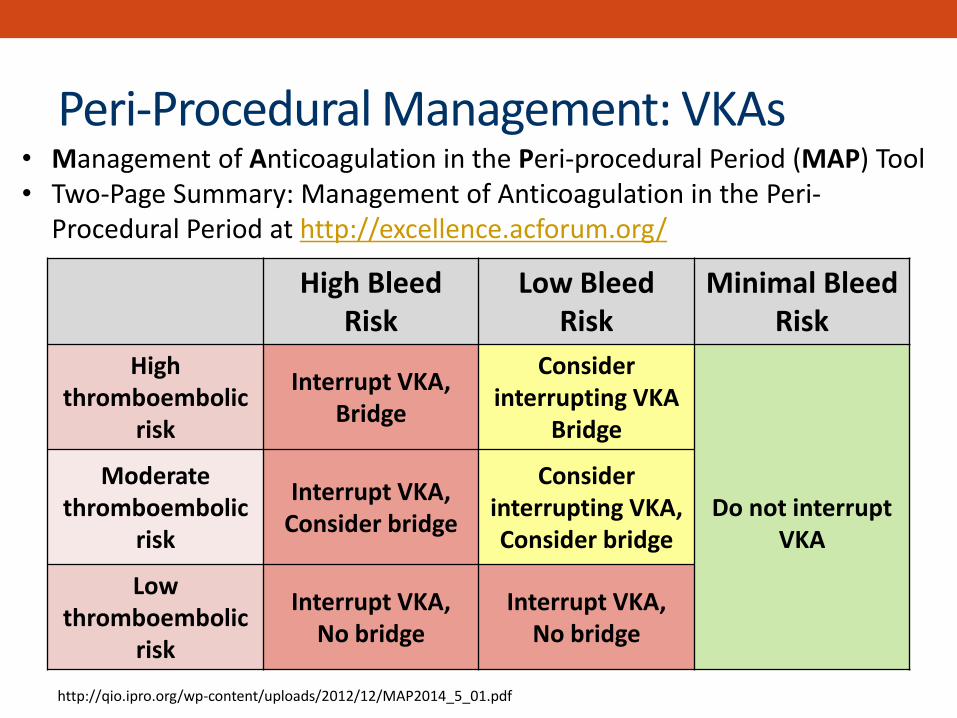
Peri-Procedural Management: VKAs
http://qio.ipro.org/wp-content/uploads/2012/12/MAP2014_5_01.pdf
High Bleed Risk
Low Bleed Risk
Minimal Bleed Risk
High thromboembolic
risk
Interrupt VKA, Bridge
Consider interrupting VKA
Bridge
Do not interrupt
VKA
Moderate thromboembolic
risk
Interrupt VKA, Consider bridge
Consider interrupting VKA, Consider bridge
Low thromboembolic
risk
Interrupt VKA, No bridge
Interrupt VKA, No bridge
• Management of Anticoagulation in the Peri-procedural Period (MAP) Tool • Two-Page Summary: Management of Anticoagulation in the Peri-
Procedural Period at http://excellence.acforum.org/

Peri-Procedural Management: DOACs
Risk Assessment
High Bleed Risk
Low Bleed Risk
Minimal Bleed Risk
High thromboembolic
risk
Interrupt DOAC
Consider interrupting
DOAC
Do not interrupt DOAC
Moderate thromboembolic
risk
Low thromboembolic
risk
Interrupt DOAC
http://qio.ipro.org/wp-content/uploads/2012/12/MAP2014_5_01.pdf
• Management of Anticoagulation in the Peri-procedural Period (MAP) Tool • Two-Page Summary: Management of Anticoagulation in the Peri-
Procedural Period at http://excellence.acforum.org/
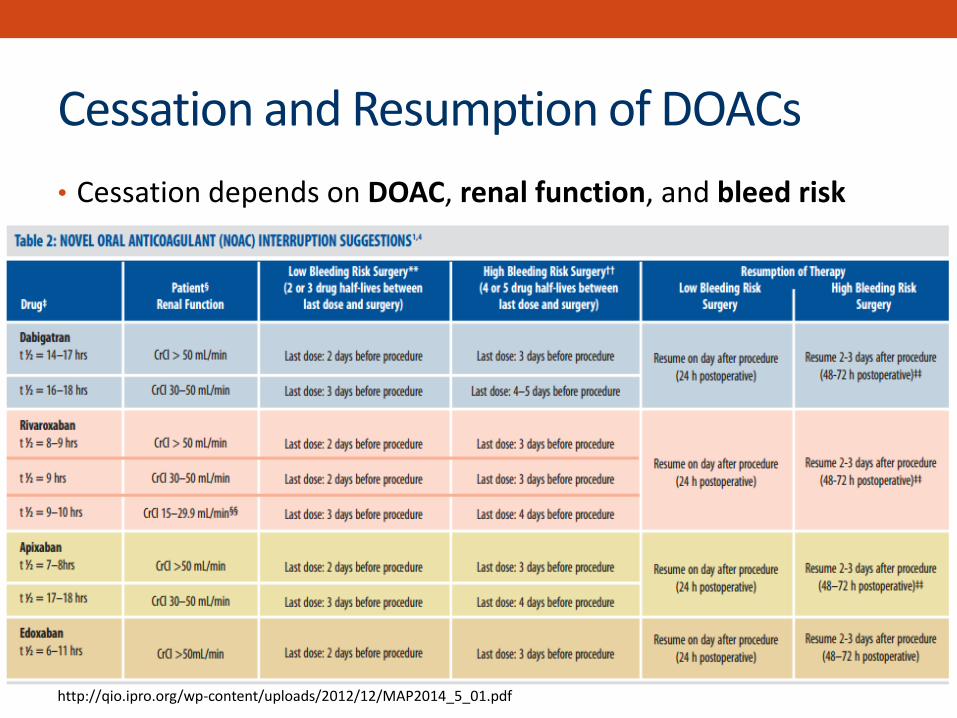
Cessation and Resumption of DOACs
• Cessation depends on DOAC, renal function, and bleed risk
http://qio.ipro.org/wp-content/uploads/2012/12/MAP2014_5_01.pdf
Peri-Procedural Management: DOACs
• Resumption of DOAC – similar to LMWH
• Rapid onset of anticoagulant effect (~1-4 hours)
• Caution with resuming too soon or too aggressively
• May consider “step-up” approach
• Lower or prophylactic dose of DOAC for initial 24-48 hours
• If tolerated, increase to treatment dose DOAC at 48-72 hours
Spyropolous AC, et al. Blood 2012; 120(15): 2954-62.
Switching Between Anticoagulants
• Reason for switching from parenteral to oral anticoagulant
–Facilitate longer-term outpatient management
• Reasons for switching from warfarin to DOAC
–Drug intolerance
–Therapeutic failure
–Patient preference
• Reasons for switching from DOAC to warfarin
–Drug intolerance
–Therapeutic failure
–Patient preference
–New comorbidity or contraindication Abo-Salem E, et al. J Thromb Thrombolysis 2014; 37: 372-79.

• Can place patients at undue risk for bleeding or thrombosis
• Requires a “carefully constructed and thoughtful approach” based on:
• Pharmacokinetic profile of each anticoagulant
• Appropriate laboratory assessment of patient’s coagulation status
• Patient’s renal function
Switching Between Anticoagulants
Abo-Salem E, et al. J Thromb Thrombolysis 2014; 37: 372-79.

• Unfractionated heparin
–Short half-life precludes need for lag time until alternative anticoagulant is initiated
• DOACs and SQ injectables (LMWH, fondaparinux)
– Longer half-life requires lag time until alternative anticoagulant is initiated
–Start alternative anticoagulant when the next dose of original anticoagulant would be due
• Warfarin
–Extremely long half-life requires confirmed offset via INR
–Slow onset may require overlap of rapid-acting anticoagulant
Switching Between Anticoagulants
Abo-Salem E, et al. J Thromb Thrombolysis 2014; 37: 372-79.

Abo-Salem E, et al. J Thromb Thrombolysis 2014; 37: 372-79.
Switching Between Anticoagulants

Switching Between Anticoagulants
Abo-Salem E, et al. J Thromb Thrombolysis 2014; 37: 372-79.

• DOACs are a viable alternative to
traditional anticoagulants in
appropriately selected patients
– Equal or better efficacy for
VTE treatment and stroke
prevention in NVAF
– Improved safety profile
compared to warfarin
– Significant reduction in major,
fatal, intracranial hemorrhage
– GIB caution: dabigatran and
rivaroxaban
DOAC Summary
• Optimal use of DOACs requires
familiarity with:
–Pharmacokinetic/dynamic
profiles
–Dosing strategies
– Lab measurement
–Peri-procedural strategies
–Switching between agents
–Bleed management
–Reversal strategies

AC Forum- Centers of Excellence
http://excellence.acforum.org/