powerpoint slides english brazilian portuguese translation ... · and a nice place to begin is with...
TRANSCRIPT

1
PowerPoint Slides English Brazilian Portuguese Translation
Cancer-related Fatigue and Sleep Disorders Video Transcript
Fadiga e transtornos do sono relacionados ao câncer Transcrição de vídeo
Professional Oncology Education Cancer-related Fatigue and Sleep Disorders Time: 29:49
Educação Profissional em Oncologia Fadiga e transtornos do sono relacionados ao câncer Duração: 29:49
Ellen F. Manzullo, M.D. Professor, General Internal Medicine, Ambulatory Treatment and Emergency Care The University of Texas MD Anderson Cancer Center
Dra. Ellen F. Manzullo, M.D. Professora, Medicina Interna Geral, Tratamento Ambulatório e Cuidado de Emergência MD Anderson Cancer Center – Universidade do Texas
I’m Dr. Ellen Manzullo and I’m a professor of Medicine here at the University of Texas MD Anderson Cancer Center and I am going to be talking with you regarding cancer-related fatigue and sleep disorders
Eu sou a Dra. Ellen Manzullo e sou professora de Medicina aqui, no MD Anderson Cancer Center da Universidade do Texas, e vou falar sobre fadiga relacionada ao câncer e transtornos do sono.
2
And a nice place to begin is with the accepted definition of cancer-related fatigue.
Um bom ponto para começar é com a definição aceita de fadiga relacionada ao câncer.
The definition of cancer-related fatigue is that it’s a distressing, persistent, subjective sense of tiredness or exhaustion related to cancer or cancer treatment that is not proportional to recent activity and it interferes with usual functioning.
A fadiga relacionada ao câncer é definida como a sensação de cansaço ou exaustão angustiante, persistente e subjetiva relacionada ao câncer ou ao tratamento antineoplásico que não é proporcional às atividades recentes e interfere com a funcionalidade usual.
3
Now it’s important to keep in mind several characteristics of cancer-related fatigue. Cancer-related fatigue is really a multidimensional symptom and it can encompass not only physical aspects, but also mental, and emotional aspects. And in addition it can really occur anywhere along the spectrum of cancer care. And up to 30% of cancer survivors have been reported to have a loss of energy years after they have completed their treatment.
É importante levar em consideração várias características da fadiga relacionada ao câncer. A fadiga relacionada ao câncer é, de fato, um sintoma multidimensional e pode abranger aspectos não apenas físicos, mas mentais e emocionais. Além do mais, pode ocorrer em qualquer ponto dos diversos âmbitos de atenção ao câncer. Foi relatado que até 30% dos sobreviventes de câncer tiveram perda de energia anos após completaram seu tratamento.
Now there’s really several barriers to both the assessment and treatment of this symptom, which is really the most common and most distressing symptom in our patient population. The first is that there are naturally time constraints in a busy outpatient practice. Physicians are very busy as well as nurse practitioners in the outpatient setting and that is not really at times conducive regarding asking the patient about this symptom. In addition, many times patients are reluctant to mention fatigue. They don’t want to be perceived as a complainer and also there’s concern that if they mention that they’re having fatigue that this potentially could have an impact on their cancer treatment. Also, another important barrier is that many times physicians feel uncomfortable discussing this symptom simply due to a lack of knowledge in this area. And then finally some patients just think that this is an expected outcome of their cancer and cancer treatment and they just don't mention this during their clinic visit. So, these are all several really important barriers to both the assessment and treatment of cancer-related fatigue.
Contudo, há diversas barreiras contra a avaliação e o tratamento desse sintoma, que, na verdade, é o sintoma mais comum e mais angustiante em nossa população de pacientes. A primeira é que há, naturalmente, limitações de tempo em consultórios muito ocupados. Médicos e enfermeiras especialistas estão muito ocupados no setor de atendimento ambulatorial, o que, às vezes, não é conducente a perguntar ao paciente sobre esse sintoma. Além do mais, muitas vezes, os pacientes relutam em mencionar a fadiga. Eles não querem ser percebidos como pessoas que só se queixam e também se preocupam com o possível impacto no seu tratamento contra o câncer caso mencionem sentir fadiga. Além disso, outra barreira importante é que, às vezes, muitos médicos não se sentem à vontade para discutir sobre este sintoma simplesmente por não terem conhecimento nesta área. E, finalmente, alguns pacientes somente pensam que é um resultado esperado do câncer e do tratamento contra o câncer e simplesmente nem falam disso durante as consultas na clínica. Todas essas diversas barreiras são muito importantes para a avaliação e o tratamento da fadiga relacionada ao câncer.
4
When we look at the causes of cancer-related fatigue, there are really many important factors. And it’s important to keep in mind that cancer-related fatigue also correlates with decreased daytime activity and also increased nocturnal wakefulness. Some of the important causes of cancer-related fatigue are: the cancer treatment that the patient is undergoing as well as comorbid conditions that the patient has, such as hypothyroidism; and what I will be discussing later, sleep disorders. Also --- we also want to keep in mind patient’s medications can also contribute to the fatigue they’re experiencing. And then some also important causes are poor nutrition as well as symptoms that normally cluster, or can potentially cluster with fatigue, such as pain, anxiety, depression. And so I will be going over all of these potential causes of cancer-related fatigue to begin with.
Quando examinamos as causas da fadiga relacionada ao câncer, [constatamos que] há muitos fatores importantes. É importante levar em consideração que a fadiga relacionada ao câncer também se correlaciona com a redução das atividades diurnas e o aumento da vigília noturna. Algumas das causas importantes de fadiga relacionada ao câncer são: o tratamento antineoplásico que o paciente recebe, bem como comorbidades de que o paciente padece, como hipotireoidismo, e os que discutirei depois, os transtornos do sono. Além disso, devemos lembrar que os medicamentos do paciente também podem contribuir à fadiga que sentem. Outras causas importantes também seriam a má nutrição e sintomas que normalmente se agrupam, ou que potencialmente podem se agrupar com a fadiga, como a dor, a ansiedade, a depressão. Começarei discorrendo sobre todas essas possíveis causas da fadiga relacionada ao câncer.
Nutritional im --- imbalances is an important one and the patients can experience weight changes as they undergo their cancer treatment. And it’s important to keep in mind that it could be that they gain weight as well as lose weight. Patients commonly think that since they have a cancer diagnosis and they’re undergoing treatment for their cancer, that they will lose weight. But we have found, in certain patient populations, this is not the case at all. And, in fact, patients can also have a significant weight gain and this can also have an impact on their symptom of fatigue. Also, we keep in mind that patients can have motility disorders, particularly in our diabetic patients. And also patients as they are actively undergoing their cancer treatment, they can experience significant nausea, vomiting, diarrhea, all of this which has a negative impact on their nutrition. And then as a result they can also develop fluid and electrolyte imbalances and, for example, have decreases in their potassium and magnesium. So in addition to these nutritional imbalances, another important factor is: patients can experience physical function changes. Many times, as they’re undergoing their chemotherapy or radiotherapy, they will have
O desequilíbrio nutricional é uma [causa] importante e os pacientes podem experimentar mudanças no seu peso durante o tratamento contra o câncer. É importante observar que eles tanto ganham quanto perdem peso. Normalmente, os pacientes pensam que, por terem diagnóstico de câncer e estarem recebendo tratamentos contra o câncer, perderão peso. Mas descobrimos que, em certas populações de pacientes, esse não é o caso. Aliás, os pacientes também podem ter um ganho significativo de peso e isto também pode ter impacto no sintoma de fadiga. Também, levamos em consideração que os pacientes podem apresentar transtornos de motilidade, sobretudo nos pacientes diabéticos. E, durante o período ativo do tratamento contra o câncer, os pacientes podem experimentar náusea, vômito e diarreia significativos. Tudo isto, por sinal, tem impacto negativo em sua nutrição. Consequentemente, eles também podem apresentar desequilíbrios hídrico e eletrolítico e, por exemplo, apresentar redução [nas concentrações] de potássio e magnésio. Além desses desequilíbrios nutricionais, outro fator importante é a alteração nas funções físicas dos pacientes. Muitas vezes, quando são submetidos a quimioterapia ou radioterapia,

5
decreased physical activity and they will subsequently have decreased physical conditioning. This is why, in many times when we see patients in our cancer-related fatigue, one of the first interventions that we talk to patients about is exercise, telling them the recommendations for all of us is to try to get 30 minutes of exercise on a daily basis, provided that they don’t have any specific limitations as a result of their cancer or their cancer treatment.
apresentam diminuição da atividade física e subsequente diminuição do condicionamento físico. Isto é por que, muitas vezes quando examinamos pacientes com fadiga relacionada ao câncer, uma das primeiras intervenções sobre as quais conversamos com eles é o exercício. Dizemos que as recomendações para todos nós é tentar praticar 30 minutos de exercício por dia, desde que não haja nenhuma limitação específica decorrente do câncer ou do tratamento.
Cancer treatments also interfere – or are related to cancer-related fatigue and I have listed here simply all the potential cancer treatments that a patient can be undergoing, such as chemotherapy, radiation therapy, surgery, bone marrow transplantation, biologic response modifiers, as well as hormonal treatments.
Os tratamentos contra o câncer também interferem com a fadiga relacionada ao câncer ou se relacionam a ela. Eu indiquei aqui simplesmente todos os possíveis tratamentos de câncer aos que um paciente pode se submeter, como quimioterapia, radioterapia, cirurgia, transplante de medula óssea, modificadores de resposta biológica, bem como tratamentos hormonais.
Medications are also a very important factor to keep in mind when evaluating a patient with cancer-related fatigue. And a couple of examples would be, for example, beta-blockers the patients might be on, for the control of hypertension or for some underlying cardiac disease. In addition, patients can be on sedating agents that could contribute to their fatigue. It’s important to keep in mind that there are normally symptoms that cluster with fatigue. And some of the most common symptoms that cluster with fatigue are, for example, pain, anxiety, depression, and what we will be focusing on later on, sleep disorders. And that’s why we always evaluate our patients when we initially see them in our cancer-related fatigue clinic for these symptoms by having them complete questionnaires.
Os medicamentos também são um fator muito importante que devemos ter em mente ao avaliar um paciente com fadiga relacionada ao câncer. Alguns exemplos seriam, por exemplo, os beta bloqueadores que os pacientes talvez estejam recebendo para o controle da hipertensão ou para alguma doença cardíaca subjacente. Além disso, os pacientes podem estar recebendo sedativos que poderiam contribuir à fadiga que sentem. É importante observar que, normalmente, há sintomas que se agrupam com a fadiga. Alguns dos sintomas mais comuns que se agrupam com a fadiga são, por exemplo, a dor, a ansiedade, a depressão e os que focaremos depois: os transtornos do sono. Essa é a razão pela qual sempre avaliamos os pacientes com relação a esses sintomas, por meio de questionários, quando os examinamos inicialmente em nossa clínica de fadiga relacionada ao câncer.
6
Comorbid conditions are also a very important factor to keep in mind when patients are being rel --- evaluated for cancer-related fatigue. For example, anemia: patients when they have a hemoglobin lab --- level usually of 10 or less, they will begin to experience some level of fatigue; also patients with neurologic disorders as well as cardiac dysfunction. It’s important when we evaluate a patient for fatigue to also make certain that they don’t have, for example, an underlying cardiac disorder that could be contributing or could be actually the cause of their fatigue. We also evaluate patients for pulmonary disorders, hepatic disorders, renal dysfunction, rheumatologic disorders. In particular patients with fibromyalgia can experience fatigue, and this is very important to keep in mind. And then of course infectious processes, especially if a patient, for example, is having fever and or requiring --- and is requiring antibiotic therapy this also can impact their fatigue. Finally, endocrine disorders are also very important to keep in mind when evaluating patients for fatigue and, in particular, hypothyroidism, as well as hypogonadism, and adrenal insufficiency. These are three common dis --- endocrine disorders that can have a potential impact on the patient’s fatigue.
As condições de comorbidade também são um fator muito importante das quais devemos ter presente quando os pacientes forem reavaliados para a fadiga relacionada ao câncer. Por exemplo, a anemia: quando os resultados dos exames de laboratório de hemoglobina dos pacientes forem iguais ou superiores a 10, eles começarão a sentir um pouco de fadiga; também, pacientes com transtornos neurológicos, bem como disfunção cardíaca. Quando avaliamos um paciente quanto a fadiga, também é importante verificar se não têm, por exemplo, um transtorno cardíaco subjacente que poderia estar contribuindo para a fadiga ou que poderia ser a causa da fadiga. Além disso, avaliamos pacientes quanto a transtornos pulmonares, transtornos hepáticos, disfunção renal, transtornos reumáticos. Especialmente, os pacientes com fibromialgia podem sentir fadiga, e isto é muito importante ter presente. E, é claro, os processos infeciosos, especialmente se um paciente, por exemplo, tiver febre e precisar de terapia antibiótica, isto também poderá influenciar a fadiga. Finalmente, é muito importante considerar os transtornos endócrinos na avaliação de pacientes para fadiga, especialmente, o hipotireoidismo, bem como o hipogonadismo e a insuficiência adrenal. Esses são três transtornos endócrinos comuns que podem ter um impacto na fadiga do paciente.
As far as interventions that are useful for patients with their cancer-related fatigue, a nice way of thinking about it, is that there are non-pharmacologic interventions as well as pharmacologic interventions. Non-pharmacologic interventions would be, for example, psychosocial interventions. As I mentioned previously, exercise is something which is very important and patients many times will sa --- will question how can we ask them to exercise when they are so fatigued? But actually there have been some studies that have been performed in certain patient populations, which have suggested that exercise, with the eventual goal of getting to 30 minutes of exercise a day, can have a very positive impact on the patients’ level of fatigue and decrease the level of their fatigue. Sleep therapy is another very important non-pharmacologic intervention, and this particular relates to sleep hygiene. Patients need to be
No que se refere a intervenções úteis para pacientes com fadiga relacionada ao câncer, uma boa maneira de se pensar sobre o assunto é que existem intervenções não farmacológicas e intervenções farmacológicas. As intervenções não farmacológicos seriam, por exemplo, as intervenções psicossociais. Como mencionei antes, o exercício é muito importante mas, muitas vezes, os pacientes questionam quando lhes pedimos para fazer exercícios já que se sentem tão cansados. Mas, na realidade, em alguns estudos realizados com certas populações de pacientes foi sugerido que o exercício, com a meta final de 30 minutos de exercício por dia, pode ter um impacto muito positivo no grau de fadiga dos pacientes e diminuir o grau de fadiga. A terapia do sono é outra intervenção não farmacológica muito importante, e especificamente está relacionada à higiene do sono. Os pacientes devem ser
7
counseled on the importance of trying to go to bed at the same time every day of the week, getting up at the same time, trying to restrict their bedtime just to simply going to bed and turning off the TV, so that they don’t have any sort of distractions while they are preparing for bed. And then another important non-pharmacologic intervention is acupuncture. Some pharmacologic interventions that have been --- that are being studied, and as well have been used in the past, are stimulant therapy, such as modafinil. Patients can have some improvement in their fatigue with this intervention. However, we pre --- prior to going ahead and prescribing this, we make sure to do a complete history and physical exam on the patient to make certain that there are not any contraindications to the use of these medications. Also antidepressants at times can be helpful. For example, if a patient really is having significant depression, which could be contributing to their fatigue. And then, in some patient populations, steroid therapy is helpful, but temp --- typically this is more in a palliative care setting and this is really not commonly used for the purpose of just cancer-related fatigue.
aconselhados sobre a importância de tentar dormir ao mesmo tempo todos os dias da semana, levantar-se ao mesmo tempo, tentar limitar a hora de dormir a simplesmente ir para a cama e desligar a televisão, de modo a não ter nenhum tipo de distração quando se preparam para ir dormir. Outra intervenção não farmacológica importante é a acupuntura. As intervenções farmacológicas que foram... que estão sendo estudadas, e que também eram utilizadas antes, são as terapias estimulantes, como o modafinila. A fadiga dos pacientes pode melhorar um pouco com esta intervenção. Contudo, antes de ir em frente e prescrevê-la, sempre fazemos uma anamnese e exame físico completos no paciente para verificar se não há nenhuma contraindicação ao uso desses medicamentos. Os antidepressivos também podem ser úteis às vezes. Por exemplo, quando um paciente sofre de depressão significativa que poderia estar contribuindo para a fadiga. E, depois, em algumas populações de pacientes, a terapia com esteroides é útil, mas isto é mais comum em ambientes de cuidado paliativo e não é tão utilizado com o objetivo de tratar somente a fadiga relacionada ao câncer.
So it’s important to not only define cancer-related fatigue, which I have already done, but it’s also to be --- it’s important to have a good definition for a sleep disorder. And a simple definition is that a sleep disorder is defined as any disorder that affects, disrupts, or involves sleep
Por isso, é importante não apenas definir a fadiga relacionada ao câncer, o que já fiz, mas também é importante ter uma definição boa para o transtorno do sono. Uma definição simples seria que o transtorno do sono é qualquer transtorno que afeta, transtorna, ou implica o sono
8
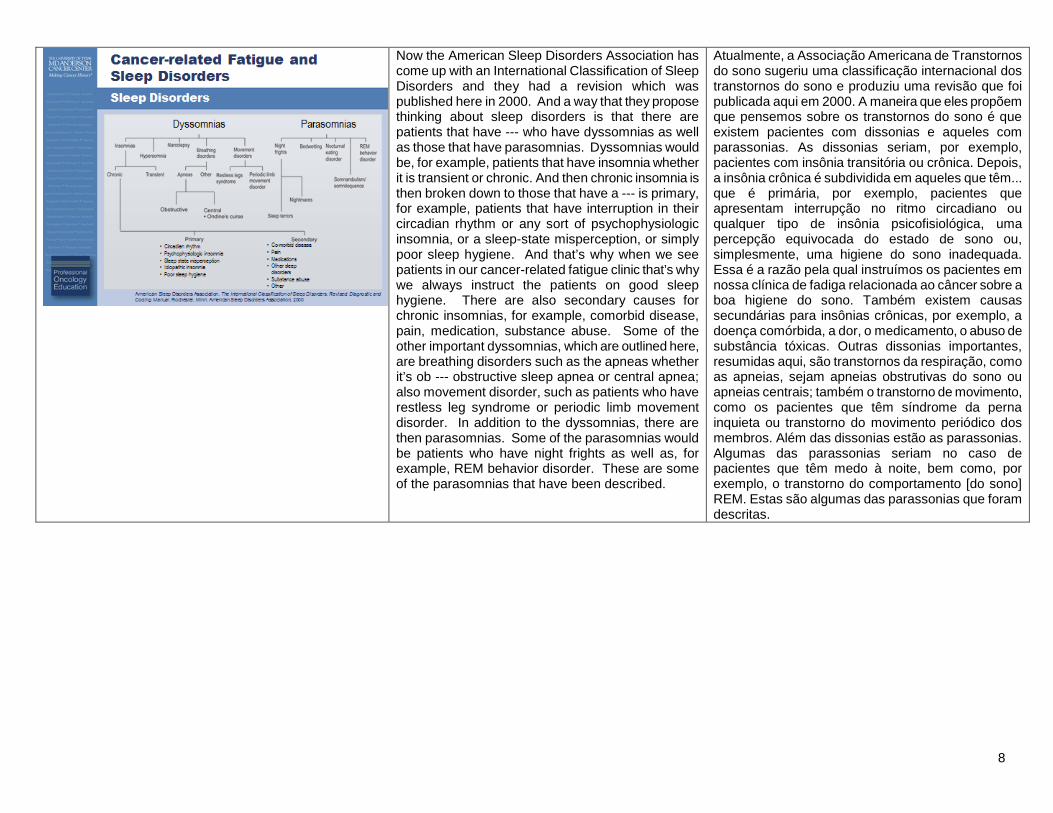
Now the American Sleep Disorders Association has come up with an International Classification of Sleep Disorders and they had a revision which was published here in 2000. And a way that they propose thinking about sleep disorders is that there are patients that have --- who have dyssomnias as well as those that have parasomnias. Dyssomnias would be, for example, patients that have insomnia whether it is transient or chronic. And then chronic insomnia is then broken down to those that have a --- is primary, for example, patients that have interruption in their circadian rhythm or any sort of psychophysiologic insomnia, or a sleep-state misperception, or simply poor sleep hygiene. And that’s why when we see patients in our cancer-related fatigue clinic that’s why we always instruct the patients on good sleep hygiene. There are also secondary causes for chronic insomnias, for example, comorbid disease, pain, medication, substance abuse. Some of the other important dyssomnias, which are outlined here, are breathing disorders such as the apneas whether it’s ob --- obstructive sleep apnea or central apnea; also movement disorder, such as patients who have restless leg syndrome or periodic limb movement disorder. In addition to the dyssomnias, there are then parasomnias. Some of the parasomnias would be patients who have night frights as well as, for example, REM behavior disorder. These are some of the parasomnias that have been described.
Atualmente, a Associação Americana de Transtornos do sono sugeriu uma classificação internacional dos transtornos do sono e produziu uma revisão que foi publicada aqui em 2000. A maneira que eles propõem que pensemos sobre os transtornos do sono é que existem pacientes com dissonias e aqueles com parassonias. As dissonias seriam, por exemplo, pacientes com insônia transitória ou crônica. Depois, a insônia crônica é subdividida em aqueles que têm... que é primária, por exemplo, pacientes que apresentam interrupção no ritmo circadiano ou qualquer tipo de insônia psicofisiológica, uma percepção equivocada do estado de sono ou, simplesmente, uma higiene do sono inadequada. Essa é a razão pela qual instruímos os pacientes em nossa clínica de fadiga relacionada ao câncer sobre a boa higiene do sono. Também existem causas secundárias para insônias crônicas, por exemplo, a doença comórbida, a dor, o medicamento, o abuso de substância tóxicas. Outras dissonias importantes, resumidas aqui, são transtornos da respiração, como as apneias, sejam apneias obstrutivas do sono ou apneias centrais; também o transtorno de movimento, como os pacientes que têm síndrome da perna inquieta ou transtorno do movimento periódico dos membros. Além das dissonias estão as parassonias. Algumas das parassonias seriam no caso de pacientes que têm medo à noite, bem como, por exemplo, o transtorno do comportamento [do sono] REM. Estas são algumas das parassonias que foram descritas.
9
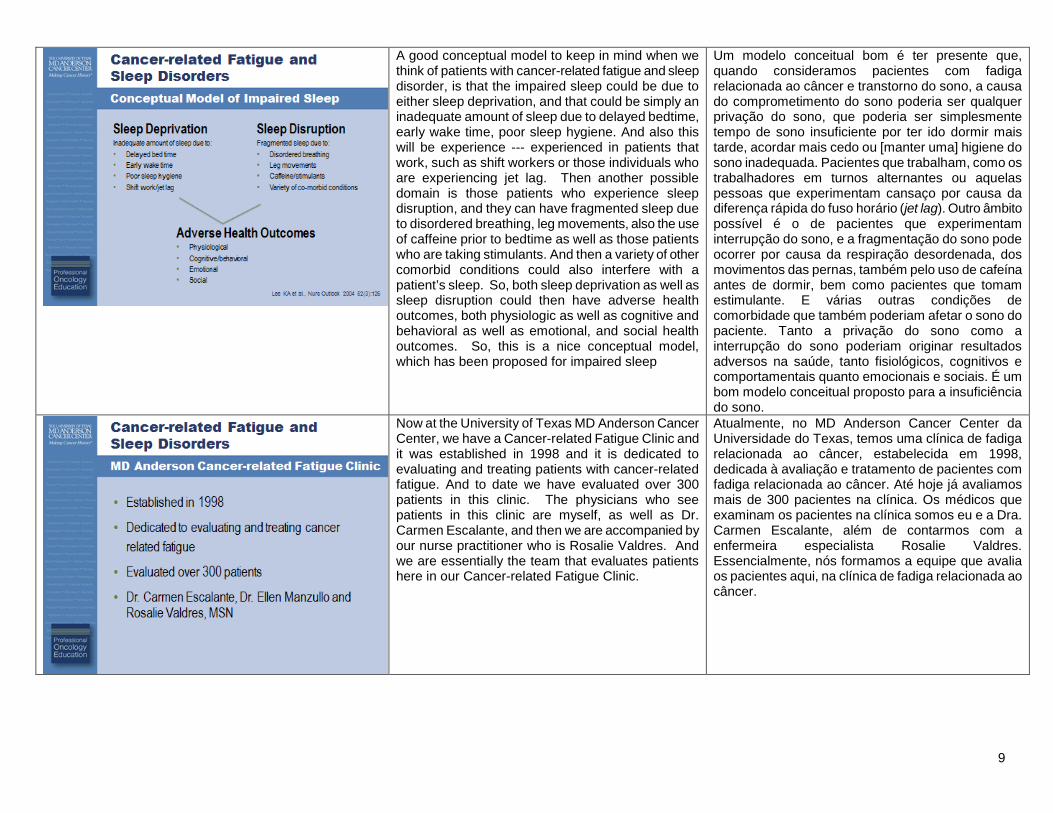
A good conceptual model to keep in mind when we think of patients with cancer-related fatigue and sleep disorder, is that the impaired sleep could be due to either sleep deprivation, and that could be simply an inadequate amount of sleep due to delayed bedtime, early wake time, poor sleep hygiene. And also this will be experience --- experienced in patients that work, such as shift workers or those individuals who are experiencing jet lag. Then another possible domain is those patients who experience sleep disruption, and they can have fragmented sleep due to disordered breathing, leg movements, also the use of caffeine prior to bedtime as well as those patients who are taking stimulants. And then a variety of other comorbid conditions could also interfere with a patient’s sleep. So, both sleep deprivation as well as sleep disruption could then have adverse health outcomes, both physiologic as well as cognitive and behavioral as well as emotional, and social health outcomes. So, this is a nice conceptual model, which has been proposed for impaired sleep
Um modelo conceitual bom é ter presente que, quando consideramos pacientes com fadiga relacionada ao câncer e transtorno do sono, a causa do comprometimento do sono poderia ser qualquer privação do sono, que poderia ser simplesmente tempo de sono insuficiente por ter ido dormir mais tarde, acordar mais cedo ou [manter uma] higiene do sono inadequada. Pacientes que trabalham, como os trabalhadores em turnos alternantes ou aquelas pessoas que experimentam cansaço por causa da diferença rápida do fuso horário (jet lag). Outro âmbito possível é o de pacientes que experimentam interrupção do sono, e a fragmentação do sono pode ocorrer por causa da respiração desordenada, dos movimentos das pernas, também pelo uso de cafeína antes de dormir, bem como pacientes que tomam estimulante. E várias outras condições de comorbidade que também poderiam afetar o sono do paciente. Tanto a privação do sono como a interrupção do sono poderiam originar resultados adversos na saúde, tanto fisiológicos, cognitivos e comportamentais quanto emocionais e sociais. É um bom modelo conceitual proposto para a insuficiência do sono.
Now at the University of Texas MD Anderson Cancer Center, we have a Cancer-related Fatigue Clinic and it was established in 1998 and it is dedicated to evaluating and treating patients with cancer-related fatigue. And to date we have evaluated over 300 patients in this clinic. The physicians who see patients in this clinic are myself, as well as Dr. Carmen Escalante, and then we are accompanied by our nurse practitioner who is Rosalie Valdres. And we are essentially the team that evaluates patients here in our Cancer-related Fatigue Clinic.
Atualmente, no MD Anderson Cancer Center da Universidade do Texas, temos uma clínica de fadiga relacionada ao câncer, estabelecida em 1998, dedicada à avaliação e tratamento de pacientes com fadiga relacionada ao câncer. Até hoje já avaliamos mais de 300 pacientes na clínica. Os médicos que examinam os pacientes na clínica somos eu e a Dra. Carmen Escalante, além de contarmos com a enfermeira especialista Rosalie Valdres. Essencialmente, nós formamos a equipe que avalia os pacientes aqui, na clínica de fadiga relacionada ao câncer.
10
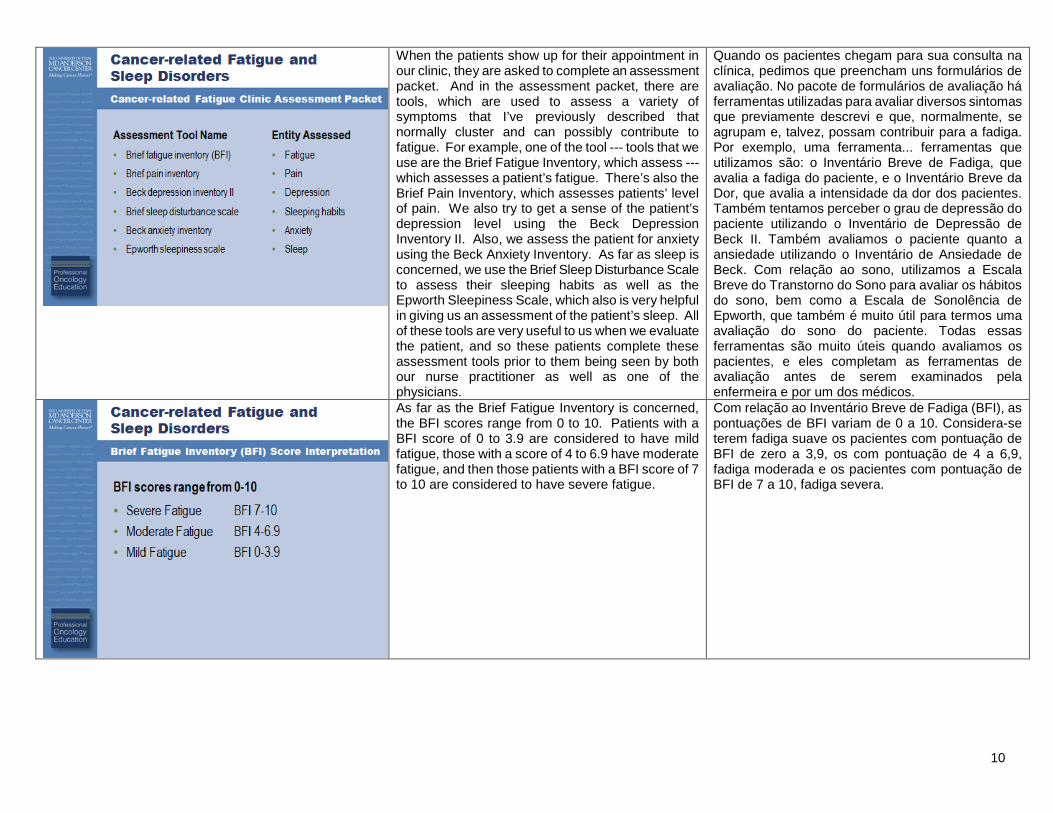
When the patients show up for their appointment in our clinic, they are asked to complete an assessment packet. And in the assessment packet, there are tools, which are used to assess a variety of symptoms that I’ve previously described that normally cluster and can possibly contribute to fatigue. For example, one of the tool --- tools that we use are the Brief Fatigue Inventory, which assess --- which assesses a patient’s fatigue. There’s also the Brief Pain Inventory, which assesses patients’ level of pain. We also try to get a sense of the patient’s depression level using the Beck Depression Inventory II. Also, we assess the patient for anxiety using the Beck Anxiety Inventory. As far as sleep is concerned, we use the Brief Sleep Disturbance Scale to assess their sleeping habits as well as the Epworth Sleepiness Scale, which also is very helpful in giving us an assessment of the patient’s sleep. All of these tools are very useful to us when we evaluate the patient, and so these patients complete these assessment tools prior to them being seen by both our nurse practitioner as well as one of the physicians.
Quando os pacientes chegam para sua consulta na clínica, pedimos que preencham uns formulários de avaliação. No pacote de formulários de avaliação há ferramentas utilizadas para avaliar diversos sintomas que previamente descrevi e que, normalmente, se agrupam e, talvez, possam contribuir para a fadiga. Por exemplo, uma ferramenta... ferramentas que utilizamos são: o Inventário Breve de Fadiga, que avalia a fadiga do paciente, e o Inventário Breve da Dor, que avalia a intensidade da dor dos pacientes. Também tentamos perceber o grau de depressão do paciente utilizando o Inventário de Depressão de Beck II. Também avaliamos o paciente quanto a ansiedade utilizando o Inventário de Ansiedade de Beck. Com relação ao sono, utilizamos a Escala Breve do Transtorno do Sono para avaliar os hábitos do sono, bem como a Escala de Sonolência de Epworth, que também é muito útil para termos uma avaliação do sono do paciente. Todas essas ferramentas são muito úteis quando avaliamos os pacientes, e eles completam as ferramentas de avaliação antes de serem examinados pela enfermeira e por um dos médicos.
As far as the Brief Fatigue Inventory is concerned, the BFI scores range from 0 to 10. Patients with a BFI score of 0 to 3.9 are considered to have mild fatigue, those with a score of 4 to 6.9 have moderate fatigue, and then those patients with a BFI score of 7 to 10 are considered to have severe fatigue.
Com relação ao Inventário Breve de Fadiga (BFI), as pontuações de BFI variam de 0 a 10. Considera-se terem fadiga suave os pacientes com pontuação de BFI de zero a 3,9, os com pontuação de 4 a 6,9, fadiga moderada e os pacientes com pontuação de BFI de 7 a 10, fadiga severa.

11
As mentioned previously, we use the Brief Sleep Disturbance Scale. And this is used to assess the patient’s sleeping habits, and it’s broken down to those patients who score with a mild sleep disturbance, who have a score of 22 to 29; and that ranges to those patients who are considered to have a severe sleep disturbance and those patients will have a score of greater than 35.
Como mencionei antes, utilizamos a Escala Breve do Transtorno do Sono. Ela é utilizada para avaliar os hábitos de sono do paciente e é subdividida para aqueles pacientes com pontuação indicativa de um transtorno leve do sono, com pontuação de 22 a 29 e abrange pacientes que padecem de um transtorno grave do sono e os com pontuação acima de 35.
We also use the Epworth Sleepiness Scale. Now this is used to measure excessive daytime sleepiness; and it’s primarily been evaluated --- it’s primarily validated in patients with obstructive sleep apnea and the average score for the normal population is 0 to 9. And patients that have a score of anywhere usually above 10, a sleep specialist is recommended.
Nós também utilizamos a Escala de Sonolência de Epworth. Ela é utilizada para medir o excesso de sonolência diurna e é validada principalmente em pacientes com apneia obstrutiva do sono, e a pontuação média para a população normal é de 0 a 9. Geralmente, para pacientes com pontuação acima de 10, recomendamos [consultar] um especialista do sono.
12
We are fortunate here at the University of Texas MD Anderson Cancer Center not only to have our Fa---clinic focused on cancer-related fatigue, but we also have a Sleep Center. Now our Sleep Center was opened in September of 2006 and today greater than 600 sleep studies have been performed. With our Sleep Center, we have three board-certified sleep technologists as well as three board-certified sleep physicians, who are Dr. David Balachandran, Dr. Lara Bashoura, and Dr. Saadia Faiz.
Aqui no MD Anderson Cancer Center da Universidade do Texas temos sorte de contar não apenas com uma clínica dedicada à fadiga relacionada ao câncer, mas também com um Centro do Sono. O Centro do Sono foi aberto em setembro de 2006 e, atualmente, mais de 600 estudos sobre sono foram realizados. Com o Centro do Sono, temos três tecnologistas do sono credenciados, bem como três médicos especialistas em sono credenciados, que são o Dr. David Balachandran, a Dra. Lara Bashoura e a Dra. Saadia Faiz.
And so, we are in a very unique position here at our institution to be able to evaluate the relationship between cancer-related fatigue and sleep disorders.
Por isso, estamos em uma posição privilegiada em nossa instituição ao podermos avaliar a relação entre a fadiga relacionada ao câncer e os transtornos do sono.

13
And so, physicians in both the Department[s] of General Internal Medicine, Ambulatory Treatment and Emergency Care as well as physicians in this Sleep Center began to ask the question, “What is the relationship between sleep disorders and fatigue in cancer patients?” And actually this resulted in our initial sleep disorder study.
Os médicos dos Departamentos de Medicina Interna Geral e de Tratamento Ambulatorial e Cuidados de Emergência, bem como os médicos do Centro do Sono começaram a se perguntar: “Qual é a relação entre os transtornos do sono e a fadiga em pacientes com câncer?” E, na verdade, isso resultou em nosso estudo inicial de transtornos do sono.
And we performed a retrospective study and we looked at the patients who were evaluated in the Cancer-related Fatigue Clinic, and the study period that we used was September 1, 2006, to May 31, 2008. And we identified patients who were referred by the Cancer-related Fatigue Clinic for a sleep consult. We --- reviewed patient demographic information as well as clinical factors. And then we did a review of the symptom status data. And the symptom --- symptom status data came from the results of the assessment tools they completed prior to their initial consult visit in our clinic. And those symptoms, which I prior --- mentioned prior, are, for example, pain, sleep disorders, depression, and anxiety. In this study, we also determined if patients had a sleep study completed and then we reviewed the results of the sleep study.
Realizamos um estudo retrospectivo e examinamos pacientes que tinham sido avaliados na Clínica de Fadiga Relacionada ao Câncer, e o período de estudo que usamos foi de 1o de setembro de 2006 a 31 de maio de 2008. Identificamos pacientes que tinham sido encaminhados pela Clínica de Fadiga Relacionada ao Câncer para uma consulta sobre sono. Revimos as informações demográficas dos pacientes e fatores clínicos. Depois, fizemos uma revisão dos dados do estado dos sintomas. Os dados do estado dos sintomas provieram dos resultados das ferramentas de avaliação que eles tinham preenchido antes de sua consulta inicial em nossa clínica. Os sintomas, que tinha mencionado antes, são, por exemplo, dor, transtornos do sono, depressão e ansiedade. Nesse estudo, também determinamos se os pacientes tinham concluído um estudo do sono e examinamos os resultados.
14
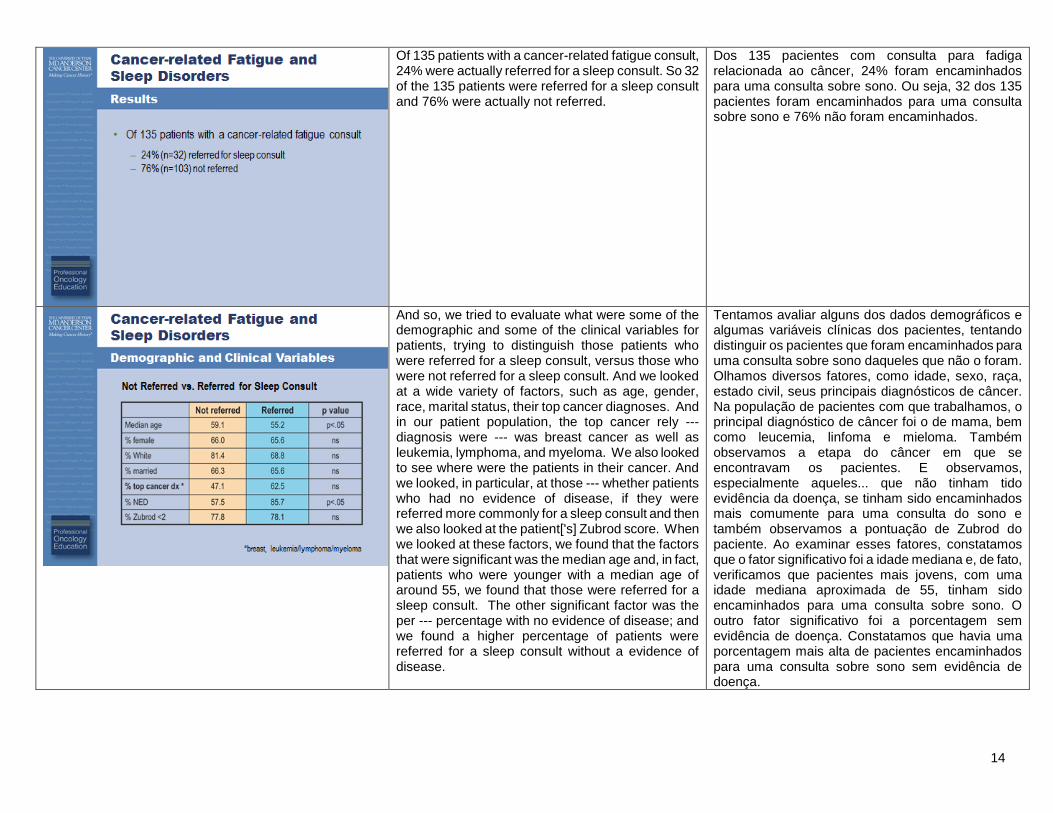
Of 135 patients with a cancer-related fatigue consult, 24% were actually referred for a sleep consult. So 32 of the 135 patients were referred for a sleep consult and 76% were actually not referred.
Dos 135 pacientes com consulta para fadiga relacionada ao câncer, 24% foram encaminhados para uma consulta sobre sono. Ou seja, 32 dos 135 pacientes foram encaminhados para uma consulta sobre sono e 76% não foram encaminhados.
And so, we tried to evaluate what were some of the demographic and some of the clinical variables for patients, trying to distinguish those patients who were referred for a sleep consult, versus those who were not referred for a sleep consult. And we looked at a wide variety of factors, such as age, gender, race, marital status, their top cancer diagnoses. And in our patient population, the top cancer rely --- diagnosis were --- was breast cancer as well as leukemia, lymphoma, and myeloma. We also looked to see where were the patients in their cancer. And we looked, in particular, at those --- whether patients who had no evidence of disease, if they were referred more commonly for a sleep consult and then we also looked at the patient['s] Zubrod score. When we looked at these factors, we found that the factors that were significant was the median age and, in fact, patients who were younger with a median age of around 55, we found that those were referred for a sleep consult. The other significant factor was the per --- percentage with no evidence of disease; and we found a higher percentage of patients were referred for a sleep consult without a evidence of disease.
Tentamos avaliar alguns dos dados demográficos e algumas variáveis clínicas dos pacientes, tentando distinguir os pacientes que foram encaminhados para uma consulta sobre sono daqueles que não o foram. Olhamos diversos fatores, como idade, sexo, raça, estado civil, seus principais diagnósticos de câncer. Na população de pacientes com que trabalhamos, o principal diagnóstico de câncer foi o de mama, bem como leucemia, linfoma e mieloma. Também observamos a etapa do câncer em que se encontravam os pacientes. E observamos, especialmente aqueles... que não tinham tido evidência da doença, se tinham sido encaminhados mais comumente para uma consulta do sono e também observamos a pontuação de Zubrod do paciente. Ao examinar esses fatores, constatamos que o fator significativo foi a idade mediana e, de fato, verificamos que pacientes mais jovens, com uma idade mediana aproximada de 55, tinham sido encaminhados para uma consulta sobre sono. O outro fator significativo foi a porcentagem sem evidência de doença. Constatamos que havia uma porcentagem mais alta de pacientes encaminhados para uma consulta sobre sono sem evidência de doença.
15
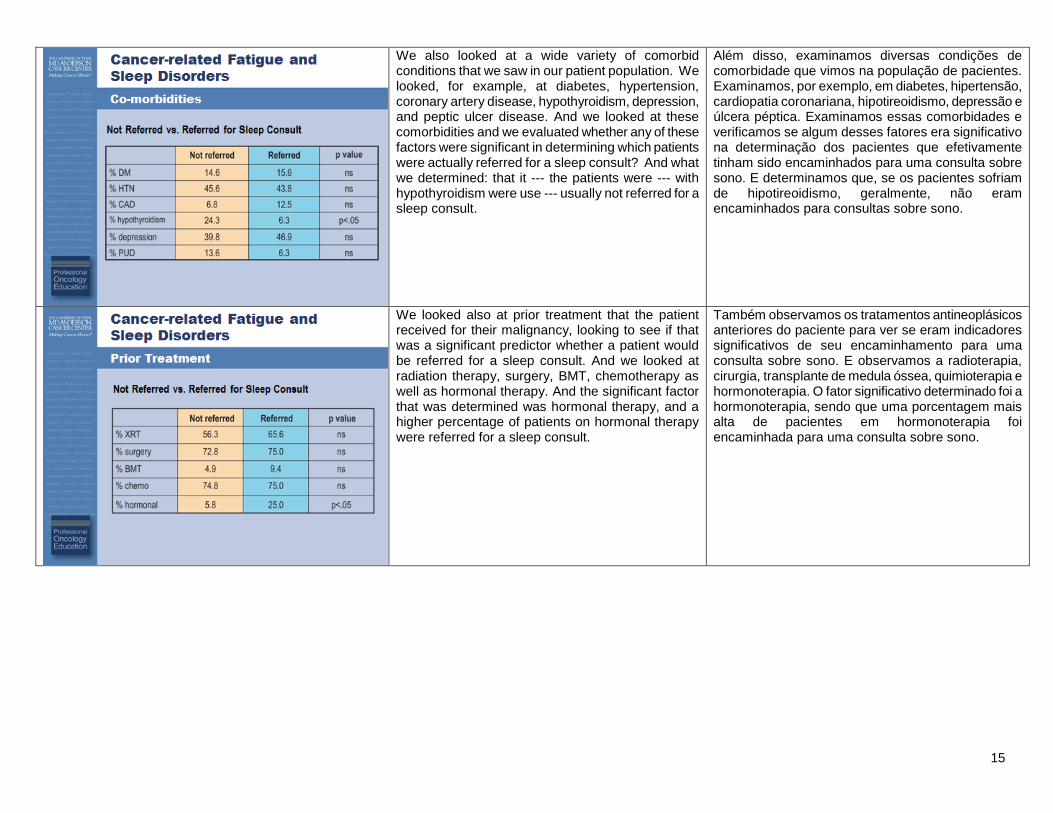
We also looked at a wide variety of comorbid conditions that we saw in our patient population. We looked, for example, at diabetes, hypertension, coronary artery disease, hypothyroidism, depression, and peptic ulcer disease. And we looked at these comorbidities and we evaluated whether any of these factors were significant in determining which patients were actually referred for a sleep consult? And what we determined: that it --- the patients were --- with hypothyroidism were use --- usually not referred for a sleep consult.
Além disso, examinamos diversas condições de comorbidade que vimos na população de pacientes. Examinamos, por exemplo, em diabetes, hipertensão, cardiopatia coronariana, hipotireoidismo, depressão e úlcera péptica. Examinamos essas comorbidades e verificamos se algum desses fatores era significativo na determinação dos pacientes que efetivamente tinham sido encaminhados para uma consulta sobre sono. E determinamos que, se os pacientes sofriam de hipotireoidismo, geralmente, não eram encaminhados para consultas sobre sono.
We looked also at prior treatment that the patient received for their malignancy, looking to see if that was a significant predictor whether a patient would be referred for a sleep consult. And we looked at radiation therapy, surgery, BMT, chemotherapy as well as hormonal therapy. And the significant factor that was determined was hormonal therapy, and a higher percentage of patients on hormonal therapy were referred for a sleep consult.
Também observamos os tratamentos antineoplásicos anteriores do paciente para ver se eram indicadores significativos de seu encaminhamento para uma consulta sobre sono. E observamos a radioterapia, cirurgia, transplante de medula óssea, quimioterapia e hormonoterapia. O fator significativo determinado foi a hormonoterapia, sendo que uma porcentagem mais alta de pacientes em hormonoterapia foi encaminhada para uma consulta sobre sono.

16
With respect to current treatment, we looked to see where --- where the patients were with their cancer treatment, whether they were getting radiation therapy, chemotherapy, or hormonal treatment? And the significant factors were: patients who were presently on chemotherapy usually were not referred for a sleep consult. However, those patients, particularly, for example, the breast cancer patients who were getting hormonal treatment for their underlying malignancy; that was a significant factor for being referred for a sleep consult.
Com relação ao tratamento atual, procuramos observar se os pacientes estavam recebendo tratamento contra o câncer, se estavam recebendo radioterapia, quimioterapia ou hormonoterapia. Os fatores significativos foram: em geral, pacientes que estavam no momento recebendo quimioterapia não foram encaminhados para uma consulta sobre sono. No entanto, esses pacientes, sobretudo, por exemplo, pacientes com câncer de mama que recebiam hormonoterapia para a neoplasia maligna subjacente, esse foi um fator significativo para o encaminhamento de pacientes a uma consulta sobre sono.
So, the overall results from our initial sleep retrospective study was that, of the 32 patients referred for a sleep consult, we found that 66% of those patients were female, 69% were white, and 66% were married. We also looked at the patient’s BMI and we noted that the median BMI was 30. And a BMI of 30 is in the obese range, and we took into consideration that this could be possibly a contributing factor for patients, for example, having some sort of obstructive sleep apnea. What we found, the two most frequent cancer diagnoses in our patients were breast and --- as well as leukemia, lymphoma, and myeloma.
Nos resultados globais de nosso estudo retrospectivo inicial do sono descobrimos que, dos 32 pacientes encaminhados para uma consulta sobre sono, 66% eram do sexo feminino, 69% eram da raça branca e 66% eram casados. Também observamos o IMC do paciente, cujo valor mediano foi 30. Um IMC de 30 está na faixa da obesidade, e tomamos em consideração que isso talvez fosse um fator que contribuísse à apresentação, por exemplo, de algum tipo de apneia obstrutiva do sono nos pacientes. Descobrimos que os dois diagnósticos mais frequentes de câncer nos pacientes foram o câncer de mama e... além de leucemia, linfoma e mieloma.
17
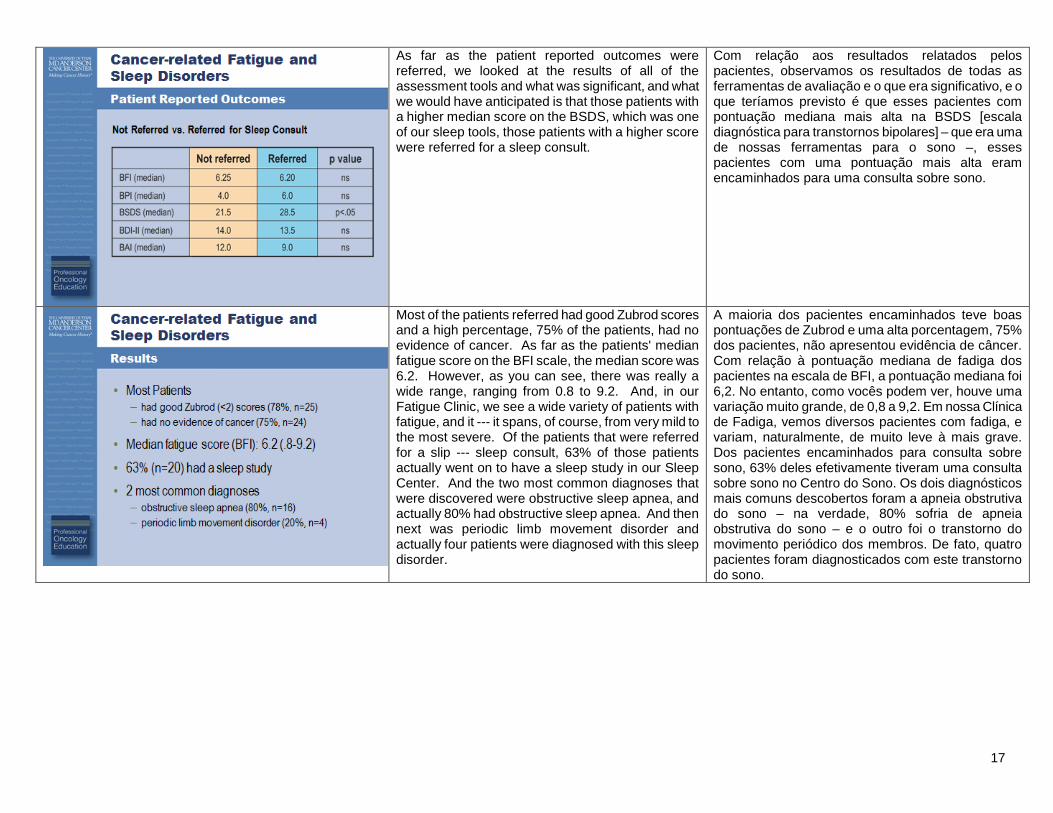
As far as the patient reported outcomes were referred, we looked at the results of all of the assessment tools and what was significant, and what we would have anticipated is that those patients with a higher median score on the BSDS, which was one of our sleep tools, those patients with a higher score were referred for a sleep consult.
Com relação aos resultados relatados pelos pacientes, observamos os resultados de todas as ferramentas de avaliação e o que era significativo, e o que teríamos previsto é que esses pacientes com pontuação mediana mais alta na BSDS [escala diagnóstica para transtornos bipolares] – que era uma de nossas ferramentas para o sono –, esses pacientes com uma pontuação mais alta eram encaminhados para uma consulta sobre sono.
Most of the patients referred had good Zubrod scores and a high percentage, 75% of the patients, had no evidence of cancer. As far as the patients' median fatigue score on the BFI scale, the median score was 6.2. However, as you can see, there was really a wide range, ranging from 0.8 to 9.2. And, in our Fatigue Clinic, we see a wide variety of patients with fatigue, and it --- it spans, of course, from very mild to the most severe. Of the patients that were referred for a slip --- sleep consult, 63% of those patients actually went on to have a sleep study in our Sleep Center. And the two most common diagnoses that were discovered were obstructive sleep apnea, and actually 80% had obstructive sleep apnea. And then next was periodic limb movement disorder and actually four patients were diagnosed with this sleep disorder.
A maioria dos pacientes encaminhados teve boas pontuações de Zubrod e uma alta porcentagem, 75% dos pacientes, não apresentou evidência de câncer. Com relação à pontuação mediana de fadiga dos pacientes na escala de BFI, a pontuação mediana foi 6,2. No entanto, como vocês podem ver, houve uma variação muito grande, de 0,8 a 9,2. Em nossa Clínica de Fadiga, vemos diversos pacientes com fadiga, e variam, naturalmente, de muito leve à mais grave. Dos pacientes encaminhados para consulta sobre sono, 63% deles efetivamente tiveram uma consulta sobre sono no Centro do Sono. Os dois diagnósticos mais comuns descobertos foram a apneia obstrutiva do sono – na verdade, 80% sofria de apneia obstrutiva do sono – e o outro foi o transtorno do movimento periódico dos membros. De fato, quatro pacientes foram diagnosticados com este transtorno do sono.
18
So, in summary, sleep disorders may be under-recognized in cancer-related fatigue patients. And what we found is that 24% of patients that were evaluated for cancer-related fatigue in our Fatigue Center were found appropriate for sleep consult. So, we --- what this shows is that sleep disorders should be considered when evaluating patients with cancer-related fatigue. This was our initial study. We’re planning to continue the work, evaluating the relationship between cancer-related fatigue and sleep disorders. And, in particular, we want to continue to focus on the impact of sleep dysfunction on cancer-related fatigue, particularly as interventions are made when available. Thank you for very much and I hope this presentation has been helpful.
Em resumo, os transtornos do sono podem ser sub-reconhecidos em pacientes com fadiga relacionada ao câncer. Constatamos que 24% dos pacientes avaliados para fadiga relacionada ao câncer no Centro de Fadiga foram considerados adequados para receberem uma consulta sobre sono. Isto mostra que os transtornos do sono devem ser considerados ao avaliar pacientes com fadiga relacionada ao câncer. Esse foi nosso estudo inicial. Planejamos continuar o trabalho, avaliar a relação entre a fadiga relacionada ao câncer e os transtornos do sono. E, sobretudo, queremos continuar a focar no impacto da disfunção do sono na fadiga relacionada ao câncer, especialmente por meio de intervenções quando estiverem disponíveis. Muito obrigada. Espero que esta apresentação tenha sido útil.