postoperative care by dr. muath mustafa department of surgery, bmc hod: dr. ashraf balbaa
TRANSCRIPT

POSTOPERATIVE CARE
BY
Dr. Muath Mustafa
Department of Surgery, BMC
HOD: Dr. Ashraf Balbaa

• Definition
• Objectives
• Introduction and Phases of post operative care
• Management of the patient during each phase
• Daycase Surgery
• Conclusion

Definition:
The management of the patient immediately after surgery until complete of recovery.

Objectives:• To understand the principles of the patient
management in the recovery phase immediately after surgery.
• To understand the general management of the surgical patient in the ward.
• To consider the initial management of common acute complications during the postoperative period

Introduction and Phases of post operative care.
The intensity of the postoperative care monitoring depends upon the type of surgery performed and the severity of the patient`s condition.

Three phases:
• Immediate post operative care (The recovery phase).
• Care in the ward until discharge from hospital.
• Continuing care after discharge (e.g. wound care,
stoma care, physiotherapy, surveillance).
The recovery phase:
• Time: Immediately after surgery.
• Place: Recovery ward or area adjacent to the theater.
• By: One Nurse per patient.
• What to do?

1. Airway and Breathing:
• The patient may have oral airway, nasopharyngeal airway
or still intubated (the artificial airway is left in situ until the
patient can maintain own airway).
• Give O2 by mask, and monitor saturation by pulse
oximeter.

• Special care for Tracheostomy (suction,
bleeding, dislodge).
• Suction of all secretions.

Breathing maybe depressed by:
Airway obstruction.
Residual anesthetic gases.
The depressant effect of opioids

2. Circulation:
• Monitor BP every 15mins, Pulse rate regularly.
• Monitor the wound and any drains for signs of
reactionary bleeding.

3. Position in bed:
Operations in the nose and mouth:
• They should be on their sides with the face down to protect against aspiration of mucus, blood, or vomitus.


Abdominal operations:
• More comfortable with the head slightly elevated and the thighs and knees slightly flexed.
• The heels must be raised at least as high as the knees, to prevent stasis of blood in the calves.

Patients with a spinal anesthesia:
• They should lie flat in bed for four to six hours to minimize post-spinal headache and postural hypotension
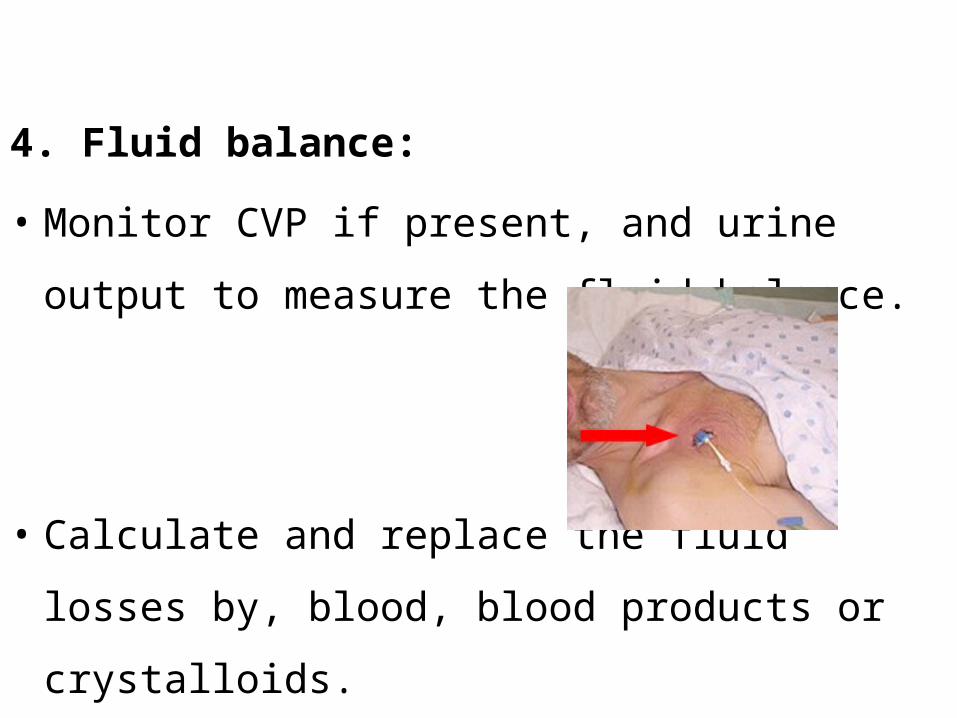
4. Fluid balance:
• Monitor CVP if present, and urine output to
measure the fluid balance.
• Calculate and replace the fluid losses by, blood,
blood products or crystalloids.

5. Core temperature:
• Monitor the temperature and correct it if needed (e.g. space blanket)

6. General condition of the patient:
• Relief of pain and anxiety.
• Administering mouthwashes.
• Patient`s position and care for pressure points.• Prophylaxis against atelectasis by deep
breathing and venous stasis by passive leg exercises.

7.Special care for: DM, Cardiac disease, Orthopedic surgery, Neurosurgery, Urology and Vascular surgery.

Care in the ward:
• Time: The patient may be discharged from the recovery area when able to maintain vital functions independently.
• Place: The ward (general unit).
• By: Nursing staff and medical staff
• Aim: To maintain a stable general condition and detect any complications early by close and frequent observation as done in the recovery room.
• What else to do? :

1. General care:
• Talk to the patient about the operation and its
outcome, their feelings, fears and anxiety, and
reassure regarding pain control.
• Changing the position and early ambulation.
2. Pain control:
• To make smooth recovery.
• Administer adequate analgesia via, I/V, I/M,
Continuous infusion, Patient controlled, epidural or
oral, and chose the agent according to pain scale.
• Avoid NSAIDs in asthmatics and those with peptic
ulcer history.

3. Fluid balance:
• Calculate the fluid requirement by recording the CVP,
Urine output, NG tube output and Drains output then
add the daily fluid requirement and insensible looses.

• Monitor adequacy by CVP, peripheral perfusion,
Urine output and thirst.
• Monitor serum electrolytes and replace them if
needed.

• Monitor for overload by, Edema, auscultation of
the chest and tachycardia.
• Monitor for hypovolaemia by, Oliguria and
search for blood or fluid looses.

4. Blood transfusion:
• Measure Hb to guide you and give blood or blood
products accordingly.
• During transfusion, frequent, regular monitoring of
pulse, BP, and temperature are routine to detect a
transfusion reaction.
.

5. Nutrition:• Allow orally once the patient is conscious and
the GI function is achieved.
• The patient may need nutritional support (parenteral), in case of face, mouth, or esophagus surgeries.
6. Surgical drains:
• Should be monitored and charted (e.g. NG tube,
Chest tube, Drains at the operative site).
• Remove once served its function.
• Look for complications ( introduction of infection,
bleeding, and dislodgment).
7. Special care for patient`s co-morbid conditions, and previous medications.

8.Discharging Order:
• Date and time of discharge.• Discharge diagnosis.• Discharge medications.• Date and time of follow up.

Care after hospital discharge:
• The key is good communication with Pt, Family and
General Practicioner
• Ensure arrangements are made to communicate to
histology results to the patient and plans for additional
investigation or treatment have been made and explained
to the patient

Daycase Surgery:
The patient admitted Same day of surgeryThe patient discharged

The postoperative period is inevitably short, but the management should follow the same basic principles outlined above.

Points to consider:
1. Discharge to a suitable environment.
2. Pain control.
3. Possible side effects of sedation and anaesthesia.

Patients who have had sedation or general anesthesia
must be accompanied home,
should not drive for at least 24hrs, and
written instruction given to the patient and relatives

Patients who have had local anaesthesia:
The doctor should be aware of systemic toxicity and reactionary bleeding.

Toxicity:
Paraesthesia around the lips.
Tinnitus.
Visual disturbances.
Dizziness.
Convulsions.
Cardiac arrythmias.
Collapse.

Sedation:
Give O2 and monitor by pulse oximeter until fully awake.
Observe for at least 2hrs before sending home.
Conclusion:

THANK YOU