postnatal diagnosis and management of the baby with chd ... · • vsd still usually missed...
TRANSCRIPT

Postnatal diagnosis and management of the baby with CHD
and trisomy 21
Frances Bu’Lock
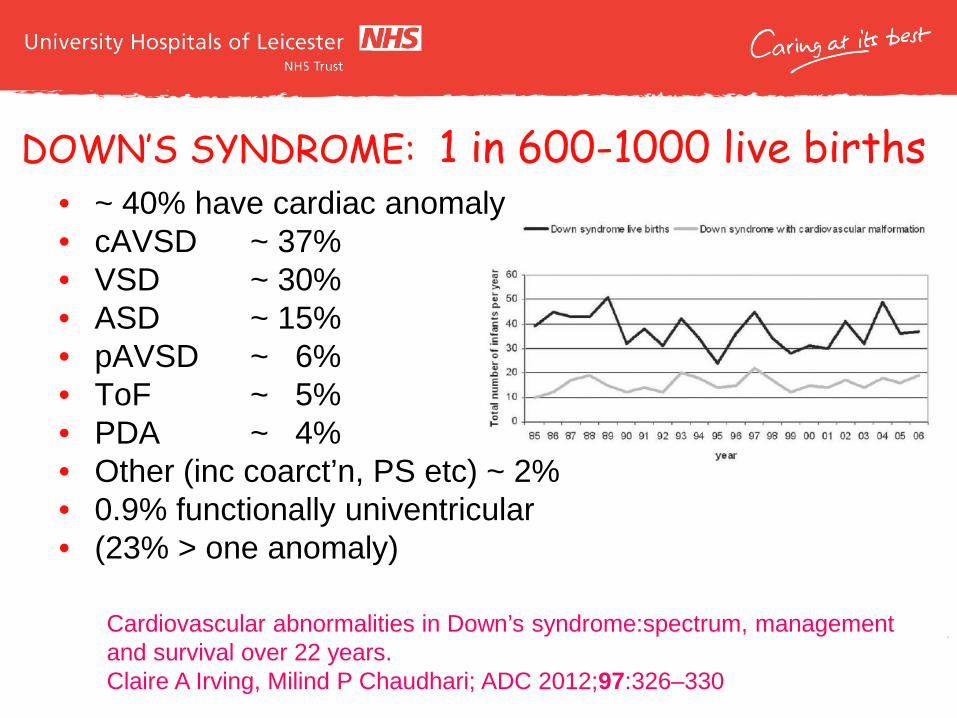
DOWN’S SYNDROME: 1 in 600-1000 live births
Cardiovascular abnormalities in Down’s syndrome:spectrum, management and survival over 22 years. Claire A Irving, Milind P Chaudhari; ADC 2012;97:326–330
• ~ 40% have cardiac anomaly • cAVSD ~ 37% • VSD ~ 30% • ASD ~ 15% • pAVSD ~ 6% • ToF ~ 5% • PDA ~ 4% • Other (inc coarct’n, PS etc) ~ 2% • 0.9% functionally univentricular • (23% > one anomaly)

Prenatal Diagnosis
• In 2013 there were 1,886 diagnoses of Down syndrome, 65% of which were made prenatally, a rate of 2.7 per 1,000 births.
• In 2013 there were an estimated 728 Down syndrome live births, a live birth rate of 1.0 per 1,000 live births.
• The proportion of women under 35 receiving a prenatal diagnosis of Down syndrome has increased from 55% in 2009 to 62% in 2013.
National Down Syndrome Cytogenetic Register 20012-13. Queen Mary University of London

UK Congenital Cardiac interventions




POSTNATAL DIAGNOSIS • cAVSD still commonly missed prenatally
(about 70% missed in non-Downs; 60% in Downs!)
• VSD still USUALLY missed prenatally (93% missed in Downs, 87% in non-Downs).
• Despite 65% prenatal detection of trisomy 21; - surprising !!
• All ASDs and PDAs detected postnatally

AVSD / AVSD ToF
AVSD

All AVSDs

Complete AVSDs

ASD / PDA • Post natal diagnosis only • Still may need surgery • Cannot guarantee normality
before birth
• (similar for Hirschprungs disease, leukaemia etc)

ASD/PDA • 10–15 ASDs/yr closed surgically (18 in 2012) • 10-15 ASDs/yr closed percutaneously (30: 2012) • Similar to non-Down’s ASD
• 4-8 Surgical PDAs/yr vs 15-25 devices in Down’s
- different from non-Down’s (350 vs 550); --- the preterm duct
• TGA vanishingly rare (1 switch in 10 years; ? miscoded)
• Single ventricle surgery about 3 per annum • Mitral valve replacement 2-5 pa (increasing;
suggests about 5% of cAVSD pts may eventually need MVR)
• Coarctation / arch problems also rare 2-3 pa • 2 Norwoods in 2004.
Other lesions

Outcomes
Cardiovascular abnormalities in Down’s syndrome: spectrum, management and survival over 22 years Claire A Irving, Milind P Chaudhari; ADC 2012;97:326–330

2012

Postnatal pathways

Postnatal pathways; should probably now read
In a new, postnatal diagnosis of Down’s syndrome, even if the cardiovascular examination is normal an echocardiogram need to be arranged within the first week of life; contact the on-call Cardiology Registrar or consultant at Glenfield by phone or using the urgent referral form. Most patients should be seen within the first week of life.
When there has been a normal fetal echocardiogram, postnatal cardiac review is needed at 2-3 months of age to ensure atrial septal and ductal closure



Support Groups Support Groups
• http://www.downs-syndrome.org.uk • http://dhg.org.uk


And then? • Pulmonary vascular resistance • Frequency of follow-up; VSD / AVSD 4-6 weeks • Coarctation… with VSD vs AVSD? • Role of PA banding? • Admissions? ACE, diuresis; protocols? • Timing of surgery • The functionally single ventricle? • Mitral Valve prolapse?! • ECMO

Thank you