post-mastectomy syndrome: evaluation michael d. stubblefield, m.d. national medical director for...
TRANSCRIPT

POST-MASTECTOMY SYNDROME: EVALUATION
Michael D. Stubblefield, M.D.National Medical Director for Cancer RehabilitationSelect Medical CorporationMedical Director for Cancer RehabilitationKessler Institute for Rehabilitation American Board of Physical Medicine & RehabilitationAmerican Board of Electrodiagnostic MedicineAmerican Board of Internal Medicine

2
Post-mastectomy SyndromeDisclosures
None

3
Post-mastectomy SyndromeKey Components of Evaluation
• History• Physical• Laboratory• Imaging• Electrodiagnostic

4
Post-mastectomy SyndromeKey Components of History
• Diagnosis date• Conditions of diagnosis• Histology• Grade• Biomarker status• Stage• Resection• Reconstruction • Chemotherapy• Radiotherapy• Hormonal therapy• Complications• Recurrence

5
Post-mastectomy SyndromeBreast Cancer Histology
• Noninvasive– Lobular carcinoma in situ– Ductal carcinoma in situ
• Invasive– Ductal– Lobular– Mixed ductal/lobular– Mucinous– Comedo– Inflammatory– Tubular– Medullary– Papillary
Li CI, Uribe DJ, Daling JR. Clinical characteristics of different histologic types of breast cancer. Br J Cancer 2005;93:1046-52.

6
Post-mastectomy SyndromeBiomarker Status
• Estrogen • Progesterone• HER2

7
Post-mastectomy SyndromeBreast Cancer Staging
Tumor Nodes Metastases
Stage 0 Tis N0 M0
Stage IA T1* N0 M0
Stage IB T0 N1mi M0
T1* N1mi M0
Stage IIA T0 N1** M0
T1* N1** M0
T2 N0 M0
Stage IIB T2 N1 M0
T3 N0 M0
*T1 includes T1mi**T0 and T1 tumors with nodal micrometastases only are excluded from Stage IIA and are classified as Stage IB

8
Post-mastectomy SyndromeBreast Cancer Staging
Tumor Nodes Metastases
Stage IIIA T0 N2 M0
T1* N2 M0
T2 N2 M0
T3 N1 M0
Stage IIIB T4 N0 M0
T4 N1 M0
T4 N2 M0
Stage IIIC Any T N3 M0
Stage IV Any T Any N M1
*T1 includes T1mi
9
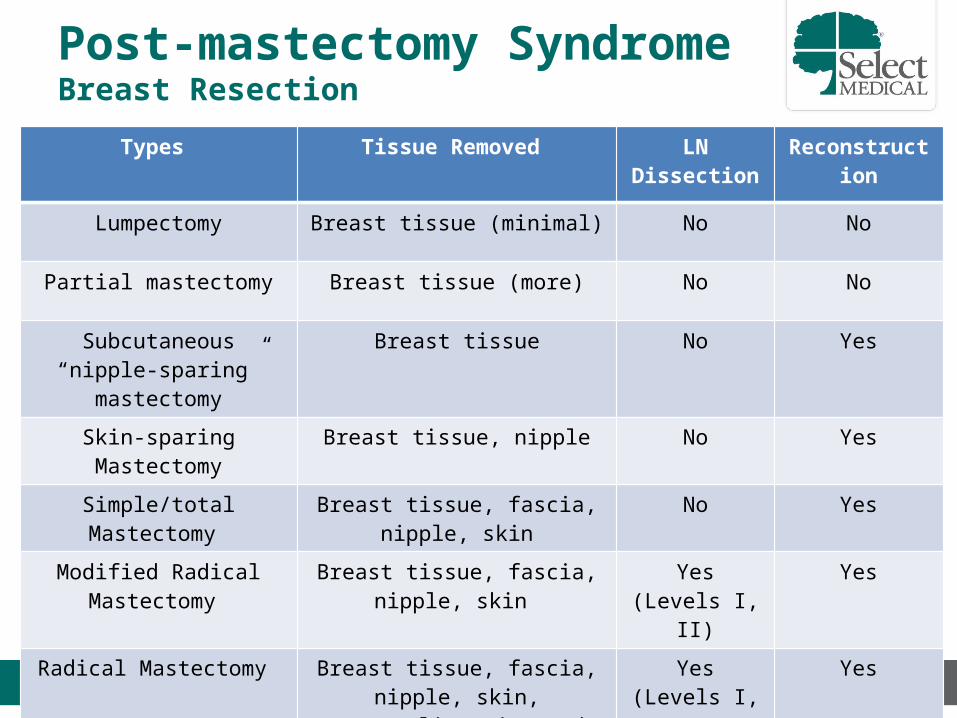
Post-mastectomy SyndromeBreast Resection
Types Tissue Removed LN Dissection Reconstruction
Lumpectomy Breast tissue (minimal) No No
Partial mastectomy Breast tissue (more) No No
Subcutaneous “nipple-sparing” mastectomy
Breast tissue No Yes
Skin-sparing Mastectomy Breast tissue, nipple No Yes
Simple/total Mastectomy Breast tissue, fascia, nipple, skin No Yes
Modified Radical Mastectomy Breast tissue, fascia, nipple, skin Yes (Levels I, II) Yes
Radical Mastectomy Breast tissue, fascia, nipple, skin, pectoralis major and minor
Yes (Levels I, II, III)
Yes

10
Post-mastectomy SyndromeLumpectomy & Partial Mastectomy
• Lumpectomy involves removal of the breast tumor (the "lump") and a small amount of normal surrounding tissue
• Partial mastectomy involves removal of the breast tumor and a larger amount of normal surrounding tissue relative to lumpectomy

11
Post-mastectomy SyndromeMastectomy Incisions

12
Post-mastectomy SyndromeSubcutaneous (“Nipple-Sparing") Mastectomy
• Subcutaneous ("nipple-sparing") mastectomy involves removal of all breast tissue with preservation of the nipple
• Subcutaneous mastectomy is performed less often than simple or total mastectomy because residual breast tissue may harbor cancer cells

13
Post-mastectomy SyndromeSkin-sparing Mastectomy

14
Post-mastectomy SyndromeSkin-sparing Mastectomy
• In a skin-sparing mastectomy, all of the breast skin, except the nipple and the areola, is preserved. This makes reconstruction easier and most importantly avoids making any scars on the breast, allowing for better results after breast reconstruction

15
Post-mastectomy SyndromeSimple/Total Mastectomy
• Appropriate for women with multiple or large areas of ductal carcinoma in situ (DCIS) and for women seeking prophylactic mastectomies.
• Entire breast removed.• No axillary lymph node
dissection.• No muscles are removed.

16
Post-mastectomy SyndromeModified Radical Mastectomy
• Generally used for invasive breast cancer.
• Entire breast removed.• Axillary lymph node dissection
(levels I and II) performed.• No muscles are removed from
beneath the breast
17
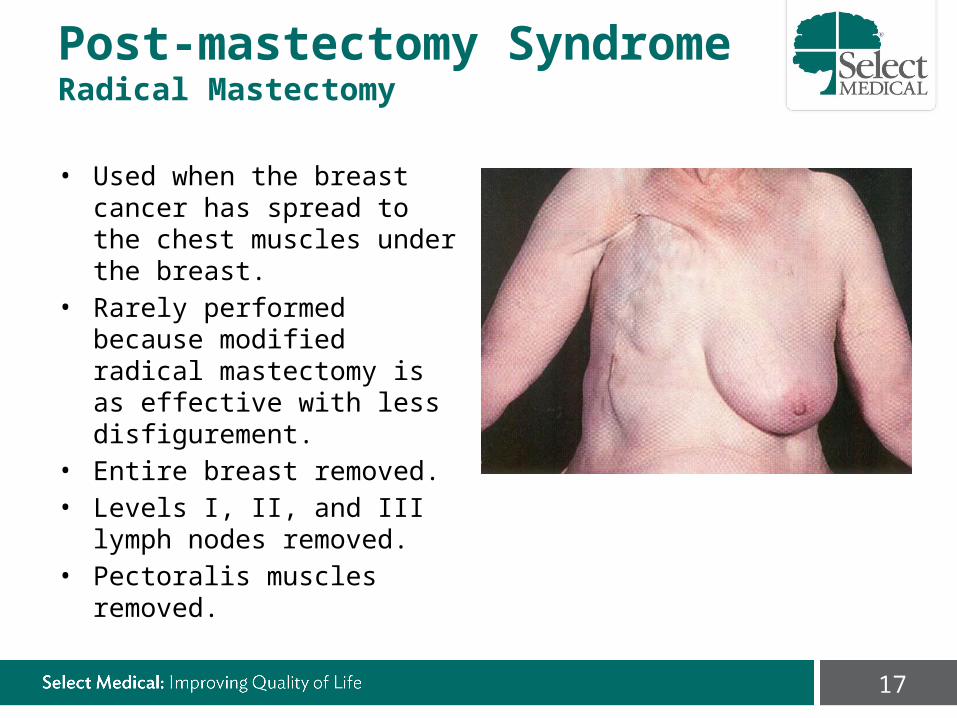
Post-mastectomy SyndromeRadical Mastectomy
• Used when the breast cancer has spread to the chest muscles under the breast.
• Rarely performed because modified radical mastectomy is as effective with less disfigurement.
• Entire breast removed.• Levels I, II, and III lymph nodes
removed.• Pectoralis muscles removed.

18
Post-mastectomy SyndromeLymph Node Dissection
• Level I is the bottom level, below the lower edge of the pectoralis minor muscle.
• Level II is lying underneath the pectoralis minor muscle.
• Level III is above the pectoralis minor muscle.
19
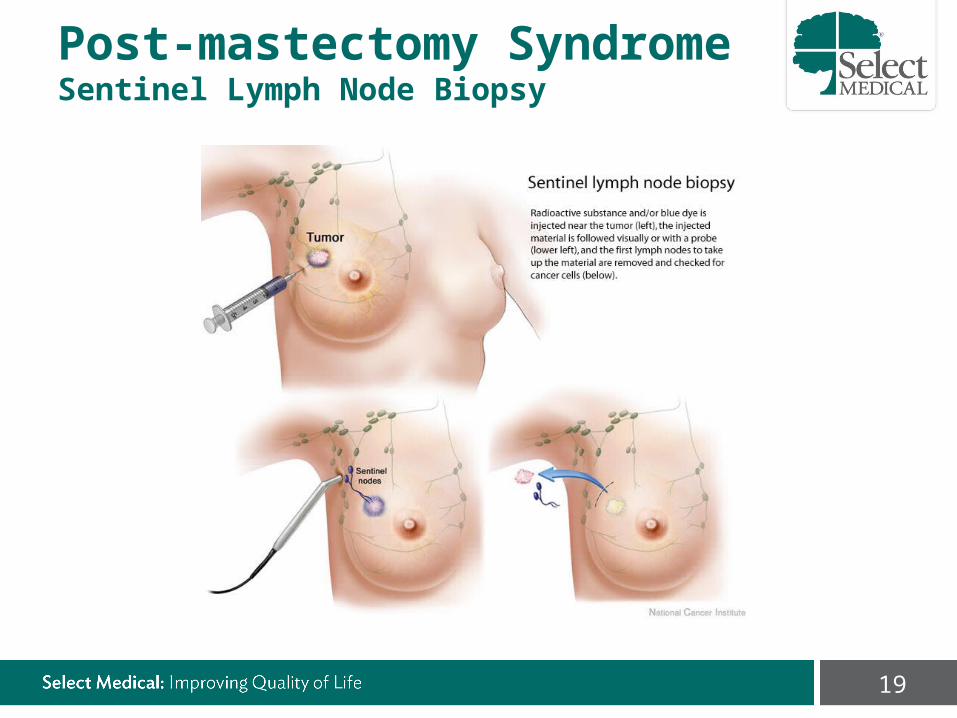
Post-mastectomy SyndromeSentinel Lymph Node Biopsy

20
Post-mastectomy SyndromeBreast Reconstruction Options
• Implants– Immediate implant– Tissue expander Implant
• Autologous tissue transplantation– Fat grafting– Pedicle flap
• Transverse Rectus Abdominis Myocutaneous Flap (TRAM)– Free/muscle sparing flap
• Transverse Rectus Abdominis Myocutaneous Flap (TRAM)• Deep Inferior Epigastric Perforator (DIEP) • Transverse Upper Gracilis (TUG)• Gluteal Free Flap/Gluteal Artery Perforator (GAP)
• Breast implants and autologous tissue transplantation– Latissimus dorsi flap

21
Post-mastectomy SyndromeTissue Expander

22
Post-mastectomy SyndromeBreast Implant
• Implants have a silicone shell filled with either silicone gel or saline. – Silicone gel-filled implants do not
increase the risk of immune system dysfunction.
– “Gummy bear” implants and are made of highly cohesive silicone and are more accurately called form-stable implants.
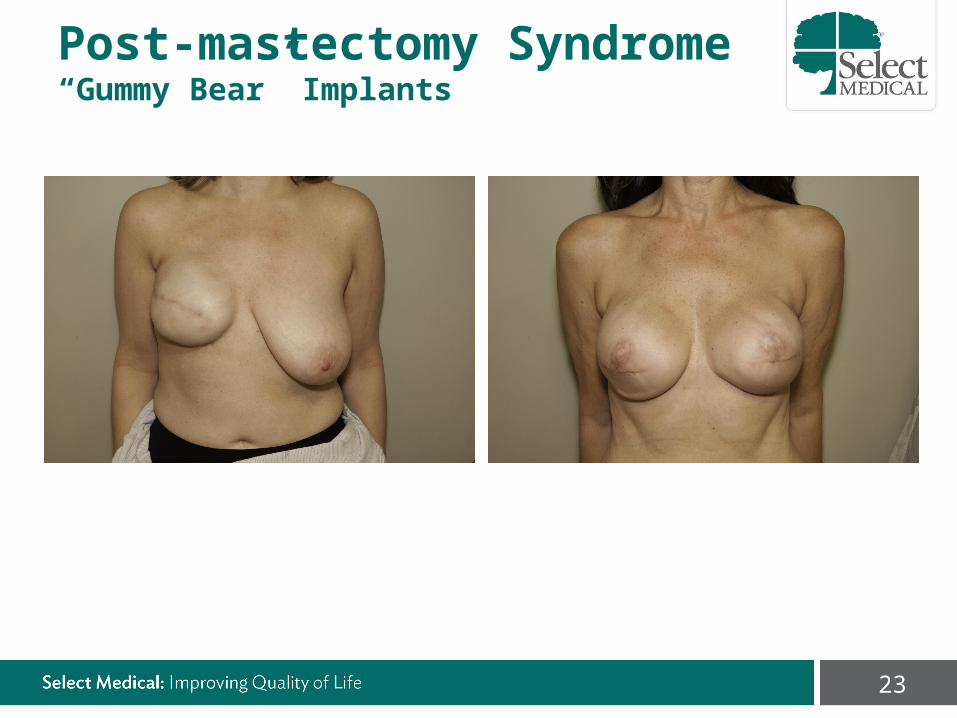
23
Post-mastectomy Syndrome“Gummy Bear” Implants
24
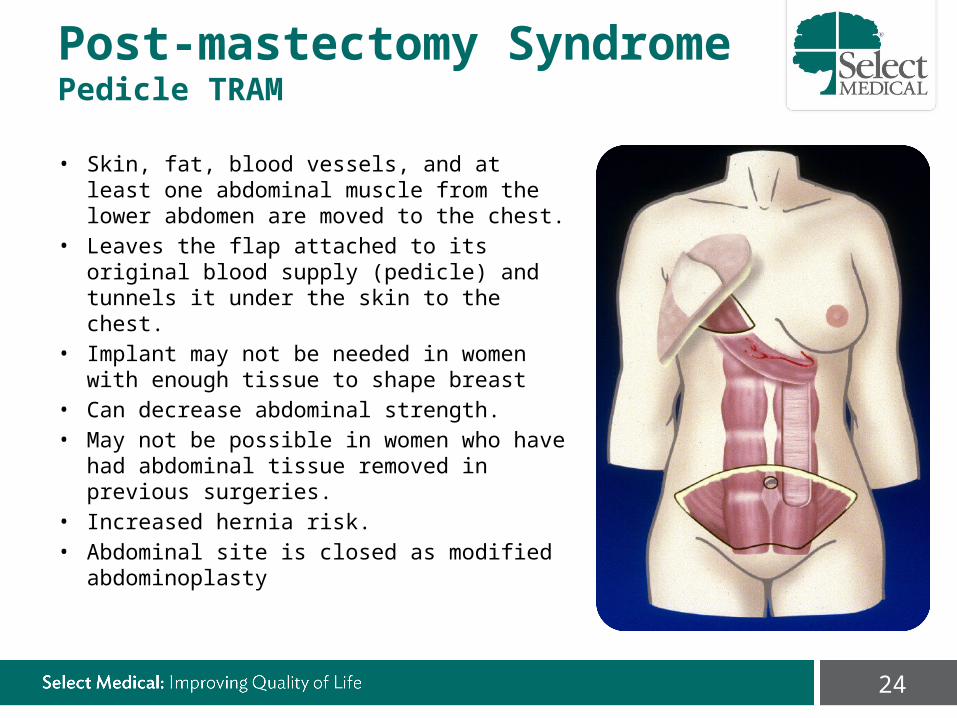
Post-mastectomy SyndromePedicle TRAM
• Skin, fat, blood vessels, and at least one abdominal muscle from the lower abdomen are moved to the chest.
• Leaves the flap attached to its original blood supply (pedicle) and tunnels it under the skin to the chest.
• Implant may not be needed in women with enough tissue to shape breast
• Can decrease abdominal strength.• May not be possible in women who have had
abdominal tissue removed in previous surgeries.
• Increased hernia risk.• Abdominal site is closed as modified
abdominoplasty

25
Post-mastectomy SyndromeFree/Muscle Sparing TRAM
• Required less muscle than pedicle TRAM.• Free flap requiring microsurgical
anastomose to the thoracodorsal or internal mammary artery.
• Surgery takes longer than pedicle TRAM flap.
• The blood supply to the flap is usually better than with pedicle flap.
• Donor site often more cosmetic• Less hernia risk than pedicle TRAM

26
Post-mastectomy SyndromeDeep Inferior Epigastric Perforator (DIEP) Flap
• Uses fat and skin from the same area as the TRAM flap but NOT muscle to form the breast mound.
• Results in reduced fat in the lower abdomen (“tummy tuck”).
• Free flap requiring microsurgery to anastomose blood vessels.
• Less risk of a hernia because no muscle is taken.

27
Post-mastectomy SyndromeTransverse Upper Gracilis (TUG) Flap
• Uses muscle and fatty tissue from along the bottom fold of the buttock extending to the inner thigh.
• Free flap requiring microsurgery to anastomose blood vessels.
• Not a good option for women with thin thighs.
• Only available in some centers.

28
Post-mastectomy SyndromeGluteal Free Flap/Gluteal Artery Perforator (GAP)
• Uses tissue from the buttocks, including the gluteal muscle, to create the breast mound.
• Free flap requiring microsurgery to anastomose blood vessels.
• It may be an option for women who cannot or do not wish to use the abdominal sites due to thinness, incisions, failed flap, or other reasons.
• Only available in some centers.
29
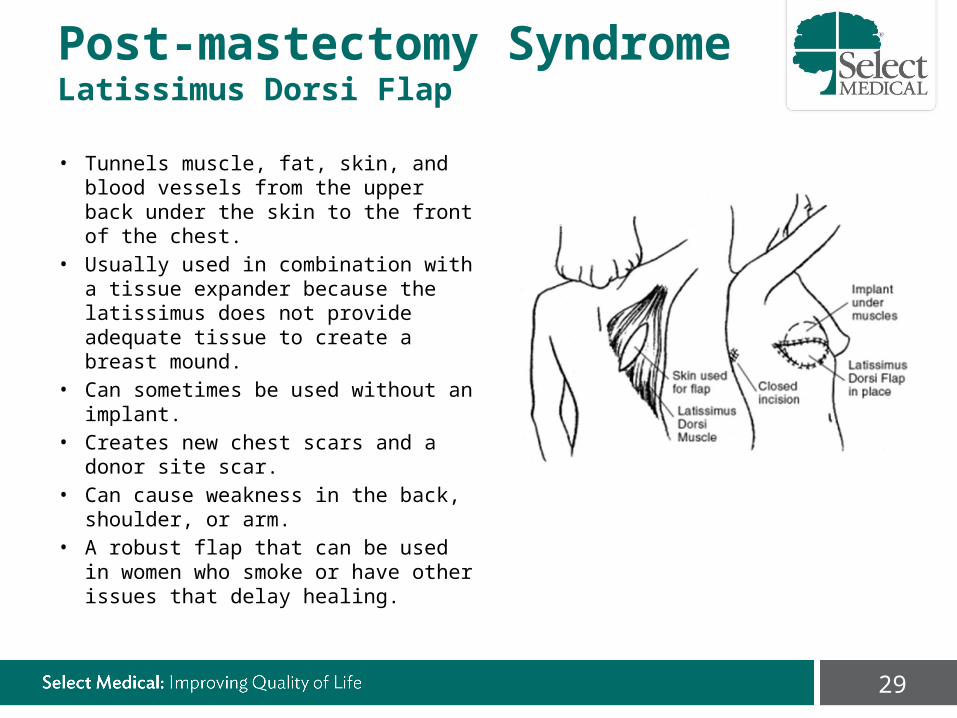
Post-mastectomy SyndromeLatissimus Dorsi Flap
• Tunnels muscle, fat, skin, and blood vessels from the upper back under the skin to the front of the chest.
• Usually used in combination with a tissue expander because the latissimus does not provide adequate tissue to create a breast mound.
• Can sometimes be used without an implant.
• Creates new chest scars and a donor site scar.
• Can cause weakness in the back, shoulder, or arm.
• A robust flap that can be used in women who smoke or have other issues that delay healing.

30
Post-mastectomy SyndromeNeoadjuvant/Adjuvant Chemotherapy for Breast Cancer
• HER2-negative disease– Dose-dense AC (doxorubicin/cyclophosphamide) followed by paclitaxel every
2 weeks– Dose-dense AC (doxorubicin/cyclophosphamide) followed by weekly
paclitaxel– TC (docetaxel and cyclophosphamide)
• HER2-positive disease– AC followed by T + trastuzumab ± pertuzumab
(doxorubicin/cyclophosphamide followed by paclitaxel plus trastuzumab ± pertuzumab)
– TCH (docetaxel/carboplatin/trastuzumab ± pertuzumab

31
Post-mastectomy SyndromeRadiotherapy in Breast Cancer
• Whole Breast Radiation– Targets majority of breast tissue– May use wedges, IMRT, respiratory
gating, prone positioning, etc. to obtain uniform dose distribution with minimal normal tissue toxicity
– Dose usually 45-50 Gy in 23-25 fractions or 40-42.5 Gy in 15-16 fractions
– Boost to tumor bed recommended for higher risk patients (age <50 years and high-grade disease)
– Typical boost doses 10-16 Gy at 2Gy/fx
– Dose schedules are given 5 days per week

32
Post-mastectomy SyndromeBreast Radiotherapy - Supine

33
Post-mastectomy SyndromeBreast Radiotherapy - Prone

34
Post-mastectomy SyndromeBreast Radiotherapy - Boost

35
Post-mastectomy SyndromeRadiotherapy in Breast Cancer
• Chest Wall Radiation– Targets includes ipsilateral chest wall, mastectomy scar, and drain sites
where possible– My include breast reconstruction– CT-based treatment planning should be used to minimize exposure to
lung and hear.

36
Post-mastectomy SyndromeRadiotherapy in Breast Cancer
• Regional Nodal Radiation– CT-based treatment planning should be used– Prescription depth for paraclavicular and axillary nodes varies based
on patient anatomy– Dose 50-50.4 Gy in 1.8-2.0 Gy fractions– May include scar boost of 2 Gy per fraction to total dose of 60 Gy– Dose schedule 5 days per week
37
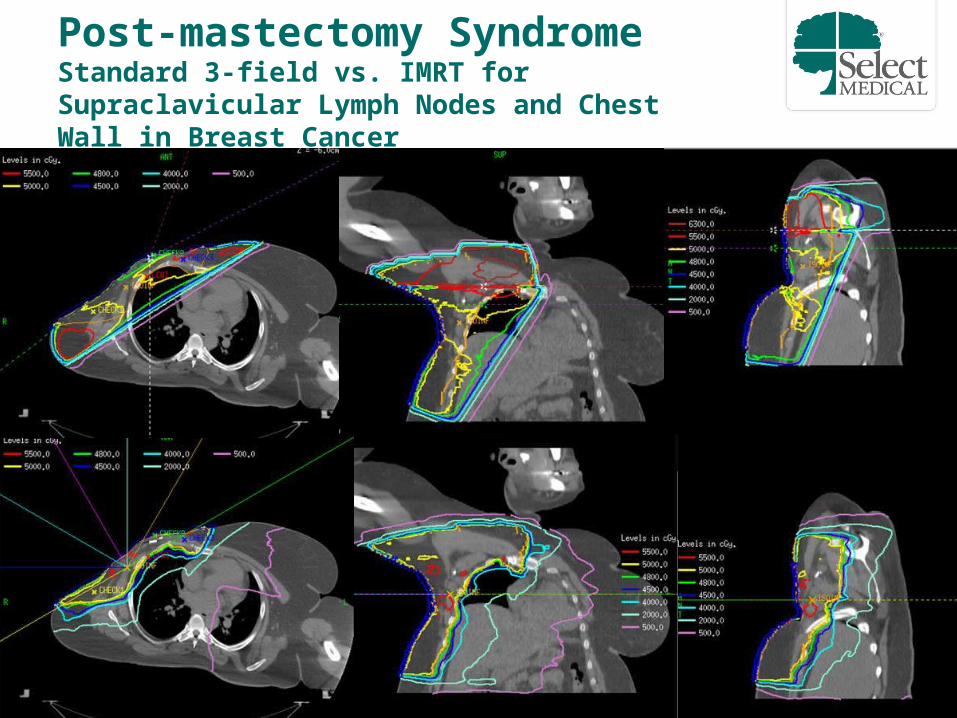
Post-mastectomy SyndromeStandard 3-field vs. IMRT for Supraclavicular Lymph Nodes and Chest Wall in Breast Cancer

38
Post-mastectomy SyndromeUpper Body Pain Disorders in Breast Cancer Survivors
Neuromuscular Cervical radiculopathyLeptomeningeal diseaseBrachial plexopathyPolyneuropathy Chemotherapy Induced Peripheral Neuropathy Diabetic Peripheral Neuropathy Mononeuropathy Dorsal scapular (Rhomboids C5) Suprascapular (Supraspinatus and infraspinatus C5-C6) Long thoracic (Serratus anterior (C5-C6-C7) Lateral pectoral (Pectoralis major and minor (C5 to T1) Medial Pectoral (Pectoralis major and minor (C5 to T1) Thoracodorsal (Latissimus dorsi C6-C7-C8) Median
Carpal tunnel syndrome Ulnar
Cubital tunnel Guyon canal Radial
Radial groove Intercostal
Anterior cutaneous branch Lateral cutaneous branch
Anterior branch Intercostobrachial (lateral cutaneous branch of 2nd
intercostal nerve)Complex Regional Pain Syndrome
Musculoskeletal Post-surgical painRotator cuff diseaseBicipital tendonitisAdhesive capsulitisBony metastasesEpicondylitisDeQuervain’s tenosynovitisArthralgiasArthritis
Lymphovascular LymphedemaAxillary web syndrome/cordingDeep vein thrombosisPost-thrombotic syndrome
Integumentary CellulitisRadiation dermatitisRadiation fibrosisSeromaImplant rupture
Stubblefield MD, Keole, N. Upper Body Pain and Functional Disorders in Breast Cancer Patients. PMR. 2014;6(2):170-83.

39
Physical Examination

40
Post-mastectomy SyndromePhysical Examination by System/Body Area
• Constitutional• Eyes• ENMT• Neck• Respiratory• Cardiovascular• Breasts• Gastrointestinal (Abdomen)• Genitourinary• Lymphatic• Musculoskeletal• Skin• Neurologic• Psychiatric
https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/eval_mgmt_serv_guide-ICN006764.pdf

41
Post-mastectomy SyndromePhysical Examination by System/Body Area
• • • • • • • Breasts• Gastrointestinal (Abdomen)• • Lymphatic• Musculoskeletal• Skin• Neurologic•
https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/eval_mgmt_serv_guide-ICN006764.pdf

42
Post-mastectomy SyndromePhysical Examination - Breasts
• Scars• Symmetry• Capsule contraction• Necrosis• Atrophy

43
Post-mastectomy SyndromePhysical Examination - Abdomen
• Scars• Hernias• Muscle contraction• Seroma

44
Post-mastectomy SyndromePhysical Examination - Musculoskeletal
• Inspection: atrophy, deformity, asymmetry, spasm, fasciculations, myokymia, posture, scapulothoracic motion
• Palpation: muscles(cervical paraspinals, trapezius, rhomboids, levator scapulae, pectoralis major, serratus anterior), joints, tendons, ligaments for tenderness, spasm, consistency
• Maneuvers: AROM, PROM, Neer’s, Hawkin’s, empty can test

45
Post-mastectomy SyndromePhysical Examination - Lymphatic
• Lymphedema• Cording/Axillary Webbing

46
Post-mastectomy SyndromePhysical Examination - Skin
• Radiation changes• Cellulitis• Seroma• Tattoos• Mediport

47
Post-mastectomy SyndromePhysical Examination - Neurologic
• Strength• Reflexes• Sensory changes

48
Post-mastectomy SyndromeLaboratory Testing
• Complete blood count with differential• Comprehensive metabolic profile• B-12 level (with methylmalonic acid & homocysteine if
equivocal)• Lyme titer• TSH• Vitamin D levels• ANA/RF

49
Post-mastectomy SyndromeImaging
• Implant rupture– MRI – USG– CT– Mammography
• Shoulder (RTC tendonitis, adhesive capsulitis, AVN)– X-ray– MRI– CT
• Spine (Stenosis, disk)– X-ray– MRI– CT

50
Post-mastectomy SyndromeElectrodiagnostic Evaluation
Tashiro K, Furukawa M, Nakata T, et al. [Electrophysiological study on the atrophied pectoralis major muscle after modified radical mastectomy]. Nihon Geka Gakkai Zasshi. Mar 1989;90(3):429-433.
• Denervation changes observed in the pectoralis major muscle
• Chronic denervation in 16/20 patients (80%)
• Pectoral nerve injury during lymph node dissection

51
Thank You!