post instability echte
TRANSCRIPT
POSTERIOR INSTABILITY
W.Jaap Willems,
Lairesse Kliniek
Amsterdam, The Netherlands

Disclosures
Consultant - Smith and Nephew
- Tornier
Reearch grants - Tornier
Classification
• Complete traumatic dislocation
- locked
- recurrent
• Traumatic subluxation: (involuntaryinstability)
• Voluntary instability
• Voluntary turned into involuntary instability
Etiology
Posterior shoulder instability
* Bigliani 1995, Bottoni 2005, Kim 2003 McIntyre 1997, Robinson 2005
• traumatic microtrauma atraumatic
• less laxity more laxity
• rec. dislocation provocative test

Etiology
• unidirectional multidirectional
• involuntary voluntary
Posterior shoulder instability
* Bigliani 1995, Bottoni 2005, Kim 2003 McIntyre 1997, Robinson 2005
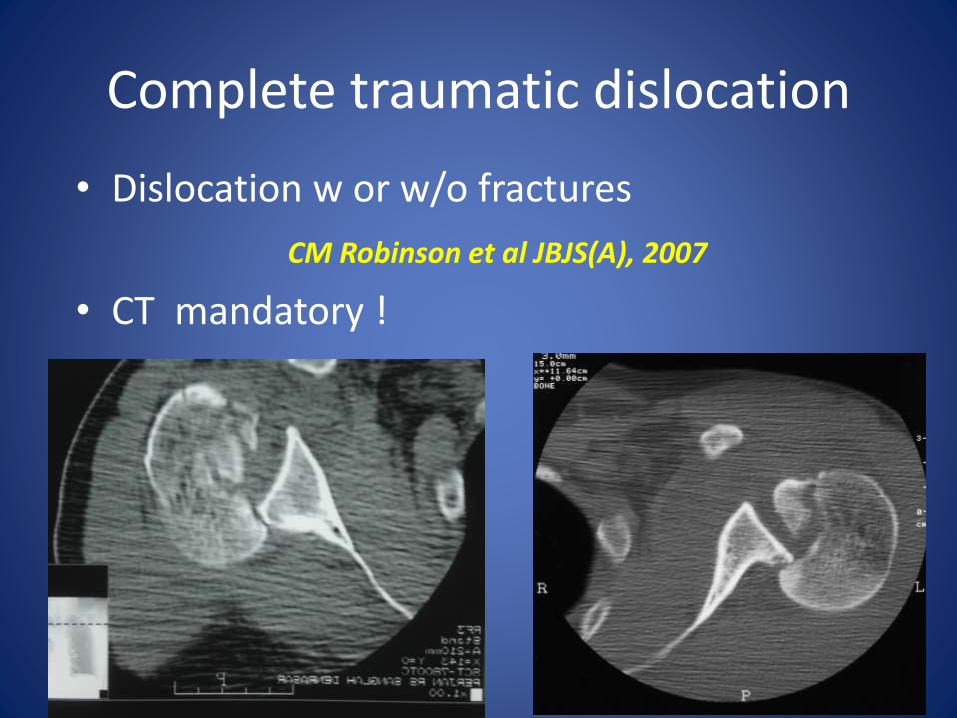
Complete traumatic dislocation
• Dislocation w or w/o fractures
CM Robinson et al JBJS(A), 2007
• CT mandatory !
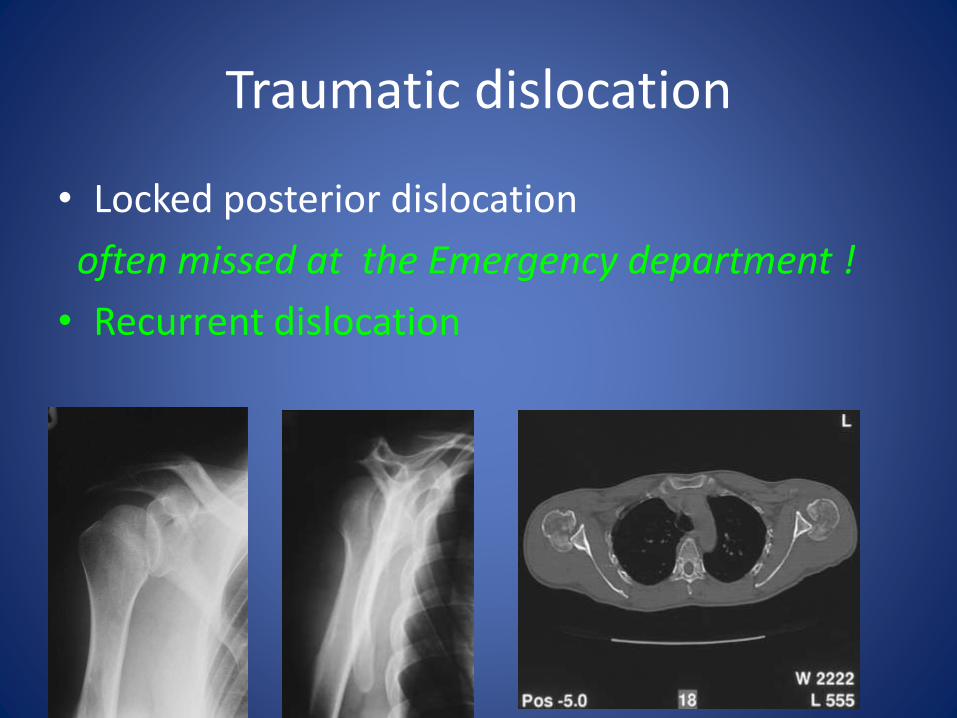
Traumatic dislocation
• Locked posterior dislocation
often missed at the Emergency department !
• Recurrent dislocation
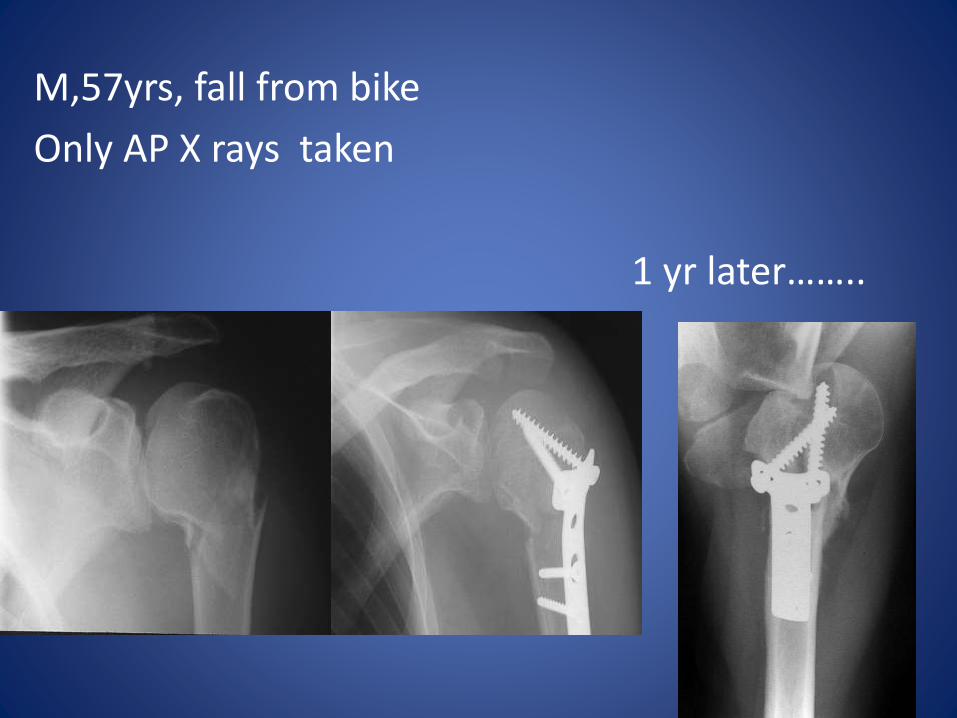
M,57yrs, fall from bike
Only AP X rays taken
1 yr later……..
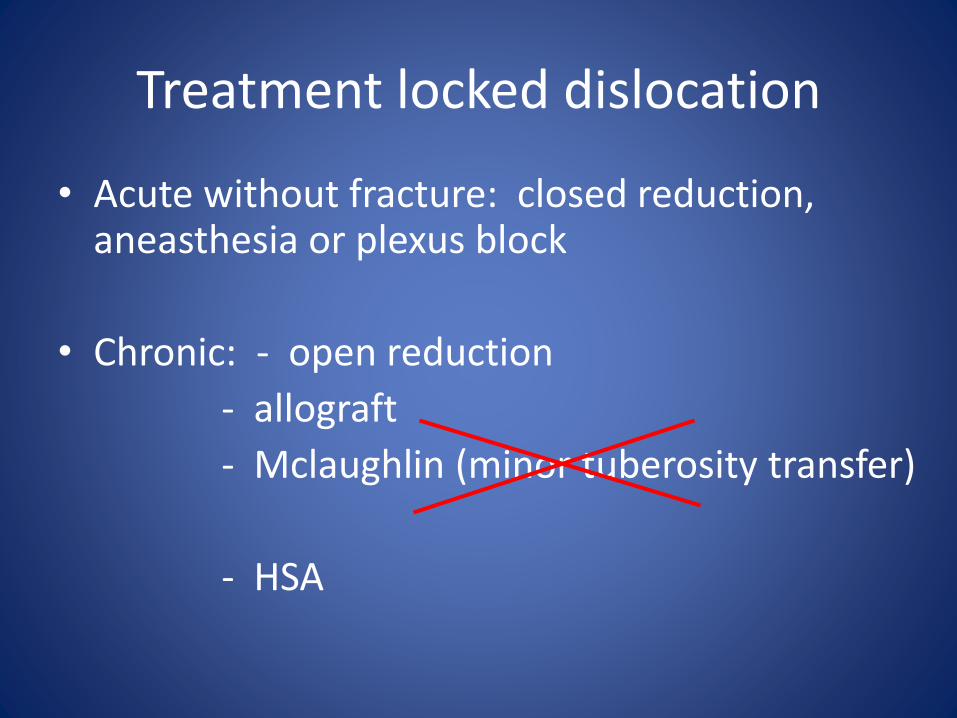
Treatment locked dislocation
• Acute without fracture: closed reduction, aneasthesia or plexus block
• Chronic: - open reduction
- allograft
- Mclaughlin (minor tuberosity transfer)
- HSA
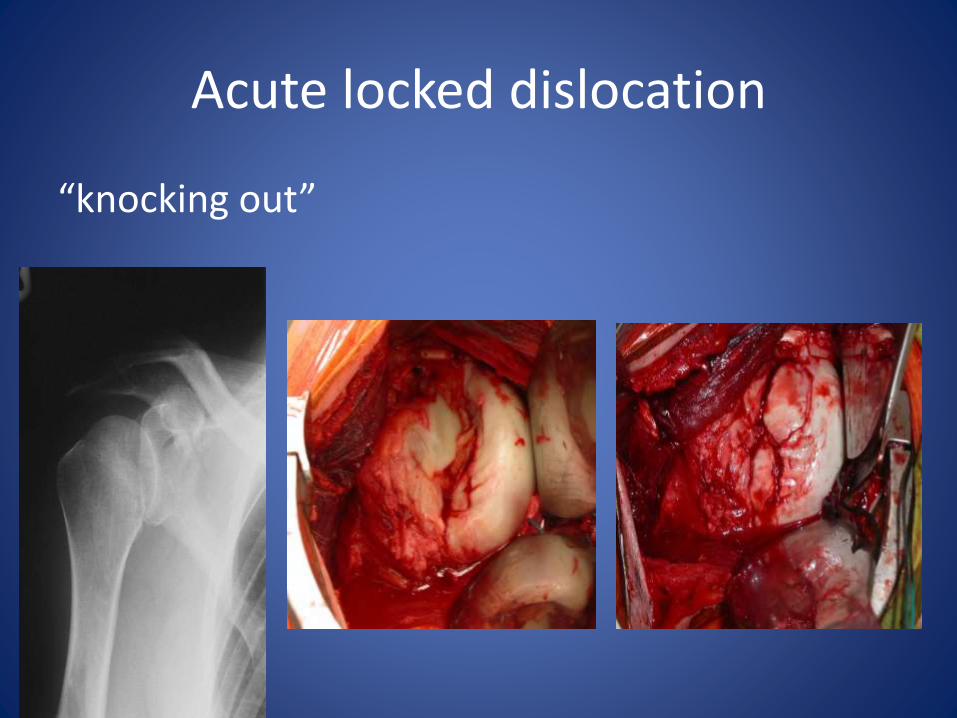
Acute locked dislocation
“knocking out”
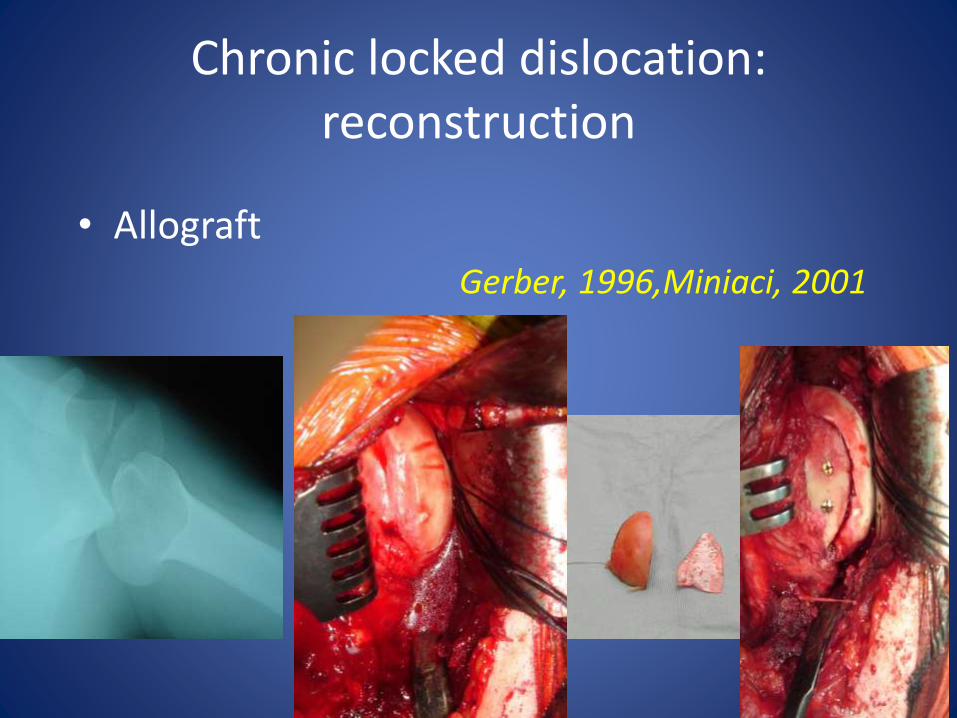
Chronic locked dislocation: reconstruction
• Allograft
Gerber, 1996,Miniaci, 2001
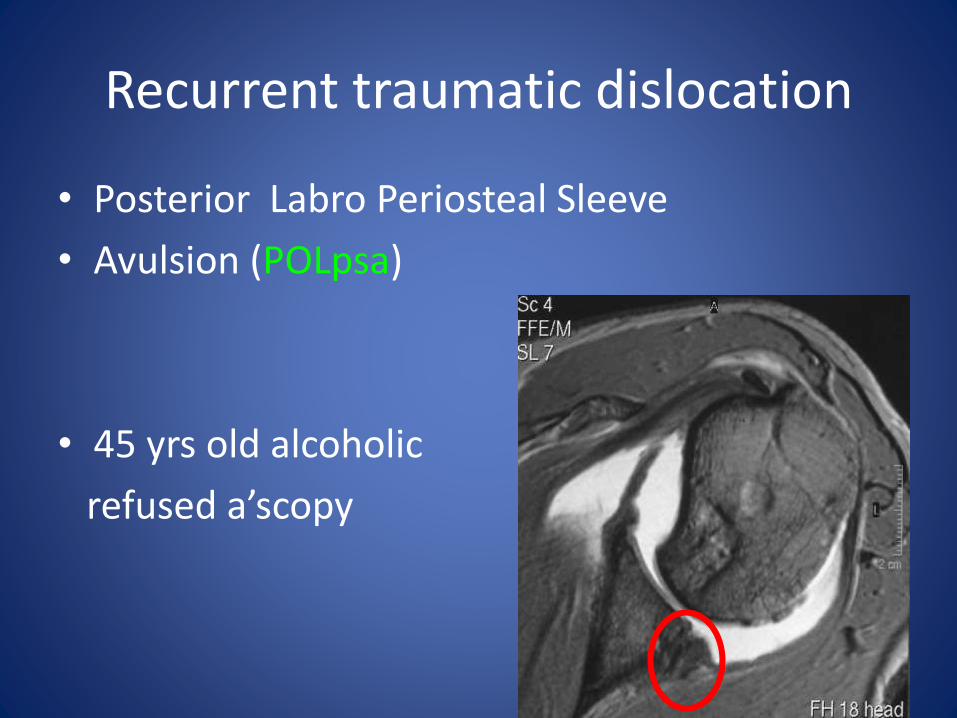
Recurrent traumatic dislocation
• Posterior Labro Periosteal Sleeve
• Avulsion (POLpsa)
• 45 yrs old alcoholic
refused a’scopy
Recurrent traumatic subluxation
• Etiology: acute trauma
or
recurrent microtrauma
• Symptoms : - posterior shoulder pain
- instability symptoms
Diagnostic tests
• Jerk test
• Posterior load and shift
• Sulcus sign
• Posterior apprehension test
• Hyperlaxity tests
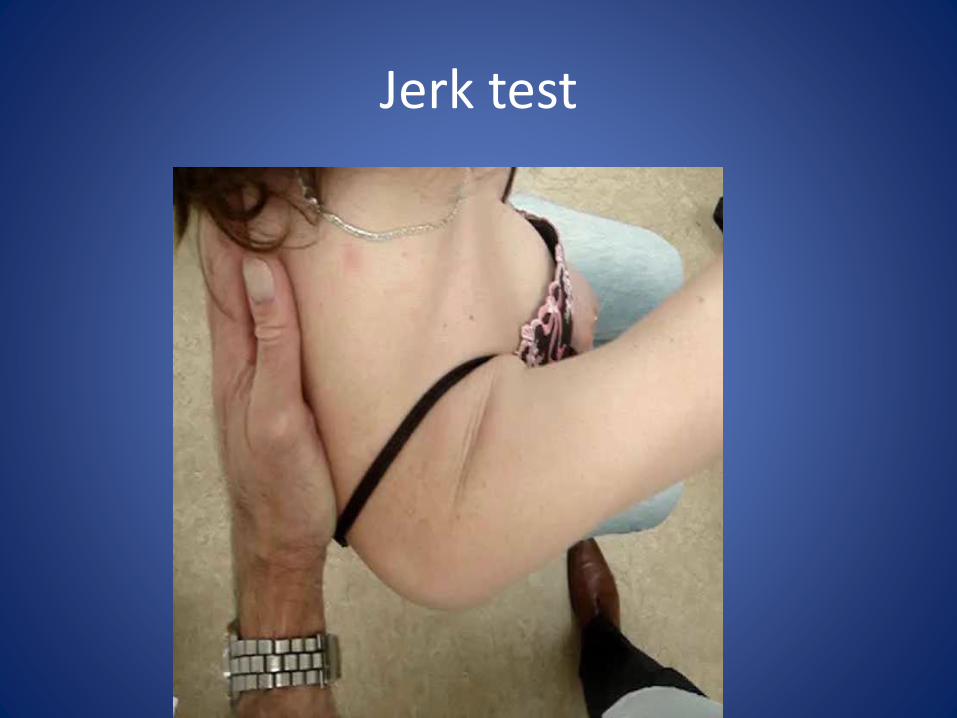
Jerk test
• Dynamic test, simulates posterior subluxation and reproduces symptoms
• Axial posterior load onto a arm flexed at 90°, adducted and internally rotated
• Predictive measure for non-operative treatment
Kim, 2001
Jerk test
Pathophysiology
• Bony anatomic deformities
• Excessive capsular laxity
• Labral lesions
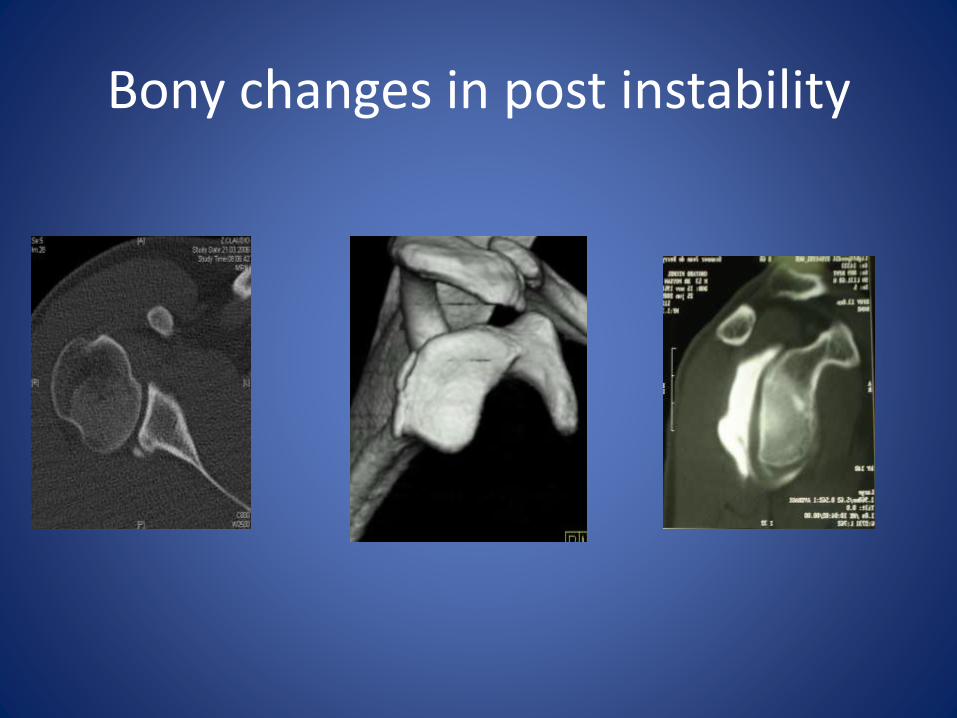
Bony changes in post instability
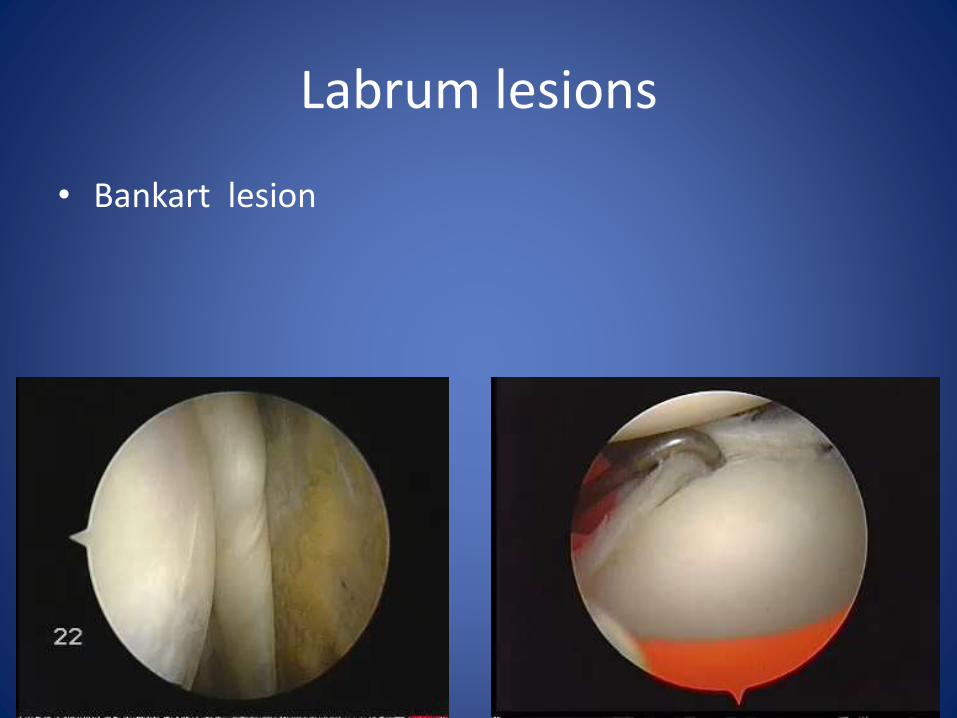
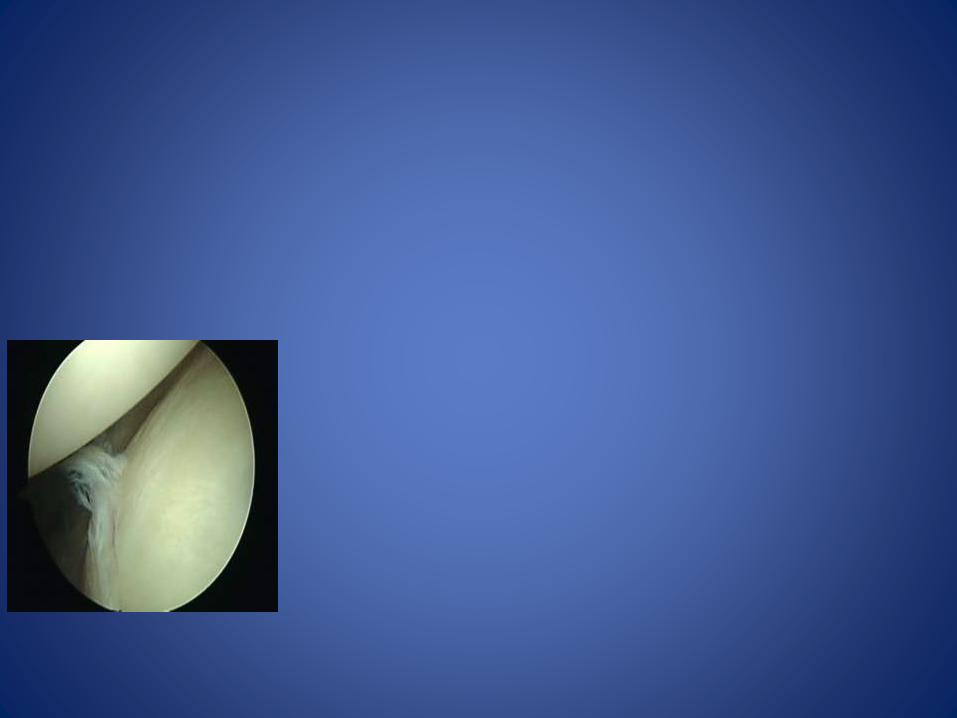
Labrum lesions
• Bankart lesion
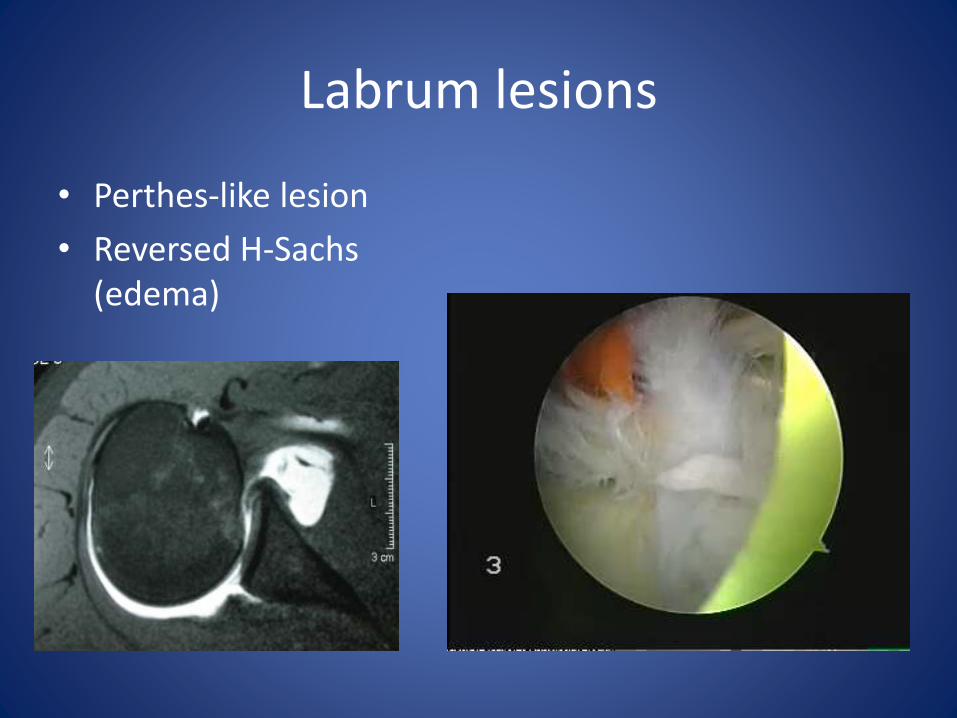
Labrum lesions
• Perthes-like lesion
• Reversed H-Sachs (edema)
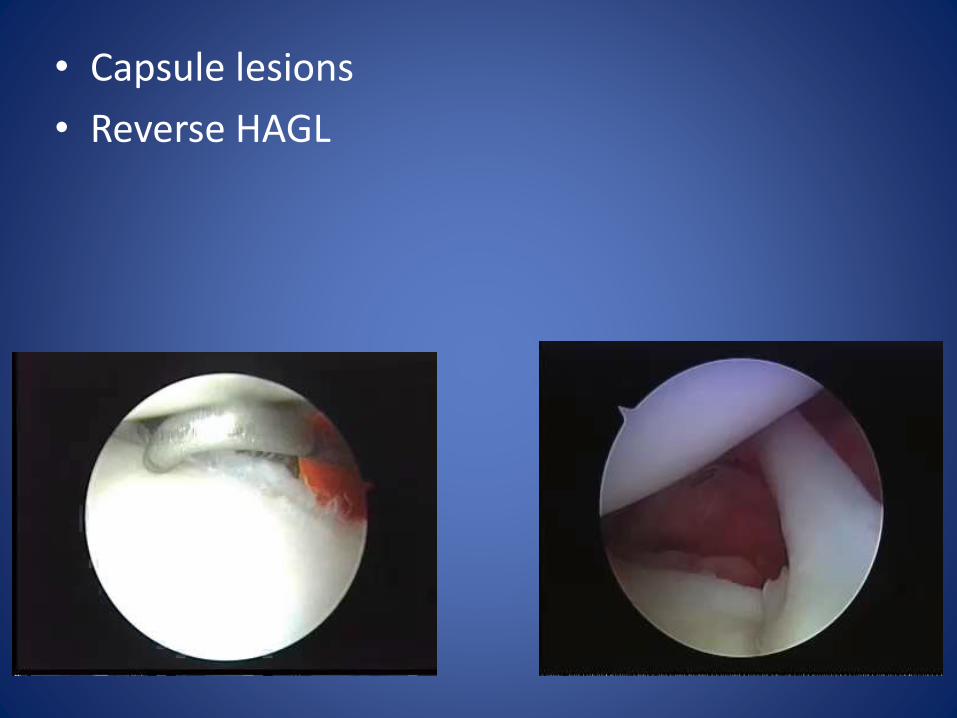
• Capsule lesions
• Reverse HAGL
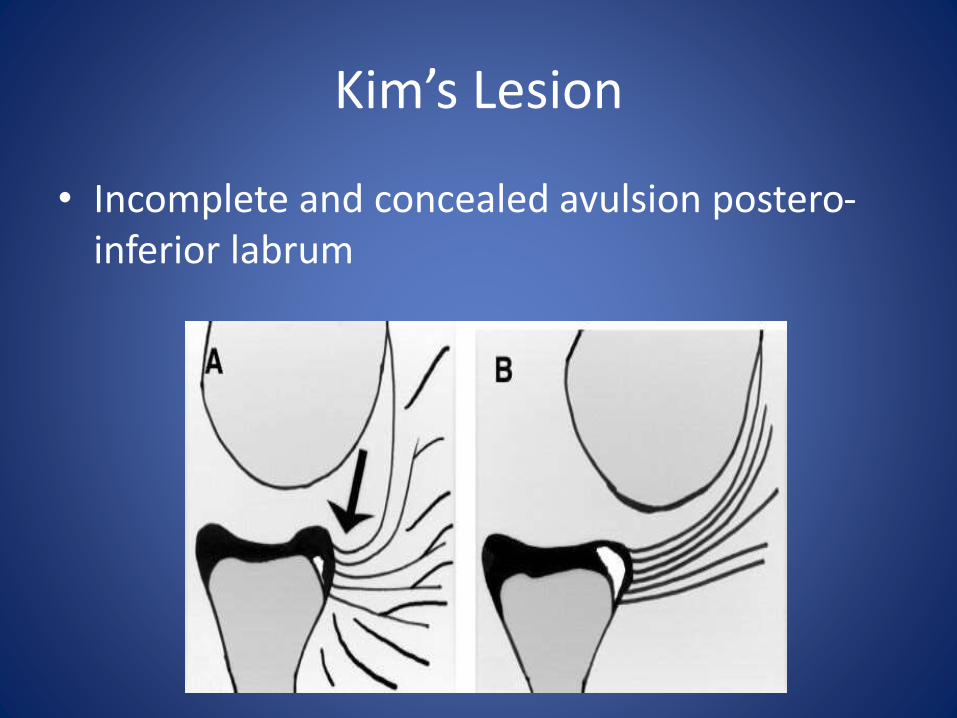
Kim’s Lesion
• Incomplete and concealed avulsion postero-inferior labrum
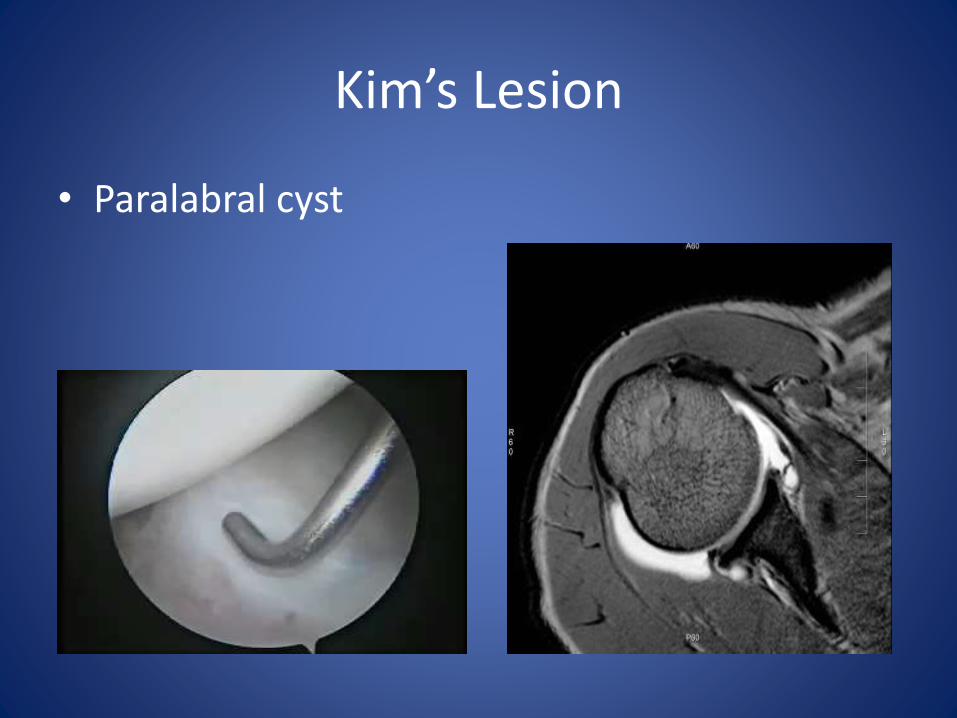
Kim’s Lesion
• Paralabral cyst
Voluntary instability
• No indication for surgery
• However:
subset of patients, who start with VI
turning into involuntary instability
Treatment of posterior instability
• Open treatment modalities
• open capsulorraphy
• glenoid osteotomy
• bone block procedure
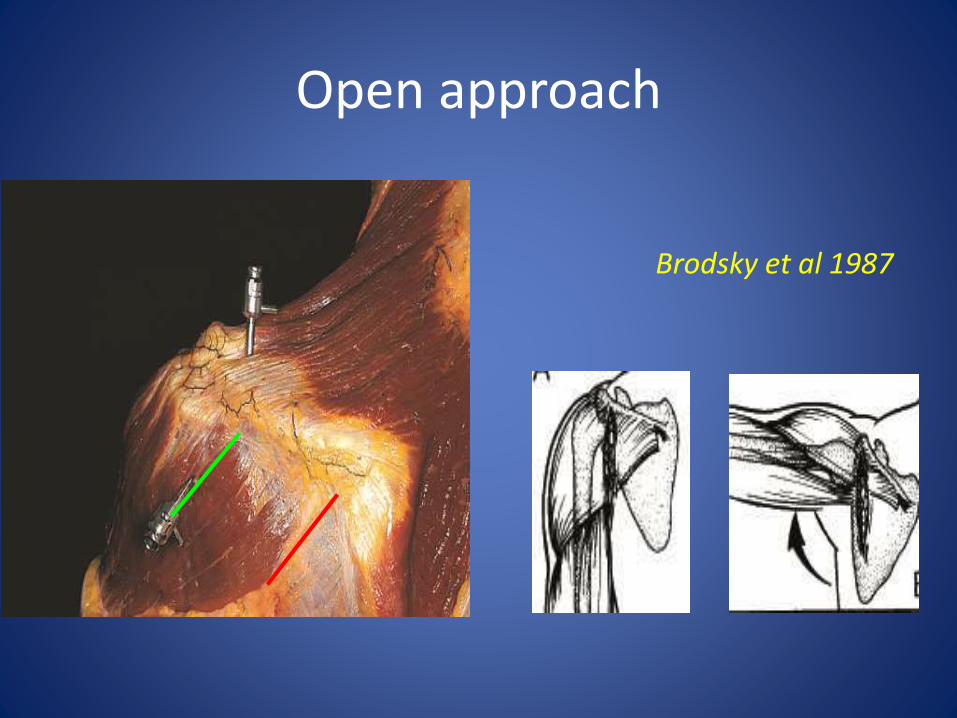
Open approach
Brodsky et al 1987
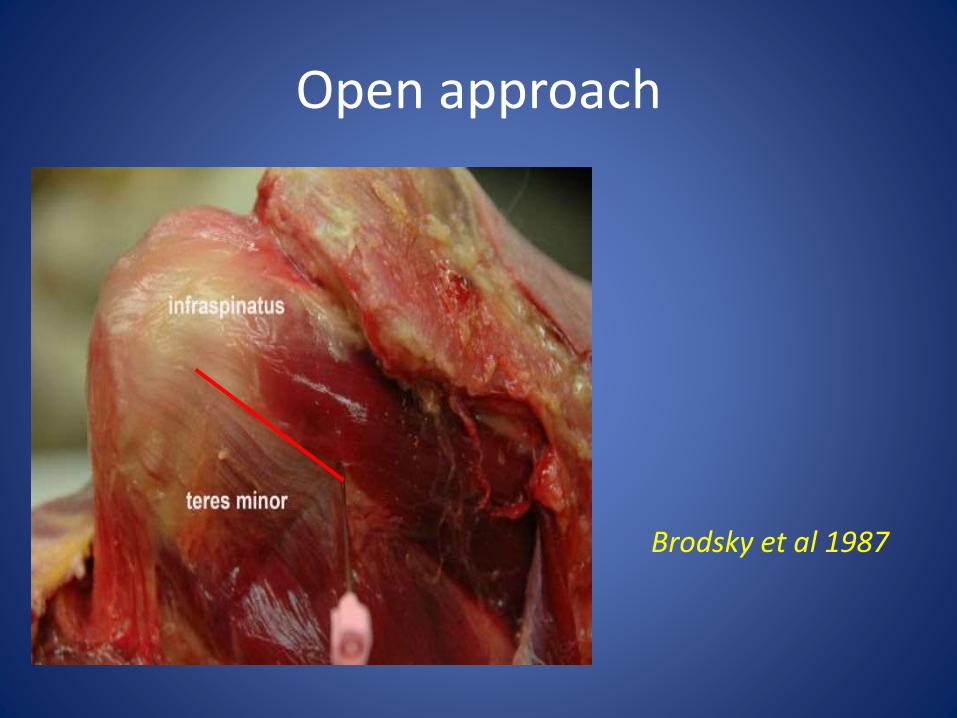
Open approach
Brodsky et al 1987
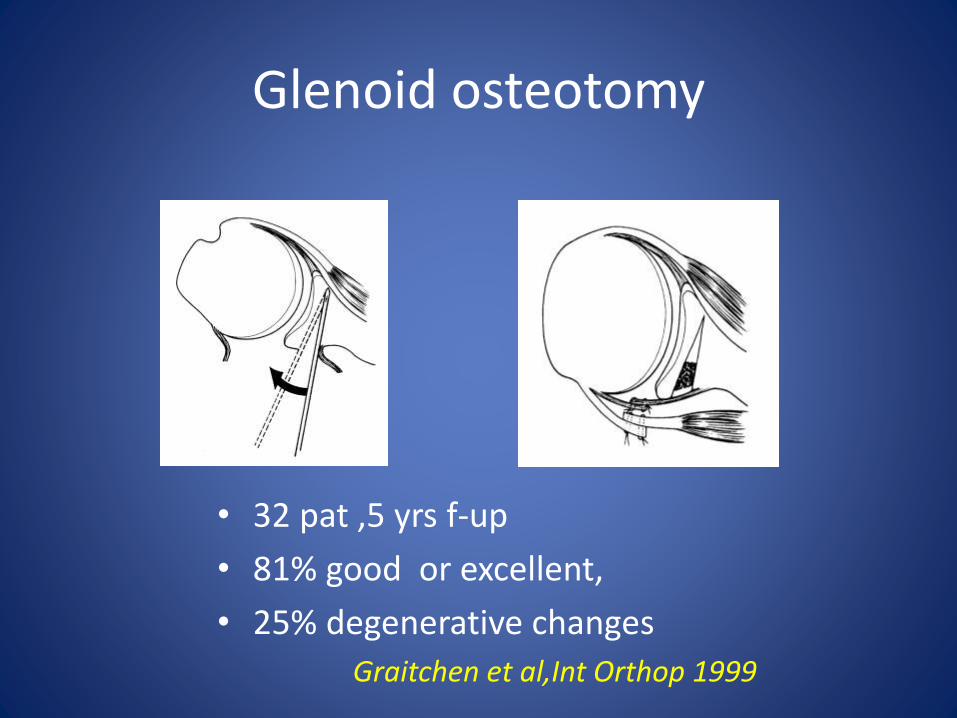
Glenoid osteotomy
• 32 pat ,5 yrs f-up
• 81% good or excellent,
• 25% degenerative changes
Graitchen et al,Int Orthop 1999
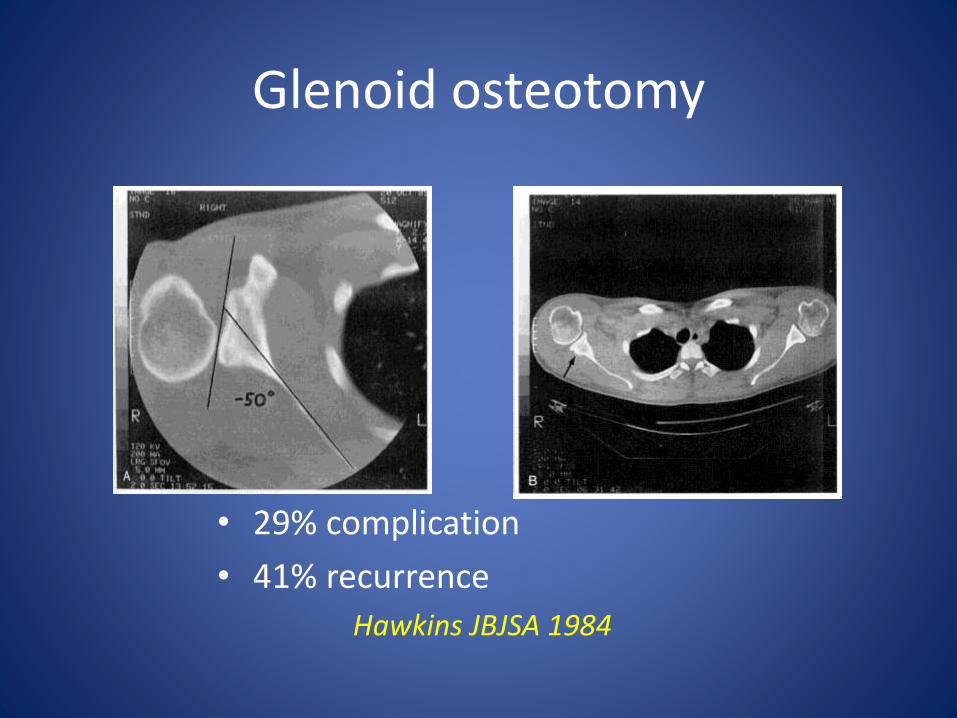
Glenoid osteotomy
• 29% complication
• 41% recurrence
Hawkins JBJSA 1984
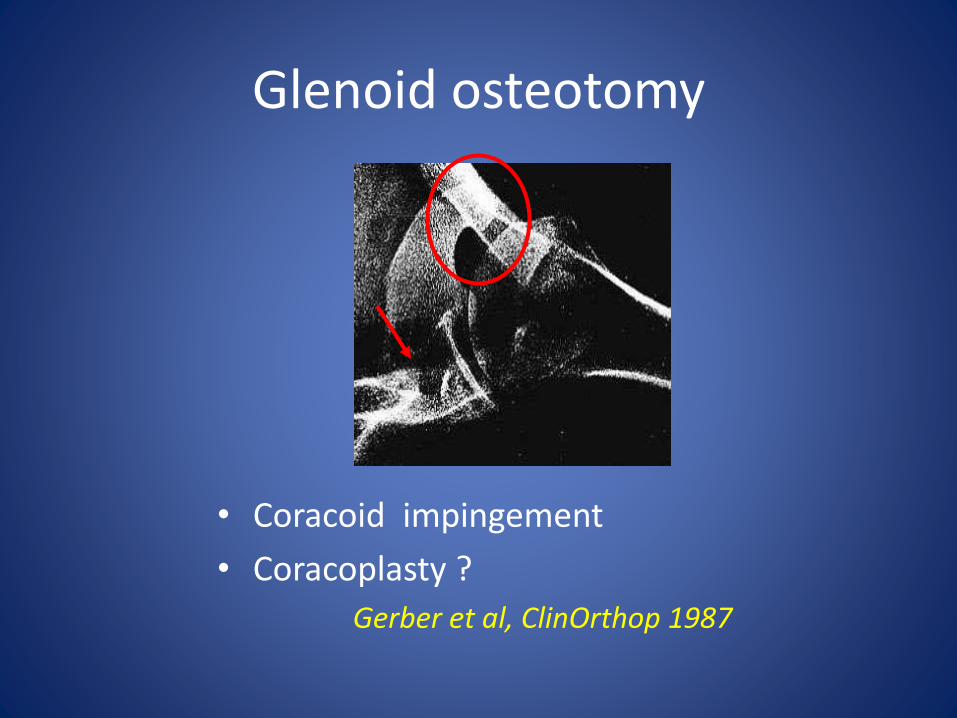
Glenoid osteotomy
• Coracoid impingement
• Coracoplasty ?
Gerber et al, ClinOrthop 1987
Bone block
• 20 patients with involuntary instability
• Posterior bone block, 5-10 mm overhang
• 3 failures; 60% very satisfied, 40% satisfied
Walch et al, KSSTA 2007
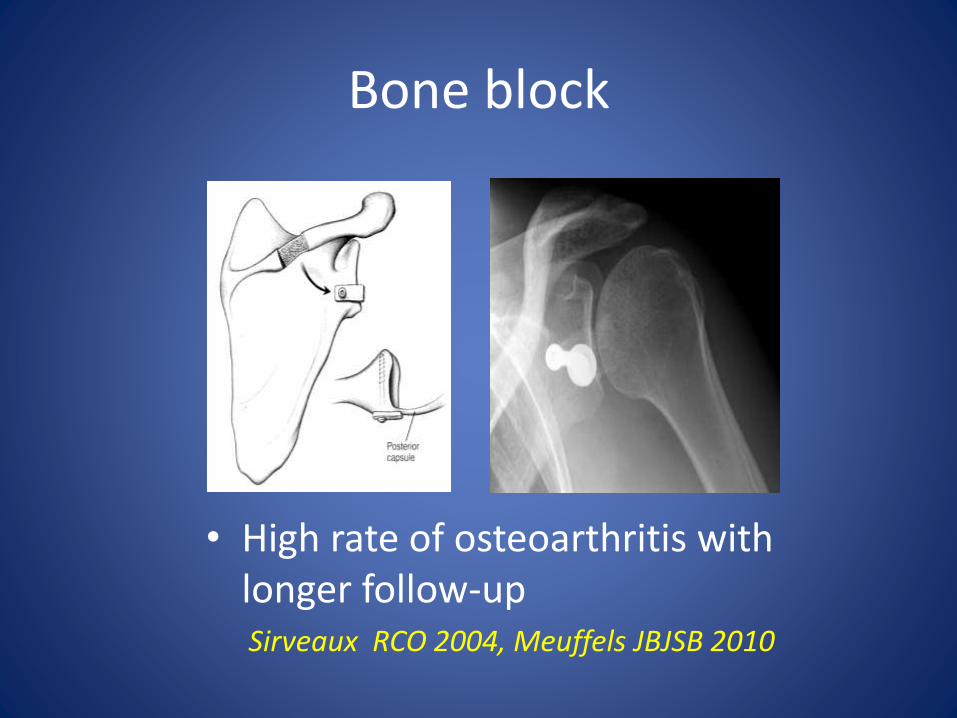
Bone block
• High rate of osteoarthritis withlonger follow-upSirveaux RCO 2004, Meuffels JBJSB 2010
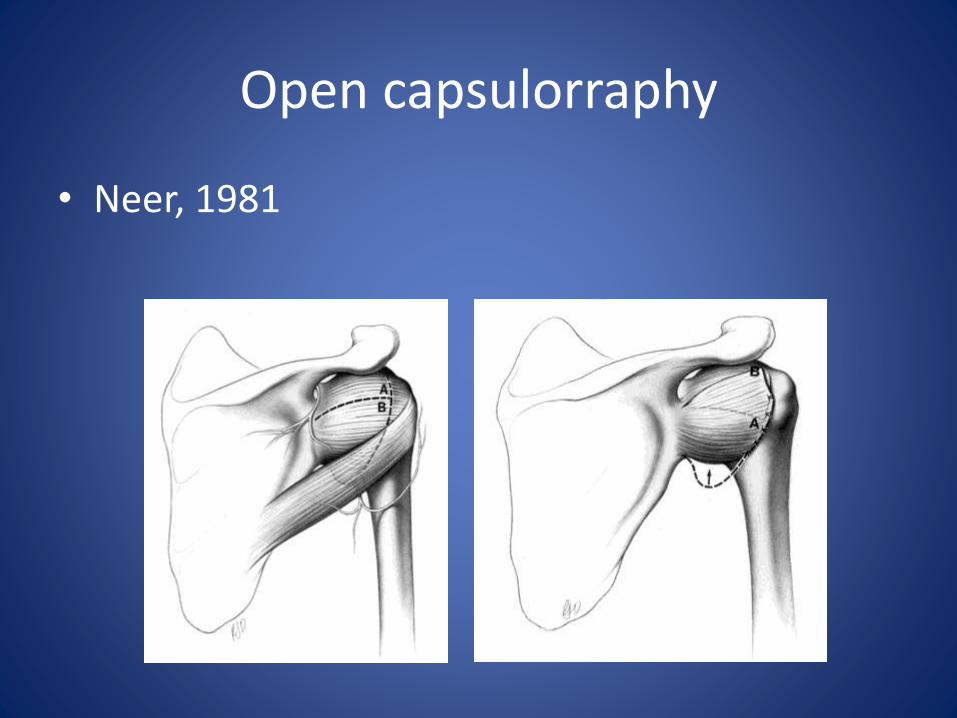
Open capsulorraphy
• Neer, 1981

Arthroscopic treatment
• with or without labral detachment
• labral repair +/- capsulorraphy
• rotator interval ?
Capsulorraphy
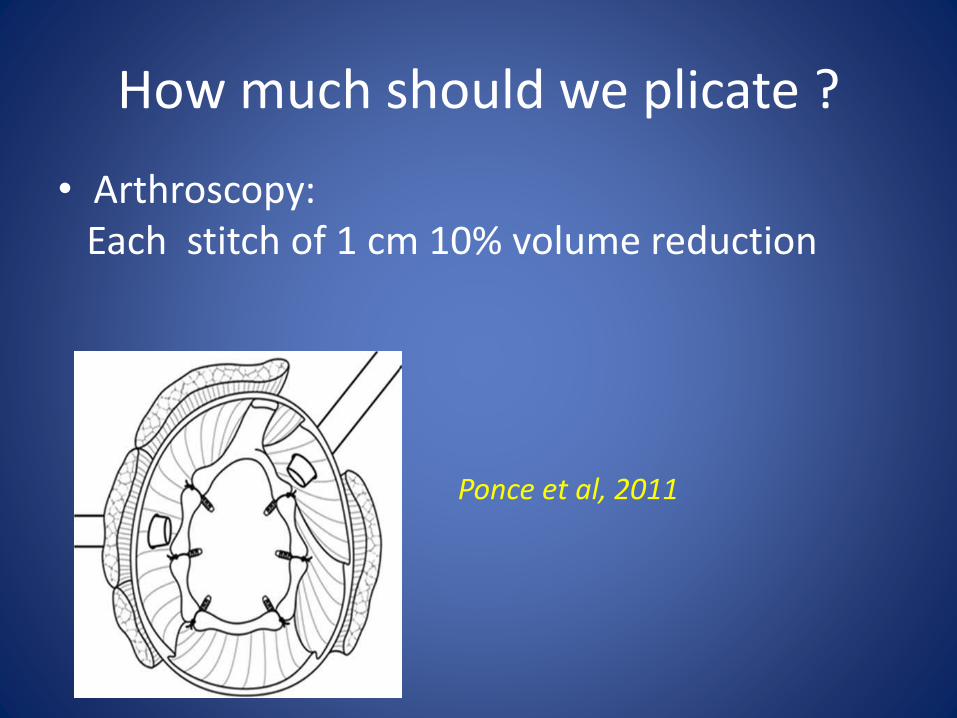
How much should we plicate ?
• Arthroscopy:Each stitch of 1 cm 10% volume reduction
Ponce et al, 2011
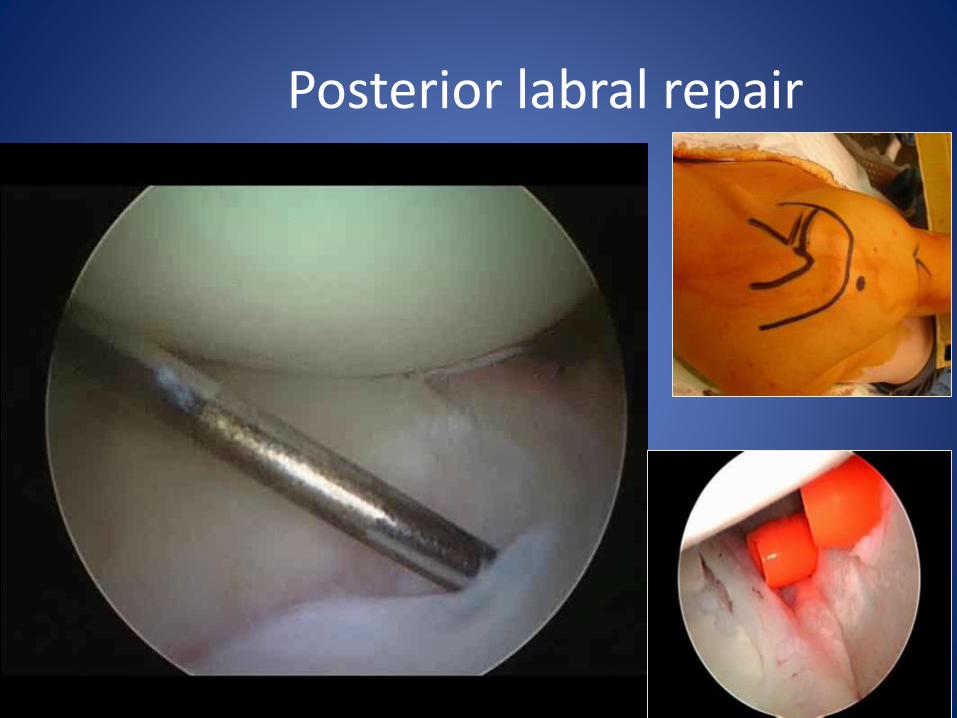
Posterior labral repair
• Comprehensive analysis open and @ soft tissue repair of posterior instability
Kakar et al Am.J Orthop 2007
open : 173 ( 9 studies)
@ : 186 ( 7 studies)
satisfaction and return to sports : equal
Thank you for your attention
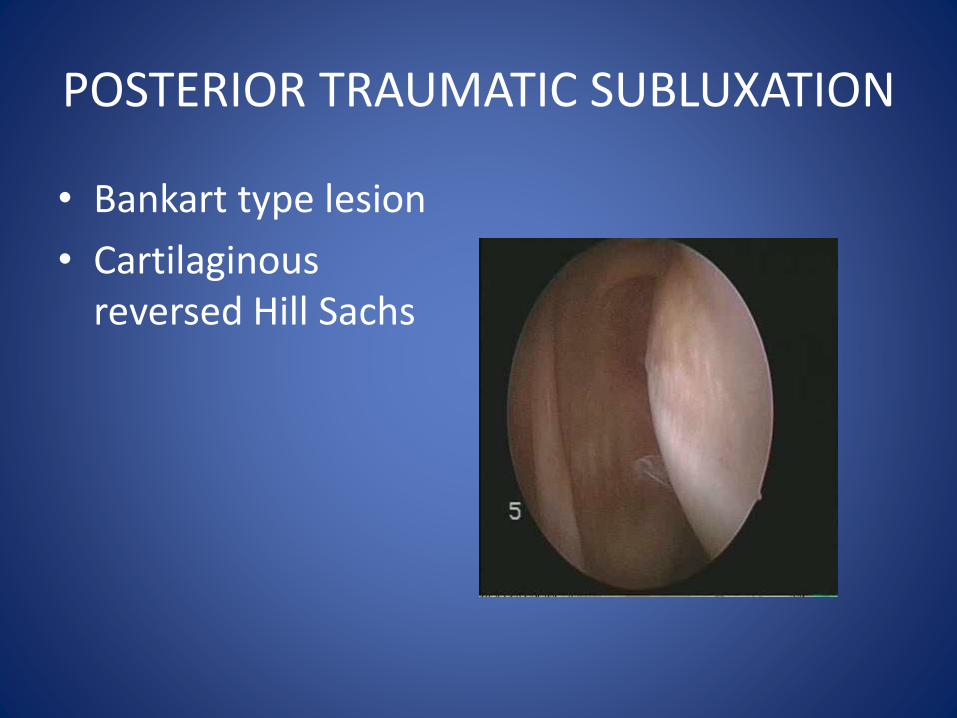
POSTERIOR TRAUMATIC SUBLUXATION
• Bankart type lesion
• Cartilaginous reversed Hill Sachs
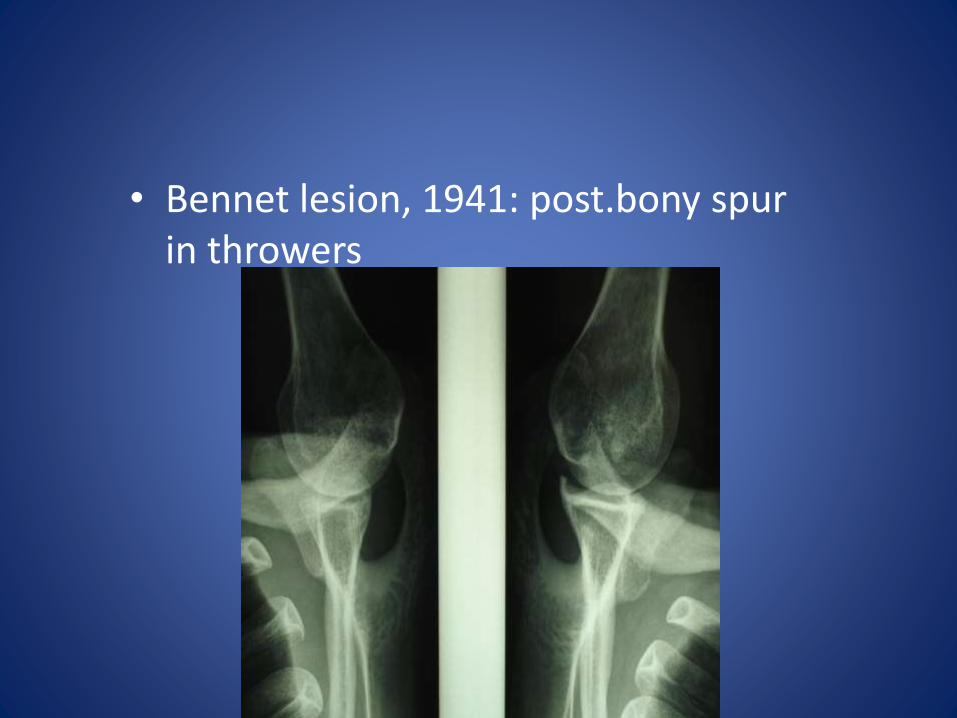
• Bennet lesion, 1941: post.bony spur in throwers
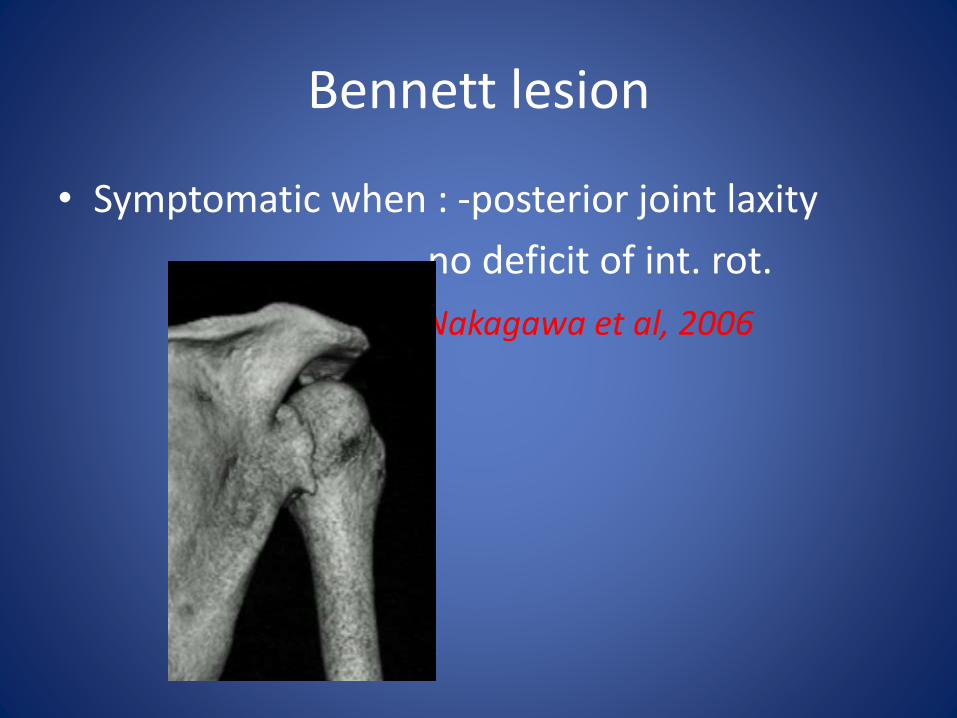
Bennett lesion
• Symptomatic when : -posterior joint laxity
- no deficit of int. rot.
Nakagawa et al, 2006
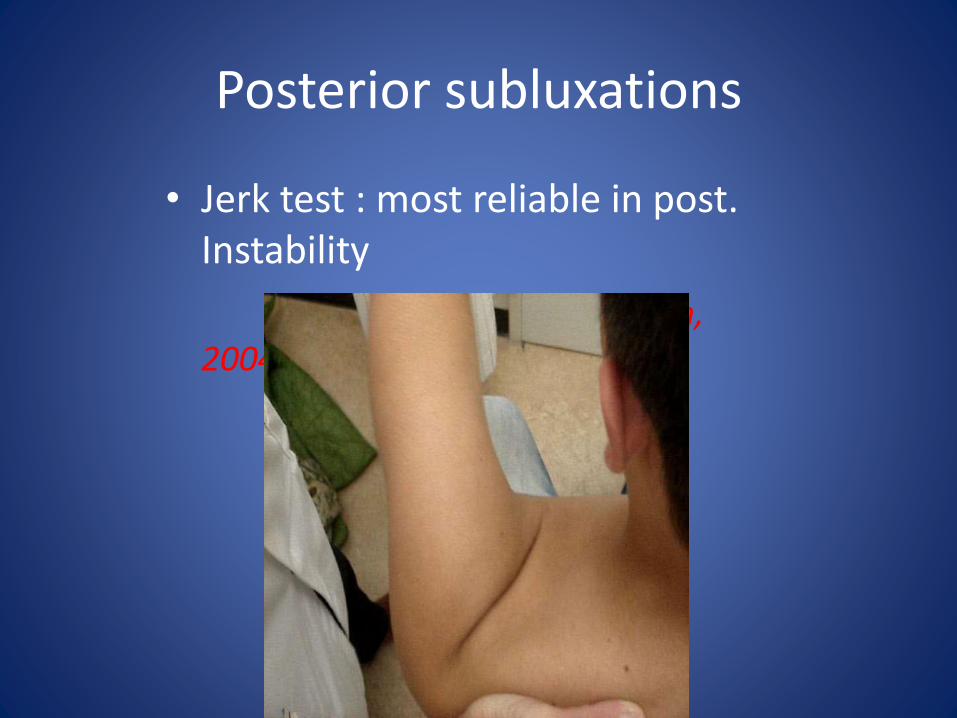
Posterior subluxations
• Jerk test : most reliable in post. Instability
Kim, 2004
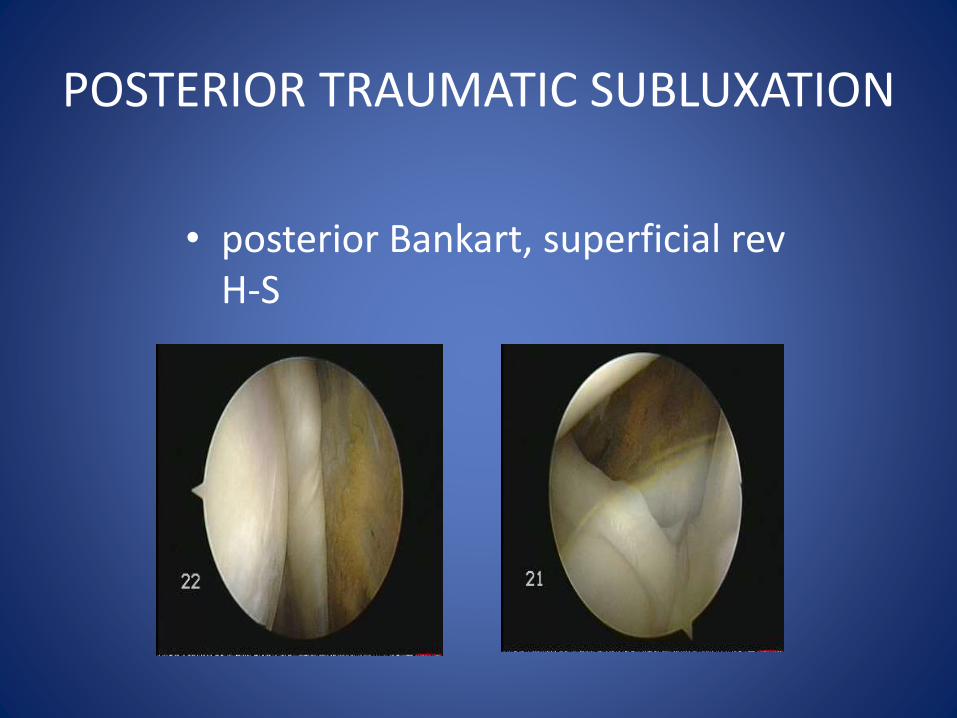
POSTERIOR TRAUMATIC SUBLUXATION
• posterior Bankart, superficial rev H-S
POSTERIOR TRAUMATIC SUBLUXATION
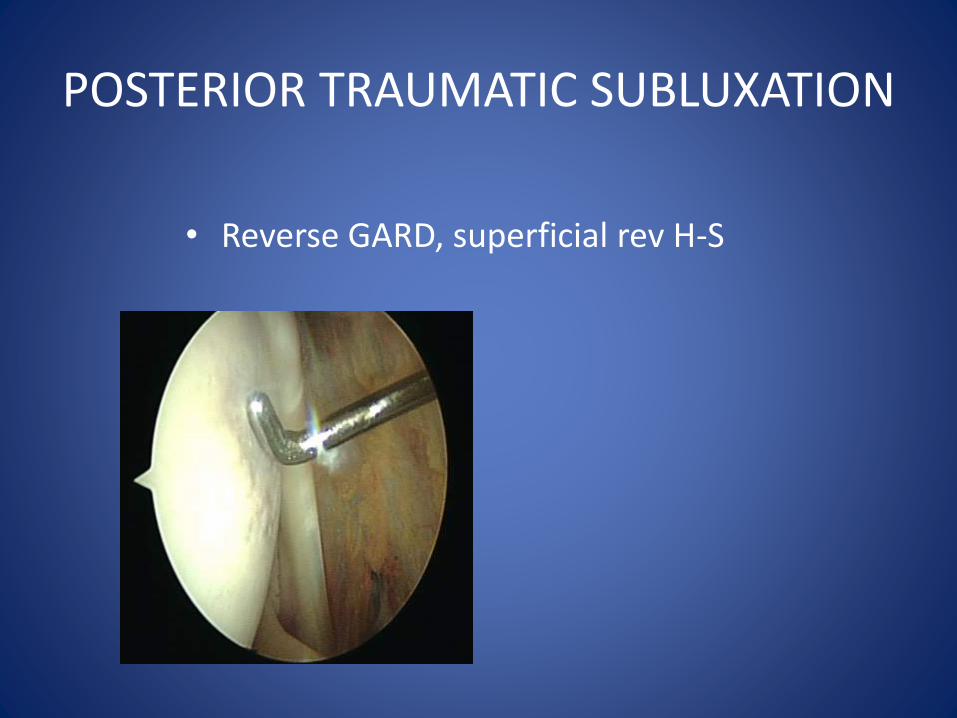
• Reverse GARD, superficial rev H-S
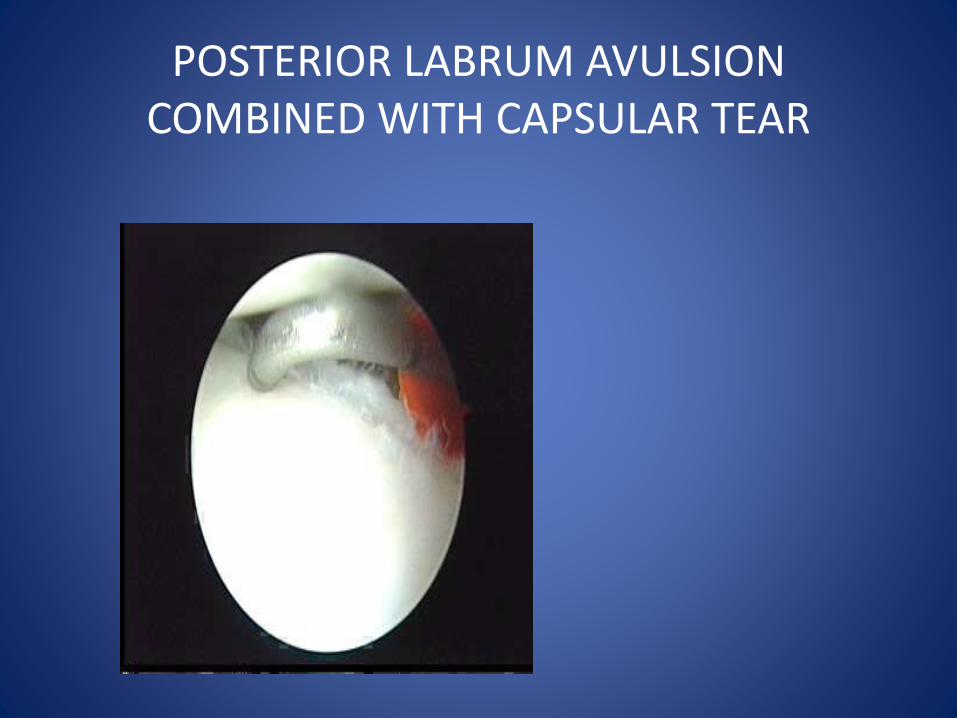
POSTERIOR LABRUM AVULSION COMBINED WITH CAPSULAR TEAR

Reverse HAGL
ANATOMY OF POSTERIOR LABRUM
• Detrisac and Johnson:
• 2 types: -wedge labrum
-firmly attached
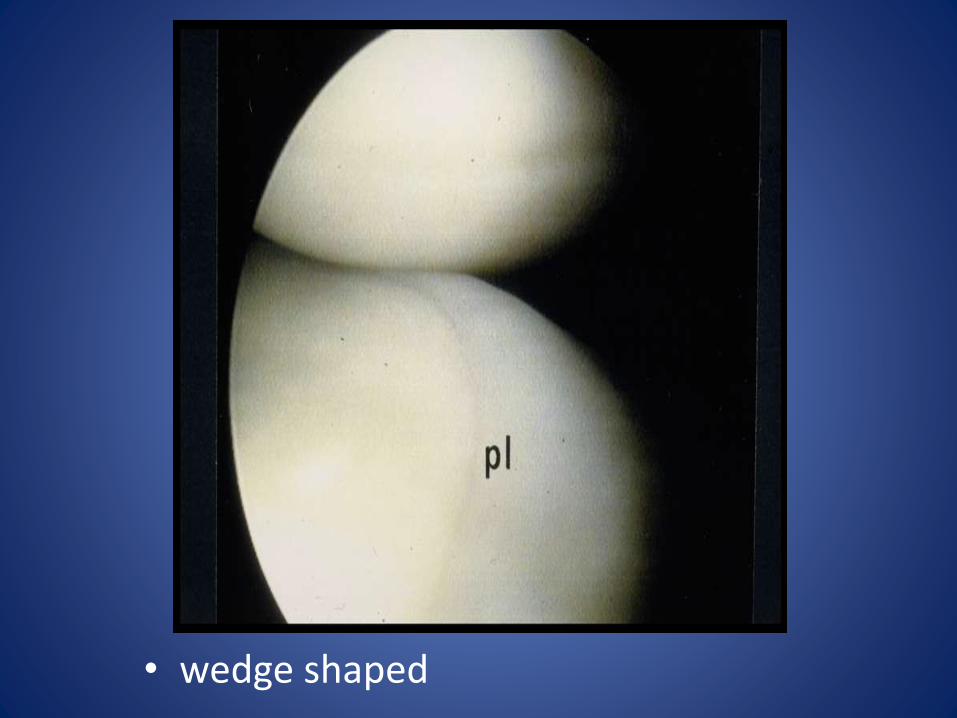
• wedge shaped
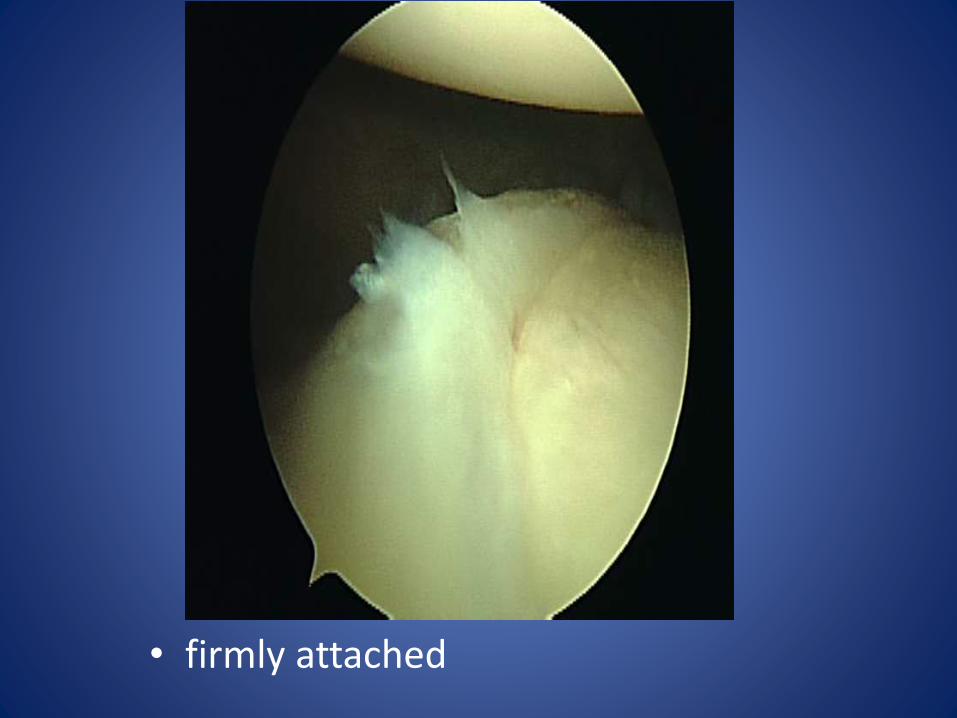
• firmly attached