post icd-10 clinical documentation improvement (cdi
TRANSCRIPT

1
Post ICD-10 Clinical Documentation Improvement (CDI) Program RevitalizationNorth Carolina Health Information Management Association
May 4, 2016
MeShawn Foster, RHIT, MJ Senior Consultant, Deloitte & Touche LLP
Peggy Meli, PhD, RHIA, CHC, LHRM (FL)Specialist Master, Deloitte & Touche LLP

2
Session objectives
• Assess previous state (ICD-9) of CDI program against current state post ICD-10
• Identify and leverage leading practices in clinical documentation and when to modify program with ICD-10
• Discuss impact ICD-10 has had on CDI programs
• Discuss impact of technology systems with CDI programs
• Discuss key performance metrics to monitor CDI program’s operations and success
• Better understanding of reimbursement systems
3
Introduction
Previous state
Current state
Revitalization of a CDI program is a proactive step that an organization may take to trend towards leading practices and enhance the quality of an existing program.
• What were our processes?• How was performance
tracked and monitored?• What technology was
used?• What was our program
visibility?
• Have our processes changed?• Did we modify our tracking and
monitoring?• What are our technology needs?• How visible is our program?
Beginning with a state-to-state assessment can allow for identification of gaps, changes, and improvements.
Copyright © 2016 Deloitte Development LLC. All rights reserved.

4
State-to-state assessment A robust assessment should consider people, processes, tools and sustainability.
PEOPLE
WHAT?
PROCESSESHOW?
TOOLS
WHO?
SUSTAINABILITY
Copyright © 2016 Deloitte Development LLC. All rights reserved.

5
State-to-state assessment (cont.)
What is the vision?
Identifying Gaps
Continual Monitoring
• Develop a vision for the CDI program that aligns with established leading practice goals
• Identify your stakeholders and obtain their buy‐in for continual improvement
• Develop an internal benchmark based on previous state peak results
• Define benchmarks for your organization• Evaluate previous and current state against
defined leading practices• Document gaps and develop a strategy for
minimization
• Perform initial monitoring as a comparative before transitioning to continual qualitative analysis
• Shift monitoring to accommodate productivity changes due to ICD‐10
• Develop ongoing monitoring process with automation where possible
Copyright © 2016 Deloitte Development LLC. All rights reserved.

6
CDI Program Sustainability Post ICD-10
Clinical Documentation Stakeholder Collaboration
• Strong and consistent operational leaders and managers
• Teaming and communication between CDI Specialists, Coders and Physicians
Clinical Documentation Governance
• Physician and executive leadership engagement
• Physician communication• Alignment with related
enterprise initiatives (e.g., system replacement)
Enterprise Technologies & Tools
• Operational tools to drive daily workflow, documentation and tracking of work and exceptions flagging
• Clinical documentation customized query templates within the EMR and/or CDI tool
• Education and training tools in multiple formats
• Interoperable CDI tools
Metrics & Performance Management
Operational Sustainability
• Monitoring and reporting tools to track results in terms of case mix index (CMI), severity of illness (SOI), risk of mortality (ROM) and patient safety indicators (PSI)
Process Standardization
• Resilient governance structure
• Periodic external review and feedback
• Annual CDI Specialist and Coder training
• CDI performance metrics for physicians, CDI, coding and management
• Structured policies and procedures to standardize program requirements
• Specialty‐specific approach to physician training
• Consistent coding accuracy program
Copyright © 2016 Deloitte Development LLC. All rights reserved.

7
Identifying Leading PracticesAn organization may define leading practices according to best practices established by American Health Information Management Association (AHIMA) and Association for Clinical Documentation Improvement Specialists (ACDIS)
Deloitte Advisory has developed a maturity model to help organizations determine the current state of the program compared to their desired future state.
I ‐ Beginning II ‐ Developing III ‐ Effective IV ‐ Advanced V ‐ Exceptional
The Maturity Model offers a structured mechanism to assess an organization’s performance against industry leading practices.
Copyright © 2016 Deloitte Development LLC. All rights reserved.

8
Modifying Existing ProgramsAssessment results should provide an indication of how mature your current CDI program is along with identifying opportunities with ICD-10 to advance your program further.
I - Beginning II - Developing III - Effective IV - Advanced V -Exceptional
• Little to no policies and procedures
• Decentralized operations
• Polices and procedures exist but not documented
• Limited Centralization
• Standardized, documented, applied and enforced polices and procedures
• Polices and procedures are routinely tested to confirm compliance
• Serve as a model for other organizations; shared service centersPr
oces
ses

9
Common ICD-10 Impacts to CDI ProgramsICD-10 has created opportunities to better capture medical necessity, further identify severity of illness, and enhanced detail of conditions and procedures that will lead to better management of healthcare quality.
• Understanding key focus areas for diagnoses that require specific documentation in order to be coded
• Emphases on translation of clinical language to coding language to better capture full clinical picture of patients
• Clarifying that Documentation of suspected, possible and probable conditions when treatment and monitoring is occurring is appropriate
• Recognizing overall DRG shifts due to changes between the code sets
• Performing mortality reviews for cases that have APR-DRG SOI and ROM that is less than 4
• Identify top Medicare Severity Diagnosis Related Groups (MS-DRGs) and top surgeries and determine potential shifts and/or documentation challenges
Documentation
Reimbursement
Copyright © 2016 Deloitte Development LLC. All rights reserved.

10
TechnologySelection of vended software is an essential element to advancing and revitalizing a CDI program post ICD-10.
Is there interoperability with my EMR?
What are the reporting capabilities?
Will benchmarking beavailable?
Is the return on investment substantial?
Copyright © 2016 Deloitte Development LLC. All rights reserved.

11
Key Performance MetricsOngoing monitoring of key performance metrics enables tracking and trending towards a leading CDI program.
CDI Metrics
Initial Review Volume
Physician Agreement and Response Rates
Query Rates (Concurrent and Retrospective) and DRG mismatch rates
Follow-up Review Volume
Copyright © 2016 Deloitte Development LLC. All rights reserved.
12
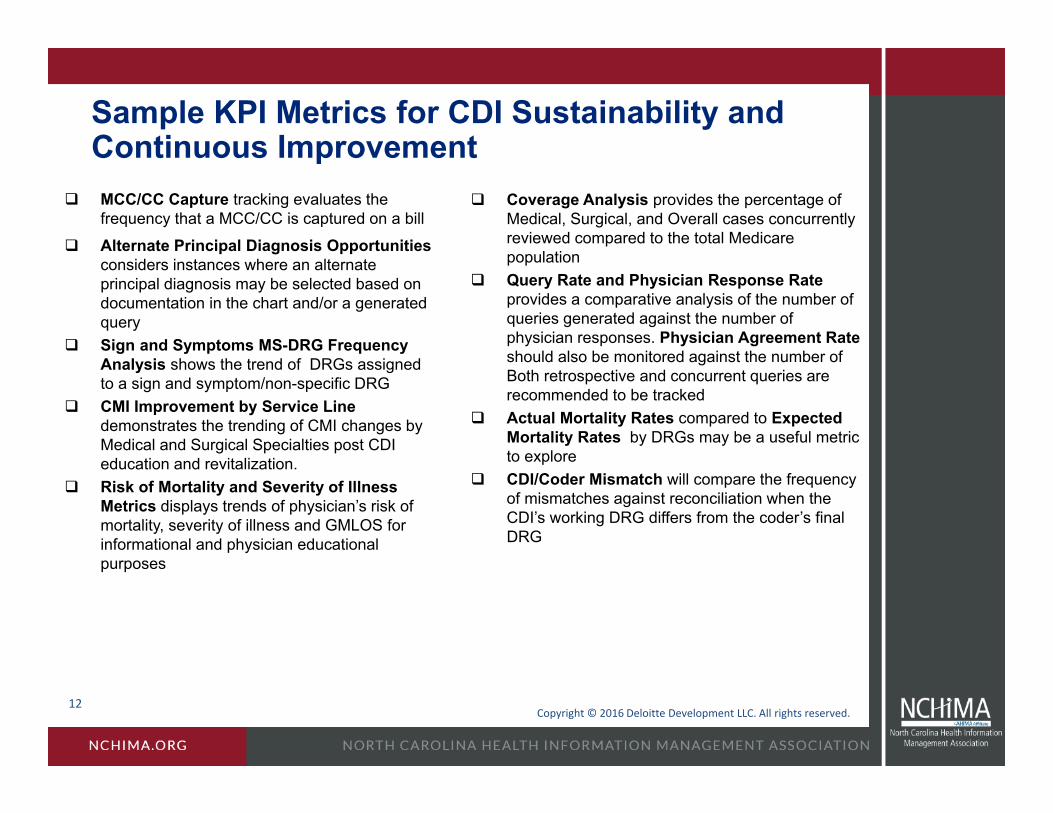
Sample KPI Metrics for CDI Sustainability and Continuous Improvement
MCC/CC Capture tracking evaluates the frequency that a MCC/CC is captured on a bill
Alternate Principal Diagnosis Opportunities considers instances where an alternate principal diagnosis may be selected based on documentation in the chart and/or a generated query
Sign and Symptoms MS-DRG Frequency Analysis shows the trend of DRGs assigned to a sign and symptom/non-specific DRG
CMI Improvement by Service Line demonstrates the trending of CMI changes by Medical and Surgical Specialties post CDI education and revitalization.
Risk of Mortality and Severity of Illness Metrics displays trends of physician’s risk of mortality, severity of illness and GMLOS for informational and physician educational purposes
Coverage Analysis provides the percentage of Medical, Surgical, and Overall cases concurrently reviewed compared to the total Medicare population
Query Rate and Physician Response Rate provides a comparative analysis of the number of queries generated against the number of physician responses. Physician Agreement Rate should also be monitored against the number of Both retrospective and concurrent queries are recommended to be tracked
Actual Mortality Rates compared to Expected Mortality Rates by DRGs may be a useful metric to explore
CDI/Coder Mismatch will compare the frequency of mismatches against reconciliation when the CDI’s working DRG differs from the coder’s final DRG
Copyright © 2016 Deloitte Development LLC. All rights reserved.

13
Understanding Reimbursement SystemsClassification of inpatient stay resource intensity and illness severity is tied to reimbursement groupings. These groupings helps measure the case mix of an entity’s patient population.
MS-DRG
APR-DRG
• MS-DRGs are assigned to each inpatient stay.• MS-DRGs are divided into 25 major diagnostic categories (MDCs)• Select diagnosis codes are categorized as major
complications/comorbidities (MCCs) or complications/comorbidities (CCs)
• MS-DRGs have a weighted value depending on whether they are a single, pair or triplet combination inclusive of MCCs/CCs
• All Patient Refined Diagnosis Related Groups (APR-DRGs) focus on resource intensity
• There are 315 base APR-DRGs• There are two sets of subclasses, SOI and ROM that are added to the
base• APR-DRG is driven by principal diagnosis, procedures performed, all
secondary diagnoses, age and gender
Copyright © 2016 Deloitte Development LLC. All rights reserved.

14
Calculating Case Mix IndexCase Mix Index is calculated using the average diagnosis related group relative weight for a hospital.
DRG RW # of Cases Total RW
195 Simple pneumonia w/o MCC/CC 0.7044 9 6.3396193 Simple pneumonia with MCC 1.4491 12 17.3893291 Heart failure with MCC 1.5097 5 7.5485293 Heart failure w/o MCC/CC 0.6762 10 6.7620689 UTI w MCC 1.1172 4 4.4688682 Renal Failure with MCC 1.5194 5 7.5970683 Renal Failure w CC 0.9512 3 2.8536871 Septicemia w/o vent w MCC 1.8072 4 7.2288872 Septicemia w/o vent w/o MCC 1.0528 3 3.158465 Intracranial hemorrhage or cerebral infarction w CC 1.0643 5 5.3215
Total 60 68.6675
CMI = Sum of RW / Total # of Cases 1.1444
Copyright © 2016 Deloitte Development LLC. All rights reserved.

15
Severity of Illness and Risk of Mortality
The focus of the CDI department is to emphasis on improving the overall quality of the documentation regardless of the impact on CC/MCC capture
SOI and ROM are scored on a scale of 1-4
Recognizing the importance of SOI/ROM The mortality index is the ratio of actual deaths to
expected deaths:• Secondary diagnoses capture impacts to the
expected mortality rate The SOI/ROM scores are a key component in the
algorithm used to calculate the expected mortality rateHow is the SOI/ROM determined? Each diagnosis has its own intrinsic SOI/ROM value
of 1–4 A complex formula is used to calculate the SOI/ROM
of the DRG/case In order for the DRG/case to be a 4/4, at least two
diagnoses used to calculate the DRG must have a value of 4/4
Through complete documentation, physicians accurately represent their patient’s severity of illness and risk of mortality
1 = minor2 = moderate3 = major4 = extreme
Copyright © 2016 Deloitte Development LLC. All rights reserved.

16
Reimbursement Systems and Your PatientWithout
Accurate and Complete Documentation
WithAccurate and Complete
Documentation
Primary Diagnosis Urosepsis Septicemia
Secondary Diagnoses Dehydration Dehydration
COPD COPD
UTI
Malnutrition
Stage 1 Pressure Ulcer
Septic Shock
Medicare DRG690: Kidney and Urinary Tract Infection 871: Septicemia w/o MV
Medicare Relative DRG Weight 0.7794 1.8072
Reimbursement: $4600 $10,666 6066 ~$ change
MS-DRG Expected Length of Stay 3.1 days 5.1 days 2 days added
APR DRG 463 720
Severity of Illness Level 2 Moderate 4 Extreme
Risk of Mortality Level 2 Moderate 4 Extreme
SOI Weight 0.5253 2.7338 5 X increase
Expected Mortality Rate 1.0% 47.4% 46 point increaseCopyright © 2016 Deloitte Development LLC. All rights reserved.
17
Key Takeaways
• ICD-10 offers an opportunity to obtain better quality data due to the specificity offered within the code set
• A leading CDI program can leverage ICD-10 with a focus on documentation that should better reflect the severity of the patient substantiating resource use
• A leading CDI program should have a holistic approach that considers quality, complete documentation and reimbursement
• A leading CDI program increases MCC and CC capture, reflects the correct SOI/ROM values and potentially raises case mix
• Known shifts should be examined and monitored to determine their impact post ICD-10
Copyright © 2016 Deloitte Development LLC. All rights reserved.
18
Questions
Q A
Copyright © 2016 Deloitte Development LLC. All rights reserved.

19
AppendixBios and Contact Information

20
Speaker Bios
QA
Peggy Meli, PhD, RHIA, CHC, LHRM, Deloitte Advisory Specialist Master Deloitte & Touche LLP
Dr. Peggy Meli provides HIM operations, coding and clinical documentation reviews as well as Legal EHR designation, release of information operations, HIPAA compliance, ICD-10-CM/PCS coding, HIM IT coordination and healthcare risk management functions, training and educational solutions for healthcare facilities and physician practices. Peggy’s recent engagements at Deloitte Advisory include HIM Interim Management, ICD-10 implementation and charge capture review, Clinical Documentation Excellence and monitoring, ICD-10-CM/PCS Training and Implementation and HIM and coding review and process improvement. Additional engagements have included professional fee (E& M) coding, auditing, and physician compliance reviews.
Vickie Monteith, RN, MBA, Deloitte Advisory Director, Deloitte & Touche LLP
Vickie is Deloitte Advisory’s national leader for the ICD-10 and Clinical Information Integrity and Maturity (CIIM) solutions, and co-leads the Clinical Documentation Excellence (CDE) practice. She has more than 27 years of experience in the healthcare industry in the areas of scheduling, patient access, medical necessity processing, utilization management, case management, medical records, patient accounting, billing compliance, charge integrity, chart-to-bill audits, CDE, charge description master (CDM) reviews and standardization, compliance risk assessments, compliance effectiveness reviews, compliance program development, internal control reviews, Recovery Audit Contractor (RAC) readiness, Medicare compliance, ICD-10, nursing, and supply chain.
Copyright © 2016 Deloitte Development LLC. All rights reserved.

21
Speaker Bios, cont.
QA
MeShawn Foster, MJ, RHIT, Deloitte Advisory Senior ConsultantDeloitte & Touche LLP
MeShawn is a senior consultant in Deloitte’s Advisory health care practice with significant health information management experience focusing on finance, operations, and risk transformation in both the provider and payer environments. MeShawn possesses robust and diverse experience in end-to-end revenue cycle, data management governance, information governance, health system implementation, remediation, provider auditing, clinical documentation improvement, data analysis, ICD-9, ICD-10 and CPT coding and billing, payer system remediation, policy development, legal research, and technical solutions.
Copyright © 2016 Deloitte Development LLC. All rights reserved.

22
QPeggy Meli Specialist Master | Deloitte Advisory Deloitte & Touche LLP [email protected]+1 813 480 9673
MeShawn FosterSenior Consultant | Deloitte AdvisoryDeloitte & Touche [email protected]+1 904 608 8807
Contact Information
Vickie MonteithDirector | Deloitte AdvisoryDeloitte & Touche LLP [email protected]+1 704 906 2221
Copyright © 2016 Deloitte Development LLC. All rights reserved.

23
QThis presentation contains general information only and Deloitte Advisory is not, by means of this presentation, rendering accounting, business, financial, investment, legal, tax, or other professional advice or services. This presentation is not a substitute for such professional advice or services, nor should it be used as a basis for any decision or action that may affect your business. Before making any decision or taking any action that may affect your business, you should consult a qualified professional advisor.
Deloitte Advisory shall not be responsible for any loss sustained by any person who relies on this presentation.
As used in this document, “Deloitte Advisory” means Deloitte & Touche LLP, which provides audit and enterprise risk services; Deloitte Financial Advisory Services LLP, which provides forensic, dispute, and other consulting services; and its affiliate, Deloitte Transactions and Business Analytics LLP, which provides a wide range of advisory and analytics services. Deloitte Transactions and Business Analytics LLP is not a certified public accounting firm. These entities are separate subsidiaries of Deloitte LLP. Please see www.deloitte.com/us/about for a detailed description of the legal structure of Deloitte LLP and its subsidiaries. Certain services may not be available to attest clients under the rules and regulations of public accounting.
Disclaimer
Copyright © 2016 Deloitte Development LLC. All rights reserved.