porcelain fracture
TRANSCRIPT

DR. BAHJAT ABU HAMDANCONSULTANT PROSTHODONTISTBDS,CES,DSODAMASCUS UNIV. PARIS V,VI,VII UNIVS.
Porcelain fracture, reasonsand management.

A. Introduction
In spite of the sophisticated structure of the hard tooth tissues, enamel and dentin are prone to extended damage in the oral cavity. However it is a real challenge to find a man made materials that compete with these hard tissues.
In addition to the mechanical properties, a dental material should be biocompatible, aesthetic, corrosion resistant, easy to process and reasonable inexpensive.
2

A. Introduction.
Ceramics are widely accepted and used in dentistry with a high degree of general success.
However, fracture of these restorations does occur and usually frustrates the dentist and the patient.
In case of PFM, incidence of porcelain fracture is increased with the long term survival due to cyclic fatigue.
3

A. Introduction.
Incidence of porcelain fracture was the second most common cause for FPD replacement.
Porcelain fracture is considered the most common cause failure with PFM Crown.
(Walton et al)
Clinical study revealed that prevalence of ceramic fractures is 5-10% over 10 years of use.
4

A. Introduction.
In all ceramic restorations, veneering porcelain fracture remains one of the primary complicationaffecting longevity.
Clinical evaluation of 323 porcelain laminate veneers, over a period of 3-11 years, reveals failure due to porcelain fracture was 4% and 97% of the cases was satisfactory.
(Maria G-Ruiz et al) Chipping rates are 3 to 50% for FPD with zirconia framework after 3 years and 2.9% with metal framework.
5

B. Porcelain restoration
Types of porcelain restorations ;
• Simple Feldspathic Veneers
• Porcelain Jacket Crowns and Bridges ( PFZ) • Metal-Ceramic Crowns and Bridges
• Inlays and Onlays
• Implant Superstructures.
6

C. DENTAL Porcelain composition
7

C. Dental Porcelain….
8

C. Dental porcelain…
Indications for feldspathic porcelains • Highly esthetic veneers or anterior crowns in cases where color masking is not an issue
Indications for leucite-reinforced ceramics • Esthetic veneers and anterior crowns • As a layering porcelain on leucite-reinforced, lithium disilicate, alumina, or zirconia cores
Indications for lithium disilicate ceramics; Veneers Premolars and molars - inlays, onlays and crowns • Three-unit bridges – anterior and premolar region
Indications for zirconia-based ceramics • Anterior and posterior crowns • Bruxers – full-contour crowns • Anterior and posterior bridges (maximum 14-unit bridges, span depends on product and number of abutments) • Endodontically treated teeth • Implant abutments • Inlay bridges • Maryland bridges • Block-out of darkened tooth structure or cores.
9

C. Dental porcelain…
A summary of the strength of all-ceramic materials is shown in below:
Silica-based Ceramics Flexural Strength Feldspathic porcelain 65-120 MPa
Leucite-reinforced ceramic 120-140 MPaLithium disilicate ceramic 300-400 Mpa
Non-silica-based
Ceramics Alumina 650 Mpa
Zirconia 800-1500 MPa
10

D. Contributing factors..technical
1. surface treatment and design of the metal coping; the oxide layer is necessary forbonding the metal to the porcelain. Absenceof the oxide layer or thick layer have been shown to increase the risk of bonding and porcelain fracture at this level. (Graig et al).
The design of the metal framework should ensure strength, avoid sharp angles and has no flexibility, and ensure uniform thickness of porcelain.
11

12

D. Contributing factors..technical
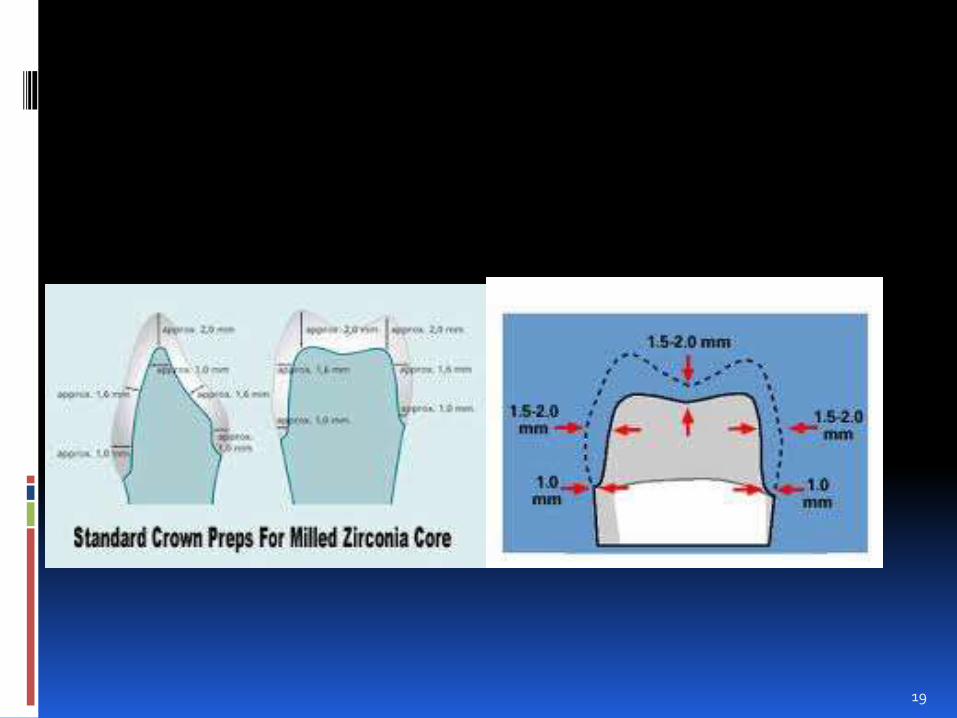
With zirconia, form and thickness, copings should resemble dentinal tooth substructures with relatively even and uniform thickness of enamel over dentin.
Zirconia is a (milled) material and could not exist without CAD/CAM, with the best zirconia using “virtual design”. Copings of standard thickness (that is, 0.5 millimeter) do not account for individual anatomical crown.
Anatomically designed copings are better able to reduce chipping.
13

14

D. Contributing factors..Technical.
2. Compatibility between coefficient of thermal expansion; difference of coefficient about 0.5x1/1000000 between the metal and the porcelain is desirable. Such relation put the porcelain under compression after firing.
For PFM veneering leucite is added to the feldespath to adjust the thermal expansion compatibility with the metal. Fast cooling causes cracks, at any step of sintering, and later on breaks.
15

D. Contributing factors..technical
In PFZ, mismatch of CTE between the core and veneer has resulted in an increase in failure loads for Zr-ceramic systems.
(Denry I et al) Another issue concerning the incidence of chipping in PFZ is the low thermal conductivity of the zirconia.
(Baldassarri M. et al)
16
D. Contributing factors..technical
3. Ceramic build up and firing techniques; porcelain cracks can be caused by air entrapment and porosity due to lack of densification. This lead to cracks coupled with low fracture toughness.
Rate of cooling affect the stress concentration at the metal ceramic interface.
Repeated firings or excessive temperatures are regarded as causes of super facial imperfections.
(Baretto, M.T.)
17

D. Contributing factors..technical
4. Thickness of porcelain; Increased porcelain thickness leads to a fragile restoration, this is caused by the increase of stress concentrationand weakness of the porcelain under tension.
A fairly uniform thickness of porcelain (1.5-2mm)minimize the formation of microcracks.
The incidence of cracks is expected to increase with greater porcelain veneer thicknesses, especially in combination with fast cooling rates.
(Guazzato M et al).
18
19

D. Contributing factors..technical
5. Elastic modulus of the used alloy; modulus of elasticity means resistance to deformation. Lack of rigidity and distortion of the metal framework is a frequent reason for porcelain fracture.
EM of the framework should be higher than that of the porcelain.
Porcelain is at fracture risk when the frameworkis perforated, if a trace of opaque is noticed inside the crown, it means simply that the framework is perforated.
20

Elasticity modulus
21

D. Contributing factors..technical
6. Porcelain-metal contact lines; it is important that the occlusal contact in centric occlusion avoid the metal-porcelain junction, so that the dentist and the technician should discuss whether the occlusion will on the metal or on the porcelain, ( it is up to the clinical situation and tooth prep). Porcelain metal junction should have 90 degree.
22
D. Contributing factors..technical
7. Substructure material used for fabrication of crowns or FPD can be ;
Metal alloy framework veneered by porcelain (PFM), which has been used for over 40 years.
Zirconia substructure material which is regarded as offering high mechanical qualities over the ceramic materials. (used over the last 15 years)
23

D. Contributing factors..technical
Veneering ceramics designed to be used with modern zirconia framework restorations have been reported to fracture occasionally in vivo. This veneer is leucite free, its fracture toughness is 0.73 MPa , which is less than that for the porcelain fused to metal (PFM) veneering ceramic: 1.10MPa) (Janet B. Quinn et al)
24

D. Contributing factors..technical
8. Cutting process induce flaws of different size in the tooth structures and dental materials.
A sandblasted glass lose 67% of its strength.
Use burs with fine grains (not more than 50 mM)
In the oral environment, the influence of water and changing temperature, called stress corrosion, can promote crack propagation and decrease the fracture strength of an all-ceramic restoration (Kelly 1995)
25

D. Contributing factors..Restorative process
Factors to Consider in the Restorative Process. The following principles, described by Dawson, based on the integration of the restoration in the context of the gnathostomatic system decreaseand limit the post-cementation complications. Of course porcelain fracture is one of these complication.
1. Properly designed centric stops; force distribution is a timing issue, equal intensity of contact have 2 purposes.
26

D. Contributing factors..Restorative process
The first is to distribute equally throughout the mouth whatever force the patient can generate. The second purpose of the centric stop is to create both vertical and horizontal stability of the teeth. To realize these purposes these contacts should be in harmony with the condyles in their CR position which is necessary in the distribution of occlusal forces between the teeth and the TMJs.
27

Restorative process
28

D. Contributing factors..restorative process
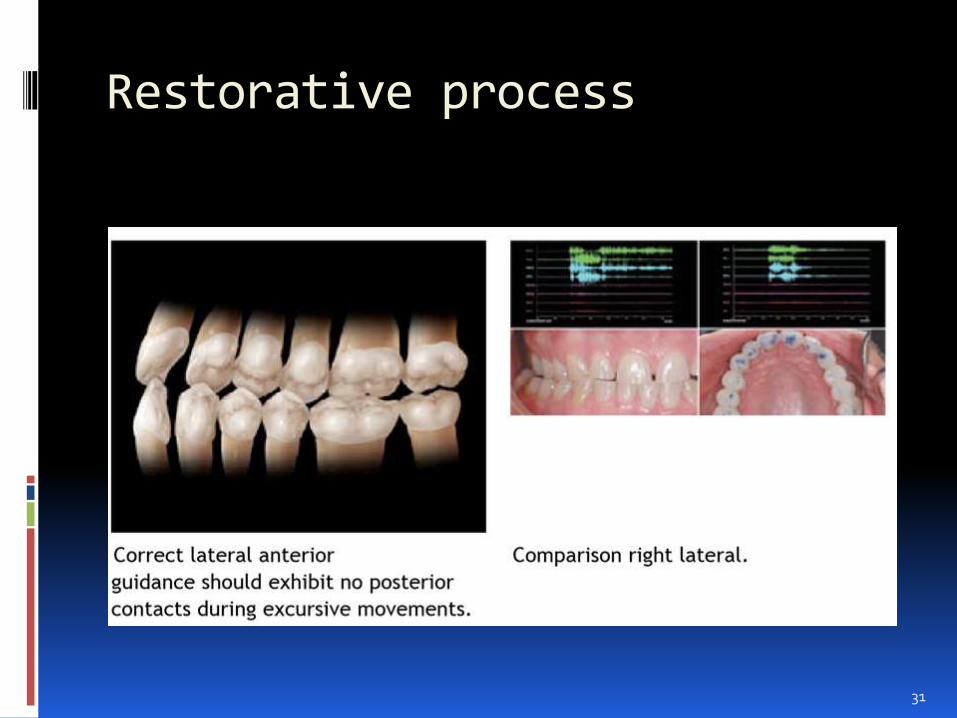
2. Correct lateral anterior guidance; When the mandible moves laterally, the goal is to have immediate disclusion of the posterior teeth on the working and balancing side. The classic work by Williamson and Lunquistillustrated the neuromuscular advantage obtained when posterior teeth are not allowed to contact in excursive movement. Anterior guidance should be worked on provisional restoration.
29

D. Contributing factors..restorative process
Acceptable anterior guidance should be coherent with the condylar guidance, so that it will not cause tooth migration, mobility or tooth fracture.
30
Restorative process
31
D. Contributing factors..restorative process
3. Correct protrusive anterior guidance; With any protrusive movement of the mandible, the goal is immediate posterior disclusion.
Just like lateral movements of the mandible, posterior tooth contact in a protrusive movement increases the force on the anterior teeth because of increased muscle activity.
32
Steep guidance patterns restrict the movement of the mandible that can lead to instability; fracture being one of the possibilities.

D. Contributing factors..restorative procee
4. Correct crossover disclusion; In lateral excursions, as the patient goes beyond the cuspid, proper occlusal design dictates that there is a smooth transition to the incisaledge of the maxillary centrals. This transition requires the proper alignment and position of the mandibular as well as the maxillary incisors. When this position is overlooked excessive loads can be placed on the distal of the lateral incisors, leading to fracture.
33

D. Contributing factors..restorative factors
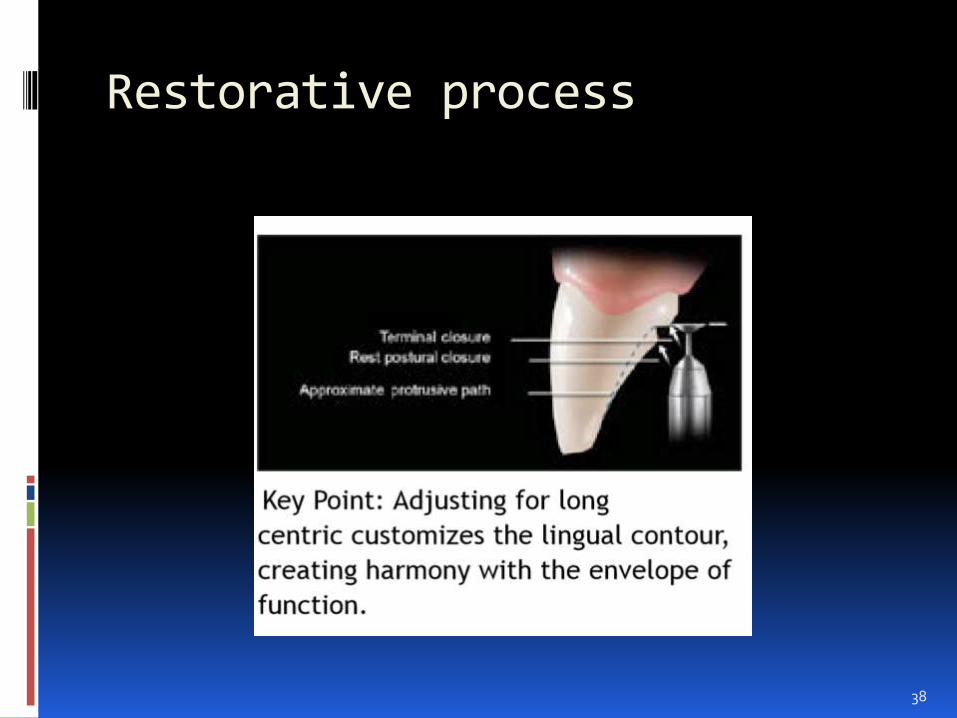
5. Lingual Contours in Harmony with the Envelope of Function; Protecting the posterior teeth from contact in excursive movements is one of the most important functions of the anterior teeth. Working with the condylarguidance, the lingual contour must be steepenough for immediate separation of the posterior morphology. Signs of instability such as wear, fremitus, or migration of the anterior teeth are all indications that a constriction occur.
34

Restorative process
35

Restorative process
36

Restorative process
37
Restorative process
38

D. Contributing factors..restorative procee
6. Parafunction; Bruxism, nail biting, sleep disturbances, chewing on pencils/pens, or any aberrant movement of the mandible that brings the teeth together in an abnormal pattern and creates signs of instability in any part of the system need to be identified during treatment planning. If it is identified that the parafunctional issues happen while the patient is asleep, a night guard should be fabricated to cover the teeth during this time.
39

Restorative process
40

Restorative process
Flexible appliance for protecting the porcelain restorations.
41

D. Contributing factors..restorative process
7. Properly Designed Tooth Preparation; One of the most common causes of fracture is overreduction of the incisal edge. Porcelain that has > 2 mm of unsupported material is at risk for fracture. Result predictability is ensured by evaluation of tooth length and the esthetic on the study models.
42

D. Contributing factors..Restorative process
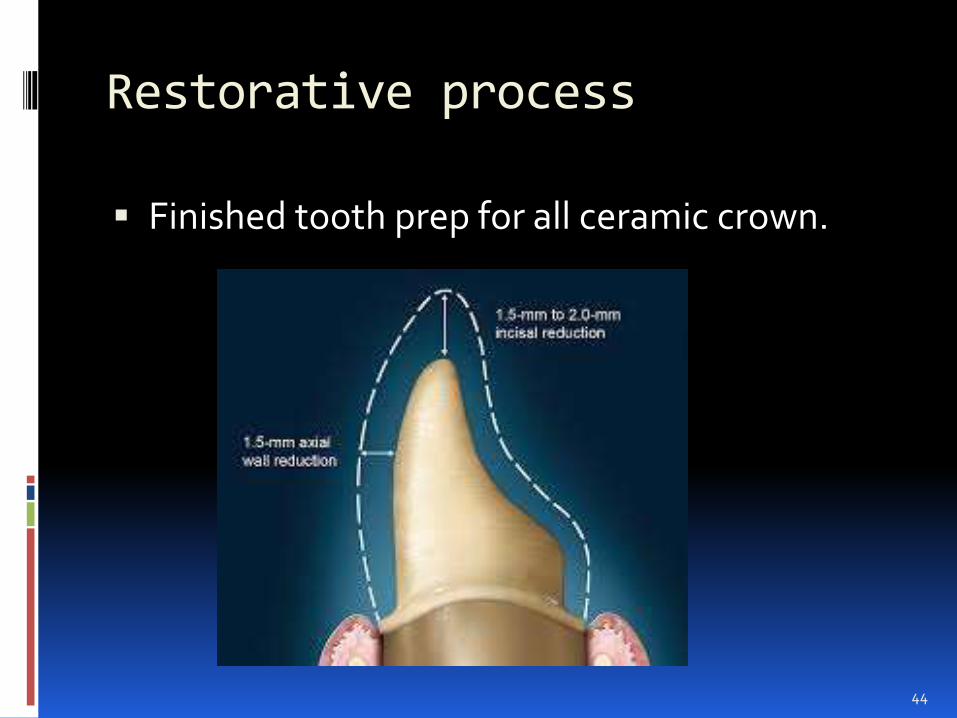
8. Properly Finished Tooth Preparations; All-ceramic dentistry requires a high degree of precision in both reduction and finishing. Sharp line angles and rough preparations are some of the major contributing factors when fractured porcelain occurs. Proper finishing will lead to cleaner impressions as well as better fitting, fracture-resistant restorations.
43
Restorative process
Finished tooth prep for all ceramic crown.
44

E. Porcelain fracture management
Fracture of veneering porcelain is a complication that can occur in every dental ceramic system. Based on the placement of the fracture, two types are considered;
a. cohesive which located in the porcelain.
b. adhesive which affects the bonding between the veneering and the framework.
Single crown survival is similar for both PFMand all ceramic, but in FPD all ceramic shows higher failure. (Heintze SD, Rousson V)
45

E. Porcelain fracture management
Fracture modes of all-ceramic restorations have changed substantially with the availability of zirconium oxide compared with glass-ceramic. (mainly for the post. T.)
Fractures of the veneering porcelain appear to be a zirconia-specific problem.
(Al-Amleh et al)
Chipping rates are 3 to 50% for FPD with zirconia framework after 3 years and 2.9% with metal framework.
46

E. Porcelain fracture management
Management of this complication is based on the evaluation of each case, based on that, treatment can be;
a. By adjustment and polishing.
b. Porcelain repair.
c. Replacement of the restoration.
The frequency of chipping that can be treated by a, b, is considerably higher for both PFM or PFZ.
47

E. Porcelain fracture management
What options are available to repair a chipped all-ceramic or PFM restoration?
1. Replace.
2. Repair the ceramic restoration intraorally,which is an interim, but reasonable, solution.
a. Polish the fractured surface. is possible only for small chippings in the posterior region and only when the metal or ceramic coping is not exposed.
48

E. Porcelain fracturemanagement
b. Replace the missing piece of porcelain with composite-based resin;
c. Reapply the broken piece of porcelain with resin cement;
d. Prepare the restoration for a new veneer and adhesively bond the ceramic veneer onto the existing restoration. This option is an attractive solution.
49
E. Porcelain fracturemanagement
To achieve functional success, the clinician has to establish reliable bonding of the veneering porcelain to the core material.
Surface conditioning is essential to the success of intra- oral repair. The challenge is to create a strong, mechanochemical bond between the hydro- phobic resin-based composite or resin cement and the fractured surface of the restoration, which often is composed of two different materials. this bond also involves chemical interactions.
50

E. Porcelain fracteuremanagement
Surface treatment depends on the exposed substructure material which can be;
Metal alloys, oxide-ceramic materials; zirconia, alumina and glass- infiltrated zirconia which are used for copings or frameworks in all-ceramic restorations.
Disilicate-ceramic materials: feldspathicceramics, which are used for anterior veneers or veneering porcelain in PFM or all-ceramic restorations.
51

E. Porcelain fracture management
Glass-ceramics, which are indicated for inlays, onlays, veneers and monolithic crowns.
Micromechanical retention of the metal or ceramic bond to resin is achieved by means of ;
1. Air abrasion with the intraoral sandblaster.
2. Or by etching with hydrofluoric acid.
porcelain etching is done by the application of 2.5 to 10 percent hydrofluoric acid for 60-90 seconds. It is indicated for use only with silicate-ceramic
52

E. Porcelain fracturemanagement
Etching breaks silicate bonds
Unsaturated oxygen bonds are also generated, which serve as bonding partners for the silane.
However, intra- oral use of hydrofluoric acid is controversial because of its hazardous properties. If hydrofluoric acid is spilled on the soft tissue, it may take hours before symptoms appear. Therefore, clinicians should use with precaution and rubber dam is mandatory also tooth tissue should well protected.
53


PORCELAIN FRACTUREMANAGEMENT
In the case of chaireside air-abrasion procedure with 50 µm Al2O3, both V and INC ceramic surfaces exhibited similar rough surface patterns that presented incorporation of sand particles on their surfaces
55

E. PORCELAIN FRACTUREMANAGEMENT
Air abrasion. Minimal safety risks by using an intraoral
sandblaster. Al oxide particles of 50 mM at 2-3 bars air
pressure will clean, roughen, enlarge the surface and activate the surface leading to a better wettability and chemical accessibility.
Lowering the pressure to.05 bar will reduce the detrimental effects on oxide ceramic materials. (high pressure cause flaws in the ceramic)
It is difficult to limit the action on the target area.
56

E. PORCELAIN FRACTUREMANAGEMENT
The chemical bond between substructure surface (metal,Al oxide,Zr oxide, silicate) and the hydrophobic resin is created by bifunctional molecules such as silanes or phosphate monomers. Silanes bond to silicate materials. On the other end of the silane molecule, an additional polymerization reaction of methacrylate groups generates a bond to resin. (Söderholm KJ et al)
57

E. Porcelain fracture management
Rrubber dam is indispensable, as contamination of the silanized surface with water inactivates the silane.
Metal- and oxide-ceramic materials, which do not contain silanol groups, also can be bonded to silanes if they are silicatized in advance.
This procedure usually is referred to as tribochemical coating.
Intraoral surface treatments become possible with a chair side system.
58

E. Porcelain fracturemanagement
(CoJet silicate-ceramic surface treatment system, 3M ESPE). The system consists of fine-grained 30-µm Al oxide particles that are doped by silica. This modification simultaneously will allow roughening and the incorporation of silica into the alloy, Zr oxide, or Al oxide. The silica enriched surface then will react with the silane.
4-META containing resin have been shown to bond on non-noble alloy via the oxide (Panavia) and are quite useful for porcelain repair.
59

60

Cohesive fracture
61

cohesive fracture
62
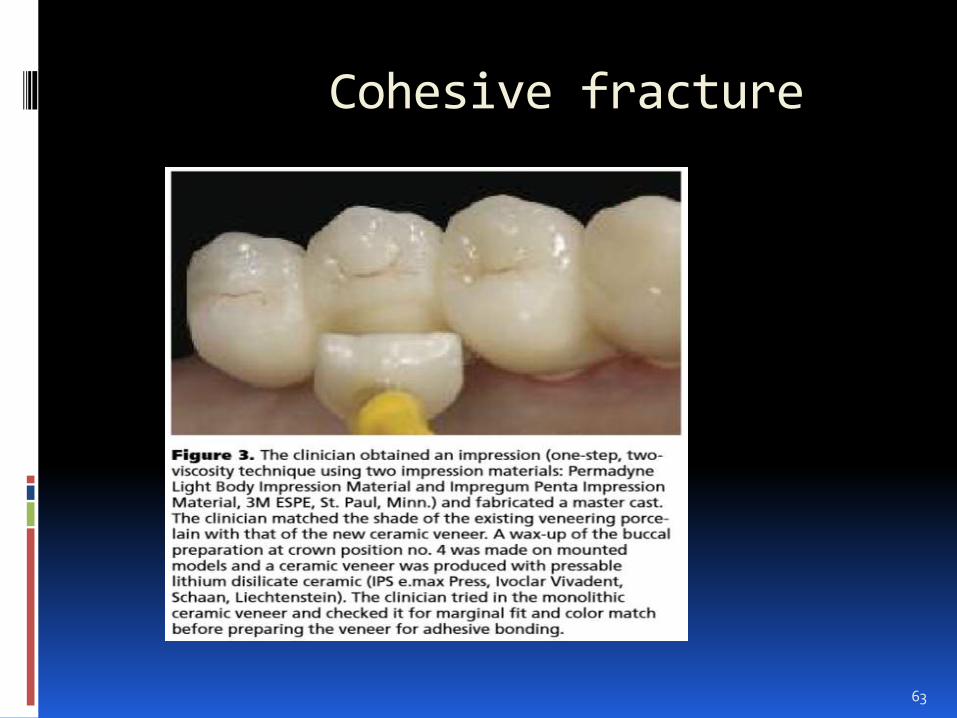
Cohesive fracture
63
E. Porcelain fracturemanagement
Bifunctional phosphate monomers.
(10- methacryloyloxydecyl dihydrogenphosphate or 4-methacryloyloxyethyl trimellitate anhydride) bond to oxides of the metal or oxide-ceramic surface on one side and to the resin on the other side. ( Uo M, Sjögren G. et al)
Bifunctional phosphate monomers can be part of the resin cement.
64

65
E. Porcelain fracturemanagement
In this case, they are called modified phosphate-monomer– containing resin cements.
Modified resin cements should be applied only on base alloys because they do not bond sufficiently to noble alloys.
(Antoniadou M. et al)
Products also are available that contain ceramic and metal primer, (silane and phosphate monomer).
66

E. Porcelain fracture management
The use of these combined primers is appropriate for the intraoral repair of a restoration if different materials are exposed on the fractured surface. (silicate and oxides)
67

68

Conclusion.
In spite of all the technical standards and the clinical precautions, porcelain cracks and fracture are still considered as a daily frustrating problem that may be confronted. Management of this failure needs meticulous diagnosis.
Treatment may need complete replacement of the restoration as last option, however certain cases can be repaired. The nature of fracture whether it is cohesive or adhesive is important to decide the nature of the material to be repaired, is it silica, Al oxide, Zr oxide or non precious alloy?
69

To obtain a good bonding on these different material, a comprehensive knowledge about the different type of bonding systems and their indications is basic.
These bonding systems include the fluoric acid, the air abrasion system, the silane,theCojet system, the phosphate monomer primer, combined primers, modified phosphate-monomer– containing resin cements.
70

Thanks
71