pocket guide - canadian cardiovascular society · pocket guide leadership. knowledge. ......
TRANSCRIPT

Pocket Guide
Leadership. Knowledge. Community.
Antiplatelet Therapy in the Outpatient Setting2011 Recommendations
For more information, please visit theCanadian Cardiovascular Society (CCS)
Antiplatelet Guidelines atwww.ccsguidelineprograms.ca.

2
Table of Contents
Introduction and Rationale………….....................................…..3Antiplatelet Therapy (APT)…….............................……….........4APT for Secondary Prevention in First Year Post-ACS…..........5Post-discharge Management of STEMI….….............................6Post-discharge Management of NSTEACS…...........................7APT for Secondary Prevention in First Year Post-PCI…............8Post-Discharge Management of Patients Undergoing PCI.........9Management of Stable CAD…................................................10Key Considerations: APT Post-ACS/PCI…..........................…11APT for Secondary Prevention Post-CABG….........................12Management Post-CABG…....................................................13APT for Secondary Prevention of Cerebrovascular Disease....14Management of TIA and Ischemic Stroke….............................15Key Considerations: APT for Cerebrovascular Disease….......16APT for Vascular Prevention in Patients with PAD...............…17Management of Peripheral Arterial Disease….........................18Management Post-Peripheral Artery Surgery….......................19APT Primary Prevention of Vascular Events…........................20Primary Prevention…...............................................................21Key Considerations: APT for Primary Prevention.................…22APT in Patients with Diabetes…..............................................23
Management of Patients with Diabetes................................…24APT in Patients with Heart Failure........................................…25Management of Heart Failure…...............................................26Management of Chronic Kidney Disease….............................27Management in Pregnancy and Lactation…............................28Perioperative Management of: Patients on APT…..............................................................29 Patients taking ASA…........................................................30 Patients taking ASA and Clopidogrel.............................….31Key Considerations: Perioperative APT Management….....................................32Management of Minor Bleeding…........................................…33Key Considerations: Management of APT in Association with Minor Bleeding….34Combination Therapy with Warfarin and ASA......................…35Management of Patients Requiring Warfarin…........................36Interaction Between Clopidogrel and PPIs…...........................37Use of Proton-Pump Inhibitors….............................................38Interaction Between ASA and NSAIDS…................................39Use of NSAIDs in Patients on ASA…......................................40APT: Drug-Drug Interactions….................................................41

3
Introduction and Rationale
2011 Canadian Antiplatelet Therapy Guidelines Development Methodology
• Identify relevant clinical guidelines for antiplatelet therapy.
• Assess quality using the AGREE (Appraisal of Guidelines for Research & Evaluation) instrument.
• Develop recommendations via consideration of:• Existing guidelines and their associated AGREE score.• Literature published subsequent to existing guidelines. • Expert opinion.
• Create graded recommendations using a system set forth by the Canadian Cardiovascular Society (CCS).
• Conduct an external review by Canadian experts in their respectivefieldswhowerenotinvolvedinthewritingprocess.
Antiplatelet therapy is underused in clinical practice.
Canadian physicians require guidance that is:• Clear.• Easily accessible.• Evidence-based.
4
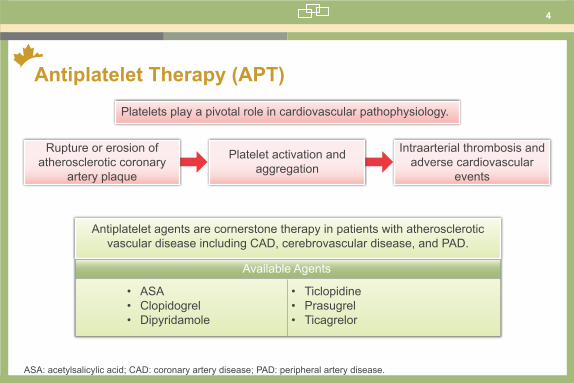
Antiplatelet Therapy (APT)Platelets play a pivotal role in cardiovascular pathophysiology.
Antiplatelet agents are cornerstone therapy in patients with atherosclerotic vascular disease including CAD, cerebrovascular disease, and PAD.
• ASA• Clopidogrel• Dipyridamole
• Ticlopidine• Prasugrel • Ticagrelor
Rupture or erosion of atherosclerotic coronary
artery plaque
Platelet activation and aggregation
Intraarterial thrombosis and adverse cardiovascular
events
Available Agents
ASA: acetylsalicylic acid; CAD: coronary artery disease; PAD: peripheral artery disease.
5
APT for Secondary Prevention in First Year Post-ACS
Coronary Artery Disease
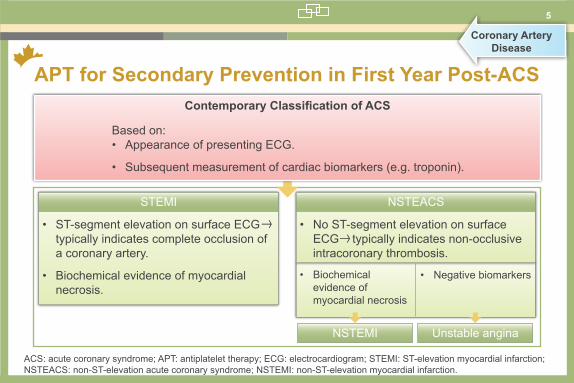
Contemporary Classification of ACS
Based on:• Appearance of presenting ECG.
• Subsequent measurement of cardiac biomarkers (e.g. troponin).
• ST-segment elevation on surface ECG typically indicates complete occlusion of a coronary artery.
• Biochemical evidence of myocardial necrosis.
• No ST-segment elevation on surface ECG typically indicates non-occlusive intracoronary thrombosis.
• Biochemical evidence of myocardial necrosis
• Negative biomarkers
STEMI NSTEACS
NSTEMI Unstable angina
ACS: acute coronary syndrome; APT: antiplatelet therapy; ECG: electrocardiogram; STEMI: ST-elevation myocardial infarction; NSTEACS: non-ST-elevation acute coronary syndrome; NSTEMI: non-ST-elevation myocardial infarction.

6
Post-discharge Management of STEMI
In general, the ADP P2Y12 receptor antagonist added to ASA in the acute setting should be maintained for the duration of the therapy (Class I, Level C). ADP: adenosine diphosphate; ASA: acetylsalicylic acid; CABG: coronary artery bypass graft; STEMI: ST-elevation myocardial infarction.
Percutaneousintervention
Increased risk of stentthrombosis
Medically managed
Prasugrel 10 mg daily may beconsidered in the absence of:
● increased bleeding risk● likely to undergo CABG within 7 days● history of stroke or transient ischemic attack (TIA)● age >75 years● weight <60 kg(Class IIa, Level B)
ASA 75-162 mg OD
Indefinite Therapy
(Class I, Level A)
If ASAintolerant
Clopidogrel 75 mgOD
Indefinite Therapy(Class IIa, Level B)
STEMI
Clopidogrel 75 mg OD or ticagrelor 90 mgBID in addition to ASA 75-162 mg daily for12 months (Class I, Level B). Continuation of combined therapy beyond 12 months may be
considered in patients with a high risk ofthrombosis and a low risk of bleeding
(Class IIb, Level C).
Clopidogrel 75 mg OD or ticagrelor 90 mgBID in addition to ASA 75-162 mg daily forat least 14 days (Class I, Level B) and up
to 12 months in the absence of an excessive risk of bleeding
(Class IIb, Level C).
Postdischarge Management of ST Segment Elevation Myocardial Infarction
7
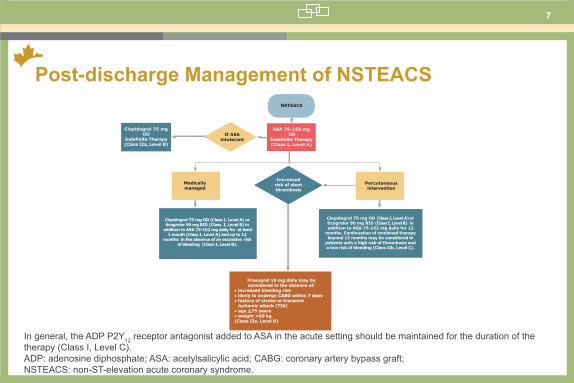
Post-discharge Management of NSTEACS
In general, the ADP P2Y12 receptor antagonist added to ASA in the acute setting should be maintained for the duration of the therapy (Class I, Level C). ADP: adenosine diphosphate; ASA: acetylsalicylic acid; CABG: coronary artery bypass graft; NSTEACS: non-ST-elevation acute coronary syndrome.
If ASAintolerant
Clopidogrel 75 mgOD
Indefinite Therapy(Class IIa, Level B)
ASA 75-162 mg OD
Indefinite Therapy(Class I, Level A)
NSTEACS
Percutaneousintervention
Increased risk of stentthrombosis
Medically managed
Prasugrel 10 mg daily may beconsidered in the absence of:
● increased bleeding risk● likely to undergo CABG within 7 days● history of stroke or transient ischemic attack (TIA)● age >75 years● weight <60 kg(Class IIa, Level B)
Clopidogrel 75 mg OD (Class I, Level A) or ticagrelor 90 mg BID (Class I, Level B) in addition to ASA 75-162 mg daily for 12
months. Continuation of combined therapy beyond 12 months may be considered in
patients with a high risk of thrombosis and a low risk of bleeding (Class IIb, Level C).
Clopidogrel 75 mg OD (Class I, Level A) or ticagrelor 90 mg BID (Class I, Level B) in
addition to ASA 75-162 mg daily for at least 1 month (Class I, Level A) and up to 12
months in the absence of an excessive risk of bleeding (Class I, Level B).
Postdischarge Management of Non-ST Segment Elevation Acute Coronary Syndrome
8
APT for Secondary Prevention in First Year Post-PCI
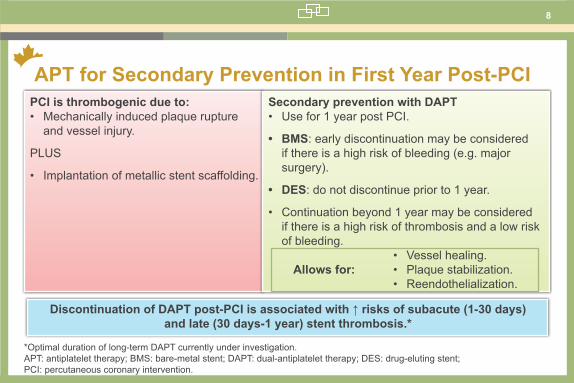
*Optimal duration of long-term DAPT currently under investigation. APT: antiplatelet therapy; BMS: bare-metal stent; DAPT: dual-antiplatelet therapy; DES: drug-eluting stent; PCI: percutaneous coronary intervention.
PCI is thrombogenic due to:• Mechanically induced plaque rupture
and vessel injury.
PLUS
• Implantation of metallic stent scaffolding.
Discontinuation of DAPT post-PCI is associated with ↑ risks of subacute (1-30 days) and late (30 days-1 year) stent thrombosis.*
Secondary prevention with DAPT • Use for 1 year post PCI.
• BMS: early discontinuation may be considered if there is a high risk of bleeding (e.g. major surgery).
• DES: do not discontinue prior to 1 year.
• Continuation beyond 1 year may be considered if there is a high risk of thrombosis and a low risk of bleeding.
Allows for:• Vessel healing.• Plaque stabilization.• Reendothelialization.
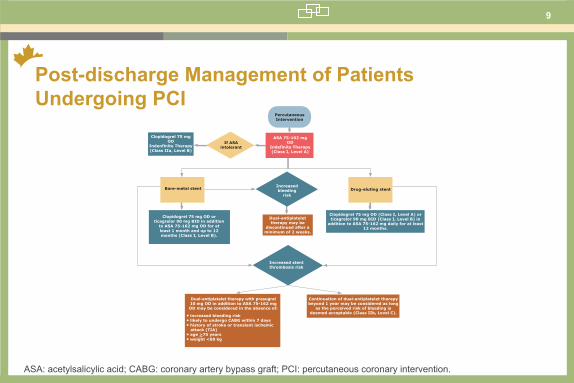
9
PercutaneousIntervention
ASA 75-162 mgOD
Indefinite Therapy(Class I, Level A)
If ASAintolerant
Clopidogrel 75 mg OD
Indenfinite Therapy(Class IIa, Level B)
Clopidogrel 75 mg OD orticagrelor 90 mg BID in addition
to ASA 75-162 mg OD for atleast 1 month and up to 12 months (Class I, Level B).
Bare-metal stent
Dual-antiplatelettherapy may be
discontinued after aminimum of 2 weeks.
Increased stentthrombosis risk
Dual-antiplatelet therapy with prasugrel10 mg OD in addition to ASA 75-162 mg OD may be considered in the absence of:
• increased bleeding risk• likely to undergo CABG within 7 days• history of stroke or transient ischemic attack (TIA)• age >75 years• weight <60 kg
Clopidogrel 75 mg OD (Class I, Level A) orticagrelor 90 mg BID (Class I, Level B) in
addition to ASA 75-162 mg daily for at least 12 months.
Continuation of dual-antiplatelet therapybeyond 1 year may be considered as long
as the perceived risk of bleeding isdeemed acceptable (Class IIb, Level C).
Drug-eluting stentIncreasedbleeding
risk
Postdischarge Management of Patients Undergoing Percutaneous Coronary Intervention
Post-discharge Management of Patients Undergoing PCI
ASA: acetylsalicylic acid; CABG: coronary artery bypass graft; PCI: percutaneous coronary intervention.

10
Management of Stable CAD
ACS: acute coronary syndrome; ASA: acetylsalicylic acid; CAD: coronary artery disease.
ASA 75-162 mgOD
Indefinite Therapy(Class I, Level A)
If ASA intolerant
ACS >1 yearpost event
Clopidogrel 75 mgOD
Indefinite Therapy(Class IIa, Level B)
If high risk ofthrombosis and
low risk ofbleeding
Dual-antiplatelet therapywith ASA 75-162 mg OD
and clopidogrel 75 mg ODmay be considered (Class IIb, Level C).
Management of Stable Coronary Artery Disease
11
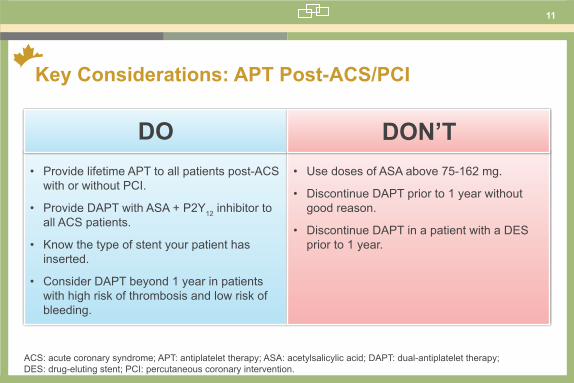
Key Considerations: APT Post-ACS/PCI
ACS: acute coronary syndrome; APT: antiplatelet therapy; ASA: acetylsalicylic acid; DAPT: dual-antiplatelet therapy; DES: drug-eluting stent; PCI: percutaneous coronary intervention.
• Provide lifetime APT to all patients post-ACS with or without PCI.
• Provide DAPT with ASA + P2Y12 inhibitor to all ACS patients.
• Know the type of stent your patient has inserted.
• Consider DAPT beyond 1 year in patients with high risk of thrombosis and low risk of bleeding.
DO• Use doses of ASA above 75-162 mg.
• Discontinue DAPT prior to 1 year without good reason.
• Discontinue DAPT in a patient with a DES prior to 1 year.
DON’T

12
APT for Secondary Prevention Post-CABG
APT: antiplatelet therapy; ASA: acetylsalicylic acid; CABG: coronary artery bypass graft.
APT is the gold standard in preventing saphenous vein graft closure after CABG.
• Givenindefinitelymayprevent adverse clinical events post-CABG.
• No evidence of improved arterial graft patency.
Warfarin appears to be as effective as
antiplatelet therapy in preventing saphenous
graft closure post-CABG, but it is associated with a higher risk of bleeding
complications.
• Recommended for patients allergic or intolerant to ASA.
• Safer than other available therapies (e.g. ticlopidine).
• No randomized trial has specificallystudiedtheefficacyofclopidogrelintheprevention of post-CABG vein graft closure.
ASA Clopidogrel

13
Management Post CABG
TheoutpatientmanagementofpatientsafterCABGisoutlinedinthisfigureandmayincludedual-antiplatelettherapywhenarecently stented vessel is not adequately bypassed. ASA: acetylsalicylic acid; ATP: antiplatelet therapy; CABG: coronary artery bypass graft; PCI: percutaneous coronary intervention.
Coronary ArteryBypass Graft
ASA 75-162 mgOD
Indefinite Therapy(Class I, Level A)
In patients undergoing CABG afterPCI, dual-antiplatelet therapy with
ASA 75-162 mg daily andclopidogrel 75 mg daily may be
maintained for 9-12 months unlessthe stented vessel is adequatelybypassed (Class IIb, Level C).
If ASAintolerant
Clopidogrel 75 mgOD
Indefinite Therapy(Class IIa, Level B)
Management Post Coronary Artery Bypass Graft
14
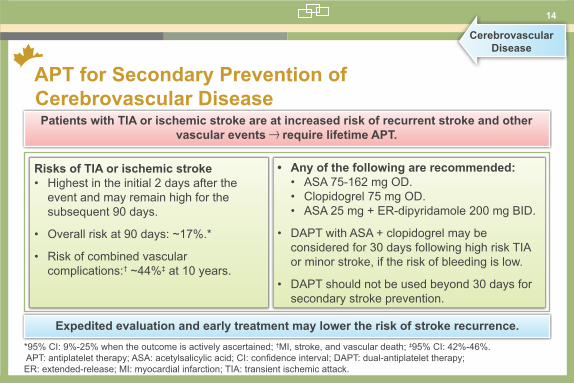
APT for Secondary Prevention of Cerebrovascular Disease
*95% CI: 9%-25% when the outcome is actively ascertained; †MI, stroke, and vascular death; ‡95% CI: 42%-46%. APT:antiplatelettherapy;ASA:acetylsalicylicacid;CI:confidenceinterval;DAPT:dual-antiplatelettherapy; ER: extended-release; MI: myocardial infarction; TIA: transient ischemic attack.
CerebrovascularDisease
Patients with TIA or ischemic stroke are at increased risk of recurrent stroke and other vascular events require lifetime APT.
Risks of TIA or ischemic stroke• Highest in the initial 2 days after the
event and may remain high for the subsequent 90 days.
• Overall risk at 90 days: ~17%.*
• Risk of combined vascular complications:† ~44%‡ at 10 years.
• Any of the following are recommended: • ASA 75-162 mg OD.• Clopidogrel 75 mg OD.• ASA 25 mg + ER-dipyridamole 200 mg BID.
• DAPT with ASA + clopidogrel may be considered for 30 days following high risk TIA or minor stroke, if the risk of bleeding is low.
• DAPT should not be used beyond 30 days for secondary stroke prevention.
Expedited evaluation and early treatment may lower the risk of stroke recurrence.

15
Management of TIA and Ischemic Stroke
TheoutpatientmanagementofTIAorischemicstrokeofnoncardiacorigincanincludedual-antiplatelettherapyforthefirstmonth.ASA: acetylsalicylic acid; ER: extended-release; TIA: transient ischemic attack.
TIA or ischemicstroke of
noncardiac origin
ASA 75-162 mg once daily
(Class I, Level A)
Clopidogrel 75 mgonce daily
(Class I, Level A)
ER-dipyridamole 200 mg twice daily plus
ASA 25 mg twice daily
(Class I, Level A)
The combination of ASA 75-162 mg daily plus clopidogrel 75 mg daily
in the first month after TIA or minor ischemic stroke may be superior to ASA alone in
patients not at a high risk of bleeding (Class IIb, Level C).
The combination of ASA 75-162 mg daily plus clopidogrel 75 mg daily should not be used for secondary
stroke prevention beyond 1 month unless otherwise indicated and
the risk of bleeding is low (Class III, Level B).
Management of TIA and Ischemic Stroke
16
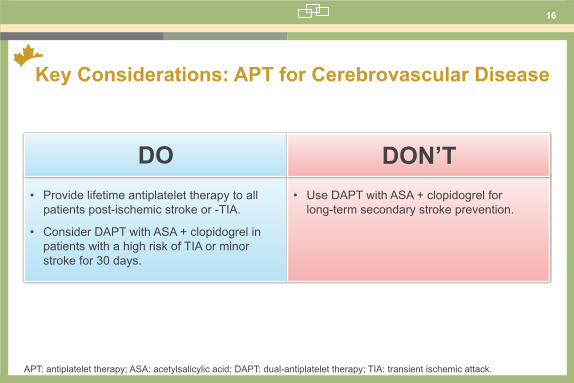
Key Considerations: APT for Cerebrovascular Disease
APT: antiplatelet therapy; ASA: acetylsalicylic acid; DAPT: dual-antiplatelet therapy; TIA: transient ischemic attack.
• Provide lifetime antiplatelet therapy to all patients post-ischemic stroke or -TIA.
• Consider DAPT with ASA + clopidogrel in patients with a high risk of TIA or minor stroke for 30 days.
DO• Use DAPT with ASA + clopidogrel for
long-term secondary stroke prevention.
DON’T

17
APT for Vascular Prevention in Patients with PAD
*ABI <0.9.ABI: ankle-brachial index; APT: antiplatelet therapy; PAD: peripheral arterial disease.
Peripheral ArterialDisease
• Bruit found along major vessels, peripheral pulsations reduced or absent.
OR
• Abnormally enlarged artery (possible aneurysm).
• Usually harbour traditional risk factors.
• Evidence shows patients with ABI <0.9 present a cardiovascular morbidity and mortality rate approx. halfway between that of a patient with a normal ABI and that of a patient with claudication.
Characteristics
Vascular Risk
• Claudication.
OR
• Rest pain.
OR
• Ischemic lesions.
• High risk of cardiovascular events and total mortality, even when taking into account usual risk factors.
Asymptomatic PAD* Symptomatic PAD*
18
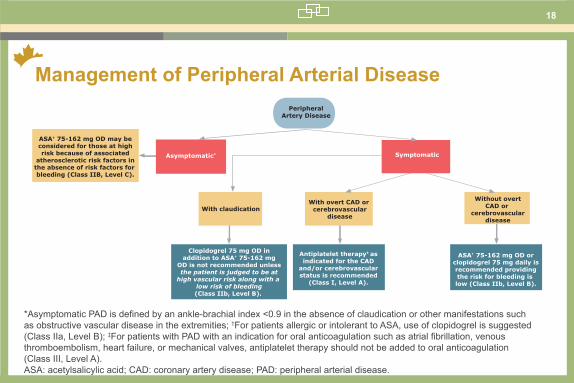
Management of Peripheral Arterial Disease
*AsymptomaticPADisdefinedbyanankle-brachialindex<0.9intheabsenceofclaudicationorothermanifestationssuchas obstructive vascular disease in the extremities; †For patients allergic or intolerant to ASA, use of clopidogrel is suggested (Class IIa, Level B); ‡ForpatientswithPADwithanindicationfororalanticoagulationsuchasatrialfibrillation,venousthromboembolism, heart failure, or mechanical valves, antiplatelet therapy should not be added to oral anticoagulation (Class III, Level A).ASA: acetylsalicylic acid; CAD: coronary artery disease; PAD: peripheral arterial disease.
PeripheralArtery Disease
ASA† 75-162 mg OD may beconsidered for those at highrisk because of associated
atherosclerotic risk factors inthe absence of risk factors for bleeding (Class IIB, Level C).
ASA† 75-162 mg OD orclopidogrel 75 mg daily isrecommended providingthe risk for bleeding is low (Class IIb, Level B).
Antiplatelet therapy‡ asindicated for the CAD
and/or cerebrovascularstatus is recommended
(Class I, Level A).
Clopidogrel 75 mg OD inaddition to ASA† 75-162 mg
OD is not recommended unlessthe patient is judged to be at
high vascular risk along with a low risk of bleeding(Class IIb, Level B).
Symptomatic
Without overtCAD or
cerebrovasculardisease
With overt CAD or cerebrovascular
diseaseWith claudication
Asymptomatic*
Management of Peripheral Arterial Disease

19
Management Post-peripheral Artery Surgery
*For patients allergic or intolerant to ASA, use of clopidogrel is suggested (Class IIa, Level B).The outpatient management of patients after peripheral arterial surgery or percutaneous revascularization or presenting an abdominal aortic aneurysm AAA. AAA: abdominal aortic aneurysm; ASA: acetylsalicylic acid; PAD: peripheral arterial disease.
Peripheral ArteryDisease with
Surgical Indication
In those with infrainguinalgrafts and a high risk of thrombosis or limb loss,
combination therapy with a vitamin K antagonist and ASA*
75-162 mg OD may be of benefit (Class IIB, Level C).
ASA* 75-162 mg OD shouldbe given to patients who undergo lower-extremity
balloon angioplasty with or without stenting for chronic
symptomatic PAD (Class IIa, Level C).
ASA* 75-162 mg OD maybe considered for all
patients with an AAA, particularly those with
clinical or subclinical PAD(Class IIb, Level C).
Management Post Peripheral Artery Surgery

20
APT Primary Prevention of Vascular Events
ASA: acetylsalicylic acid; APT: antiplatelet therapy; MI: myocardial infarction; TIA: transient ischemic attack.
Primary Prevention of Vascular Events
• Maybedefinedasantiplateletstrategies,administeredtoindividualsfreeofanyevidenceofmanifest atherosclerotic disease in any vascular bed, to prevent clinical vascular events or manifestations thereof.
• Atherosclerotic disease may include, but is not limited to:• Syndromes of angina pectoris.• MI.• Ischemic stroke.• TIA.• Intermittent claudication.• Critical limb ischemia.
Primary prevention
The benefits of ASA and APT for primary prevention have not been demonstrated.

21
Primary Prevention
Forthepurposeofthisguideline,primarypreventionisdefinedasantiplateletstrategies,administeredtoindividualsfreeofanyevidence of manifest atherosclerotic disease in any vascular bed, to prevent clinical vascular events or manifestations thereof. ASA: acetylsalicylic acid.
In special circumstances in men and women without evidence of
manifest vascular disease in whom vascular risk is considered high and bleeding risk low, ASA
75-162 mg daily may be considered (Class IIb, Level C).
PrimaryPrevention
ASA at any dose is not recommended for
routine use to prevent ischemic vascular
events (Class III, Level A).
Clopidogrel plus ASA at any dose is not
recommended to prevent ischemic vascular events
(Class III, Level B).
Primary Prevention
22
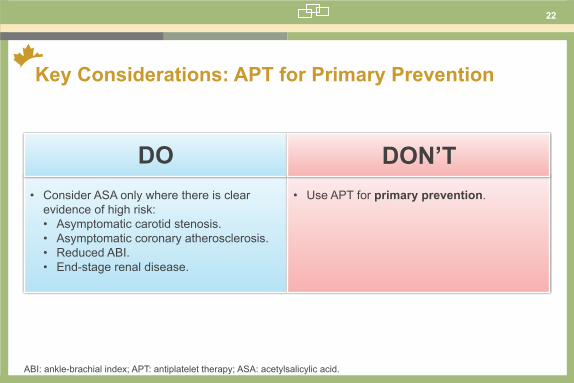
Key Considerations: APT for Primary Prevention
ABI: ankle-brachial index; APT: antiplatelet therapy; ASA: acetylsalicylic acid.
• Consider ASA only where there is clear evidence of high risk:• Asymptomatic carotid stenosis.• Asymptomatic coronary atherosclerosis.• Reduced ABI.• End-stage renal disease.
DO• Use APT for primary prevention.
DON’T

23
APT in Patients with Diabetes
Diabetes
Patients with diabetes have a variety of risk factors and alterations to platelet function that predispose them to platelet activation and thrombosis.
The absence of clear primary prevention benefits for antiplatelet therapy in patients with diabetes may indicate that patients with diabetes are a specific subgroup of patients in
whom mechanisms such as ASA resistance are manifest.
Platelet alterations may include:• Increased platelet turnover.• Enhanced platelet aggregation.• Increased thromboxane synthesis.
Despite clear evidence of a procoagulant state in patients with diabetes, the balance between benefitsandpotentialharmofantiplatelettreatment appears less favourable in patients with diabetes compared with those in other high cardiovascular risk groups.
APT: antiplatelet therapy; ASA: acetylsalicylic acid.

24
Management of Patients with Diabetes
*For patients allergic or intolerant to ASA, use of clopidogrel 75 mg OD is suggested (Class IIa, Level B).ASA: acetylsalicylic acid.
Routine use of ASA* at any dose is not recommended for the primary prevention of vascular ischemic events
in patients with diabetes (Class III, Level A).
ASA* 75-162 mg OD may be considered for secondary
prevention in patients with diabetes and manifest vascular disease for which its benefits
are established(Class I, Level A).
Patients >40 years and at low risk for major bleeding, low-dose ASA* 75-162 mg OD may be considered for primary prevention in patients
with other cardiovascular risk factors for which its benefits are established (Class IIb, Level B).
Diabetes
Management of Patients with Diabetes

25
APT in Patients with Heart Failure
Heart Failure
Largely due to reduced cardiac output, HF is associated with increased risk of thromboembolic events and other ischemic cardiovascular events.
Antiplatelet therapy should be used in all patients with ischemic HF.*Limited evidence suggests ASA may ↑ secondary risk of hospitalization for HF.
HF aetiology:• Ischemic: 70% of patients.
• Hypertension and idiopathic causes: 30% of patients.
Despite HF being associated with a prothrombotic state, antiplatelet therapy is not recommended in the absence of coronary ischemia.
*NoevidenceofbenefitforpatientswithnonischemicHF(otherthanforsecondarypreventionofHFduetoCAD).APT: antiplatelet therapy; ASA: acetylsalicylic acid; CAD: coronary artery disease; HF: heart failure.

26
Management of Heart Failure
CAD: coronary artery disease.
Heart Failure
Ischemic
Antiplatelet therapyshould be dictated by the underlying CAD(Class IIa, Level A).
Routine use of antiplatelet agents is
not recommended(Class III, Level C).
Nonischemic
Management of Heart Failure
27
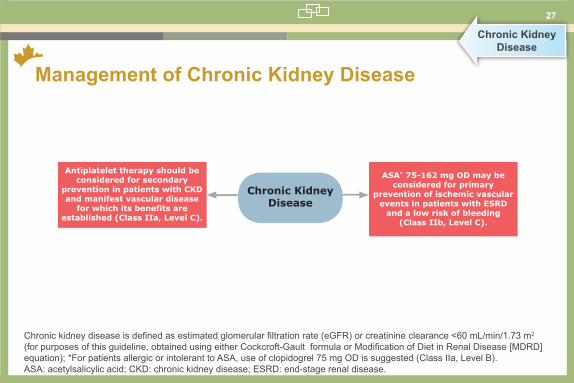
Management of Chronic Kidney Disease
Chronic Kidney Disease
Chronickidneydiseaseisdefinedasestimatedglomerularfiltrationrate(eGFR)orcreatinineclearance<60mL/min/1.73m2 (forpurposesofthisguideline,obtainedusingeitherCockcroft-GaultformulaorModificationofDietinRenalDisease[MDRD]equation); *For patients allergic or intolerant to ASA, use of clopidogrel 75 mg OD is suggested (Class IIa, Level B).ASA: acetylsalicylic acid; CKD: chronic kidney disease; ESRD: end-stage renal disease.
ASA* 75-162 mg OD may beconsidered for primary
prevention of ischemic vascular events in patients with ESRD
and a low risk of bleeding(Class IIb, Level C).
Chronic KidneyDisease
Antiplatelet therapy should be considered for secondary
prevention in patients with CKD and manifest vascular disease
for which its benefits areestablished (Class IIa, Level C).
Management of Chronic Kidney Disease

28
Management in Pregnancy and Lactation
Pregnancy and Breastfeeding
*Use of antiplatelet agents other than low-dose ASA for cardio- or cerebrovascular indications during pregnancy and lactation shouldonlybeconsideredifmaternalbenefitsclearlyoutweighpotentialfetal/infantrisks(ClassIIb,LevelC).ASA: acetylsalicylic acid.
ASA* 75-162 mg OD may beconsidered for use inbreastfeeding women
(Class I, Level C).
Pregnancy andLactation
ASA* 75-162 mg OD is likely safe for use
during the firsttrimester of pregnancy
(Class IIa, Level A).
ASA* can be used safely during the second and
third trimester ofpregnancy
(Class I, Level A).
For cardio- or cerebrovascular disease in which antiplatelet therapy would be indicated innonpregnant women, there
should be similar considerationsfor its use in pregnancy
(Class IIa, Level A).
Management in Pregnancy and Lactation
29
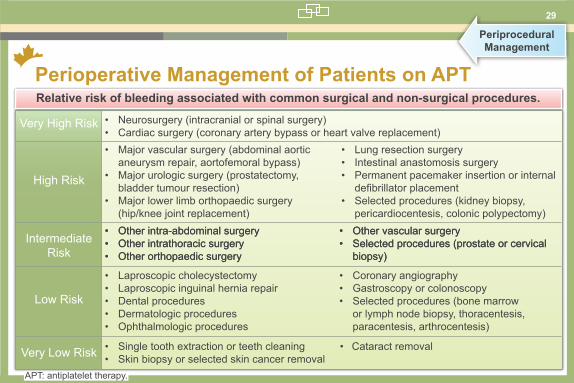
Perioperative Management of Patients on APT
Periprocedural Management
• Neurosurgery (intracranial or spinal surgery)• Cardiac surgery (coronary artery bypass or heart valve replacement)• Major vascular surgery (abdominal aortic
aneurysm repair, aortofemoral bypass)• Major urologic surgery (prostatectomy,
bladder tumour resection)• Major lower limb orthopaedic surgery
(hip/knee joint replacement)
• Lung resection surgery• Intestinal anastomosis surgery• Permanent pacemaker insertion or internal
defibrillatorplacement• Selected procedures (kidney biopsy,
pericardiocentesis, colonic polypectomy)• Other intra-abdominal surgery• Other intrathoracic surgery• Other orthopaedic surgery
• Other vascular surgery• Selected procedures (prostate or cervical
biopsy)
• Other intra-abdominal surgery• Other intrathoracic surgery• Other orthopaedic surgery
• Other vascular surgery• Selected procedures (prostate or cervical
biopsy)
• Laproscopic cholecystectomy• Laproscopic inguinal hernia repair• Dental procedures• Dermatologic procedures• Ophthalmologic procedures
• Coronary angiography• Gastroscopy or colonoscopy• Selected procedures (bone marrow
or lymph node biopsy, thoracentesis, paracentesis, arthrocentesis)
• Single tooth extraction or teeth cleaning• Skin biopsy or selected skin cancer removal
• Cataract removal
Very High Risk
High Risk
Intermediate Risk
Low Risk
Very Low Risk
Relative risk of bleeding associated with common surgical and non-surgical procedures.
APT: antiplatelet therapy.

30
Perioperative Management of Patients taking ASA
The perioperative antiplatelet management will vary depending on the risk of bleeding related to the diagnostic or surgical procedure and the risk of cardiovascular ischemic event. ASA: acetylsalicylic acid; CABG: coronary artery bypass graft.
Patients having minor dental(extraction, root canal), eye(cataract), or skin (biopsy,
skin cancer excision)procedure may continue ASA
without interruption(Class IIa, Level A).
Patient receivingASA requiring
procedure
Diagnostictest/procedureArthrocentesisMinor dental, eye,
skin procedureNoncardiac
surgeryCABG
surgery
Patients having a diagnostic test/procedure associated with a
low risk for bleeding may continueASA without interruption; patients
having a test associated with a highrisk for bleeding should stop ASA
7-10 days before the test/procedure(Class IIa, Level C).
Patients havingarthrocentesis may
continue ASA withoutinterruption
(Class IIb, Level C).
Patients should stop ASA 7-10days before surgery if the risk for cardiovascular events islow and continue ASA if thecardiovascular risk is high
(Class IIa, Level B).
Patients should continue ASA up to the time of surgerywithout interruption
(Class I, Level B).
Perioperative Management of Patients taking ASA

31
Perioperative Management of Patients taking ASA and Clopidogrel
The perioperative antiplatelet management of patients receiving dual-antiplatelet therapy after a coronary stent will vary depending on the type of stent and the urgency of the surgery. ASA: acetylsalicylic acid; BMS: bare-metal stent; CABG: coronary artery bypass graft; DES: drug-eluting stent.
Diagnostic test/procedureArthrocentesisMinor dental, eye,
skin procedure Noncardiac
surgeryCABG
surgery
Patients should continue ASA until the time of
surgery but stop clopidogrel at least 5 days before
surgery (Class I, Level B). Urgent
No Yes
Whenever possible, elective surgery should be deferred for at least 6 weeks after
BMS placement and at least 12 months after DES
placement (Class I, Level B).
For patients with a BMS who require surgery within 6 weeks of placement,
ASA and clopidogrel should be continued in the perioperative period
(Class I, Level B).For patients with a DES who require
surgery within 12 months of placement, ASA and clopidogrel should
be continued in the perioperative period (Class I, Level B).
Patients having minor dental (extraction, root
canal), eye (cataract), or skin (biopsy, skin cancer
excision) procedure should stop clopidogrel
7-10 days before the procedure if it can be done safely (Class IIa, Level C).
Patients should stop clopidogrel 7-10 days before the procedure
if it can be done safely
(Class IIb, Level C).
Patients should stop clopidogrel 7-10 days before the procedure if it can be done so safely (Class IIb, Level C); patients should also stop
ASA before diagnostic tests associated with a high risk for bleeding (Class IIa, Level C).
Perioperative Managementof Patients taking ASA and Clopidogrel
Patient receiving ASA + clopidogrel for a
coronary stent- requiring procedure

32
Key Considerations: Perioperative APT Management
ASA: acetylsalicylic acid; APT: antiplatelet therapy; BMS: bare-metal stent; DAPT: dual-antiplatelet therapy; DES: drug-eluting stent.
• Delay procedures in patients taking DAPT.
• Stop clopidogrel for 7-10 days prior if it can be done so safely.
• Stop ASA for 7-10 days for high-risk surgical procedures.
DO• Discontinue DAPT prior to 1 year in patients
with a DES.
• Discontinue DAPT prior to 6 weeks in patient with a BMS.
• Stop ASA for minor procedures including:• Arthrocentesis. • Dental procedures.• Cataract surgery.• Skin excisions.
DON’T
33
Management of Minor Bleeding
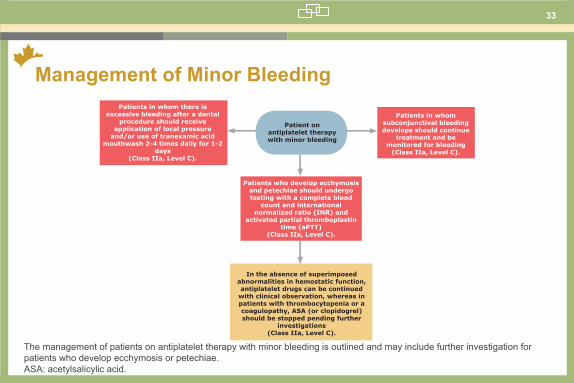
The management of patients on antiplatelet therapy with minor bleeding is outlined and may include further investigation for patients who develop ecchymosis or petechiae.ASA: acetylsalicylic acid.
In the absence of superimposed abnormalities in hemostatic function, antiplatelet drugs can be continued
with clinical observation, whereas in patients with thrombocytopenia or a coagulopathy, ASA (or clopidogrel) should be stopped pending further
investigations(Class IIa, Level C).
Patients who develop ecchymosis and petechiae should undergo testing with a complete blood
count and internationalnormalized ratio (INR) and
activated partial thromboplastin time (aPTT)
(Class IIa, Level C).
Patients in whom there is excessive bleeding after a dental
procedure should receiveapplication of local pressure
and/or use of tranexamic acid mouthwash 2-4 times daily for 1-2
days(Class IIa, Level C).
Patient onantiplatelet therapywith minor bleeding
Patients in whomsubconjunctival bleedingdevelops should continue
treatment and bemonitored for bleeding
(Class IIa, Level C).
Management of Minor Bleeding
34
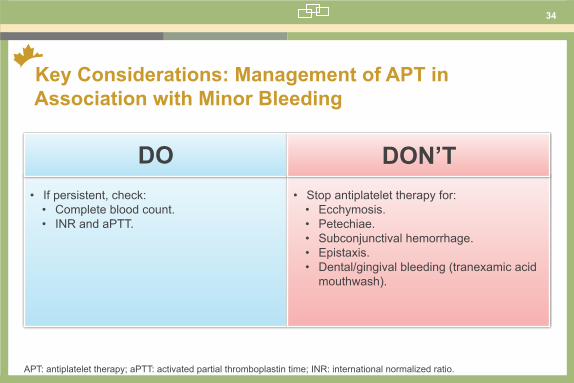
Key Considerations: Management of APT in Association with Minor Bleeding
APT: antiplatelet therapy; aPTT: activated partial thromboplastin time; INR: international normalized ratio.
• If persistent, check:• Complete blood count.• INR and aPTT.
DO• Stop antiplatelet therapy for:• Ecchymosis.• Petechiae.• Subconjunctival hemorrhage.• Epistaxis.• Dental/gingival bleeding (tranexamic acid
mouthwash).
DON’T
35
Combination Therapy with Warfarin and ASA
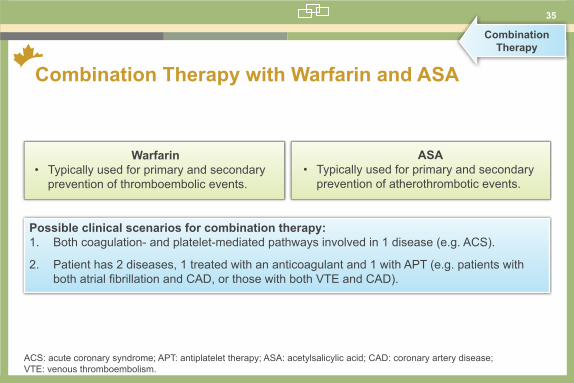
Combination Therapy
Possible clinical scenarios for combination therapy:1. Both coagulation- and platelet-mediated pathways involved in 1 disease (e.g. ACS).
2. Patient has 2 diseases, 1 treated with an anticoagulant and 1 with APT (e.g. patients with bothatrialfibrillationandCAD,orthosewithbothVTEandCAD).
Warfarin• Typically used for primary and secondary
prevention of thromboembolic events.
ASA• Typically used for primary and secondary
prevention of atherothrombotic events.
ACS: acute coronary syndrome; APT: antiplatelet therapy; ASA: acetylsalicylic acid; CAD: coronary artery disease; VTE: venous thromboembolism.

36
Management of Patients Requiring Warfarin
The management of patients requiring warfarin therapy requires an assessment of the risk of bleeding and the medical conditions for which combination therapy may be reasonable. ACS: acute coronary syndrome; ASA: acetylsalicylic acid; BMS: bare-metal stent; CABG: coronary artery bypass graft; DES: drug-eluting stent; INR: international normalized ratio.
Patients who develop ACS that is treated with medical therapy alone, combination warfarin (target INR, 2.0-3.0)/ASA (75-162 mg daily)
therapy is reasonable for up to 12 weeks, at which time ASA may be withdrawn if there are no further
cardiac events(Class IIb, Level C).
Patients with a mechanical prosthetic heart valve, combination warfarin
(target INR, 2.0-3.0) and ASA 75-162 mg daily should be considered, especially in
patients with any mechanical mitral valve or in patients with an older
caged-ball or bileaflet mechanical aortic valve
(Class IIa, Level A).
Patient with anindication for
warfarin therapy
Management of Patients Requiring Warfarin
Although there is insufficient evidence to provide graded recommendations, otherconditions for which combinationwarfarin/antiplatelet therapy is reasonableinclude:
• Patients who have an indication for long-term warfarin therapy and undergo CABG.• Patients with atrial fibrillation who develop a stroke syndrome despite therapeutic anticoagulation with warfarin.• Patients receiving long-term warfarin who receive a coronary stent, 6 weeks of combination warfarin-ASA-clopidogrel is reasonable for patients with a BMS and 12 months of this treatment is reasonable for patients with a DES, with the caveat that a BMS is preferred over a DES in this clinical setting.

37
Interaction Between Clopidogrel and PPIs
Drug Interactions
Clopidogrel requires activation by cytochrome P450 isozyme CYP2C19 in the liver.
The management of patients on dual antiplatelet therapy may include the use of proton-pump inhibitors with minimal inhibition of cytochrome P2C19 in patients considered at increased risk of upper gastrointestinal bleeding. PPI: proton-pump inhibitor.
Interaction with PPIs
• May inhibit CYP2C19• Lansoprazole• Omeprazole• Esomeprazole
• Pantoprazole
Stronginhibitors
Weakinhibitor
38
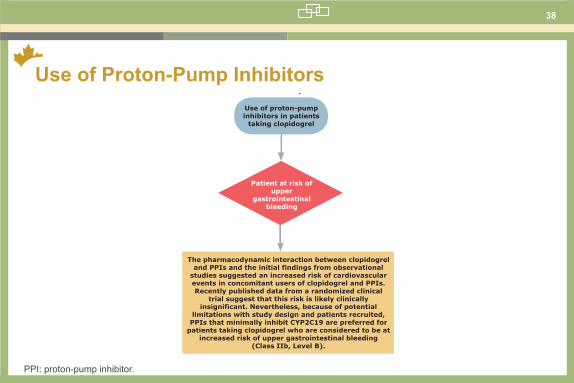
Use of Proton-Pump Inhibitors
PPI: proton-pump inhibitor.
Use of proton-pumpinhibitors in patients
taking clopidogrel
Patient at risk ofupper
gastrointestinalbleeding
The pharmacodynamic interaction between clopidogrel and PPIs and the initial findings from observational
studies suggested an increased risk of cardiovascular events in concomitant users of clopidogrel and PPIs. Recently published data from a randomized clinical
trial suggest that this risk is likely clinicallyinsignificant. Nevertheless, because of potential
limitations with study design and patients recruited, PPIs that minimally inhibit CYP2C19 are preferred for
patients taking clopidogrel who are considered to be at increased risk of upper gastrointestinal bleeding
(Class IIb, Level B).
Use of Proton-Pump Inhibitiors
39
Interaction Between ASA and NSAIDs
ASA binds irreversibly to serine residue at position 529 of platelet COX-1, preventing platelet aggregation.
*InpatientsonASA,theuseoftraditionalNSAIDsshouldbeavoidedandifananti-inflammatorydrugisrequired,aspecificcycloxygenase-2 inhibitor should be considered. ASA:acetylsalicylicacid;COX-1:cycloxygenase-1;NSAID:non-steroidalanti-inflammatorydrug.
Interaction with NSAIDs*
• Traditional NSAIDs form a reversible complex with COX-1, dependent on serum concentrations of the drug with dissociation, platelets assume normal function.
• May inhibit binding of ASA to COX-1.

40
Use of NSAIDs in Patients on ASA
ASA:acetylsalicylicacid;Coxib:cycloxygenase-2inhibitor;NSAID:non-steroidalanti-inflammatorydrug.
Use of NSAIDs inpatients on ASA
Individuals taking ASA for vascular protection should avoid the concomitant use of traditional (non-coxib)
NSAIDs(Class III, Level C).
If a patient taking ASA for vascular protection requires an anti-inflammatory drug, specific
coxibs should be chosen over traditional NSAIDs(Class III, Level C).
All NSAIDs and coxibs should be avoided in patients at increased cardiovascular risk (Class III, Level A).
Use of NSAIDs in Patients on ASA
41
APT: Drug-Drug Interactions
APT: antiplatelet therapy; ASA: acetylsalicylic acid; Coxib: cycloxygenase-2 inhibitor; CV: cardiovascular; NSAID:non-steroidalanti-inflammatorydrug;PPI:proton-pumpinhibitor;UGI:uppergastrointestinal.
• Use PPIs with minimal effect on CYP2C19 in patients at increased risk of UGI bleeding taking clopidogrel.
• Use coxibs over traditional NSAIDs in patients taking ASA for CV prevention but only if absolutely necessary.
DO• Use PPIs that inhibit CYP2C19 in patients
taking clopidogrel or prasugrel.
• Use NSAIDs or coxibs in patients at increased risk of vascular events.
DON’T