pmtct hiv and syphilis implementation - aids 2014 -...
TRANSCRIPT

PMTCT HIV AND SYPHILIS IMPLEMENTATION
Dr John Kinuthia, MBChB, MMED, MPHConsultant Obstetrician & Gynaecologist
Honorary Lecturer, Department of Obstetrics & Gynaecology, UoNHead, Research & Programs, Kenyatta National Hospital
20th International AIDS Conference , July 20th 2014, Melbourne, Australia.
1
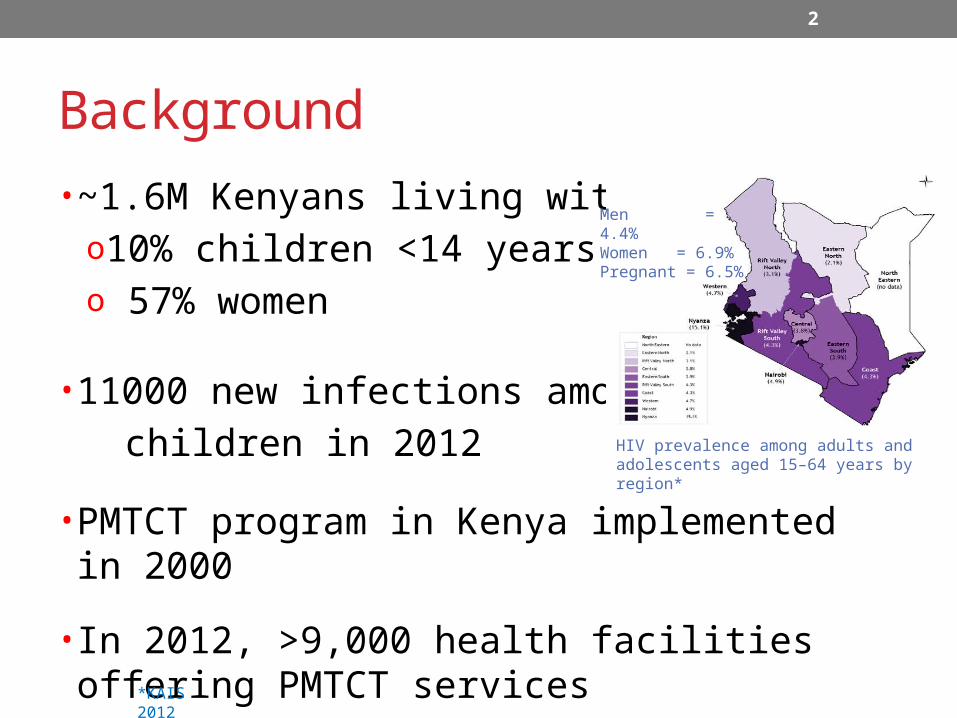
Background• ~1.6M Kenyans living with HIVo10% children <14 yearso 57% women
• 11000 new infections among children in 2012
• PMTCT program in Kenya implemented in 2000
• In 2012, >9,000 health facilities offering PMTCT services
*KAIS 2012
HIV prevalence among adults and adolescents aged 15–64 years by region*
Men = 4.4%Women = 6.9%Pregnant = 6.5%
2

Trends in HIV screening during pregnancy in Kenya
3
KDHS 2003; #KAIS 2008-9; *Kinuthia 2010; **Kiarie 2011;***KAIS 2012

• PMTCT programs focus on women with chronic HIV infection
• Women in window period & those infected after HIV after after HIV testing go unrecognizedo Increased HIV incidence during pregnancy reported**o Increased MTCT risk***
New HIV infections among children reducing
*UNAIDS, 2013;NASCOP, 2011;**Drake 2014; Kinuthia 2010;Gray 2005;*** Kourtis, 2010; Ioannidis, 1999; Pitt ,1997; Garcia,1999; Mofenson,1999
Estimated number of new infections in children aged (0-14): Global trends and projections 2001-20015
oIncreased HIV otesting*
oIncreased availability
o& use of ARVs*
4

HIV-1 incidence during pregnancy and postpartum Kinuthia CROI 2014
• Prospective cohort
• Study populationo HIV-1 rapid antibody test negative
– Day of enrolment or within 3 monthso Resident until 9 months postpartum
• RPR as part of ANC
• HIV testingo Pooled nucleic acid amplification test
(NAAT)– 10 samples
Bondo Hospital HIV prevalence at ANC 26%
Ahero Hospital HIV prevalence at ANC 22%
Rapid test ≤3 months
NAAT testPooled Individual NAAT
-ve Serial NAAT
+ve
-ve
5

Antenatal care services & enrolment
Laboratory
Study clinic• 1304 (56%) enrolled*• RPR 1020 (78.2%)
_
MCH Clinic
Laboratory
HTC • 38 (0.9%) Declined • 799 (18.8%) HIV-1+ve• 3408 (80.3%) HIV-1-ve
Clinical ANC • Palpation• Hematinic• IPT and ITN• TT injection• Infant feeding
coundeling• ARVs
Antenatal profile• Hemoglobin• RPR• Blood group• Urinalysis
Home
Registration• 4245 women• May 2011-June 2013
ReviewNurse/clinician
*2351 women met eligibility criteria
6

Baseline characteristics (n=1304)Characteristic N n (%) or Median (IQR)Age 1304 22 (19 - 27)
Education level (years) 1304 8 (7 - 10)
Married 1304 1022 (78)
Marriage duration (years) 1019 4 (1 - 8)
Partner age difference* 1171 6 (4 - 10)
Gravida 1304 2 (1 - 4)
History of STI 87 (7)
Partner HIV statusPositiveNegativeUnknown
130418 (1)841 (64)445 (34)
* Years older
7

HIV-1 incidencePre-enrollment Enrollment Follow up
24 New HIV infections2.34
(0.56 – 4.34)
5 Seroconversion detected at enrollment 1.11 (0.61 – 2.00)
-ve +ve5 Acute infection detected at enrollment 5.00
(0.62 – 19.38)
-ve +ve14 Acute infection detected during follow-up 3.11
(0.38 – 5.84)
-ve –ve
Incidence rate95% CI
+ ve repeat rapid antibody test
- ve repeat rapid antibody test
+ ve NAAT test
Rapid test ≤3 months
NAAT testpooled Individual NAAT
-ve Serial NAAT+ve
8

Correlates of acute HIV-1 infectionOR (95% CI) p
Age (per year increase) 1.0 0.9 – 1.0 0.2
Married 0.7 0.3 – 1.7 0.4
Shorter marriage duration (yrs) 1.14 0.3 – 1.7 0.05
Partner age difference* 1.00 0.98 – 1.02 0.88
History of STI 3.8 1.4 – 10.6 0.01
CT 2.6 0.7 – 8.8 0.14
GC 1.8 0.2 – 14.1 0.58
TV 1.2 0.7 – 2.3 0.50
Syphilis 10.0 2.0 – 46.0 0.005
BV 2.6 1.2 – 5.8 0.019
9

Baseline STIs/genital tract Infections
10

Challenge of incident maternal HIV infections to eMTCT
• High HIV viral load*
• Mother not known to be HIV infected
• No HIV PMTCT interventionoNo maternal ARVoNo infant ARVoObstetrical interventionsoEnhanced counseling on
exclusive breastfeeding
• Infant infection due to• Maternal infection after• ANC testing o 26% (2008) to 34%
(2014) in South Africa**
o 43% of infant infections iBotswana in 2007***
*Kourtis 2010; Ioannidis 1999; Pitt 1997; Garcia1999; Mofenson 1999; **Johnson 2012; ***Lul CROI 2009
11
J Acquir Immune Defic Syndr. 2012 ;59(4):417-25. The contribution of maternal HIV seroconversion
during late pregnancy and breastfeeding to mother-to-child transmission of HIV**
16th CROI 2009. Montreal. Abstract 91HIV Incidence in Pregnancy and the First Post-
partum Year and Implications for PMTCT Programs, Francistown, Botswana, 2008
“In this mature and successful PMTCT programme, new and undetected maternal infections may be causing nearly half of infant infections.” Lul et al

HIV retesting in pregnancy• High acceptability*
• Cost effective **
• Limitationo Increased workloado Overstretched workforce o Late initiation of ANCo Miss infection during window
period
• Role of more sensitive assays****Willams 2013; Kinuthia2010; **Soorapanth 2006;Sansom 2003; ***Busch1997;Morandi 1998;Quinn 2000; Hecht 2002
12
Obstet Gynecol. 2003 Oct;102(4):782-90.Human immunodeficiency virus retesting during pregnancy: costs and effectiveness in preventing
perinatal transmission**
• 6.2 per 1000 person-years HIV incidence• 192 infections in women detected • 37 infant infections prevented• 655 infant life-years saved per 100,000
women tested• 5.2 million US$ net saving
“Second test would result in net savings in populations with HIV incidence of 1.2 per 1000 person-years or higher” Sansom

• HAART for HIV infected pregnant and breast feeding women irrespective of CD4 count, WHO stage
• Option A and B is being phased out
13

Syphilis in pregnancyPLoS Med. 2013;10(2)
Global estimates of syphilis in pregnancy and associated adverse outcomes: analysis of multinational antenatal surveillance data
Bull World Health Organ. 2013 Mar 1;91(3):217-26
Untreated maternal syphilis and adverse outcomes of pregnancy: a systematic review
and meta-analysis
Prematurity or low birth weight; 6%
Neonatal death; 9%
Congenital syphilis; 15%
Fetal loss or stillbirth,; 21%
Not affected; 49%
Chart Title
Premature or low birth weight infants; 65000
Neonatal deaths; 90000
Congenital syphilis; 150000
Still births or early neonatal
deaths; 215000
Chart Title
. *Newman;**Gomez
14

Syphilis increase risk of HIVAIDS. 2006 Sep 11;20(14):1869-77.
Maternal syphilis infection is associated with increased risk of mother-to-child transmission of HIV
in Malawi
• Maternal syphilis associated with Intrauterine HIV MTCT, after adjusting for maternal log10 HIV-1 viral load and low birth weight
ARR, 2.77; 95% CI, 1.40–5.46]
• Maternal syphilis associated with Intrapartum/postpartun MTCT after adjusting for recent fever, breast infection, LBW and maternal log10 HIV-1 viral load
ARR, 2.74; 95% CI, 1.58–4.74)
• Concurrent maternal syphilis infection associated vertical HIV transmission compared with only history of treated syphilis 100% vs. 21%, P = 0.01 or
100% vs. 14% ,p = 0.0015 for women with no history of syphilis
• Non-Zidovudine exposed women with concurrent syphilis transmitted HIV to their infants compared to those with only a history of syphilis
100% vs. 0% (P = 0.006)
15
Mwapasa 2006
Int J Gynaecol Obstet. 1998 Dec;63(3):247-52.Maternal syphilis and vertical perinatal transmission of human immunodeficiency virus type-1 infection
Lee 1998

Prevalence of syphilis and HIV among pregnant women - Kenya
KAIS 2007 KAIS 2012
HIV positive; 8.9%
HIV & VDRL nega-tive; 89.5%
VDRL Positive; 1.6%
HIV positive; 6.5%
HIV negative; 93.5%
16

Screening for syphilis during pregnancy
• Routine test in antenatal care
• 1st ANC visit o CDC recommends repeat in 3rd trimester*
• Non-treponomal tests o RPR/RPR
*CDC 2002;** KAIS 2012
Counselled on MTCT Counselled on HIV testing Counselled on syphilis screening
0%10%20%30%40%50%60%70%80%90%
100%
76.6%90.1%
47.2%
Counselling experience among women aged 15 -54 years attending ANC**
17
• Barriers to screeningo Costo ANC non-attendanceo Stock out of test kitso Wait time for results

Correlates of Syphilis infection (n=1020)OR (95% CI) p
Age (years) 1.05 (0.97-1.16) 0.2
Education (years) 0.82 (0.64-1.05) 0.11
Married 3.12 (0.40-24.3) 0.3
Ever trade sex 1.22 (0.54-2.73) 0.63
History of STI 10.36 (3.20-33.55) <0.001
Partnership duration (yrs) 1.09 (1.00-1.19) 0.055
Unknown partner HIV status 1.71 (0.53-5.42) 0.37
Multiple sex partners 11.36 (1.30-98.7) 0.03
18
*yrs=years

X
19

Dual eliminations strategies supports attainment of MDGs • Prevent Congenital syphilis
• Fewer spontaneous abortions•
• Fewer still births
• Reduced risk of HIV acquisition
• Reduced HIV shedding
• Reduce risk of MTCT of HIV
20

Why combine efforts towards elimination of MTCT of HIV and syphilis
• Sexually transmitted infections that can affect foetus/infant
• ANC entry point for care
• Point of care testing possible
• Effective interventions availableo Syphilis treatableo PMTCT of HIV reduce risk to <2%
• Combined services more efficient
21

Acknowledgements• Mama Salama Study participants
• Ahero and Bondo study staff
• Research team
• KNH/UoN• John Kinuthia• Daniel Matemo• James Kiarie
• UW• Grace John-Stewart• Alison Drake• Katherine Odem-Davis• Barbara Lohman Payne• Barbra Richardson• Jennifer Slyker• Jennifer Unger• Julie Overbaugh• Scott McClelland • Carey Farquhar • Anjuli Wagner • Gwen Ambler
• CDC/KEMRI• Clement Zeh• Lisa Mills
• Funding• NIH (P01 HSD 064915)• CFAR (P30 AI27757)
: